
Abstract
Objectives:
Mental illness is often accompanied by poor physical health and shorter life expectancy. Second-generation antipsychotics (SGAs) are suspected of increasing cardiovascular risk, possibly through development of metabolic syndrome (MetS), and the risk of adverse outcome is even higher if obesity or metabolic aberration starts in childhood or adolescence.
Methods:
Drug-naive adolescents were recruited after contact with an outpatient Psychosis Team. Changes relative to baseline in body mass index (BMI), waist circumference (WC), blood pressure (BP), fasting blood glucose (FBG), triglycerides (TG), and high-density lipoprotein (HDL) cholesterol were determined through regular follow-ups.
Results:
The sample included 35 SGA-naive patients aged 7–19 (mean: 15.5) with a diagnosis of psychosis. Over 12 months, the overall rate of MetS changed significantly (from 0% to 20% [p < 0.016]). There was a significant increase in BMI (18.4% [p < 0.001]), WC (14.3% [p < 0.001]), TG (25.2% [p = 0.039]), and FBG (3.6% [p = 0.038]), whereas there was a significant decrease in HDL (−11.5% [p < 0.001]). No significant change was found for BP. Compared with the 2014 Danish references BMI-for-age charts, after 12 months the participants' BMI had increased from 0.5 to 1.57 standard deviation (SD) above the 50th percentile for age and gender (p = 0.0001).
Conclusion:
To our knowledge, this is the first study to include all the aspects of MetS in a sample of drug-naive adolescents followed over the first 12 months after starting SGA treatment. A significant shift in all parameters (except BP) toward MetS was found, presumably due to SGA use. Therefore, these adolescents will need proper follow-up, consisting of not only monitoring but also preventive measures to diminish these effects of SGA use.
Introduction
T
Use of second-generation antipsychotics (SGAs) has been on a steady rise since their introduction, in both Europe and the United States (Vitiello et al. 2009). SGAs have been proven effective for both psychotic disorders, autism spectrum disorders (Vitiello et al. 2009) and attention-deficit/hyperactivity disorder (RADS 2013). In Denmark, SGA use in the age group 0–17 years increased by more than 150% between 2002 and 2011 (SSI 2012).
Almost since their first appearance, SGAs have been suspected of disturbing the metabolic balance of the patients treated. Further, it is well established that a large weight gain in childhood and adolescence often extends into adulthood (Engeland et al. 2004; Deshmukh-Taskar et al. 2006) and may lead to more severe outcomes (Biro and Wien 2010) than if contracted at a later age. In addition, adolescents have been found to be more susceptible than adults to the changes in body mass index (BMI) caused by SGAs. This has held true when compared with both non-naive (Kryzhanovskaya et al. 2012) and naive adults (Roy et al. 2010).
Altogether, this points to a lifelong struggle for adolescents who are treated with SGAs and develop metabolic disturbances as a consequence.
The metabolic syndrome (MetS) is a cluster of risk factors that increase the patients' vulnerability to cardiovascular events and DM 2. This study employs the definition of the MetS of the International Diabetes Federation (IDF 2006). The IDF defines the MetS as central obesity (waist circumference [WC] ≥94 cm for men and ≥80 cm for women), plus two of the following factors: • triglycerides (TG) >1.7 mmol/L • high-density lipoprotein (HDL) cholesterol <1.03 mmol/L in men and <1.29 mmol/L in women • raised systolic blood pressure (BP) ≥130 mmHg or diastolic BP ≥90 mmHg • fasting blood glucose (FBG) >5.6 mmol/L
Drastic weight gain and metabolic side-effects have been observed in adults after SGA treatment, and the first 12 months have been proposed as the “critical period” for the development of cardiovascular risk factors (Perez-Iglesias et al. 2014).
The metabolic effects of SGAs in adults affect several aspects of the MetS definition. Moreover, the effects can become evident quite rapidly, as demonstrated in a study of otherwise physically and mentally healthy adults who were administered olanzapine for 3 days (Albaugh et al. 2011), resulting in HDL cholesterol decreasing by 10%, and TG increasing by 22%.
Further, a comprehensive review by Galling and Correll (2015) found that changes in FBG in children/adolescents occur early with SGA treatment, and that the prevalence of DM 2 is increased eight times compared with normal controls, and 1.5 times compared with psychiatric controls. This highlights the need for using drug-naive participants in studies on the effects of SGA treatment.
Hypertension, the final element of the definition of MetS, has not been widely studied in children/adolescents. However, in one naturalistic cohort study, 26% of the adults treated with SGAs suffered from hypertension (Steylen et al. 2013), and this illustrates the potential harm that SGAs might do after some years of treatment.
In adults receiving SGAs, MetS was present in 32.5% (Mitchell et al. 2011). For adolescents, one of the few studies on the prevalence of MetS in SGA-treated children found it to be 19% (Panagiotopoulos et al. 2012).
The advantage of studying adolescents is that their measurements are most likely taken in conjunction with their first exposure to antipsychotic drugs, which means that their metabolic measurements are not clouded by previous exposure. In addition, as mentioned earlier, changes in adolescents may be different and/or larger than in adults. Studies looking into adolescents, SGAs, and the MetS have, however, mostly been short term (12 weeks or less), or have only studied BMI plus one or two of the components of MetS at the same time.
This article aims at demonstrating weight gain and metabolic side-effects in baseline drug-naive adolescents over the first 12 months of SGA treatment. This is done in a naturalistic setting, consequently with less focus on the types/dosages of SGAs, and with more focus on describing all of the individual features of the MetS, as well as the syndrome as a whole.
Methods
Hypotheses
We hypothesized that there would be a statistically significant increase in BMI, WC, FBG, TG, and BP. A statistically significant decrease was hypothesized for HDL cholesterol. The increase in BMI was hypothesized to be greater than that expected for their age, here represented by the 2014 Danish references BMI-for-age charts.
Design
A 12-month retrospective follow-up cohort study, based on clinical records.
Subjects
All patients referred to the Early Intervention Team at the Unit for Child and Adolescent Psychiatry in Odense, Denmark, between 2011 and 2014 (Fig. 1).
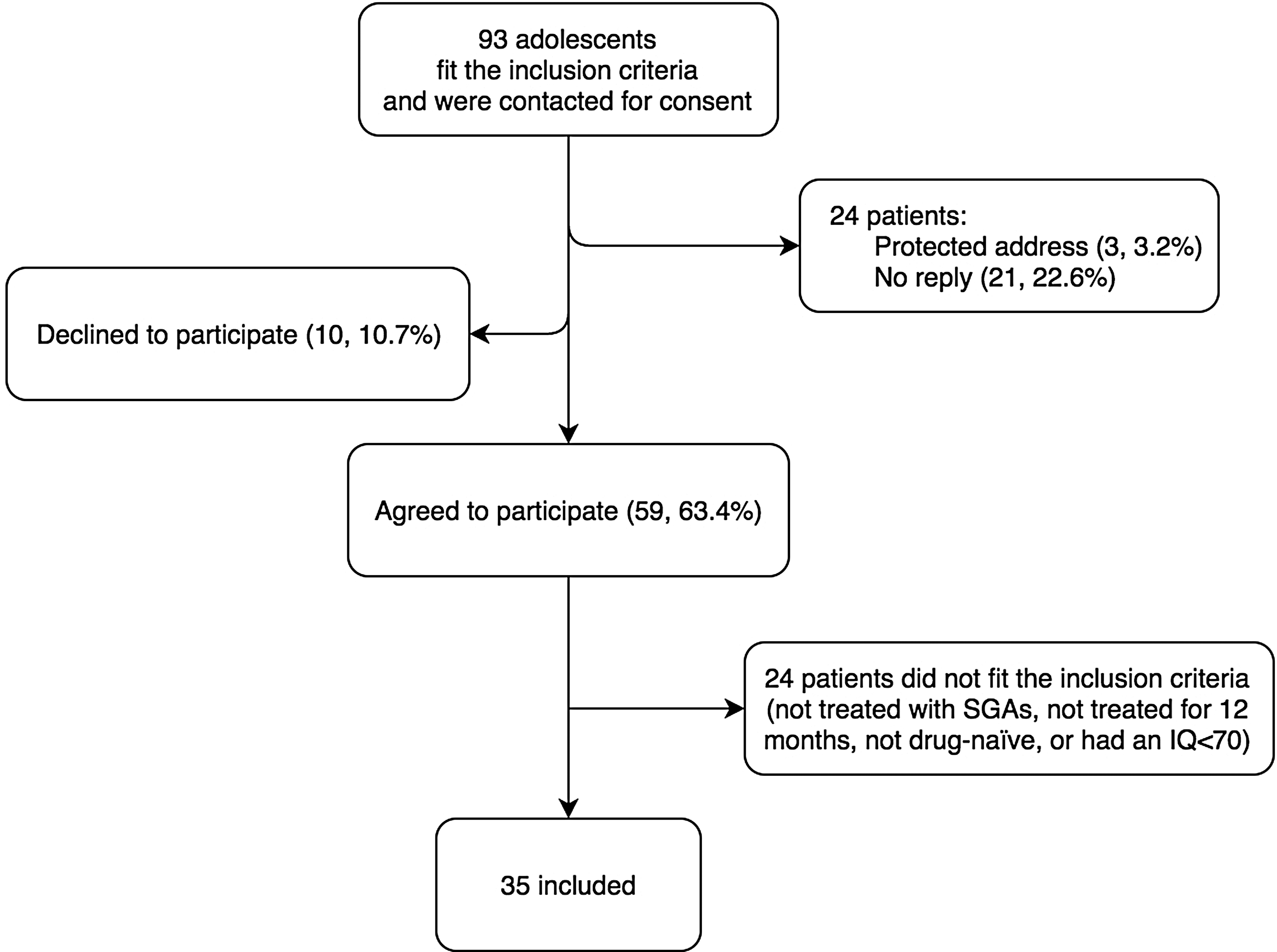
Study population in flowchart.
Inclusion criteria
Less than 20 years of age at the beginning of treatment, a diagnosis of psychosis, and having been treated with SGAs for 12 months or more.
Exclusion criteria
IQ below 70, diagnosis within the autism spectrum, somatic illness affecting metabolism, not drug naive at baseline, or declined to participate.
Measurements
Data were extracted from the patients' medical records.
Clinical and paraclinical variables
Weight, height, WC, and BP were registered in our database at baseline and were followed up over the first 12 months after starting medication. Height and weight were measured by using wall-mounted stadiometers and calibrated scales. Serum lipids and glucose from fasting blood samples were registered in the database from baseline and at every 3rd or 4th month of treatment.
Diagnostic attainment was based on clinical assessment, including Schedule for Affective Disorders and Schizophrenia for School-Aged Children (K-SADS) interview, Positive and Negative Syndrome Scale (PANSS) rating, and psychological testing, all of which were done by trained staff.
Outcome variables
BMI, WC, TG, HDL cholesterol, and FBG were used as both outcome and explanatory variables. This was done to determine whether metabolic status at baseline affected the outcome.
Statistics
To examine the significance of each variable on a group level, a mixed-effects model was fitted in Stata. Time in treatment with SGAs was considered the exposure, with data divided into intervals of 28 days.
Two mixed-effects models were fitted to examine this: one in which only the intercept was random, and one in which both intercept and slope were random. The model with the best fit according to Akaike's information criterion and the Bayesian information criterion was reported (Table 2).
Counted as 13 of the 28-day periods.
BMI, body mass index; CI, confidence interval; DBP, diastolic blood pressure; FBG, fasting blood glucose; HDL, high-density lipoprotein; SBP, systolic blood pressure; SD, standard deviation; TG, triglyceride; WC, waist circumference.
As most variables did not have a perfect normal distribution, the robust variance estimator was used.
The change in the number of patients fulfilling the criteria for MetS before and after treatment was examined by a McNemar test.
To account for expected weight gain due to growth, individual data on BMI were compared with the 2014 Danish references BMI-for-age charts (Tinggaard et al. 2014). BMI data were converted into standard deviations (SDs) from the 50% percentile of the reference material, and they were expressed as the mean difference in SD compared with the reference. A Student t-test was performed to assess the difference between our sample and the reference material.
Stata (Version 14.0; StataCorp) was used for all statistical analyses.
Procedure
Permission to access clinical records and to contact the patients was obtained through consent forms mailed to the patients and/or parents, in accordance with Danish legislation.
Results
From the cohort, 93 patients were eligible for further study, that is, were suspected of suffering from a psychotic disorder, among whom 35 were included (Fig. 1). There were substantially more women (27, 77%) than men (8) (Table 1), even when considering that the eligible cohort consisted of 61% (57) women (only gender was known from the eligible cohort). Sixty-three percent of the patients in the sample were diagnosed with schizophrenia, and 59% received mixed medications (Table 1).
Median age 15.5 years, range 7.3–19.6 years.
After 1 year of treatment.
A combination of quetiapine, aripiprazole, olanzapine, and/or risperidone.
Medication used exclusively for 11 out of 12 months.
ICD-10, International Classification of Diseases, version 10; SD, standard deviation.
Outcome variables
Table 2 presents summary statistics for the baseline and follow-up values of all the outcome variables for the sample. Overall, there was a significant increase in BMI, WC, TG, and FBG, whereas there was a significant decrease in HDL cholesterol. No significant change was found for BP.
The measurements at the beginning of treatment were not significantly correlated with the change in measurements during treatment for any of the outcome variables.
The BMI increase was compared with the 2014 Danish references BMI-for-age charts (Tinggaard et al. 2014). At the beginning of treatment, the patients were on average 0.25 SD (95% confidence interval [CI]: −0.14 to 0.63) above the 50th percentile for age and gender. After 12 months, they were on average 1.57 SD (95% CI: 0.98–2.14) above the 50th percentile for age and gender, with a p-value of 0.0001 (Fig. 2).
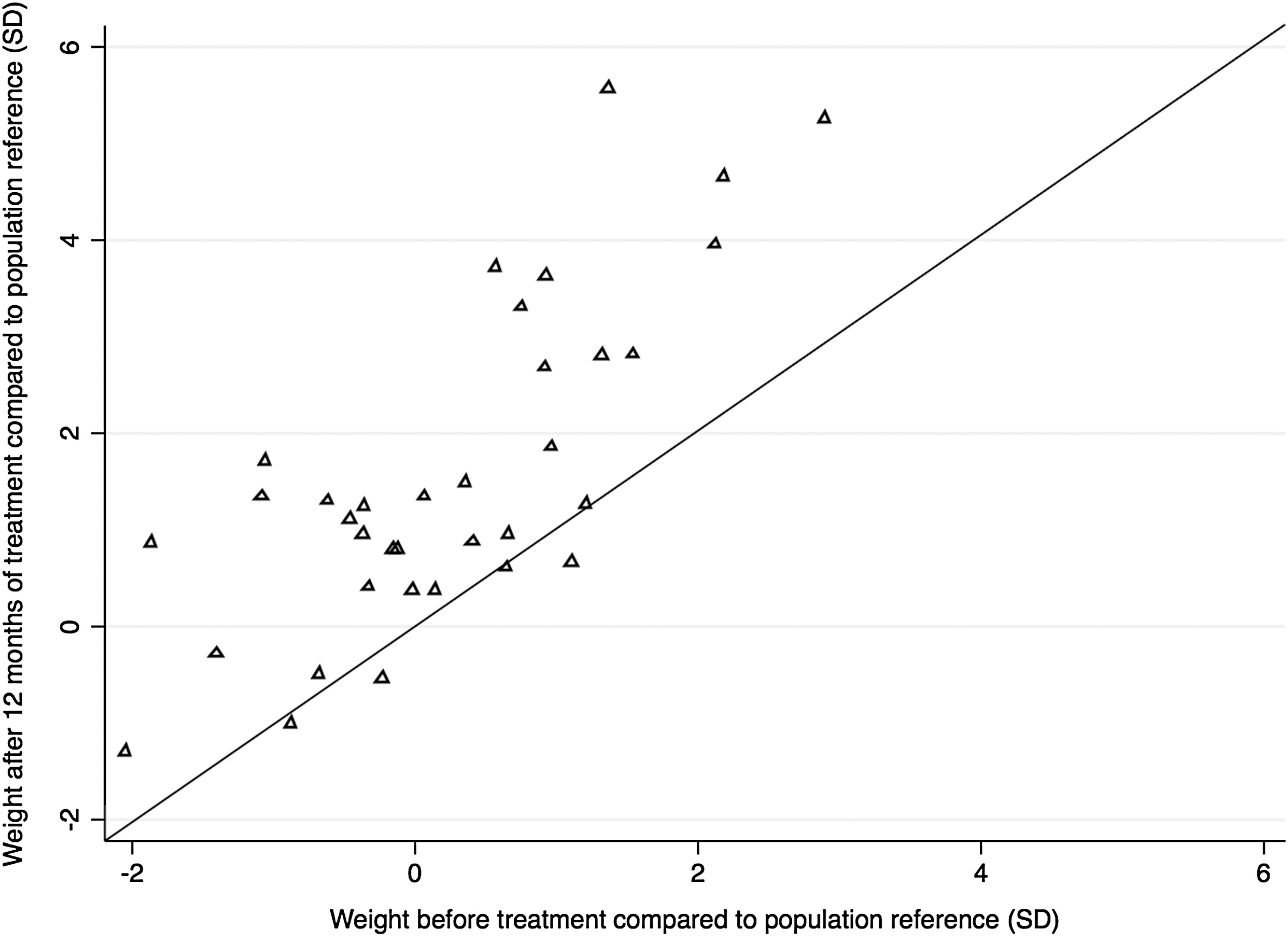
Weight before and after 12 months of SGA treatment, compared with reference for age and gender. Values above the diagonal reference line indicate weight gain from baseline, and values below indicate weight loss. p-Value <0.0001 on the mean weight change from baseline. SGA, second-generation antipsychotic.
MetS before and after 12 months
At the beginning of the study, no patient fulfilled the criteria for MetS; whereas at the end, seven patients did (p < 0.016). Of these, 11 patients met the criteria for elevated FBG, 13 patients had decreased levels of HDL, 7 patients had elevated TG, and 12 patients exceeded the cut-off for WC, according to gender. Eight patients did not have sufficient measurements for their MetS status to be determined, and they were, therefore, excluded from the analyses.
Discussion
The objective of this study was to determine whether SGAs are associated with development of MetS in a population of drug-naive adolescents with a diagnosis of psychosis who were treated with SGAs for 12 months. To our knowledge, this is the first study to examine all of the factors of the MetS in drug-naive adolescents over an extended period.
Overall, there was a significant increase in the presence of MetS, BMI, TG, FBG, and WC, whereas there was a significant decrease in HDL cholesterol. The increase in BMI was also significant when compared with standard growth curves, taking into account normal growth for the age group. No significant change was found for BP.
The SGA medications
The aim of this study is to demonstrate, in a clinical setting, how drug-naive adolescents treated with SGAs are at risk of developing metabolic aberrations. Given this condition, and with such a long follow-up period, most of the patients have been treated with more than one drug and in varying dosage. Many of the patients were treated with, for example, olanzapine for shorter periods in the first acute psychotic phase; later, they were treated for longer periods with, for example, quetiapine or aripiprazole, or with a combination of several SGAs, all the while adjusting dosages. This naturalistic design makes it near impossible to calculate the relative risks of developing MetS according to drugs. But it is also not strictly relevant for the more clinical viewpoint of this study.
The metabolic syndrome
To date, few studies have looked into the development of MetS over time in a similar population. A study by Panagiotopoulos (2012) did, however, find a prevalence of MetS of 19% in children treated with SGAs over a median period of 14 months, which was close to our finding.
Since the first submission of this article for review, the IDF has formulated a new definition regarding MetS in children and adolescents (IDF 2016). In this, adolescents older than 16 years of age follow the adult definition for MetS. Children aged 10–15 years do too, in large part, but the obesity/WC has to be in the 90th percentile for their age. Also, the level of HDL has to be considered a risk of MetS in children, and is set at <1.03 mmol/L for both genders. Children younger than 10 years cannot get the diagnosis, according to this definition.
In our sample, there were 35 patients, 23 of whom were older than 16 years at the end of the study. Of the remaining 12, only 1 was younger than 10 years at the end of the study. The patient who was younger than 10 years did not meet any of the adult criteria for MetS, and, therefore, did not affect the results any more than if we had used this new definition for the analyses. As for the 11 patients between 10 and 15 years of age, the new definition did not matter — the same number of patients met both definitions for MetS. One female patient did not meet the HDL criteria anymore, as they were lowered to the male criteria for those younger than 16 years.
It should also be noted that 2 out of the 15 patients in our sample who had a normal BMI at 12 months actually still fulfilled the criteria for having MetS. This confirms the need for close follow-up—also for patients who do not suffer a dramatic weight gain.
Body mass index
This study found an overall increase in BMI of 18.4%, or 3.8 kg/m2, over the course of 12 months. This finding is somewhat higher than in similar studies. A prospective cohort study of a medication-naive adult population in a 3-year follow-up found that BMI increased significantly (23.2–26.9 kg/m2, equivalent to 16%) over the first 12 months (Perez-Iglesias et al. 2014). Further, a retrospective study by Roy et al. (2010) compared SGA-naive adolescents with adults, and they found a significant increase of BMI in both populations, with increases of 11.8% and 13.1%, respectively, after 6 months. A comparison of SGA-naive adolescents with the background population is important, as it helps to clarify some of the (possibly confounding) variables that are near impossible to control in clinical studies. In the next paragraph, our finding is compared with the background population. In a retrospective cohort study by Ghate et al., adolescents recently initiated on SGAs were likewise compared with untreated adolescents, and they were followed for 395 days. The average percentage increase in BMI in the exposure group at follow-up was significantly different from the controls, showing a 3.7% increase (Ghate et al. 2013). This increase is much lower than what was discovered in our sample, which may be because their comparison group, which consisted of patients matched based on gender and age, was drawn from a U.S. population, in which nearly 1/3 of teenagers are already obese (Ogden et al. 2014).
Increase in BMI, that is, body weight for most of these adolescents, may be the most commonly used parameter for predicting lifestyle diseases in the general population. This is certainly true for our sample, as all of them were weighed regularly; however, only 21 had their WC taken frequently enough to be analyzed. A 4%–18% increase in BMI, depending on the study, over 1 year is usually not health promoting. The definition of MetS for adults does not consider BMI, but if the patients' BMI is more than 30, it can be assumed that their WC meets the criteria. However, BMI is not always a sufficient criterion for MetS (as mentioned earlier) and is more complicated to calculate than, for example, WC.
BMI compared with Danish standard growth curves
When comparing the changes in BMI in our study with the 2014 Danish references BMI-for-age charts (Tinggaard et al. 2014), we found a significant increase, from 0.25 to 1.57 SD, in the patients' BMI relative to the BMI of the background population. However, it should be noted that the patients were on average slightly, yet insignificantly, heavier before beginning treatment with SGAs—0.25 SD over the 50th percentile for age and gender. However, considering that 16 out of the 35 patients were under the 50th percentile at the beginning of treatment, this slight deviation is most likely of no significance.
Waist circumference
We found a mean increase in WC of 14.3%, or 10.8 cm, over the course of 12 months. This statistically significant increase in WC generally corresponds to the previous work of other researchers in this area, although it is one of the more recent elements of the MetS to be considered for study.
WC alone has been found to be a reliable indicator of MetS in both adults (Papanastasiou 2013) and children (Panagiotopoulos et al. 2012). In the latter, a cross-sectional study, WC was found to be 40.7% higher in the SGA-medicated group and 10.1% higher in the SGA-naive children after the treatment period. In comparison with this study, however, the individual duration of SGA treatment varied widely, and about half of the patients were exclusively treated with risperidone. A prospective study of somewhat younger adolescents (11.2 ± 2.7 years) treated with risperidone over the course of 2.9 years found a 12.7% increase in WC (Calarge et al. 2012). In a prospective study of SGA-naive adolescents, abdominal obesity was found to be present in 18% of the patients at the 3-month follow-up (Sadeghye et al. 2014), which was 25% of the time to the final follow-up in our study.
An increased WC is the only mandatory criterion for MetS, and it assesses abdominal obesity. And, as mentioned earlier, MetS can arise even in patients with a normal BMI. Several studies have found WC to increase quickly and significantly while patients are treated with SGAs. The other parameters, however, barring BP, are more invasive and time consuming to measure, whereas WC is a quick, informative, and yet easily overlooked measurement for what might be or become metabolic aberrations.
TG, HDL cholesterol, and FBG
We found a mean increase in TG levels of 25.2%, or 0.286 mmol/L, over the course of 12 months. HDL cholesterol decreased significantly by 11.5%, or 0.16 mmol/L, whereas FBG increased significantly by 3.6%, or 0.19 mmol/L, in the same period.
In a systematic review by Mitchell et al., hypertriglyceridemia in first-episode adult schizophrenia patients was found in 19.6%, low HDL cholesterol in 21.9%, and hyperglycemia in 8.7% of the sample. In the medicated schizophrenia patients, the rates were more than double: 41.1%, 44.7%, and 27.8%, respectively. Similarly, in the 3-year study of adults with first-episode psychosis also mentioned under the Body Mass Index section, a significant increase was found in the number of patients with abnormal TG (22.5%) and HDL cholesterol (23%), but not for FBG (Perez-Iglesias et al. 2014).
In the cross-sectional study by Panagiotopoulos (2012), the prevalence of hypertriglyceridemia in SGA-treated adolescents was 33.7%. The corresponding percentage in our study was lower, 20.0%, and the difference between these findings might be due to the sample and methodological differences mentioned under the Waist Circumference section; that is, differences in diagnoses, time to follow-up, and type of medication.
However, the mean TG level increased by 48% to the time of follow-up in the 7-month cohort study by O'Donoghue et al. (2014), whereas the level of HDL cholesterol did not increase significantly. In other words, the increase in TG was almost double that of our result, and considerably larger than most other studies. Meanwhile, the 6-month retrospective study by Roy et al. (2010) also discussed in the Body Mass Index section, comparing SGA-naive adolescents and adults, only found abnormalities in lipid metabolism in the adult group and found no change for either group regarding the level of FBG. Both of these findings deviate quite substantially from the findings of this study and from those mentioned in the larger of the studies. These discrepancies may be due to sample and methodological differences.
Some even shorter studies have also examined the effect of SGAs on glucose and lipid metabolism. For example, an insignificant increase in both TG and FBG was found in a population of children treated for an average of 6 months (range 3–12 months) (Margari et al. 2013). Likewise, the prospective 3-month study of SGA-naive children and adolescents by Moreno et al. (2010) found insignificant changes in both TG, HDL cholesterol, and FBG. Meanwhile, the 3-month prospective study by Sadeghye et al. (2014) revealed a 6% significant TG increase, and a 7% significant FBG increase in 3 months.
These findings are obviously quite different from those of this study, but the differences might be accounted for by the following sample and methodological differences: All of the three studies mentioned lasted for 3 months only, and between half and all of the patients were exclusively treated with risperidone. Both Margari and Sadeghye had considerably younger sample mean ages than this study (12 ± 3.2 years and 11.67 ± 2.97 years, respectively). Margari's and Moreno's samples only partially consisted of psychotic diagnoses, two thirds and one half, respectively; Sadeghye and others did not report the diagnostic makeup of their sample.
So, although significant abnormalities have been found in lipids and FBG in SGA-naive adult populations, the results for pediatric populations have been more mixed, although usually with at least some insignificant changes pointing in the same direction. That is, although the degree of change varies, TG tends to increase and HDL tends to decrease, whereas FBG does not appear to be as strongly affected in paediatric samples. This might be due to the duration of the studies performed (the former adult trials lasted for at least 1 year), or the changes in glucose metabolism might be slower to develop.
Blood pressure
As for BP, several other studies on children and adolescents have had similar insignificant results as this study (Moreno et al. 2010; Margari et al. 2013; Cote et al. 2014; Sadeghye et al. 2014). It could be argued that more lasting cardiovascular changes will take more than 12 months to develop. In support of this, in a population-based study, Liao et al. (2011) found that younger schizophrenic patients taking SGAs were at a higher risk of developing hypertension later on than the older patients in the sample. Similarly, one retrospective cohort study of adolescents found that the risk of developing cardiovascular conditions over time was 14.2% in the exposure group, and just 3.4% in the control group (Jerrell and McIntyre 2008).
To sum up, hypertension is presumably an aspect of the MetS that, if it does develop due to SGA use, develops later than the other factors.
Methodological considerations
This is the first study to include all aspects of MetS in an adolescent population getting SGA treatment. It is important to look at the syndrome as a whole because it is a known fact that this population is at an increased risk of subsequent heart disease and diabetes, and that having MetS is a risk factor for the same unfortunate outcomes. Examining this population early on to discover how prevalent MetS is may provide us with a better understanding of where this group's ensuing somatic diseases arise from.
A comparison of the development of BMI in our sample with a standardized control group (i.e., the 2014 Danish references BMI-for-age charts) tells us that there is not only a significant increase, which to some extent could be natural during puberty, but also a clear difference between this sample and the background population.
All patients had regular prescriptions written out and were followed up routinely to ensure, admittedly without measuring serum levels, that they took their medication as prescribed over the course of the 12 months.
The baseline and follow-up anthropomorphic measurements were made in different locations in the Region of Southern Denmark, by different people, using different equipment. This could imply biases in the measurements taken. On the other hand, we believe that it strengthens the overall nature of the measurements, removing any systematic errors arising from malfunctioning scales and lack of inter-measurer reliability.
This is a naturalistic study. It involves certain biases, for instance that the patients were not randomized to their medication, and that clinicians were free to change medications during the follow-up period. Certain atypical antipsychotics, notably olanzapine, are known to have more pronounced metabolic effects than other SGAs, and by design this article lacks a demarcation between the effects of the various drugs and their dosages. Also, we had no non-medicated and psychiatrically ill control subjects in the study. Nonetheless, the solid findings of such negative consequences under these conditions imply a very strong relationship between psychosis, SGAs, and the risk of MetS in adolescents, and they may be even stronger than if these results had been found through a randomized controlled trial.
There were only 8 men in this sample of 35 patients, whereas the clinical population in question typically consists of more men than women (McGrath et al. 2008). One study of children (12.6 ± 2.85 years) found that after SGA use, male sex was the strongest predictor of MetS (Panagiotopoulos 2012). In another study of children/adolescents, the risk of developing DM 2 and dyslipidemia was higher in women (Jerrell and McIntyre 2008). A study of adults found hypertriglyceridemia and hypertension to be more frequent in men, whereas central obesity and reduced HDL were more pronounced in women (Fleischhacker et al. 2013).
There may, therefore, be some gender-based differences in metabolic aberrations due to SGA use. This may explain why we did not find changes in BP and only just significantly increased TG, yet a strongly significant decrease in HDL and increase in WC. However, as gender-based differences have not been extensively reviewed in either adolescents or adults, the implications for the present results are as of yet unclear.
The original cohort of eligible patients consisted of 93 patients. However, after the process of selection and consent, only 35 patients, or close to 40%, remained in the study. The sample might not have been large or long-lasting enough to say anything about BP, but it was large enough to discover significant findings on BMI, WC, HDL cholesterol, and fasting blood sugar.
Only 63% of the original cohort proved willing to participate. Possible reasons for non-participation or non-response to invitation could be chronic schizophrenia, obesity, and a reluctance to participate because of it—or it could the opposite: that the healthy and fit patient does not want to be reminded of the disease.
Those patients whose data we could not use, despite a positive response to the invitation, were mainly patients who had not been treated for 12 months, or who had begun SGA treatment with their family doctor. In the latter case, baseline measurements had frequently not been registered, and follow-up was poor or not done at all.
There may also exist a selection bias in this group. Even though it is recommended that all patients being treated with SGAs have their metabolic measurements taken regularly, clinicians may follow up on the patients with obvious weight gain more often than those who are not so noticeably affected. If that is the case, such missing data may skew the results in this article toward a more negative outcome than if all the patients treated had sufficient measurements taken.
Limited research is available on the topic of the metabolic status of people who suffer from schizophrenia but do not take SGAs, as discussed under the Body Mass Index section, compared with the background population. Nonetheless, a genetic link between DM 2 and schizophrenia has been suggested (Lin and Shuldiner 2010) and could possibly add to the effects that we now attribute to the antipsychotic drugs. When the metabolic effects of SGAs versus FGAs are compared, however, SGAs have been found to induce more severe weight gain than FGAs do, and even to have a small increased risk of DM 2 compared with FGAs (Smith et al. 2008). This is a convincing argument for attributing the metabolic abnormalities more to the drug than to the disease. However, the possible link between schizophrenia and DM 2 is not yet fully understood, and there may exist more complex explanations for this relationship than it simply being caused by SGAs.
Conclusion
In conclusion, these results tell us that simply monitoring these adolescents is not enough. Our study demonstrates a clear development toward MetS in the course of SGA use, which may turn into a lifelong suffering, in addition to whichever psychotic disease the patients were originally treated for. If we want to contain this progression, we will need to start thinking about SGAs as drugs that have serious side-effects, and future research should focus more on how to prevent these adverse effects from developing.
Clinical Significance
Our findings support the growing body of evidence that this is a vulnerable patient group in need of a considerably improved support system if they are to have any hope of being given the same standard of supplemental care and treatment that is granted without question to somatic patients.
Disclosures
C.P.S. has received financial support from the private Norwegian charitable foundation “Major and Lawyer Eivind Eckbo's Fund,” and from the Psychiatric Research Fund of the Region of Southern Denmark. She has no financial relationships with any pharmaceutical company. A.D.S. has held lectures for the pharmaceutical firm Otsuka, but has no conflicts of interest or financial ties to disclose. N.B. has lectured at seminars sponsored by Shire and Novartis, but has no conflicts of interest or financial ties to disclose in connection with the present data. All other authors have declared that no competing financial interests exist.