
Abstract
Objective:
Accumulating evidence suggests that anti-inflammatory interventions can modulate neuropsychiatric symptoms. Pediatric Acute-onset Neuropsychiatric Syndrome (PANS) is characterized by an abrupt and dramatic onset of obsessive-compulsive (OC) symptoms and/or severely restrictive food intake and at least two coinciding, equally debilitating neuropsychiatric symptoms. When associated with group A Streptococcus, the syndrome is labeled Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal infections (PANDAS). Here, we describe the course of neuropsychiatric symptoms in patients diagnosed with PANS and PANDAS after introduction or removal of nonsteroidal anti-inflammatory drugs (NSAIDs).
Study Design:
We reviewed the electronic medical records (EMR) of 218 consecutive patients evaluated in our Stanford PANS Clinic for patients who met strict PANS or PANDAS research criteria and received NSAIDs for arthritis, pain, and/or psychiatric symptoms. We describe neuropsychiatric symptoms that were noted in the EMR before, during, and after NSAIDs were introduced or removed as the sole change in pharmacologic treatment.
Results:
Seventy-seven patients were included in the current study. Of the 52 trials in which NSAID addition was the sole change in treatment, 16 (31%) coincided with an improvement in patients' neuropsychiatric symptoms. Of the 57 trials in which removal of NSAID treatment was the sole change in treatment, 20 (35%) coincided with escalation in patients' neuropsychiatric symptoms. Thirty patients (39%) experienced side effects, mainly mild gastrointestinal symptoms, which self-resolved after removal of NSAID, reduction of dose, or change in NSAID.
Conclusions:
Improvement in neuropsychiatric symptoms was evident in roughly one-third of NSAID treatment trials. A randomized clinical trial will be necessary to confirm whether NSAIDs are successful in reducing neuropsychiatric symptoms in youth with PANS.
Introduction
P
The Stanford PANS Program evaluates and treats youth with suspected PANS or PANDAS and conducts research into mechanisms and treatments for this disorder. Psychiatric symptoms can be severely debilitating, and are often accompanied by rheumatologic complaints including arthritis and joint pain that benefit from anti-inflammatory treatment.
Since the PANS clinic's inception in 2012, clinicians have noted a relationship between nonsteroidal anti-inflammatory drug (NSAID) treatment and changes in patients' neuropsychiatric symptoms. To further characterize this observation, we designed this study with the following three aims: (1) to report the course of neuropsychiatric symptoms when NSAIDs are added or removed as the only change in treatment; (2) to provide detailed descriptions of three clinical cases; and (3) to report side effects of NSAIDs in our PANS cohort when change in NSAID treatment is the sole variable.
Methods
We used an electronic navigational query method within our electronic medical record (EMR) to identify all trials of NSAIDs conducted between September 2012 and September 2016 in 218 consecutive patients who meet strict research criteria for PANS. For patients first seen by MT before starting our formal multidisciplinary PANS clinic, written records were reviewed for mention of NSAIDs. All patients received neuropsychiatric and medical evaluations (reported in their EMR) per PANS Evaluation Guidelines (Chang et al. 2015). Data extracted from the medical record include the following: demographic data, course of neuropsychiatric symptoms, medication and psychotherapy trials, and side effects of NSAIDs. NSAIDs used include: naproxen (Naprosyn), ibuprofen (Advil), sulindac (Clinoril), and celecoxib (Celebrex). All medical records were searched using these generic and brand drug names. The Stanford Panel on Human Subjects Institutional Review Board approved this study.
Patient inclusion criteria
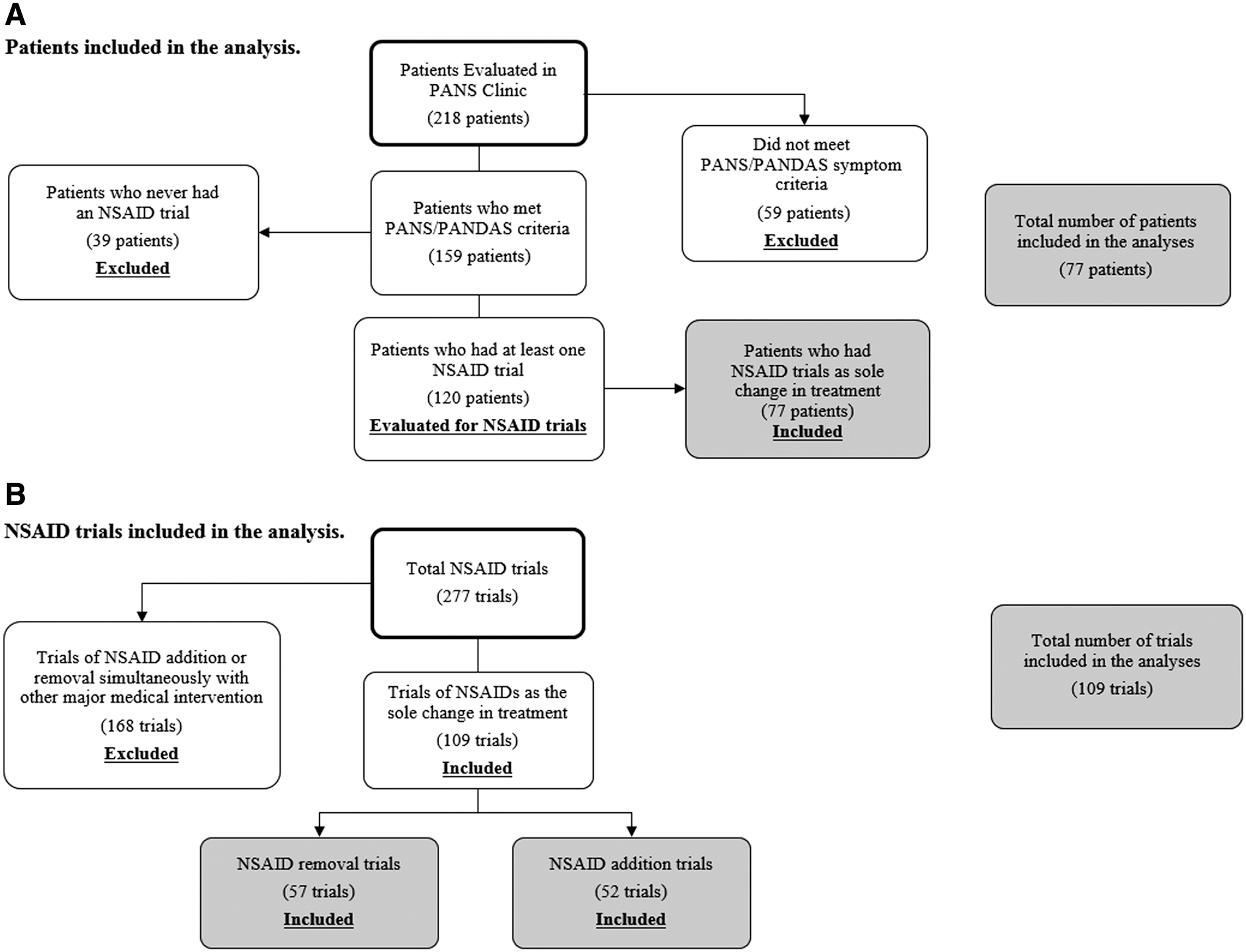
Patients who meet strict research criteria for PANS or PANDAS and who had at least one addition or removal trial of NSAIDs as the sole intervention were included in this case series (Fig. 1A).
Inclusion and exclusion of patients
NSAID treatment protocol
Patients presenting to clinic were first evaluated and treated for any underlying infection according to the PANS Research Consortium consensus statements on the evaluation and treatment of infections (Chang et al. 2015; Cooperstock et al. 2017, submitted). The following doses of NSAIDs were used generally: ibuprofen (10 mg/kg/dose, three times a day, maximum dose: 600 mg/dose), naproxen (10 mg/kg/dose, two times a day, maximum dose: 500 mg/dose), sulindac (2–4 mg/kg/day in two divided doses, maximum: 6 mg/kg/day, maximum dose 400 mg/day), and celecoxib (50–100 mg, two times a day). For PANS patients with decreased fluid intake (as determined by clinical history, high BUN/Creatinine ratio, and/or high specific gravity on urine analyses), NSAID dose was reduced or temporarily suspended until the patient had improved hydration status.
NSAID trial inclusion criteria
NSAID trials were included in this study if NSAID introduction or removal was the only treatment change (Fig. 1B).
Study exclusion criteria
NSAID trials that were initiated at the same time as antibiotics or immune-modulatory therapies (i.e., intravenous immunoglobulin [IVIG] or any corticosteroid) were excluded from the study.
Response to NSAIDs
We evaluated the course of neuropsychiatric symptoms following all NSAID introductions or removals. Response was determined by clinical assessments (documented in the EMR), parent questionnaires, the PANS Global Impairment Scale, and documented communications between parents and providers (follow-up emails and telephone calls). Clear improvement in any of PANS Criterion I or Criterion II neuropsychiatric symptoms (Swedo et al. 2012) was considered to be a positive response to NSAIDs. Response to an NSAID trial was marked unclear if the clinician and/or parent report indicated an unclear response or there was lack of adequate documentation to assess response. Patients who experienced improvement or escalation in neuropsychiatric symptoms following respective NSAID addition or removal were labeled as “responders.” “Nonresponders” are patients who did not experience improvement or escalation in neuropsychiatric symptoms following respective NSAID addition or removal. In Case 1, we include all parent-reported NSAIDs trials; however, analyses only include trials with clear and thorough clinical documentation. When possible, “time to maximum improvement/deterioration after NSAID addition/removal” (Supplementary Tables S1 and S2; Supplementary Data are available online at
Side effects
Side effects of NSAID treatment were noted when they were temporally associated with NSAID treatment.
Results
Of the 218 consecutive children seen at our PANS clinic, 159 met research criteria for PANS during the study period (Fig. 1A). Of these patients, 120 patients (75%) had a total of 277 trials of NSAID addition or removal. Of these, 168 trials (61%) were excluded because the NSAID was started or removed at the same time as another intervention. The remaining 77 consecutive patients (35% of all children seen at our PANS clinic) had 52 NSAID addition trials and 57 removal trials (as the sole change in treatment) and were included in this case series (Fig. 1B). Patients can belong to one or both subgroups. Patient characteristics are described in Table 1.
Patients who had an addition or removal trial of NSAID as the sole change in treatment.
Difference in means assessed using the t-test. Difference in proportions assessed using the chi-square test.
PANS Global Impairment Score and Caregiver Burden Inventory collected at the initial presentation to the Stanford PANS clinic.
Data are missing for some neuropsychiatric symptoms; this is reflected in the denominators of the categorical variables.
Mood dysregulation includes depression and/or emotional lability.
NSAIDs, nonsteroidal anti-inflammatory drugs; PANDAS, Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections; PANS, Pediatric Acute-onset Neuropsychiatric Syndrome.
Response to NSAIDs
Sixteen NSAID addition trials (16/52, 31%) included documentation of improvement in neuropsychiatric symptoms. Improved symptoms included OC symptoms, mood, fatigue, tics, and eating restriction. (Supplementary Table S1). Time to maximum symptom improvement ranged from 6 hours to 20 days. Twenty NSAID removal trials (20/57, 35%) included documentation of escalations in neuropsychiatric symptoms. Worsening symptoms included irritability, aggression, mood, and tics. (Supplementary Table S2). Time to neuropsychiatric deterioration ranged from 30 minutes after first missed dose (for one patient receiving ibuprofen) to one month after NSAID removal. In total, there were 32 responders (42%) and 45 nonresponders (58%) to NSAID trials (Table 2). The uses of cognitive behavioral therapy (CBT) and psychiatric medications were not significantly different between the two groups (p > 0.05). For patients who received CBT or psychiatric medications, the trajectory of psychiatric symptoms was stable before NSAID addition or removal; thus clear and rapid changes in neuropsychiatric symptoms after addition or removal of an NSAID were attributed to the NSAID intervention. Two cases (Case 7 and Case 13) exhibited a mixed response after the addition of NSAIDs, including improvement of some symptoms and worsening of others (Supplementary Table S1). One case (Case 32) exhibited a mixed response after the removal of an NSAID, including improvement of some symptoms and worsening of others (Supplementary Table S2).
Patients who did not have an improvement or deterioration in neuropsychiatric symptoms coinciding with a respective addition or removal of an NSAID as the sole change in treatment.
Difference in means assessed using the t-test. Difference in proportions assessed using the chi-square test.
PANS Global Impairment Score and Caregiver Burden Inventory collected at the initial presentation to the Stanford PANS clinic.
Data are missing for some neuropsychiatric symptoms; this is reflected in the denominators of the categorical variables.
Mood dysregulation includes depression and/or emotional lability.
PANDAS, Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal Infections; PANS, Pediatric Acute-onset Neuropsychiatric Syndrome; NSAIDs, nonsteroidal anti-inflammatory drugs.
NSAID side effects
Thirty patients (30/77, 39%) of those included in this study experienced side effects, including 14 patients with gastrointestinal symptoms (gastritis, abdominal pain, nausea, constipation, and diarrhea), two patients with psychiatric symptoms (panic attacks and irritability), and two patients with bruising. The remaining 12 patients had various other side effects including pseudoporphyria, hematuria, blood in stool, red eyes, abnormal liver enzymes (coinciding with viral gastroenteritis), dizziness, and rectal bleeding. All side effects resolved after decreasing the NSAID dose, switching to a different type of NSAID, or discontinuing the NSAID.
Case 1
A 7-year-old male patient demonstrated dramatic improvement in mood, tics, and behavior with treatment of NSAIDs (ibuprofen and naproxen), and clear deterioration in psychiatric symptoms when NSAIDs were discontinued on separate occasions.
Patient was in his usual state of good health until around 4 years of age when he developed sudden-onset tics followed by a 5- to 7-day period of severe OC symptoms, anxiety, mood issues, behavioral changes, developmental regression, deterioration in school performance, sensory issues, sleep disturbance, and urinary frequency. These symptoms appeared one day after a febrile illness that included sore throat, nasal symptoms, and cough. At the time, his father had a recurrent GAS infection, requiring five courses of antibiotics to eradicate the infection. The patient was not tested for evidence of GAS at this time.
Most of the extreme behavior and psychiatric symptoms were self-resolved, but he had ongoing motor tics, verbal tics, and attention issues in the ensuing years. His school made special classroom accommodations. He was oblivious to what was going on around him and spent a lot of time spinning around and engaging in imagination. A neurologist diagnosed him with attention-deficit/hyperactivity disorder and the patient started treatment with methylphenidate (5 mg in the morning and 2.5 mg in the afternoon) and amphetamine/dextroamphetamine (2.5 mg once daily), which escalated depression, anger, and aggression. Around the same time, he was diagnosed with sleep apnea and underwent a tonsillectomy and adenoidectomy. His sleep apnea persisted and he started continuous positive airway pressure. His ongoing neuropsychiatric symptoms included fatigue and oppositional defiant behaviors. He refused simple tasks, such as brushing his teeth. He would also frequently hit, kick, and spit.
At age 6, he started combination methylphenidate (5 mg daily) and guanfacine (2 mg daily) with some improvement in attention, although his anger and behavior continued to be problematic. He also struggled with insomnia, sleep onset, and sleep maintenance. He was evaluated for autism given his inability to engage socially, but it was ruled out after psychological and academic testing. Educational testing revealed profound learning disability but a high intelligence quotient.
At age 7 (23 kg), the patient had a sudden escalation in vocal tics, which was so severe that it prevented him from talking. He also had ongoing problems with insomnia, urinary incontinence, and motor tics. His parents started ibuprofen (200 mg daily) for the first time and reported a dramatic improvement of behavior, mood, and tics. His response was within a few hours of taking ibuprofen. It was the first time they saw their child happy in the past 3 years.
He was subsequently seen at a medical group that diagnosed him with PANS. Azithromycin (250 mg daily) was added to the ibuprofen, which was associated with further improvement in mood and behavior. The parents reported that he was a “totally different kid”; he was happy, cooperative, tic-free, and had fewer issues with learning.
Several months later, the patient stopped taking ibuprofen and guanfacine due to rising liver enzymes. His mood and aggression subsequently worsened. He became violent toward the family cats. His parents reported that he cried more frequently and became afraid of things for no apparent reason. He also developed severe separation anxiety. Upon restarting ibuprofen, his parents noted abatement of his rage, violence, tics, anxiety, and depressed mood.
One month later, the patient (27 kg) switched to naproxen (220 mg daily) for management of hand stiffness in multiple joints (hand, wrist, and neck) pains and psychiatric symptoms, which led to further improvement in all the above symptoms. Subsequent attempts to remove naproxen were unsuccessful as all removals resulted in neuropsychiatric deteriorations within 12 hours. In total, there have been eight deliberate discontinuations of naproxen and six “accidentally missed” doses that have occurred approximately every other month. Each time the family notes escalation in tics, anger, and oppositionality within 12 hours.
Case 2
A 10-year-old female patient had clear improvement in the severity and duration of neuropsychiatric symptoms with naproxen, and a clear deterioration after a short trial off naproxen.
As a young child, the patient had issues with chronic irritability, anxiety, mild compulsive traits, mood issues, and sleep disturbance. She also had a long history of frequent ear infections. At age 4, she had a sudden onset of new OC symptoms (repetitive organization and hoarding), separation anxiety, rage, and sensory issues (tactile and noise intolerance) following a rash. She had a second episode two years later following streptococcal pharyngitis, in which she experienced a sudden escalation of OC symptoms and psychotic behavior that lasted one week. The patient continued to have similar relapses characterized by OC symptoms, eating restriction, mood changes, irritability, aggression, and oppositional behavior, typically following infections and lasting two weeks. Due to residual chronic mood issues and anxiety, she was started on fluoxetine at age 6.
At age 10 (52 kg), she had another abrupt escalation of OC symptoms, anxiety, emotional lability, irritability, behavioral issues, fatigue, and pain. She was diagnosed with PANS by our clinic and given a trial of naproxen (220 mg twice daily) and a 5-day course of azithromycin, which coincided with a prompt improvement in these neuropsychiatric symptoms. She remained on naproxen until one month later when it was removed due to bruising. Following removal of naproxen, she had significant escalation in rage, emotional lability, and pain that was not attributed to any known infection or illness. The patient restarted naproxen (220 mg twice daily), and her parents reported a “vast improvement.”
Shortly afterward, the patient had another ear infection and upper respiratory infection, coinciding with a neuropsychiatric deterioration characterized by escalation of OC symptoms, irritability, violence, mood instability, behavioral regression, and polyuria. We temporarily doubled her dose of naproxen (440 mg twice daily), resulting in reduced severity of symptoms. Additionally, her episode was shorter in duration (3 days) than previous episodes (2 weeks).
Currently, the patient has high overall functioning. In particular, her anxiety, sleep disturbances, sensory amplification, and pain have substantially improved. She currently takes fluoxetine (10 mg daily) and naproxen (220 mg twice daily). We will attempt to wean the naproxen every 3 to 6 months to demonstrate ongoing need for this medication.
Case 3
A 6-year-old male patient demonstrated dramatic improvement upon treatment with ibuprofen, initially used to control his joint pain. The patient has since switched to naproxen. He has mild OC symptoms but high overall functioning.
This patient had preexisting eye-blinking and throat-clearing tics, but was otherwise in a usual state of good health until he experienced two episodes of joint swelling that were temporally associated with neuropsychiatric symptoms. The initial episode of joint swelling at age 6 was described as sudden-onset knee pain without injury. He was limping and complaining of pain. He ultimately went to the emergency room for imaging and blood work. His erythrocyte sedimentation rate was normal (11 mm/h) and the x-ray report showed normal films of the bilateral hips, left femur, and left knee. The patient received ibuprofen and the pain resolved after 3 days.
At age 6, he had a sudden onset of OC symptoms, separation anxiety, emotional lability, behavior regression, new-onset bedwetting, deterioration in handwriting, insomnia, and worsening of his tics in the setting of a respiratory illness. A throat culture for GAS was negative, but he did have a mildly positive streptozyme titer (1:100). He was treated (by a community medical group) with cefdinir and plaquenil, which temporally coincided with noticeable improvement in OC symptoms and behavior regression. The patient had ongoing throat-clearing tics. He eventually returned to his previous functioning with minimal residual symptoms.
At age 8 (44 kg), he experienced a mild escalation in OC symptoms, tics, enuresis, insomnia, and joint pain following a GAS exposure. Treatment with ibuprofen (380 mg three times daily) was helpful in controlling his joint pain. His OC symptoms (his “perfects”) had improved within 5 days and completely resolved after 20 days. His OC symptoms later returned and coincided with wrist and knee pain following a severe diarrheal illness. He was prescribed a 5-day prednisone burst and was transitioned to naproxen (250 mg twice daily) for arthritis. His OC symptoms and joint pain completely resolved. Clinical documentation describes the patient at his best level of functioning since his onset of PANS.
At age 9 (48 kg), an attempt to decrease his naproxen to 250 mg once daily resulted in an increase in OC symptoms, although this was in the setting of a GAS exposure. A second trial off naproxen resulted in a mild increase in OC symptoms, and his physical examination revealed recurrence of his arthritis and limited lumbar flexion. Thus, the patient was restarted on naproxen with rapid resolution of symptoms.
Currently, the patient is maintained on naproxen (250 mg twice daily). On this regimen, his neuropsychiatric symptoms are stably mild (nail picking, finger smelling, perfectionism) and his arthritis is in quiescence. We have recommended dose reduction or trials off naproxen every 3 to 6 months to test for ongoing need.
Discussion
This is the first study aimed to evaluate the course of neuropsychiatric symptoms after NSAID addition or removal in a cohort of patients with PANS. We found that roughly one-third of addition trials coincided with improvement in neuropsychiatric symptoms, and roughly one-third of removal trials coincided with escalations in neuropsychiatric symptoms. We also provide a detailed description of the clinical course of three patients who had dramatic improvements in their neuropsychiatric symptoms corresponding with an NSAID introduction, and clear deteriorations upon removal. Side effects were self-limited.
A growing body of literature suggests links between inflammation and neuropsychiatric symptoms. Clinical trials have demonstrated benefits of NSAIDs in bipolar disorder and depression (Abbasi et al. 2012; Arabzadeh et al. 2015); and NSAIDs are being investigated as adjuvant therapy in schizophrenia (Müller et al. 2004) and obsessive-compulsive disorder (Sayyah et al. 2011; Shalbafan et al. 2015). Psychiatric symptoms have also been described in a variety inflammatory diseases including neuropsychiatric lupus, autoimmune encephalitis, and Behçet's syndrome (Calikoglu et al. 2001; Slattery et al. 2004; Dale and Brilot 2012; Magro-Checa et al. 2016). Among patients in the Stanford PANS Clinic, 20%–30% have had at least one episode of reactive or persistent arthritis, and 26% report neck pain, sacroiliac joint pain, concerning inflammatory back pain (Frankovich et al. 2015; Brown et al. 2016). Additionally, 71% of our patients with PANS have first degree members with an inflammatory disorder, including a high rate of inflammatory back pain and spondyloarthritis (Frankovich et al. 2015; Brown et al. 2016). These arthritis conditions (which fall under the category of spondyloathritis) tend to be highly responsive to NSAIDs.
Human and animal research suggest that the mechanisms underlying PANS/PANDAS also involve neuroinflammation and autoimmunity (Hoffman et al. 2004; Yaddanapudi et al. 2010; Brimberg et al. 2012; Cox et al. 2013; Lotan et al. 2014; Macrì et al. 2015; Carapetis et al. 2016; Cutforth et al. 2016; Dileepan et al. 2016). Polymorphisms in the tumor necrosis factor (TNF)-α gene have been associated with PANDAS (Luleyap et al. 2013) and positron emission tomography imaging suggests greater microglial activation in patients with PANDAS compared to controls (Kumar et al. 2015). A recent mouse model investigating links between neuroinflammation and nasopharyngeal infections has shown that multiple GAS infections can lead to generation of antigen-specific Th17 cells that migrate along olfactory tracts into the brain to increase blood-brain barrier (BBB) breakdown, microglial activation, and changes in synaptic function (Dileepan et al. 2016). Importantly, NSAIDs can affect all of the above pathways including reduction of TNF-α (Iñiguez et al. 1999, 2010), reduction in BBB permeability (Candelario-Jalil et al. 2007; Brooks et al. 2008), reduction in Th17 response (Chizzolini et al. 2008; Napolitani et al. 2009), and reduction in microglial activation (Mackenzie and Munoz 1998; Klegeris et al. 2004).
Although we describe in detail three patients with clear responses to the addition and removal of NSAIDs, most patients who received NSAID treatment in our clinic experienced either partial responses or no response. Many of the patients who experienced partial responses exhibited improvement in several neuropsychiatric symptoms, yet continued to have residual symptoms and subsequent deteriorations while still receiving NSAIDs. Several of these patients have required more aggressive treatment, such as oral corticosteroids and IVIG. Some patients were found to respond better to particular NSAIDs, however, these responses differed among individuals in the cohort, with no clear evidence of universal superiority for one NSAID over another. The overall heterogeneity in response to treatment among children with PANS may be explained by biological differences and differences in severity of illness, duration of illness, and disease trajectory at the time of the NSAID trial.
The PANS Research Consortium recommends NSAIDs trials to treat mild disease as per the 2017 PANS immunomodulatory guideline (Frankovich et al. 2017). At this time, there is no clear indication within our PANS cohort that one NSAID is superior to others, and therefore we recommend that NSAID choice be determined by patient-specific considerations including dosing frequency, formulation, and side effects. As noted above, one patient (Patient 17) experienced neuropsychiatric deterioration within 30 minutes of missing a single ibuprofen dose, suggesting that drug half-life is also an important consideration. Our experience suggests that if a patient does not respond to one NSAID, it is appropriate to consider a trial of another NSAID for potential response. If the patient responds, then periodic trials off NSAIDs are recommended. If the patient repeatedly deteriorates when the NSAID is discontinued, it can be restarted and continued long term with continued trials of removal every 3 to 6 months. The PANS Research Consortium also recommends lab work every 3 to 6 months for patients on long-term NSAIDs, to evaluate liver enzymes, blood urea nitrogen, creatinine, complete blood count with differential, and urinalysis to evaluate hydration status. Patients who restrict fluids should not take NSAIDs (Frankovich et. al 2017).
NSAIDs can contribute to gastritis, gastroesophageal reflux disease, constipation, diarrhea, and nausea (Ruperto et al. 2005; Sobel et al. 2014). In our study, we found that roughly one-third of patients who received NSAIDs experienced side effects, mainly gastrointestinal symptoms. These side effects abated after stopping, decreasing the dose, or switching to a different type of NSAID. If NSAIDs are included in a patient's treatment plan, clinicians should conduct trials off NSAIDs per the 2017 immunomodulatory treatment guidelines (Frankovich et al. 2017).
Limitations
This retrospective study is limited by its reliance on documentation by clinicians and reports from parents. The effects of NSAIDs on neuropsychiatric symptoms were at times unclear due to lack of adequate documentation. In addition, effects of treatment could have been missed if they occurred between clinic visits and were not reported by the patient's parents. Parent reports, retrospectively describing their child's response to NSAID treatment, are sometimes vague in content and may not accurately capture the exact time to response. Because quantitative symptoms scores were not consistently acquired for all patients, our analysis relies on a qualitative analysis of each patient's symptoms.
Another limitation is the confounding factor of concurrent treatments. In our clinic, NSAIDs are often added to a patient's treatment regimen at the same time as other interventions, most often alongside antibiotics. This confound led us to exclude more than half of our NSAID trials. Even when an NSAID was the only treatment added or removed at the time, patients were often receiving concurrent treatments. While improvement may be temporally associated with the addition of the NSAID, improvement can also be attributed to a delayed effect of other interventions (antibiotics, psychiatric medications, CBT, etc.), the resolution of an infection, or organic resolution over time. Similarly, escalations of neuropsychiatric symptoms temporally associated with removal of an NSAID could be due to a number of confounding explanations, such as a new infection or a wearing off of another concurrent medication. To determine isolated effects of NSAIDs on neuropsychiatric symptoms, a randomized clinical trial is warranted.
Conclusions
Improvement in neuropsychiatric symptoms was evident in roughly one-third of NSAID addition trials. Escalations in neuropsychiatric symptoms was evident in roughly one-third of NSAID removal trials. These findings suggest that NSAIDs may be helpful for treating neuropsychiatric symptoms in some patients. More research is needed to understand the effects of NSAIDs on neuropsychiatric symptoms, and to determine the length and timing of NSAID treatment to create more clear guidelines on their use for children with PANS.
Clinical Significance
NSAIDs may be a helpful treatment in patients with PANS. Long-term use of NSAIDs can be done safely if necessary precautions are taken, including adequate hydration and lab monitoring. Trials off NSAIDs should be done periodically to assess its efficacy. A randomized clinical trial is warranted to better elucidate the effects of NSAIDs on neuropsychiatric symptoms in PANS.
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Susan Swedo, MD, The National Institute of Mental Health, the PANDAS Physicians Network, Dr. Kiki Chang, MD, and all the staff and faculty at Lucille Packard Children's Hospital and Stanford PANS Clinic who make caring for these children possible.
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.