
Abstract
Background:
There are relatively few studies of saccadic eye movements in children with attention-deficit/hyperactivity disorder (ADHD). The aim of this study was to examine inhibitory abilities of eye movements in children with ADHD and to explore the effect of methylphenidate (MPH) on eye movement performance.
Methods:
Thirty-one children with ADHD (mean age 9.9 ± 0.4 years) and 31 sex-, age-, and IQ-matched children with normal development were examined. Saccades elicited not only by the gap, step, overlap, and antisaccade paradigms but also a simple fixation paradigm have been recorded using an eye tracker. The latency of each type of saccade, the error rate of antisaccades, and the number of saccades made during fixation have been measured.
Results:
Children with ADHD and naive to treatment with respect to controls showed significantly shorter mean latency of voluntary saccades (overlap paradigm), more frequent errors during the antisaccade paradigm, and higher number of saccades made during fixation. After 1 month of MPH treatment, all these parameters changed significantly and reached control values.
Conclusion:
Taken together, these results suggest that oculomotor abilities are poor in children with ADHD, which may correlate with deficits in inhibitory mechanisms. Treatment with MPH improves oculomotor performances through adaptive strategies, which may involve brain structures related to cognitive inhibition.
Introduction
A
Saccades are rapid eye movements used to move the fovea of the retina to visual targets for detailed visual exploration. Saccades can be reflexive visually triggered movements or volitional movements. In experimental conditions, one can stimulate the different types of saccades by using different paradigms such as gap, step, overlap, and antisaccade paradigms. Visual fixation plays a pivotal role in retaining focused attention on a target and in inhibiting inappropriate eye movements (Luna et al. 2008). To perform a saccade, several cortical and subcortical areas are activated: the visual information from the retina is sent to the visual cortex, parietal cortex, frontal lobe, and superior colliculus; from there, through the cerebellum and the brain stem, the motor command is sent to the extraocular muscles (Leigh and Zee 2015). Several processes take place during the preparation of saccades, such as shifting visual attention to the new target, disengaging oculomotor fixation, and computing the parameters of the movement (Fischer and Ramsperger 1984; Findlay and Walker 1999).
Generally, the initiation of reflexive saccades involves occipital and parietal cortex, while volitional saccades and suppression of unwanted saccades are under the control of the frontal eye fields (FEFs), located around the intersection of the middle frontal gyrus with the precentral gyrus, consisting of a frontal and parietal portion (Vernet et al. 2014). Burman and Bruce (1997) explored saccade suppression in monkeys and reported that the ventral lateral area of the FEF is responsible for saccade suppression. A recent study by Goto et al. (2010) reported similar deficit in inhibitory capabilities in children with ADHD and in children with frontal lesions.
Several studies investigated eye movement performance in children with ADHD with contrasting results (for a review, see Rommelse et al. 2008). Indeed, latency of saccades has been reported to be longer and more variable in subjects with ADHD compared with controls (Klein et al. 2002; Munoz et al. 2003), but additional studies failed to detect any differences (Karatekin and Asarnow 1998; O'Driscoll et al. 2005; Hanisch et al. 2006). Similarly, the results on antisaccade performance in children with ADHD are discordant, even if most of them report an elevated number of errors in the antisaccade task (Rommelse et al. 2008). A deficit of fixation abilities was hypothesized as one of the core characteristics associated with ADHD (Gould et al. 2001; Feifel et al. 2004).
Methylphenidate (MPH) is a commonly used treatment for ADHD (for a review, see Chan et al. 2016). MPH increases the inhibitory ability of the prefrontal cortex, allowing for improved control of hyperactive and impulsive symptoms. Some authors suggested that the efficacy of MPH in ADHD is also linked to normalization of the activity of basal ganglia and the cerebellum (Czerniak et al. 2013). Recently, Ivanov et al. (2014) reported that a modification of the cerebellar volume correlated with improvement under MPH in ADHD.
The effect of MPH has been investigated on saccadic performances, but the results are quite discordant. Aman et al. (1998) reported no difference in the performance of antisaccades after MPH treatment and Mostofsky et al. (2001) did not report significant improvement either for reflexive or for voluntary saccade performance. In contrast, Klein et al. (2002) reported an improvement after MPH treatment in latency for both reflexive saccade and antisaccade paradigms and a reduction of the number of errors during the antisaccades, suggesting an improvement of voluntary control during treatment. Recently, our group (Bucci et al. 2014) explored postural and eye movement abilities in two independent groups of children with ADHD, with or without MPH. We found a significant difference in saccadic performance in the group of children with ADHD under MPH. However, the children had to perform a dual task, requesting the share of the attention resources.
In the present study, we aim to explore the performance of reflexive and voluntary saccades in children with ADHD naïve to treatment and 1 month after MPH treatment. We hypothesized that oculomotor abilities in children with ADHD would be impaired compared with those of normally developing children, especially for tasks where inhibitor functions are more requested. We hypothesized that MPH would improve oculomotor control, specifically in these more complex saccadic paradigms.
Methods
Participants
Thirty-one children with ADHD (mean age 9.9 ± 0.4 years) and 31 IQ-, sex-, and age-matched normally developing children were enrolled in the study at the Child and Adolescent Psychiatry Department, Robert Debré Hospital (Paris, France). Trained child psychiatrists assessed all the subjects. The diagnosis of ADHD according to Diagnostic and Statistical Manual of Mental Disorders, 5th ed. (DSM-5) criteria (American Psychiatric Association 2013) was carried out using the Kiddie-SADS-EP (Goldman et al. 1998). Psychiatric comorbidities were systematically screened for during the interview. ADHD symptom severity was assessed using the parental report of the ADHD Rating Scale (ADHD-RS). This scale is based on a large collection of normative data and has demonstrated reliability and discriminant validity in children and adolescents (Du Paul et al. 1998; Collett et al. 2003). Children with ADHD were also assessed using the Wechsler scale (Wechsler Intelligence Scale for Children, fourth edition), the Beery-Buktenica Developmental Test of Visual-Motor Integration (VMI, Beery et al. 1997), and the Motor Assessment Battery for Children (MABC) (Henderson and Sugden 1992). Twenty-seven of the ADHD children (mean age 9.8 ± 0.5 years) were also examined 1 month after the introduction of MPH.
Controls were directly interviewed to confirm the absence of ADHD. To be included in our study, controls also needed to have a total score ≤10 on the ADHD-RS (Dickson et al. 2011) and a neurological examination in the normal range. IQ in controls was estimated in two subtests of the Weschler scale, assessing verbal ability (the similarity subtest) and performance ability (matrix reasoning subtest). The scores on these two subtests were not significantly different between the two groups of children. For all children, visual acuity was normal (≥20/20) and neither strabismus nor any oculomotor abnormality was observed. The clinical characteristics of children with ADHD and controls are summarized in Table 1.
ADHD-RS scores after MPH treatment.
ADHD, attention-deficit/hyperactivity disorder; ADHD-RS, ADHD Rating Scale; MPH, methylphenidate.
The investigations adhered to the principles of the Declaration of Helsinki and were approved by our Institutional Human Experimentation Committee (Comité de Protection des Personnes Ile de France V, Hôpital Saint-Antoine). Informed consent was obtained from the participants' parents after the nature of the procedure had been thoroughly explained.
Ocular motor paradigms
Stimuli were presented on a PC screen of 22″; its resolution was 1920 × 1080 and the refresh rate was 60 Hz. Stimuli for saccades were presented on the screen at 22.2°. Three different paradigms were used to stimulate horizontal visually guided saccades (the gap, the step, and the overlap) and one for antisaccades. A simple fixation paradigm was also recorded. Each child had to perform two blocks of these four different types of eye movements. We shall briefly describe each of these paradigms below.
Stimulus was a white-filled circle subtending a visual angle of 0.5°, positioned at the center of the screen for a variable delay comprised between 2000 and 3500 ms. In the gap paradigm (Fig. 1A), after this fixation period, the central target was turned off and a target appeared 200 ms later (gap period) for 1000 ms on the right or on the left side of the screen. The central fixation target then reappeared, signaling the beginning of the next trial.
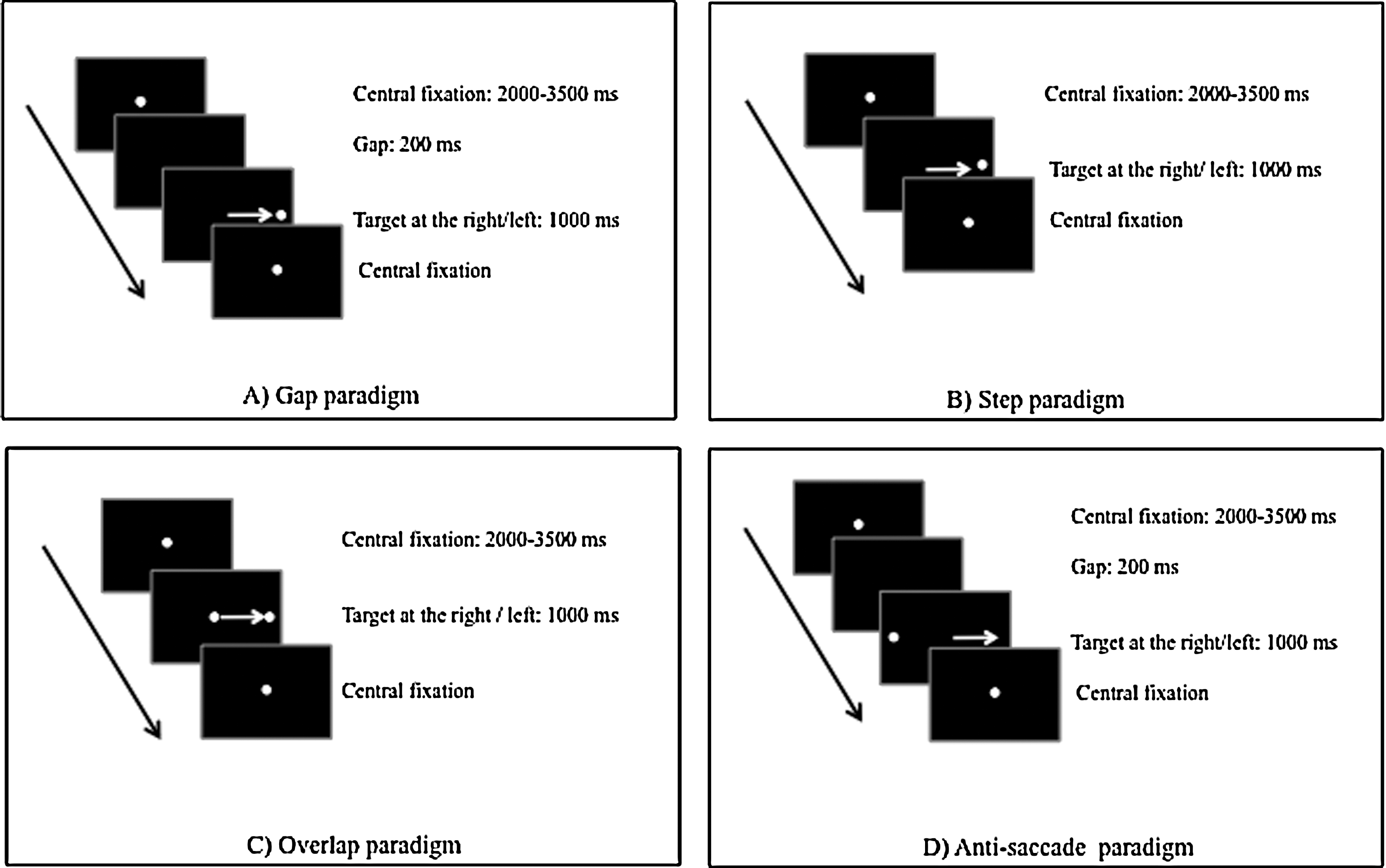
Schematic diagram of the temporal and spatial arrangement used in different paradigms [
In the step paradigm (Fig. 1B), after a variable fixation period comprised between 2000 and 3500 ms, the central target was switched off and a target on the left or on the right side of the screen was simultaneously switched on for 1000 ms. The central fixation target then reappeared, signaling the beginning of the next trial.
The overlap paradigm began similarly (Fig. 1C), with the central fixation point illuminated between 2000 and 3500 ms. In this case, it remained illuminated for 1000 ms and at the same time a target appeared on the right or on the left side of the screen. Thus, during the overlap period, both the central fixation and the target were visible. The target then disappeared and the central fixation point signaled the beginning of the next trial. In each of these three paradigms, the children were instructed to look at the target as rapidly as possible.
To explore antisaccades (Fig. 1D), the paradigm started by a fixation period in which the child was invited to fixate on the fixation target appearing in the center of the screen for a variable delay comprised between 2000 and 3500 ms, followed by its disappearance during a gap interval of 200 ms. Then, a lateral target appeared randomly on the left or on the right of the center and stayed on for 1000 ms. The central fixation target then reappeared, signaling the beginning of the next trial. The children were instructed to look at the central fixation point, then to trigger a saccade as soon as possible in the opposite direction and symmetrically to the lateral target. Thus, when the target appeared on the right, the child had to look to the left, at a distance equivalent to the central point–target distance. When the target returned to the center, the child was instructed to visually follow it back to the center. An initial training block of trials was given to ensure that the instructions were understood.
A Fixation paradigm was also recorded, in which the child was invited to fixate on the fixation target appearing in the center of the screen during a period of 30 seconds.
Eye movement recordings
Eye movements were recorded using the Mobil EBT®, a CE-marked medical eye-tracking device (SuriCog). It benefits from cameras that capture the movements of each eye independently. Recording frequency was set up to 300 Hz. The precision of this system is 0.25°. There is no obstruction of the visual field with this recording system.
Procedure
Each child was seated in a chair in a dark room, his/her head stabilized by a headrest supporting both the forehead and chin. Viewing was binocular; the viewing distance was 60 cm. Calibration was done at the beginning of each block. During the calibration procedure, children were asked to fixate on a grid of 13 points (diameter 0.5°) mapping the screen. Each calibration point required a fixation of 250 ms to be validated. A polynomial function with five parameters was used to fit the calibration data and to determine the visual angles. After the calibration procedure, an ocular motor task was presented to the child. The four different paradigms (gap, step, overlap, antisaccade) to stimulate saccades/antisaccades and fixation paradigm were randomly assigned.
Data analysis
Calibration factors for each eye were determined from the eye positions during the calibration procedure (Bucci and Seassau 2012). MeyeAnalysis® software was used to extract the defining parameters of saccadic eye movements from the data. This software automatically detects both the onset and the offset of each saccade by using a built-in saccade detection algorithm. The investigator manually checked all detected saccades. For each saccade recorded in the four different paradigms, we examined the latency in milliseconds, that is, the time between the onset of the target and the beginning of the eye movements. Furthermore, in the antisaccade paradigm, the mean error rate was also examined. For the fixation paradigm, we counted the number of saccades done during the fixation period. All saccades ≥2° were counted given that it is well known that microsaccades are normally smaller than such amplitude (for details, see Tiadi et al. 2016).
Statistical analysis
An analysis of variance (ANOVA) was performed with groups as intersubject factor and the latency of saccades, the number of errors made in the antisaccade paradigm, and the number of saccades made during the fixation paradigm as within-subject factor. Post hoc comparisons were made with the Fischer's least significant difference test. Individual Student's t-tests were used to compare such values obtained before and 1 month after MPH treatment. The effect of a factor was considered significant when the p-value was below 0.05.
Results
Oculomotor findings in children with ADHD versus normal control children
The ANOVA showed a significant main effect of group on error rate during antisaccade paradigm (Fig. 2A) (F(1,60) = 5.79, p < 0.01). The error rate was significantly higher for children with ADHD compared with controls. Figure 2B shows the number of saccades measured during the fixation paradigm. The ANOVA reported a significant effect of group (F(1,60) = 26.87, p < 0.0001): children with ADHD made significantly more frequent saccades during fixation than controls. Figure 2C shows the mean latency values (for both children with ADHD and controls) for saccades recorded with the different paradigms (gap, step, overlap, and antisaccades). The ANOVA failed to show a significant effect of group (F(1,60) = 2.34, p = 0.13), but showed a significant effect of condition (F(3,180) = 74.05, p < 0.001): latency was significantly longer for voluntary saccades (antisaccades, overlap, and step paradigm, respectively) than for reflexive saccades (gap paradigm) (all p < 0.0001). ANOVA also showed a significant interaction between groups and condition (F(3,180) = 3.58, p < 0.01); post hoc test reported that latency of overlap saccades was significantly shorter for children with ADHD than for controls (p < 0.001).
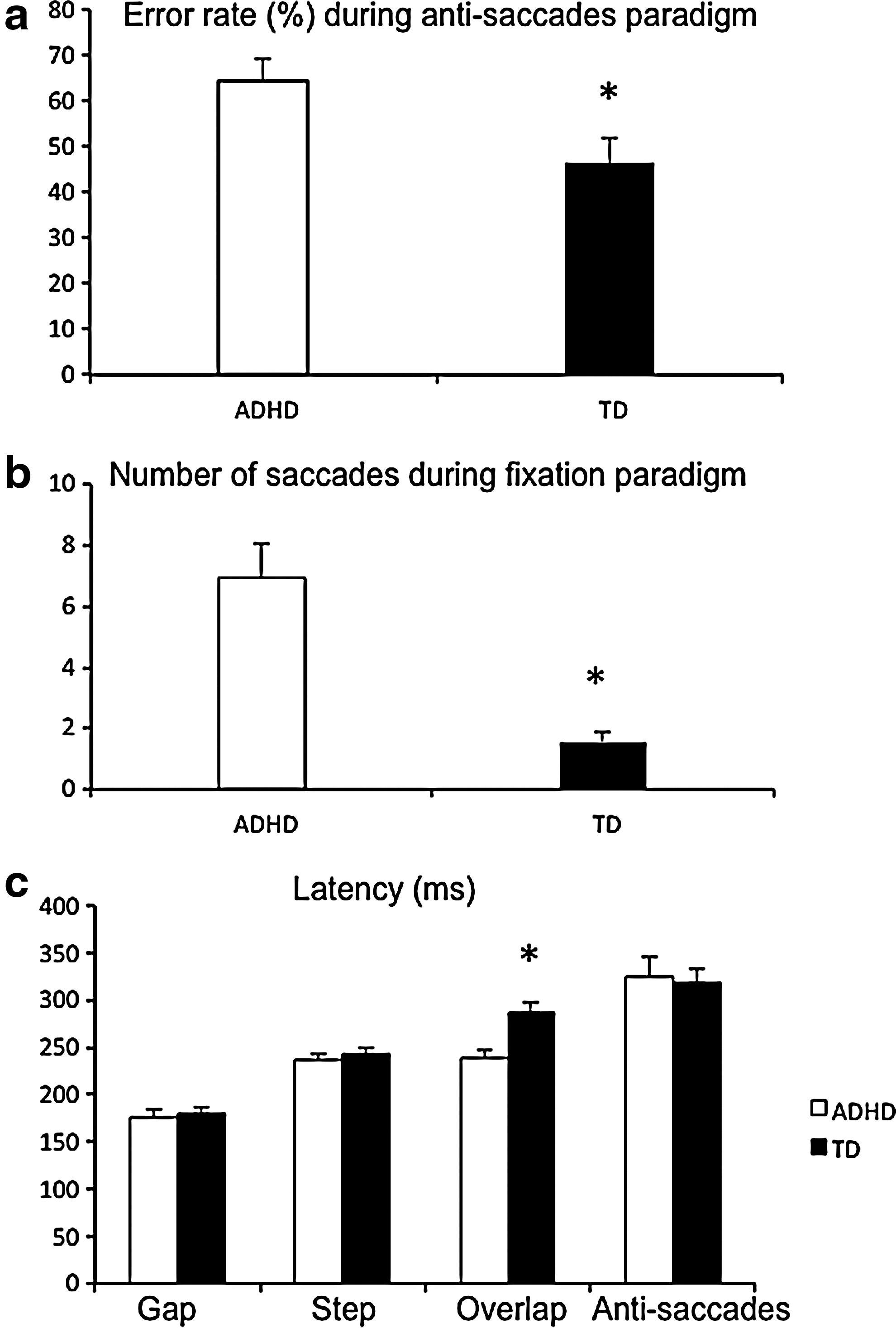
Means of error rate during antisaccade paradigm
Impact of MPH on oculomotor performance in children with ADHD
Figure 3 reports the changes after 4 weeks of treatment with MPH of latency values recorded for the four different paradigms. The t-test revealed that latency for saccades made with the overlap paradigm increased significantly after MPH treatment (p < 0.03). The error rate, which was 64% ± 5% before MPH treatment, decreased significantly to 50% ± 4% after MPH treatment (p < 0.04). Finally, the number of saccades during the fixation paradigm also decreased significantly (p < 0.003) after MPH treatment from 7.3 ± 1.2 to 2 ± 0.5.
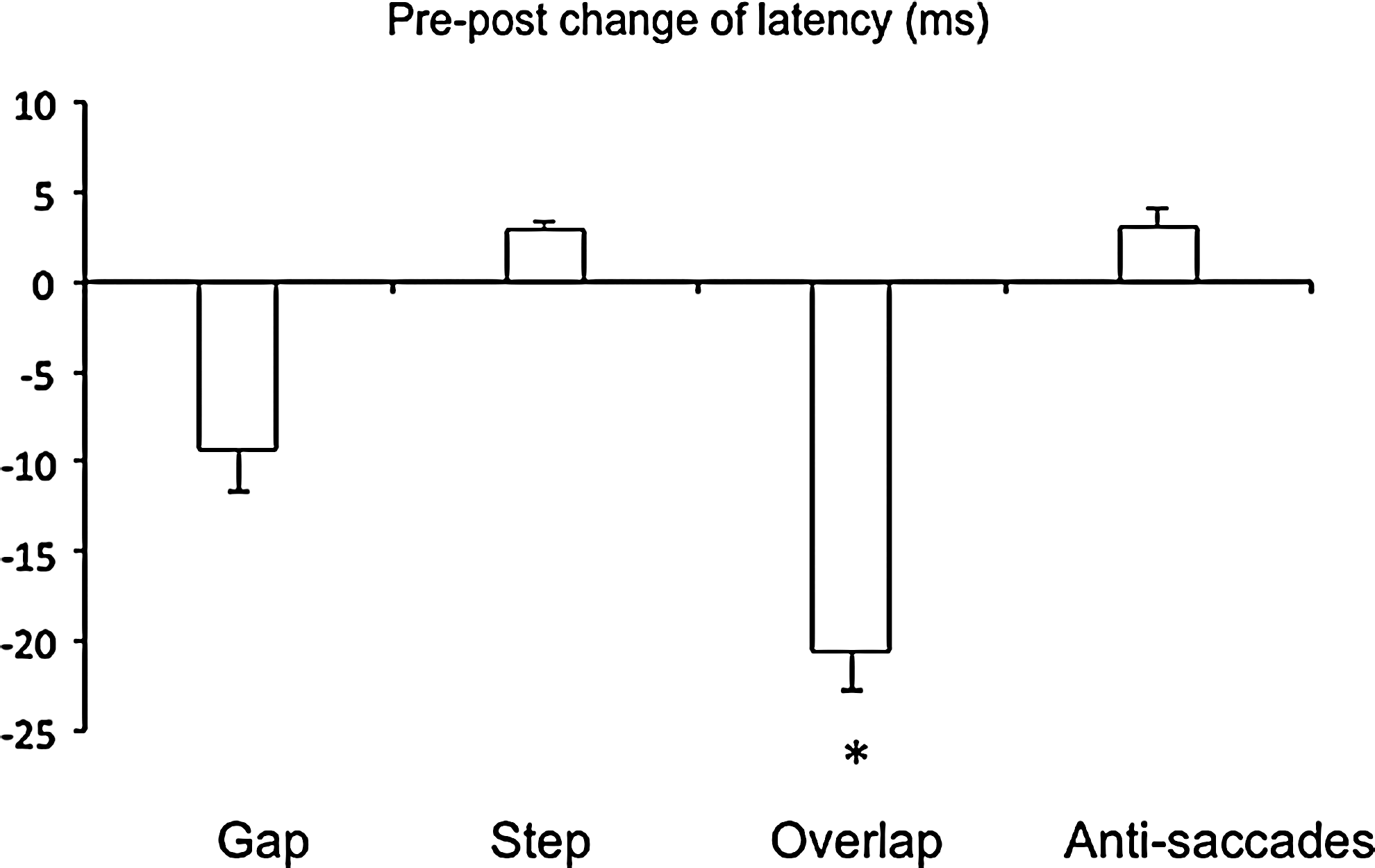
Prepost changes of latency during the gap, step, overlap, and antisaccade paradigms for attention-deficit/hyperactivity disorder children. Vertical bars indicate the standard error. *p < 0.05.
Discussion
In this study, we explored oculomotor performance in ADHD children naïve to treatment and after 1 month of MPH treatment. Based on the exploration of saccades, antisaccades, or during a fixation paradigm, we observed a global decrease of oculomotor ability in children with ADHD, suggesting a deficit in inhibitory control and in executive resources (specifically attention) dedicated to the task. However, after 1 month of treatment with MPH, we observed a significant improvement of the oculomotor control. These findings are discussed below.
Poor oculomotor performance in ADHD children suggests a deficit in inhibitory control and in the recruitment of attention resources
The present study confirms and expands previous findings, showing a deficit in oculomotor control in children with ADHD (ref). Although most studies suggest abnormal latency of saccades, results remain conflicting. In our work, we used three distinct paradigms to explore thoroughly saccades in patients with ADHD. We observed that only the latency of voluntary saccades, elicited by the overlap paradigm, was significantly shorter in children with ADHD with respect to controls. We also reported a high frequency of saccades directed in the wrong direction in the antisaccade paradigm and of saccades made during the fixation task. Associated with the literature, our findings foster the hypothesis of a deficit of inhibitor abilities of the saccadic system linked to a shortfall of the visual attention resources (Rommelse et al. 2008). For instance, during the overlap paradigm, visual attention has to be focused on the central fixation target and then shifted as rapidly as possible toward the lateral target when it appears. This task requires a partial extinction of the attention dedicated to the central fixation target and a move of the executive resources toward the lateral target. Specifically, in children with ADHD, this task is challenging, most likely by their poor inhibitory ability, leading to a difficulty performing saccades in a very rapid way. With respect to the model recently proposed by Matsuo et al. (2015), in which reflexive and volitional signals are acting together before triggering a saccade, we hypothesized that the magnitude of the volitional signal responsible for disengagement from the central fixation point and preparation of the saccade toward the peripheral target is too high, leading to shorter saccade latency.
The deficit of inhibitory control with ADHD was also suggested by the results we obtained in the antisaccade and fixation paradigms. During an acoustic antisaccade task, the activity in the anterior temporal cortex and in the medio-frontal cortex, in which both are involved in the control of cognitive inhibition, differed significantly in children with ADHD and in controls (Goepel et al. 2011). Similarly, the reduced performance at motor response inhibitory tasks in children with ADHD is correlated with the activity of the prefrontal cortex and in the anterior cingulate gyrus (Rubia et al. 2001, 2014; Durston et al. 2003). In children and adolescents with normal development, the inhibitory ability develops in parallel to the maturation of the brain (Luna and Sweeney 2004). Thus, a dysmaturity of the regions involved in inhibitory mechanisms in children with ADHD may be a central pivot of the deficits we reported (Rubia 2007). Causative factors relative to a functional brain maturation delay remain unknown, but altered white matter microstructure in children with ADHD has been consistently reported (Silk et al. 2009; Nagel et al. 2011). Susceptibility gene variants may be a risk factor for such abnormalities (Kabukcu Basay et al. 2016).
Improvement of oculomotor abilities after MPH
Oculomotor abilities of patients with ADHD were significantly improved after MPH treatment. During the overlap paradigm, MPH is associated with an increased latency of volitional saccades. Similarly, during the antisaccade paradigm, we observed a decrease in the direction errors and, during the fixation paradigm, a decrease in the number of saccades made. MPH allows a better saccadic performance and/or a reduction of occurrence of unwanted saccades, probably by an improvement of cognitive inhibitory control. Similarly, adults with ADHD performing an attention task display normal frequency values of microsaccades and blinks after MPH treatment (Fried et al. 2014). These authors suggested that MPH could cause the recovery of normal inhibitory oculomotor control of involuntary eye movements. Several studies (Tannock et al. 1989; Langleben et al. 2006; DeVito et al. 2009) report that MPH improves performance on motor inhibitory tasks. In addition, Rubia et al. (2011) showed that one single dose of MPH significantly normalized brain activation by enhancing activation of the right inferior prefrontal and premotor cortices as well as the left cerebellum and inferior and middle temporal lobes. In addition, a single dose of 40 mg of MPH in healthy adults leads to an increase in connectivity between the dorsal attention network, the thalamus, and also the left and right frontoparietal structures (Mueller et al. 2014). Specifically in children, further studies taking into account the bias induced by the normal maturation of the brain, and combining oculomotor exploration and fRMI, will be useful to improve our knowledge of brain structures involved in response to MPH in ADHD subjects.
Limitations
This study was conducted on a limited number of patients, and further research on a larger number of ADHD children with different doses of MPH would be useful to improve our understanding. In addition, the way of action of MPH remains quite unclear. It is also not excluded that there might be a slight learning effect of the task 1 month later.
Conclusion
This study allows a better knowledge of motor inhibitory abilities in children with ADHD and highlights their weakness in the recruitment of visual attention resources. MPH treatment improves oculomotor performances, probably by improvement of cognitive inhibitory control, through adaptive strategies involving the cerebello-cortical connectivity.
Our research perspectives include further studies taking into account the bias induced by normal maturation of the brain and combining oculomotor exploration and fRMI in children and adolescents. It would be useful to conduct fMRI studies to explore cortico-cerebellar activity involved in eye movements. It would allow first to highlight differences between control and ADHD children and second to assess the improvement or changes of this activity after treatment with MPH. Such a project will be useful to improve our knowledge of brain structures involved in response to MPH in ADHD patients.
Clinical Significance
• Oculomotor performances are weak in children with ADHD.
• A deficit and/or an immaturity of neural networks involved in inhibitory control may explain the abnormalities of saccades and antisaccades.
• Treatment with MPH improves oculomotor performances through adaptive strategies, which may involve brain structures related to cognitive inhibition.
Footnotes
Acknowledgments
The authors thank the eyeBRAIN society for promoting the study. They thank the children who participated in the study and Maison des Langues, Université Paris Descartes, for revising the English version of the manuscript.
Disclosures
No competing financial interests exist.