
Abstract
Objective:
To describe the methylphenidate (MPH) effects on weight, height, and body mass index (BMI) in a Spanish sample diagnosed with attention-deficit/hyperactivity disorder (ADHD).
Methods:
Patients (6–18 years) diagnosed with ADHD treated at our Unit with MPH in the last 10 years were included in an observational longitudinal study. Weight, height, and BMI Z scores were measured at baseline and at last follow-up.
Results:
Three hundred forty-two patients (mean [standard deviation] age: 10.7 [3.8] years, 80% males) were included. Mean dose was 1.25 (0.40) mg/(kg·d). After 27 (14–41) months taking MPH, weight and BMI standard deviation score (SDS) were reduced by treatment (baseline weight-SDS: 0.34 [1.22], follow-up weight-SDS: −0.06 [1.38], t-test p < 0.001; baseline BMI-SDS: 0.35 [1.10], and follow-up BMI-SDS [SDS]: −0.23 [1.08], t-test p < 0.001). In the whole sample, no differences in height before and after treatment were observed. However, considering only the group of patients who were children 6–12 years (68.6%) when starting treatment, height was slightly affected (baseline height-SDS: 0.04 [1.14], follow-up: −0.10 [1.11], p < 0.001). This effect was not observed if treatment was started during adolescence. Linear regression analysis showed that age starting MPH (B = 0.07, p = 0.003), dose (B = −0.50, p = 0.001), and duration of treatment (B = 0.07, p = 0.031) affect follow-up height.
Conclusion:
MPH slightly decreased weight and BMI in this group of ADHD patients followed naturalistically over 2.2 years, and slightly affected height only if treatment was started before the age of 12. Girls, children who started treatment being younger or children on higher MPH doses, showed greater impact in height.
Introduction
S
In a review by Faraone et al. (2008) that assessed the long-term effects on growth of stimulants in children with ADHD, some studies showed growth suppression and some did not show significant effects. This review also shows that the slight growth deficit caused by long-term treatment with stimulants tends to attenuate over time (Faraone et al. 2008).
In a recently published birth cohort study that included patients with ADHD (Harstad et al. 2014) followed for 26.2 years, stimulants were not associated with a reduction in final adult height. A group of patients with ADHD without pharmacological treatment was also included. Neither ADHD itself nor stimulants were associated with differences in the magnitude of peak height velocity (PHV) and final adult height. Only the age of PHV was slightly later among boys treated with stimulants, but not in girls. This study, which is the widest and longest done so far, suggests that ADHD treatment with stimulant medication is not associated with differences in adult height or significant changes in growth. To date, only one study about ADHD and growth performed in a Spanish population has been published (Durá-Travé et al. 2012). Authors found that, after 2 years of treatment, the mean height value was lower than expected for age, and this difference decreased after 48 months of treatment, concluding that methylphenidate (MPH) has a transitory negative effect on growth that attenuates in the long term. Our study provides more data about Spanish population, considering factors such as sex, age at starting treatment, dose, and duration of treatment.
Methods
For this observational longitudinal study, data were obtained from the review of the medical records of all patients with a DSM-IV-TR (4th ed., DSM-IV-TR; American Psychiatric Association 2000) diagnosis of ADHD, treated with MPH in the Child and Adolescent Psychiatry Unit, Clinica Universidad de Navarra. Only patients between 6 and 18 years with MPH treatment, in different formulations (pellets, osmotic release and immediate release) were included.
The initial sample was 440 patients, but children who were younger than 6 years when treatment was prescribed (n = 8), or those who were older than 18 years in the follow-up assessment (n = 69), were excluded. None of the patients was taking any other medication or had a current or past illness that may affect growth. The final sample was 342 patients, because 21 patients were not measured at follow-up.
In this observational follow-up study of a cohort group, patients' weight Z score, height Z score, and body mass index (BMI) Z score were assessed at baseline (when MPH was prescribed), and at last follow-up. Z scores were calculated as described below: - Weight Z score: (Actual weight − mean weight for age and sex)/standard deviation [SD]. - Height Z score: (Actual height − mean height for age and sex)/SD. - BMI Z score: (Actual BMI − mean BMI for age and sex)/SD.
The normalized values for Spanish children and adolescents of the Andrea Prader Center (Ferrández-Longás et al. 2004) were used as standard references.
Statistical analysis was performed with IBM SPSS Statistics v.20.0 for Windows. Results are described as mean and SD, except for variables that did not meet criteria of normality, which were expressed as median and interquartile range (25–75 percentile). Paired t-test was used to compare Z scores before and after treatment. Pearson coefficient was used to evaluate the correlation between anthropometric values and treatment-related factors. After exploring correlations, a multiple linear regression was made to assess the possible contribution of the different treatment-related factors (age at which MPH is started, dose of MPH, and duration of treatment) as the independent variables, considering height standard deviation score (SDS) at follow-up as the dependent variable. This regression was controlled by age and sex. Statistical significance was defined for all comparisons at p-value of 0.05 or less.
Results
Descriptive data
Characteristics of the sample are summarized in Table 1. Patients were 10.66 (3.8) years old when they started treatment. Two hundred forty-nine (68.6%) were children and 114 (31.4%) adolescents. Two hundred ninety (79.9%) were males and 73 (20.1%) females. All of them were treated with MPH. Mean dose was 59.6 (22.9) mg/d, or 1.25 (0.40) mg/(kg·d). Patients were treated for 27 (14–41) months, with a minimum of 1 month, and a maximum of 129 months.
Median and IQR.
IQR, interquartile range; MPH, methylphenidate; SD, standard deviation.
Baseline data
At baseline, before starting treatment, patients showed weight (baseline weight-SDS: 0.34 [1.22], t = 5.55; p < 0.001), and BMI (baseline BMI-SDS: 0.35 [1.10], t = 0.99; p < 0.001), and these differences were statistically significant. Height-SDS before starting treatment was 0.06 (1.12) SDS, and did not differ from standard population (t = 0.94, p = 0.35).
MPH and weight, height, and BMI by age
Considering the whole group, weight-SDS significantly decreased at follow-up (baseline weight-SDS 0.34 [1.22], follow-up: −0.06 [1.38]; p < 0.001). BMI-SDS is also affected: 0.35 (1.10) at baseline and −0.23 (1.08) at follow-up, p < 0.001. There were no differences in height before and after stimulant treatment: baseline 0.06 (1.12), follow-up: −0.004 (1.11), p = 0.096. The effect of MPH on growth is described in detail in Table 2 and Figures 1 –3, in which longitudinal plots, including pre and postdata of weight, height, and BMI Z scores, are shown. However, considering whether patients were children (6–12 years) or adolescents (13–18 years) when they started medication, in the group of children, height was slightly affected by treatment (baseline height-SDS: 0.04 [1.14]; follow-up height-SDS: −0.10 [1.11]; p < 0.001). This effect was not observed if MPH was started during adolescence. In such cases, height-SDS was even slightly above the average at follow-up (baseline height-SDS 0.15 [1.09], follow-up height-SDS: 0.22 [1.33]).
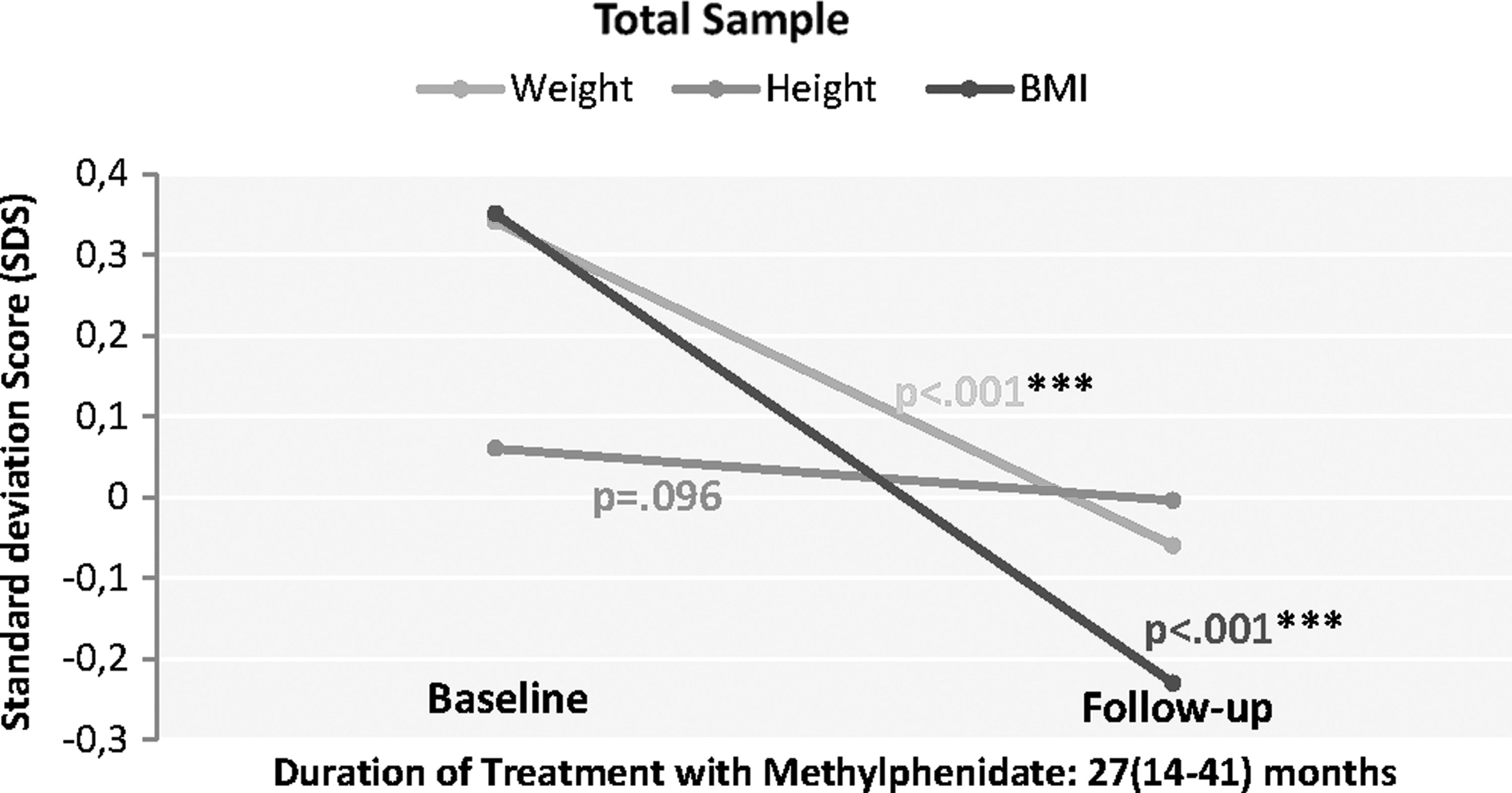
Weight, height, and BMI at baseline and after MPH treatment in total sample. Considering the whole group, weight-SDS significantly decreased at follow-up (baseline weight-SDS 0.34 [1.22], follow-up: −0.06 [1.38]; p < 0.001). BMI-SDS is also affected: 0.35 (1.10) at baseline and −0.23 (1.08) at follow-up, p < 0.001. There were no differences in height before and after stimulant treatment: baseline 0.06 (1.12), follow-up: −0.004 (1.11), p = 0.096. In Figures 2 and 3 we represent these effects considering whether patients were children or adolescents. BMI, body mass index; MPH, methylphenidate; SDS, standard deviation score.
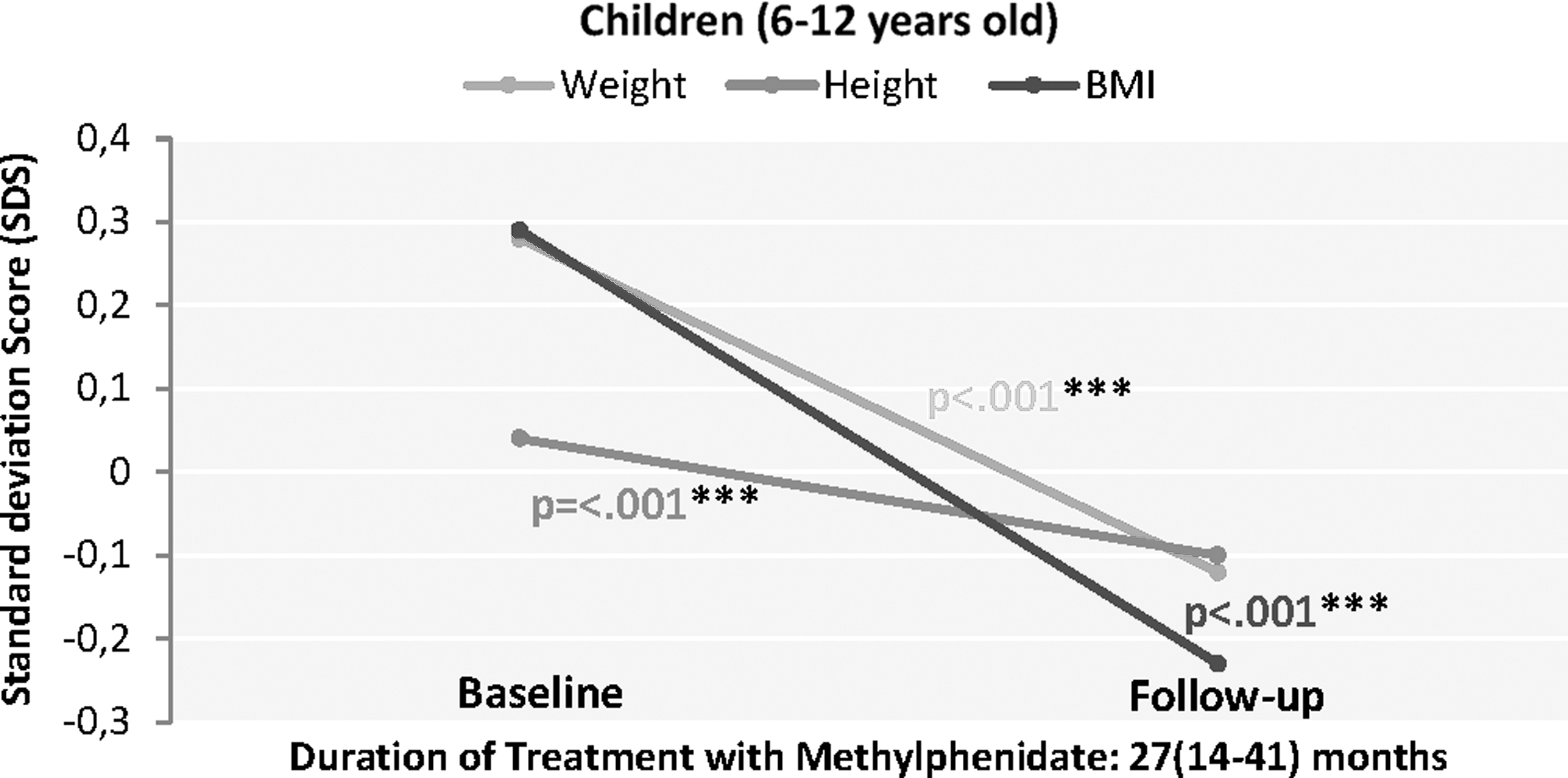
Weight, height, and BMI at baseline and after MPH treatment in children (6–12 years of age). In the group of children (6–12 years of age), height was slightly affected by treatment (baseline height-SDS: 0.04 [1.14]; follow-up height-SDS: −0.10 [1.11]; p < 0.001). Weight and BMI significantly decreased at follow-up (p < 0.001). BMI, body mass index; MPH, methylphenidate; SDS, standard deviation score.
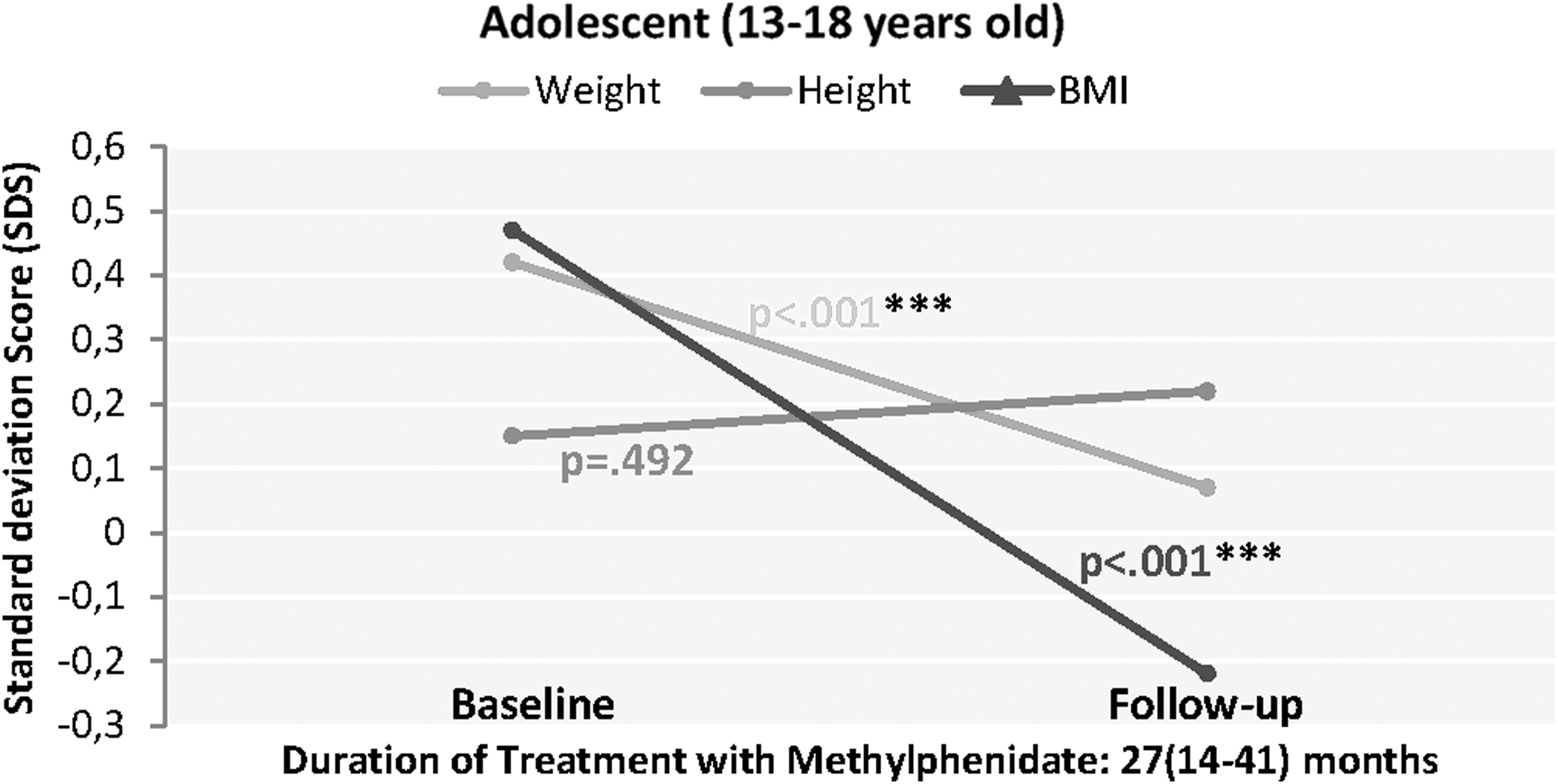
Weight, height, and BMI at baseline and after MPH treatment in adolescent (13–18 years of age). In the group of adolescents (13–18 years of age), height was not affected if MPH was started during adolescence. However, both weight and BMI significantly decreased at follow-up (p < 0.001). BMI, body mass index; MPH, methylphenidate.
In bold: p < 0.05, statistically significant.
BMI, body mass index; SDS, standard deviation score.
MPH and weight, height, and BMI by sex
If we split the sample into girls (n = 68) and boys (n = 274), before starting treatment, weight-SDS and BMI-SDS were above the average (p < 0.001) in boys and girls, but this difference was statistically significant for boys but not for girls. Although weight and BMI was reduced in boys and girls, the magnitude of this effect was stronger in the group of girls (Table 3).
In bold: p < 0.05, statistically significant.
BMI, body mass index; SDS, standard deviation score.
In the group of boys, weight and BMI were affected by treatment, but height-SDS was not reduced. However, considering only girls, MPH also reduced height-SDS significantly (baseline height-SDS: 0.12 [1.56], follow-up height-SDS: −0.10 [1.44], p = 0.01) (Table 3).
Treatment-related factors and growth
Table 4 shows the correlations between age starting treatment, dose, and duration of treatment, and growth. There was a weak but significant correlation between age starting MPH and differences in height-SDS between baseline and follow-up (R = −0.10, p = 0.04*). The higher the dose of MPH, the higher the reduction in the SDS of the anthropometric values (R = 0.1, p = 0.018* for difference in weight-SDS, R = 0.12, p = 0.026* for difference in height-SDS and R = 0.18, p < 0.001*** for BMI-SDS). The duration of treatment did not correlate significantly with height, but the longer the duration of treatment, the higher the difference between baseline and follow-up weight (R = 0.18, p < 0.001***) and BMI (R = 0.10, p = 0.004**).
All values expressed in R Pearson (p), except for aduration of treatment, expressed in Rho Spearman.
In bold: p < 0.05, statistically significant.
Dif-BMI, difference between baseline and follow-up BMI, in SDS; Dif-Height, difference between baseline and follow-up height, in SDS; Dif-Weight, difference between baseline and follow-up weight, in SDS.
BMI, body mass index; MPH, methylphenidate; SDS, standard deviation score.
Results of the multiple linear regression to assess the possible contribution of the different treatment-related factors as the independent variables, considering height-SDS at follow-up as the dependent variable, are shown in Table 5. According to this regression analysis, only age starting treatment, but not higher doses and duration of treatment predicted final height. This regression was controlled by age and sex.
In bold: p < 0.05, statistically significant.
R2 = 0.056.
CI, confidence interval; MPH, methylphenidate.
Discussion
To our knowledge, this is the largest sample and with the widest age range describing the influence of MPH on growth in ADHD children and adolescents in a Spanish sample so far.
Data regarding basal measures: height and weight
The association between ADHD and the growth process is still controversial. Some authors suggest the hypothesis that this apparent growth retardation is due to the disorder itself (Ptacek et al. 2009). Likewise, a delay in brain maturation has been described (Batty et al. 2015); if the same effect might be happening with the pubertal growth spurt, it could be delayed slightly.
Before starting treatment, in our group of patients with ADHD, height SDS was within the normal range (0.06 [1.12] SDS). These data are consistent with most of the studies that suggest that patients with ADHD do not show growth delays intrinsic to the disorder (Swanson et al. 2007; Biederman et al. 2010; Harstad et al. 2014). However, our results are not congruent with the other Spanish study (Durá-Travé et al. 2012), which showed that mean height at diagnosis was lower than expected (−0.06 SDS, height deficit: 0.42 cm). These differences between both studies may be due to sample size, age, sex, psychosocial, ethnic, or geographic factors. Although both studies were performed in Navarre (Spain), due to the characteristics of our hospital, which is a tertiary referral center for ADHD, patients come from different provinces of the country.
At baseline, weight (weight-SDS: 0.34 [1.22]) and BMI (BMI-SDS: 0.35 [1.10]) values were above the average in our sample, which is consistent with a recent meta-analysis (Cortese et al. 2016), in which the prevalence of obesity was increased by about 40% in children with ADHD. The odds ratio for overweight in children and adolescents with ADHD with no treatment is 1.5 (Waring and Lapane 2008).
As Table 2 shows, at baseline, the height, weight, and BMI data in the adolescents' subgroup are higher than in the children subgroup. Although the reasons why these differences are observed are unknown, they could be explained by a secular effect.
Reductions in weight, BMI, and height after treatment
The difference between baseline and follow-up weight in our sample, after 27 months of treatment, was −0.4 SDS (0.34 SDS minus −0.06 SDS). This would mean that, for a 10-year-old boy with an average weight (“0” SDS), the weight would be 2.3 kg less than expected for his age and sex. This result is consistent with many other studies, since decreased appetite is a common effect of MPH and other stimulants.
Although adolescent growth spurt occurs earlier in girls than boys, we decided to set the cutoff point in 12 years on both boys and girls, to distinguish between children and adolescents. For height, the difference between baseline, and follow-up was −0.06 SDS (no statistically significant), but considering only the group of children that started treatment being under 12, this difference rose to −0.14 SDS, which would mean (for a10-year-old boy) that height would be ∼0.86 cm less than expected after 2 years of treatment with MPH. These findings underline the importance of monitoring growth data in clinical practice.
As Table 2 shows, at follow-up, the height, weight, and BMI data in the adolescents' subgroup are higher than in the children subgroup. This difference is maintained in the follow-up determination. In fact, in the adolescents' subgroup only weight and BMI become reduced significantly by treatment, but not height. In the children subgroup the three variables become statistically significant. The most likely explanation for this finding is that if patients are older when they start treatment, their growth process is more advanced and, therefore, the stimulant treatment will have a smaller impact on their growth.
According to the individual differences around the time of the pubertal spurt, and considering that children can show an early or late maturation, baseline and follow-up Z scores were shown to describe the patterns of height Z scores in this longitudinal analysis (Spencer et al. 1998; Karlberg et al. 2003; Hermanussen 2010).
The subgroup analysis by age, dividing the sample into two subgroups, children (6–12 years) and adolescents (13–18 years), as shown in Table 2, represents an innovative way of turning the wide age range, which may be considered as a weakness of this study, into a strength. This strategy has allowed us to focus on a narrower age range. The results of the subgroup analysis suggest that the age at which the patients start treatment with MPH, can be considered as one of the most relevant factors on the treatment effect on growth (Tables 4 and 5).
Differences by sex
Although weight is reduced in boys and girls, the magnitude of this effect was more evident in girls, which could be due to the fact that girls, especially teenagers, may be concerned about weight.
In our study, the impact of treatment on height is higher in the group of girls (Table 3). The ratio between boys and girls (274 boys vs. 68 girls) may play a role in these findings, taking into account that this ratio is representative of the ADHD epidemiological distribution. Although girls were slightly younger when starting MPH (girls were 10.4 [2.7] years, and boys 10.9 [2.9] years, p = 0.193), and were treated for a longer period (32.7 [19.4] months, boys 29.4 [22.5], p = 0.253), none of these differences was statistically significant. There were no differences in MPH dose between girls and boys (1.22 [0.04] mg/(kg·d) for girls and 1.22 [0.02] mg/(kg·d) for boys, p = 0.930). However, in the regression analysis, neither sex nor the interaction between sex and height were predictive variables of the effect of MPH on the difference between baseline and follow-up height (Table 5). The possible reasons for this greater reduction in girls may be a greater reduction in food intake, or hormonal mechanisms, although sexual maturation does not seem to differ with stimulant treatment (Greenfield et al. 2014).
Our results differ with the findings of the study by Harstad et al. (2014), which suggest that males are more sensitive to the effect of stimulants. A positive correlation between duration of stimulant treatment and age of the pubertal spurt only among boys was found, but not in girls. In a naturalistic study, Biederman et al. (2010) did not find differences in weight or height between boys and girls. The only exception was the presence of comorbidity with depressive disorder, which was associated with smaller height in males and larger weight in females (Biederman et al. 2010). In both samples, patients were followed from childhood to adulthood. In our study, the presence of comorbidity with other psychiatric disorders was not registered. In a retrospective chart review performed in Korean children (Kim et al. 2014), as in our study, weight Z score decreased significantly more in girls compared with boys, but no differences were found for height.
Treatment-related factors that may influence growth
Mean MPH dose was 1.25 (0.40) mg/(kg·d), which is similar to the recommendations of the International Guidelines (Pliszka and AACAP Work Group on Quality Issues 2007; National Collaborating Center for Mental Health (UK) 2009).
A significant correlation between mean dose of MPH and the age of patients at baseline, with differences between baseline and final height, but not for duration of treatment, was found. Whereas an interaction between age at onset of treatment and length of stimulant treatment was very likely, the three variables were included in the regression analysis, which suggested that both age starting MPH and duration of treatment may influence the effect on height (Table 5).
Our results are consistent with several studies that concluded that height is not affected by stimulants in children and adolescents with ADHD (Kramer et al. 2000; Biederman et al. 2003; Pliszka et al. 2006), and also in adults (Biederman et al. 2010; Harstad et al. 2014). However, our results differ from previous evidence showing an impact on growth in children with prolonged stimulant medication for ADHD (Lisska and Rivkees 2003; MTA Cooperative Group 2004; Charach et al. 2006; Swanson et al. 2007; Faraone et al. 2008; Zhang et al. 2010; Durá-Travé et al. 2012; Poulton et al. 2013; Powell et al. 2015). Taken together, these results suggest that the effect of MPH on height may be greater during the initial phases of treatment and attenuates later. All these studies are heterogeneous in terms of sample size, duration of treatment, age, and boy–girl ratio, and none of them includes data from patients who have reached adulthood. Therefore, more follow-up studies to assess the evolution of these patients when they reach adulthood are needed.
The wide age range of our sample (6–18 years) is similar to other studies (Biederman et al. 2010; Poulton et al. 2013), but differs from others that focus on a narrow age range (Swanson et al. 2007). This characteristic implies that the patients' follow-up period may be longer, and the attenuation effect of the treatment impact on growth can be better observed. However, this feature may also be considered a limitation. The variations in the growth of children and adolescents during this long follow-up period can be confounded by other factors, such as individual differences in the pubertal spurt.
Considering that only one study has been published in the Spanish population, and the differences obtained in the results, we will discuss these discrepancies more deeply (Durá-Travé et al. 2012). First, patients assessed by Durá-Travé et al. were all treated with osmotic-release MPH for at least 4 years. In contrast, in our study, different types of release (Osmotic Release Oral System [OROS]-MPH, immediate release, or extended release pellets) were included, and the length of medication treatment was shorter (27 [14–41] months, with a minimum of 1 month, and a maximum of 129 months). Second, although estimated height deficit was similar in both studies (0.83 cm in the sample by Durá-Travé et al., and 0.86 cm in our sample), the difference was not statistically significant in our group. This situation could be attributed to the lower age in the sample of Durá-Travé et al.; 8.1 years versus 10.7 in our study (Durá-Travé et al. 2012). Third, at baseline, the patients of the Durá-Travé et al. sample showed mean weight and height values lower than expected for age and sex, in contrast to our patients, which showed overweight and height within the normal range. Finally, it is also important to consider the difference in sample size (342 vs. 157 patients), and the lower proportion of girls in our study (20% vs. 31%). Standard references used to calculate weight and height Z scores were taken from the Andrea Prader Center (Ferrández-Longás et al. 2004) in both studies.
In spite of the great amount of data regarding this topic, only a few reviews have been conducted (Poulton 2005; Faraone et al. 2008; Vitiello 2008; Ptacek et al. 2014), and a systematic review or a meta-analysis has not been published. Authors argue two possible theories to explain the effects of stimulants on growth. First, that stimulants produce a delay in pubertal growth spurt, and these children grow up later, as the study by Harstad et al. (2014) suggests. The second is that indeed children receiving treatment with MPH reach a lower-than-expected final height. According to the most recent findings, probably the overall evidence shows that a temporary delay in growth arrest occurs, but the final height once patients reach adulthood does not differ, so the latter theory seems more likely. However, because in our study the follow-up period is on average about 2 years, neither of the two theories can be supported with our data.
This pattern of transient negative effect on growth and subsequent attenuation is frequently observed in patients when they start treatment with stimulants. They usually show weight curves with a “U-shape” with an initial decline and later recovery, and an initial flattening with later retrieval in the height curves. When doctors are deciding on the treatment of a patient with ADHD with psychostimulants, data about the evolution of growth of that particular child should be monitored and taken into account. Our findings and other studies assessing the height of children and adolescents in treatment for ADHD, show a difference of <1 cm after 2 years of treatment between treated and untreated patients, compared with the reference population. However, this is a mean value, and in individual cases this effect could be important. In addition, studies assessing the final height reached in adulthood suggest that, despite a possible delay (about 6 months) in the pubertal growth spurt, the final height is not reduced. ADHD is a psychiatric disorder with noteworthy medical, social, academic, and legal impact, so it should be treated effectively. Considering this evidence, clinicians should individualize each case, and discuss with the family of the patient the balance between the benefit of treating and the possible harm of remaining untreated.
Limitations and future directions
This study has several limitations: we did not include a control group of nonmedicated subjects with ADHD, therefore, the results are more suggestive than definitive; we analyzed anthropometric values only at diagnosis and follow-up, without intermediate determinations; patients were treated with different formulations of MPH (pellets, osmotic release, immediate release); we did not control for adherence or medication holidays, current presentation (hyperactive–impulsive, combined, or inattentive); the wide age range (6–18 years) may be considered a limitation; psychiatric comorbidity was not taken into account; and expected final height according to familial target height was not available.
More studies considering factors such as dose, length of treatment, medication holidays, age at baseline, sex, and adult final height, in patients with ADHD taking stimulants, should be conducted. Moreover, a systematic review or meta-analysis is needed to clarify this issue.
Conclusions
In this group of ADHD patients treated with MPH for ∼2 years, their weight and BMI decreased significantly, but their height was affected only if treatment was started before the age of 12, and the real effect on height is about 0.8 cm. Girls, children who started treatment being younger or who were taking higher doses, showed greater impact on height.
Clinical Significance
In our sample of ADHD patients, long-term treatment (∼2 years) with MPH resulted in a slightly, but significant, decrease of weight, BMI, and height. Considering this evidence that support other prior investigations, clinicians should not only monitor weight, height, BMI, and height velocity in each visit, but also compare data with the general population and review the changes in the growth curve of the child. This information should be provided clearly to parents. Some issues such as different formulations of medications, or holidays during non-school periods, must be taken into account in those cases with greater impact of growth reductions. Given that our results suggest that the effect of MPH on height may be greater in children than in adolescents, the dose of MPH should be adjusted to the minimum effective, especially in younger children.
Clinical Relevance
The role of factors, such as sex, dose, age at treatment onset, and duration of stimulant treatment for ADHD, in growth remains unclear. This article includes a large sample of Spanish patients and provides data considering also age and sex.
Disclosures
A.D.-S., has received research funds for her department (non-personal) from Caja Navarra Foundation (CAN), Otsuka Pharmaceutics, Lundbeck, and Shire. She has served as Consultant/Advisory Board for Alicia Koplowitz Foundation and Editorial Médica Panamericana. She has served in the Speaker's Bureau and has given talks on Continuous Medical Education (not about a product) for Shire. M.V.-V., has received research funds for her department (non-personal) from Caja Navarra Foundation (CAN), Vasco-Navarra Society of Psychiatry (SVNP), Government of Navarra, and Spanish Society of Child and Adolescent Psychiatry (AEPNYA). She has received financial support for continuous scientific education from Shire, Janssen, and Lundbeck. J.J.M.-M., has received research funds for his department (non-personal) from Caja Navarra Foundation (CAN), Carlos III Health Institute, Government of Navarra, Qpea Foundation, and Shire. He has received financial support for continuous scientific education from Shire, Lilly, Rovi, Roche, and Pfizer. P.C.-M., has received research funds for her department (non-personal) from Caja Navarra Foundation (CAN), Eli Lilly, Lundbeck, and Shire. She has served as Consultant/Advisory Board for Alicia Koplowitz Foundation, Editorial Médica Panamericana, and Eli Lilly. She has served in the Speaker's Bureau/has given talks on Continuous Medical Education (not about a product) for Shire. C.A.S., has received research funds for his department (non-personal) from Caja Navarra Foundation (CAN), Eli Lilly, Lundbeck, Shire, and TEVA. He has served as Consultant/Advisory Board for: Alicia Koplowitz Foundation, Editorial Médica Panamericana, Eli Lilly, EUNETHYDIS (European Network on Hyperkinetic Disorder), Instituto de Salud Carlos III (FIS), NeuroTech Solutions Ltd, Spanish Health Ministry Quality Plan (Clinical Practice Guidelines on TDAH and Clinical Practice Guidelines on Depression), Rubió, and Shire. He has served in the Speaker's Bureau/has given talks on Continuous Medical Education (not about a product) for Eli Lilly, Shire, Universidad Internacional Menéndez Pelayo, and Universidad Internacional de La Rioja (UNIR). He has received Royalties from DOYMA, Editorial Médica Panamericana, EUNSA, and Mayo Ediciones.
Footnotes
Acknowledgment
The authors would like to thank Marta García-Granero for her statistical advice.