
Abstract
Objectives:
To identify mood symptoms that distinguishes bipolar disorder (BP) depression versus unipolar depression in youth during an acute depressive episode.
Methods:
Youth with BP (N = 30) were compared with youth with unipolar depression (N = 59) during an acute depressive episode using the depression and mania items derived from the Schedule for Affective Disorders and Schizophrenia for Children (K-SADS)-Present Version. The results were adjusted for multiple comparisons, and any significant between-group differences in demographic, nonmood comorbid disorders, and psychiatric family history.
Results:
In comparison with unipolar depressed youth, BP depressed youth had significantly higher scores in several depressive symptoms and all subsyndromal manic symptoms, with the exception of increased goal-directed activity. Among the depressive symptoms, higher ratings of nonsuicidal physical self-injurious acts and mood reactivity, and lower ratings of aches/pains, were the symptoms that best discriminated BP from unipolar depressed youth. Subsyndromal manic symptoms, particularly motor hyperactivity, distractibility, and pressured speech, were higher in BP depressed youth and discriminated BP depressed from unipolar depressed youth.
Conclusions:
The results of this study suggest that it is possible to differentiate BP depression from unipolar depression based on depressive symptoms, and in particular subsyndromal manic symptoms. If replicated, these results have important clinical and research implications.
Introduction
B
In general, about 20% of youth develop impairing unipolar depression that substantially increases the risk for suicidality and hampers their normal development (Brent and Birmaher 2006; Jonsson et al. 2011; Wilkinson et al. 2011). Most depressions are diagnosed as major depressive disorder (referred to in this study as unipolar depression), but they also are ubiquitous in youth with BP (Birmaher et al. 2009; Hirschfeld 2014). The differential diagnosis between these two subtypes of depression has important clinical and research implications (Birmaher et al. 2009; Hirschfeld 2014). For example, monotherapy with antidepressants is indicated for the treatment of unipolar depression, but they may exacerbate or induce mania or mixed episodes in BP depression (Diler and Birmaher 2012; Inoue et al. 2015). The presence of past episodes of hypo/mania helps to confirm the diagnosis of BP, but depressive episodes are usually the first and the most common manifestation of BP in youth (Chang 2009). Moreover, it may be difficult to recollect prior mild hypo/manic episodes (Chang 2009), and these episodes may be confused with regular adolescent behaviors (Axelson et al. 2006).
Few studies in youth have investigated whether the symptoms of unipolar and BP depression differ (Uchida et al. 2015). In comparison with unipolar depressed youth, BP depressed youth appear to have more severe depression with suicidality, anhedonia, and hopelessness, and higher rates of comorbidities (e.g., disruptive behavior, anxiety, and substance use disorders) (Wozniak et al. 2004). Also, compared with youth with other depressive disorders, including unipolar depression, BP depressed youth show higher levels of impairment and higher rates of suicidal behavior (60% vs. 30%) (Karlsson et al. 2007).
Studies in adults (DePue and Monroe 1978; Benazzi 2000; Bowden 2005; Angst et al. 2010; Hoertel et al. 2012; APA 2013; Inoue et al. 2015; Leonpacher et al. 2015; Perugi et al. 2015) suggest that atypical depressive symptoms (e.g., increased appetite/sleep, psychomotor retardation, mood reactivity) and subsyndromal manic symptoms are more common in BP depression. However, the results are inconsistent, and the studies have methodological limitations (e.g., not controlling for multiple comparisons or significant between-group differences in demographic and nonmood comorbid disorders) (Cuellar et al. 2005). There are no studies of the prevalence of subsyndromal manic symptoms in BP depressed versus unipolar depressed youth (Shon et al. 2014; Uchida et al. 2015), but a recent study showed that depressed youth with subsyndromal manic symptoms were less responsive to antidepressants than depressed youth without these symptoms (Maalouf et al. 2012).
Given the above information and the scarcity of studies, we aimed to characterize differences in mood symptomatology of an acute depressive episode in depressed BP and unipolar depressed youth. We hypothesized that mood symptomatology will distinguish BP depressed youth with more severe and atypical depressive symptoms and subsyndromal manic symptoms.
Methods
This study included BP youth who were experiencing a current major depressive episode from the Course and Outcome of Bipolar Youth (COBY) (Birmaher et al. 2009) study and unipolar depressed youth from the Neurobehavioral Changes in Pediatric Affective Disorder (NCPAD) (Ryan et al. 1987) study. Mixed episodes in BP youth as described in the Diagnostic and Statistical Manual (DSM)-IV were not included in this study (APA 2004). As noted below, both studies used similar methodology and included the same investigators.
After institutional review board approval, consent/assent was obtained from the parents/children. In COBY, current and past psychopathology was ascertained using the Schedule for Affective Disorders and Schizophrenia for School-Age Children K-SADS-Lifetime Version (K-SADS-PL) (Kaufman et al. 1997). In addition, since the K-SADS-PL only documents the presence/absence of each symptom, the severity of depressive and manic symptoms was evaluated using the Depression Rating Scale (DRS) (Kaufman et al. 1997) and the Mania Rating Scale (MRS) (Axelson et al. 2003), respectively. The DRS and MRS are derived from their respective sections in the original K-SADS (K-SADS-Present version) (Kaufman et al. 1997). In NCPAD, current psychopathology was ascertained through the K-SADS-Present version, including MRS and DRS, and past psychopathology using the K-SADS-Epidemiologic version (K-SADS-E) (Kaufman et al. 1997). In both studies, socioeconomic status was ascertained using the Hollingshead scale (Hollingshead 1975). All diagnoses were done according to the DSM-IV diagnostic criteria (APA 2004). Family psychiatric history was ascertained using the Family History-Research Diagnostic Criteria method (Andreasen et al. 1977) and the Family History Screen (Weissman et al. 2000).
As per the K-SADS instructions, mood symptoms that were also common with other psychiatric disorders (e.g., hyperactivity) were not rated as present in the mood sections unless they intensified with the onset of abnormal mood. Comorbid diagnoses were not assigned if they occurred exclusively during a mood episode. In COBY, an operationalized definition of BP-not otherwise specified (BP-NOS) was used to diagnose children who did not meet the DSM-IV criteria for BP-I or BP-II, but had distinct periods of abnormally elevated, expansive, or irritable mood (Axelson et al. 2006; Birmaher et al. 2006). We have previously shown that youth meeting these more strictly defined BP-NOS criteria have similar, but less severe, mood symptoms and similar rates of comorbid disorders, family history of mood disorders, and longitudinal course and outcome as the BP-I youth (Axelson et al. 2003). Moreover, about 45% convert into BP-I and BP-II during the 4-year follow-up (Axelson et al. 2011). For the purpose of this study, we excluded those six unipolar depressed youths in the NCPAD study who developed BP during the 12-year follow-up.
For this study, we only included youth with an “acute major depressive episode” during the intake assessment of the COBY and NCPAD studies. The DRS (total score range 0–61) ascertained the current depressive symptoms covering the past month (focusing on the most severe week) before the intake assessment. Manic symptoms identified during the same current depressive episode were evaluated using the MRS (total score range 0–63). Both scales include scores from 1 to 6, where 1 indicates absence of mood symptoms, 2 and 3 indicate subthreshold symptoms (mild and moderate severity), and 4 and higher indicate severe mood symptomatology. In accordance with the DSM-IV, atypical features were identified using K-SADS-P as mood reactivity, and two of the following depressive symptoms: increased appetite/weight gain, hypersomnia, leaden paralysis/psychomotor retardation, and rejection sensitivity/social withdrawal (APA 2004). Melancholic features were identified as presence of either loss of pleasure or not reacting to pleasant events, plus three or more of the following depressive symptoms: distinctly depressed mood, worse depression in the mornings, awakening at least 2 hours earlier than normal, significant physical slowing/agitation, significant anorexia/weight loss, and excessive guilt (APA 2004).
As described in detail elsewhere (Ryan et al. 1987; Birmaher et al. 2009), all assessments were performed by well-trained bachelors- or masters-level interviewers. The results of each interview were reviewed by a child psychiatrist or psychologist for diagnostic consensus. The overall K-SADS kappas for psychiatric disorders in both studies were ≥0.8 (Ryan et al. 1987; Birmaher et al. 2009).
Statistical analysis
Parametric and nonparametric statistics were used as appropriate to analyze between-group differences in demographic and clinical characteristics. For the analyses of mood symptoms, we first compared the mean depression and mania scores on DRS and on MRS, respectively, between depressed BP and unipolar depressed youth. Because the DRS and MRS scores were non-normally distributed (which proved irremediable by variable transformations), nonparametric Wilcoxon signed-rank tests were used to compare the two groups on symptom severity. False discovery rate-adjusted p-values were then computed to control for multiple comparisons. Finally, generalized linear models were used to adjust for significant between-group differences in demographics, comorbid disorders, and psychiatric family history (backward-manually selected with retention level = 0.2). Because many mood symptom scores were non-normally distributed, ordinal logistic regression was additionally considered to compare the two groups' symptom scores while controlling for significant confounders. However, since most models failed the proportional odds assumption, binary logistic models were implemented dichotomizing depressive symptoms at the threshold level (scores ≥4), and manic symptoms at the subthreshold level (scores ≥2). These results were similarly adjusted for significant between-group differences in demographics, comorbid disorders, and psychiatric family history. Issues of low outcome prevalence in logistic models were remedied using the Firth's penalized likelihood approach (Firth 1993). Summary measures, such as sum of depressive symptoms and sum of manic symptoms by youth, as well as percent of youth with atypical depressive (and melancholic) features, were also analyzed using linear, Poisson, and logistic regressions, respectively.
The probability that a high score on that particular mood symptom would successfully classify the youth as depressed BP versus unipolar depressed (when randomly selected from a sample of depressed youth) was analyzed using univariate logistic regression and c-statistics. The probability of 0.5 indicates random chance, a value of 1.0 indicates perfect prediction, scores >0.6 generally indicate moderate range, and >0.7 good range (Swets 1988; Zou et al. 2007).
Finally, we analyzed Spearman correlations between depressive and manic symptoms across the full sample, and then marginally within each sample to explore associations between subsyndromal manic symptoms and safety risk (suicidal ideation and nonsuicidal self-injurious acts). Statistical tests were evaluated at the 0.05 level of significance.
Results
Thirty depressed BP youth (15 with BP-I, 9 BP-II, and 6 BP-NOS) and 59 unipolar depressed youth were included in this study. BP depressed youth were significantly older than unipolar depressed youth (15.4 ± 3.7 years old vs. 11.8 ± 2.0 years old). There were no significant between-group differences in sex, race, socioeconomic status, and age of onset for mood disorders (Table 1).
Significant differences with p < 0.05 are indicated in bold.
ADHD, attention-deficit/hyperactivity disorder; DBD, disruptive behavioral disorders (i.e., oppositional defiant disorder or conduct disorder); SES, socioeconomic status; SUD, substance use disorders; SD, standard deviation.
Depressed BP youth showed higher rates of psychotic symptoms (40% vs. 8.6%), and more comorbid Axis-I diagnosis (96.7% vs. 51.7%), attention-deficit/hyperactivity disorder (ADHD) (53.3% vs. 10.3%), disruptive behavior disorders (DBD; comprised oppositional defiant disorder and conduct disorder) (43.3% vs. 22.4%), and anxiety disorders (63.3% vs. 25.9%) than unipolar depressed youth (p ≤ 0.05) (Table 1). Also, depressed BP youth had significantly more first- and second-degree relatives with mania compared with unipolar depressed youth (50% vs. 17%; p = 0.002). There were no between-group differences in the first- and second-degree relatives for other psychiatric disorders and history of suicide attempts (p > 0.2).
Depressive symptoms
Compared with unipolar depressed youth, BP depressed youth had significantly higher mean scores of mood reactivity, hopelessness, social withdrawal, craving for sweets, and nonsuicidal physical self-injurious acts, and significantly less aches/pains (all Wilcoxon p ≤ 0.04) (Table 2). Adjusting for significant confounders (e.g., age, and comorbid anxiety, psychosis, hyperactivity, and DBD in youth) showed that BP depressed youth were significantly more likely to have higher percentages of moderate to extreme mood reactivity, social withdrawal, daytime sleepiness, hypersomnia, anorexia, and nonsuicidal physical self-injurious acts, but were significantly less likely to have irritability and aches/pains compared with unipolar depressed youth. Except for (the mean scores of) hopelessness, social withdrawal, and craving for sweets, and (percentage of youth with) hypersomnia and anorexia, the above results remained significant after controlling for multiple comparisons.
Depressive symptoms were recorded on the depression rating scale derived from the K-SADS-P (Kaufman et al. 1997). Unipolar depression = major depressive disorder. Significant differences (p < 0.05) are indicated in bold. Results for linear models were covariate adjusted (e.g., older age, and higher rates of comorbid anxiety, psychosis, hyperactivity, and disruptive behavior disorders in youth with bipolar disorder).
Significant p-values after FDR adjustment.
FDR, false discovery rate; SD, standard deviation.
There was no between-group difference in DRS scores in the percentage of youth with melancholic features (33.3% vs. 30.5%, p = 0.8) and atypical features (60% vs. 40.9%, p = 0.09). Overall, the mean number of moderate to severe depressive symptoms was higher in BP depressed youth compared with unipolar depressed youth (10.2 ± 5.2 vs. 7.8 ± 4.1; F = 5.97, p = 0.02), but this effect fell to marginally nonsignificant after adjusting for confounders (F = 3.55, p = 0.06).
As shown in Table 2, diurnal mood variation, hopelessness, anhedonia, fatigue, psychomotor agitation, social withdrawal, daytime sleepiness, strong craving for sweets, and lethality of suicidal acts discriminated between BP and unipolar depressed youth moderately well (c-statistics = 0.60–0.68). Higher mood reactivity, nonsuicidal physical self-injurious acts, and lower aches/pains discriminated very well (c-statistics = 0.74–0.75) (Fig. 1). After repeating these analyses with the addition of family history as a covariate, the same set of depressive symptoms emerged as the strongest at discriminating between BP and unipolar depressed youth.
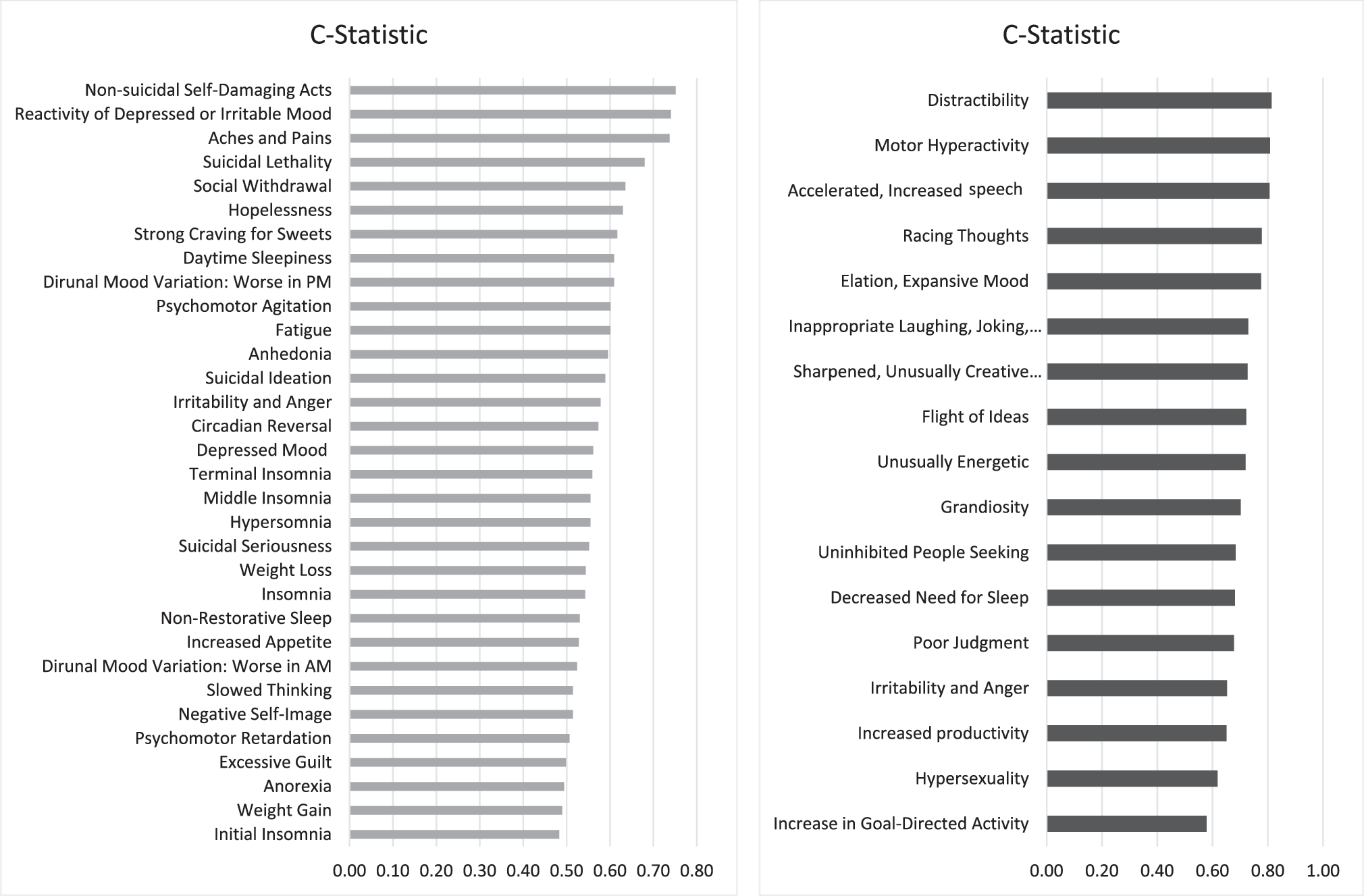
Prediction (C-statistic) values for depressive and subsyndromal manic symptoms in depressed youth to differentiate bipolar disorder (BP) depression from unipolar depression.
Subsyndromal manic symptoms
Compared with unipolar depressed youth, depressed BP youth had significantly more severe (e.g., higher mean scores) subsyndromal manic symptoms (except for increased goal-directed activity), including elation, grandiosity, decreased need for sleep, pressured speech, racing thoughts, flight of ideas, distractibility, motor hyperactivity, poor judgment, unusually energetic symptoms, inappropriate laughing, gregariousness, increased productivity, sharpened/creative thinking, and hypersexuality, and had significantly less severe irritability/anger (all p ≤ 0.02) (Table 3). Adjusting for significant confounders (e.g., age, and comorbid anxiety, psychosis, hyperactivity, and DBD in youth) showed that BP depressed youth were significantly more likely to have (i.e., higher percentages) all of the subsyndromal manic symptoms compared with unipolar depressed youth. Adjusting for multiple comparisons showed similar results. The mean number of subsyndromal manic symptoms was higher in depressed BP youth compared with unipolar depressed youth (8.4 ± 5.1 vs. 1.7 ± 2.5; χ2 = 80.97, p < 0.0001). As shown in Table 3, higher scores of decreased need for sleep, poor judgment, gregariousness, increased productivity, and hypersexuality, and lower scores of irritability, significantly discriminated moderately well between BP and unipolar depressed youth (c-statistics = 0.62–0.68). Moreover, higher scores of elation, grandiosity, pressured speech, racing thoughts, flight of ideas, distractibility, motor hyperactivity, unusually energetic symptoms, inappropriate laughing, and sharpened/creative thinking discriminated very well between BP and unipolar depressed youth (c-statistics = 0.70–0.81). After repeating these analyses with the addition of family history as a covariate, the same set of subsyndromal manic symptoms emerged as the strongest at discriminating between BP and unipolar depressed youth.
Manic symptoms were recorded on the MRS (Axelson et al. 2003) derived from the K-SADS-P (Kaufman et al. 1997). K-SADS-MRS also measures psychotic symptoms. Unipolar depression = major depressive disorder. Significant differences (p < 0.05) are indicated in bold. Results for linear models were covariate adjusted (e.g., older age, and higher rates of comorbid anxiety, psychosis, hyperactivity, and disruptive behavior disorders in youth with bipolar disorder).
Significant p-values after FDR adjustment.
FDR, false discovery rate; MRS, mania rating scale; SD, standard deviation.
Taking into account that the sample of depressed BP youth was relatively small, we did not find significant differences in depressive and subsyndromal manic symptoms between subtypes of BP (BP-I [50%] vs. BP-II [30%] vs. BP-NOS [20%]). Also, our results did not change when we controlled for differences in exposure to pharmacological treatment. Adjusting for higher rates of mania and ADHD in parents of BP youth did not change the results.
In our exploratory analyses between subsyndromal manic symptoms and safety risks, nonsuicidal self-injurious acts were positively correlated with elation, grandiosity, decreased need for sleep, racing thoughts, motor hyperactivity, inappropriate laughing, and sharpened/creative thinking across the full sample (rp = 0.43–0.52, p < 0.0006). Among unipolar depressed youth, suicidal ideation was positively correlated with elated mood and unusually energetic symptoms, and nonsuicidal self-injurious acts were positively correlated with grandiosity, decreased need for sleep, racing thoughts, and hypersexuality (rp = 0.40–0.77, p < 0.02).
Discussion
In this study, we investigated whether it is possible to differentiate between BP and unipolar depression based on the mood symptomatology presented during an acute depressive episode. As hypothesized, our results showed that depressed BP youth have distinct depressive symptomatology (e.g., higher nonsuicidal physical self-injurious acts, mood reactivity, and lower aches/pains), and more subsyndromal manic symptoms, compared with unipolar depressed youth. These differences remained significant after adjusting for multiple comparisons and between-group significant differences in parents and youth clinical and demographic variables. Among all mood symptoms, more motor hyperactivity, distractibility, pressured speech, elated mood, racing thoughts, nonsuicidal self-injurious acts, mood reactivity, and lower aches/pains showed the highest probability to differentiate BP depression from unipolar depression. Family history of mania did not improve the prediction values. The above results have important clinical implications because they suggest that careful characterization of the mood symptoms during an acute episode of depression can potentially help improve the identification of BP in youth, especially when a history of hypo/mania is not available.
Before considering the implications of these findings, it is important to discuss the study's limitations. First, the study was carried out in youth who were referred to research studies. Thus, the results may not apply to youth seen in community settings. Second, the results are post hoc analyses of existing studies. Third, unipolar depressed youth were younger than the depressed BP youth. However, after adjusting the results for between-group age and clinical (e.g., ADHD, DBD, anxiety, and psychosis) differences the results remained significant. Fourth, the sample of BP depressed youth was relatively small, limiting analyses between BP subtypes. Fifth, parents' own psychopathology could have influenced their reports about their children's psychopathology (Mick et al. 2003; Youngstrom et al. 2004; Holtmann et al. 2008; Maoz et al. 2014). Nevertheless, controlling for between-group differences in parental psychopathology did not change the results. Sixth, although we excluded those few unipolar depressed youth who developed BP during the follow-up, it is possible that some of them may develop BP in the future.
Given the treatment and prognosis implications, it is critical to differentiate between BP and unipolar depressions (Leonpacher et al. 2015). Although accumulating studies are describing neuroanatomical, neuroendocrinological, and neurophysiological correlates of unipolar depression and BP, no biological markers have yielded results of sufficient sensitivity and specificity to be used as a diagnostic tool to differentiate these disorders (Avci et al. 1997; APA 2013; Diler et al. 2013, 2014). Thus, there is a need for the identification of reliable clinical characteristic features (Shon et al. 2014; Inoue et al. 2015; Leonpacher et al. 2015). In our study, higher rates of mood reactivity and nonsuicidal physical self-injurious acts, and lower rates of aches/pains, were able to differentiate BP depression from unipolar depression, suggesting that clinicians should pay particular attention to these symptoms (Hirschfeld 2014). It is unclear why depressed BP youth showed lower aches/pains in BP than those with unipolar depression, and our findings need replication. In adults, a recent study did not find differences in pain symptoms between these two types of depressions (Ehnvall et al. 2014).
Consistent with studies in adults (Benazzi 1999; Stewart et al. 2010; Xiang et al. 2013) and one chart review in youth (Shon et al. 2014), the presence of atypical depressive features should be carefully assessed in depressed youth. In our study, atypical features were more common in BP than in unipolar depression (60% vs. 40%); however, it fell just short of statistical significance, potentially due to our small sample size. Atypical depressive features may not only herald BP depression (Akiskal and Benazzi 2005) but may also show association with worse course and less treatment response in unipolar depression (Quitkin et al. 1993; Stewart et al. 1993; Akiskal and Benazzi 2005). In addition, there is a recent surge in adult studies to identify appropriate medication intervention by characterizing the depressive symptomatology, including atypical depressive features (Stewart et al. 2010; Uher et al. 2011; Arnow et al. 2015). Thus, all depressed youth would benefit from detailed assessments for characterizing depressive symptomatology, including atypical features that can guide intervention approaches, besides the clinical question to differentiate BP.
It is important to emphasize that BP depressed youth also had more comorbid anxiety and psychosis symptoms compared with those with unipolar depression. Similar to our study, previous studies report that depression with psychosis symptoms showed association with BP rather than unipolar depression (Akiskal 2005; Forty et al. 2008; Xiang et al. 2013; Leonpacher et al. 2015), and increased risk for developing BP (Strober et al. 1993; Geller et al. 2008). In addition, anxiety is also ubiquitous in BP and may increase risk for developing BP in youth (Dickstein et al. 2005; Sala et al. 2012, 2014; Dervic et al. 2015; Hafeman et al. 2016). However, anxiety and psychotic symptoms in this study did not add to the prediction values of BP depression when depressive symptomatology was analyzed. Considering high rates of anxiety and psychotic symptoms in BP depressed youth (Dickstein et al. 2005; Tillman et al. 2008), longitudinal studies are needed in depressed youth to better map the interaction of anxiety and psychosis symptoms on depressive symptomatology, and risk for developing BP.
Little is known about subsyndromal manic symptomatology in depressed youth, and its clinical significance in differential diagnosis between BP and unipolar depression. Similar to the previous studies in adults (Dilsaver et al. 2005; Goldberg et al. 2009), depressed BP youth in this study had several subsyndromal manic symptoms, and most of these symptoms were more common in BP depression compared with unipolar depressed youth. Our results did not differ between subtypes of BP, including those nine youth (15%) with BP-II, but it has been suggested that a number of manic symptoms during depression can differentiate specifically BP-II from unipolar depression in adults (Frankland et al. 2015; Leonpacher et al. 2015). Considering that all subsyndromal manic symptoms (with the exception of goal-directed activity and irritability) were significantly higher in BP depressed youth in our study, clinicians should pay attention to the possibility of BP when one or more subsyndromal manic symptoms are identified during depression.
Increased motor hyperactivity and higher racing thoughts/pressured speech findings of this study in BP depressed youth are consistent with Kraepelin's description (Akiskal and Benazzi 2004) of “excited depression” and “depression with flight of ideas,” to distinguish BP depressive states. “Irritable depression” was described by Benazzi and Akiskal (2005) for BP mixed states in adults. However, to primarily focus on those in depressed state, we excluded youth in mixed states for this study, which could have accounted for the higher irritability in unipolar versus BP depressed youth. It is important to emphasize that irritability was a common symptom in BP depression among other mood symptoms. Future studies with larger samples, including those with and without mixed features, may shed light if irritability can help distinguish BP versus unipolar depressed youth.
Recent studies using categorical (Axelson et al. 2015) and dimensional measures (Hafeman et al. 2016) have suggested that depression with subsyndromal manic presentations increases risk for developing BP in at-risk youth. In one of these studies, the risk for developing BP in offspring of parents whose BP disorders onset early in life was about 50% when mood lability/irritability, depression/anxiety, and subsyndromal manic symptoms were all present (Hafeman et al. 2016), emphasizing the importance of ascertaining these symptoms to identify the presence or emergence of BP during depression. Subsyndromal manic symptoms may also have treatment implications, because depressed youth with these symptoms have poor treatment response to antidepressants (Maalouf et al. 2012). Furthermore, similar to other studies (Goldberg et al. 1998), our main findings and correlation analyses suggested close monitoring of suicidality/nonsuicidal self-injurious behaviors in any depressed youth with subsyndromal manic symptoms.
Conclusion
In conclusion, our results suggest that characterization of depressive symptomatology, particularly subsyndromal manic symptoms, can aid in identification of BP in youth during an acute depressive episode. Screening for the presence of subsyndromal manic symptoms is important for their high specificity for BP, and association with safety risk and poor outcome. If replicated, these results have important clinical and research implications. Future studies should investigate longitudinal trajectories and clinical outcomes of depressive symptoms, and subsyndromal manic symptoms in youth with depression.
Clinical Significance
Our results showed that depressed BP youth have distinct depressive symptomatology (e.g., higher nonsuicidal physical self-injurious acts, mood reactivity, and lower aches/pains), and more subsyndromal manic symptoms, compared with unipolar depressed youth. The depression and mania scales used in this study are available online and include comparative scoring guide (
Footnotes
Acknowledgments
The authors thank the families and their children who participated in this study. The authors also thank Dr. Shelli Avenevoli from NIMH for her support.
Disclosures
COBY data collection began in the year 2000. For the 3-year period before and during this first year (1998–2000), the authors' disclosures are as follows: Dr. Strober has received research support from NIMH and support from the Resnick Endowed Chair in Eating Disorders. Dr. Keller has been a consultant for and/or received honoraria from Pfizer, Inc., Bristol-Myers Squibb, Forest Laboratories/Parke Davis, Wyeth-Ayerst Laboratories, Merck, Inc., Janssen, Eli Lilly, Organon, and Pharmacia/Upjohn; has received grant/research support from NIMH, Wyeth-Ayerst, SmithKline Beecham, Upjohn, Pfizer, Inc., Bristol-Myers Squibb, Merck, Inc., Forest Laboratories, Zeneca, and Organon, Inc.; and has been on the advisory board for Wyeth-Ayerts, Pfizer, Inc., Bristol-Myers Squibb, Eli Lilly, Forest Laboratories/Parke-Davis, Organon, SmithKline Beecham, Merck, Inc., Janssen, Mitsubishi Pharmaceuticals, Zeneca, Scirex, and Otsuka. Dr. Yen has received research support from NIMH. Ms. Gill has received research support from NIMH. Dr. Axelson has received research support from NIMH. Dr. Ryan has received research support from NIMH and served as a consultant to or received funding from SmithKline Beecham, Wyeth-Ayerst, Pfizer, Forest Laboratories, and Lilly. Dr. Hunt has received research support from NIMH and has received honoraria from Wiley Publishers as a senior editor of the Brown University Child and Adolescent Psychopharmacology Update. Ms. Hower has received research support from NIMH. Dr. Hafeman has received research support from NIMH. Dr. Birmaher has received research support from NIMH and received royalties from Random House, Lippincott Williams & Wilkins, and UpToDate.
For the last 3-year period (2013–2016), the authors' disclosures are as follows: Dr. Diler has received research support from NIMH. Dr. Strober has received research support from NIMH and support from the Resnick Endowed Chair in Eating Disorders. Dr. Keller has received research support from NIMH. Dr. Yen has received research support from NIMH. Ms. Gill has received research support from NIMH. Dr. Axelson has received research support from NIMH. Dr. Ryan has received research support from NIMH. Dr. Hunt has received research support from NIMH and has received honoraria from Wiley Publishers as a senior editor of the Brown University Child and Adolescent Psychopharmacology Update. Dr. B. Goldstein has received honoraria from Purdue Pharma. Dr. T. Goldstein has received royalties from Guilford Press. Mr. Merranko has received research support from NIMH. Ms. Hower has received research support from NIMH. Dr. Hafeman has received research support from NIMH. Dr. Birmaher has received research support from NIMH and received royalties from Random House, Lippincott Williams & Wilkins, and UpToDate.