
Abstract
Objectives:
Sudden and severe onset of obsessive–compulsive disorder (OCD) may present secondary to infectious and/or immune-mediated triggers. We assessed the preliminary efficacy, tolerability, and safety of azithromycin compared with placebo in the treatment of OCD and associated symptoms in children with pediatric acute-onset neuropsychiatric syndrome (PANS).
Methods:
Thirty-one youth aged 4–14 years (M = 8.26 ± 2.78 years, 62.5% male) were randomized to receive either placebo or azithromycin for 4 weeks (10 mg/kg up to 500 mg per day). Both groups were administered twice daily probiotics. The primary outcome, obsessive–compulsive symptom severity, was assessed using the OCD Clinical Global Impressions Severity (CGI-S OCD) and Children's Yale-Brown Obsessive Compulsive Scale (CY-BOCS).
Results:
Participants in the azithromycin group (n = 17) showed significantly greater reductions in OCD severity on the CGI-S OCD than the placebo group (n = 14) posttreatment (p = 0.003), although there were no significant differences on the CY-BOCS. Significantly more participants in the azithromycin condition met treatment responder criteria on the CGI-I OCD at the end of week 4 (41.2%, n = 7) in comparison to the placebo group (7.1%, n = 1; p = 0.045). Tic severity moderated treatment response, with greater tic severity being associated with enhanced treatment response on the CGI-S OCD. Azithromycin was well tolerated with minimal adverse effects and no study dropouts due to side effects. However, the azithromycin group showed a trend toward significantly greater electrocardiography QTc (p = 0.060) at the end of week 4, and significantly more reports of loose or abnormal stools (p = 0.009).
Conclusion:
This double blind pilot study suggests that azithromycin may be helpful in treating youth meeting the PANS diagnosis, especially those with elevated levels of both OCD and tic symptoms. Azithromycin was well tolerated, but the potential for cardiac risks suggests that additional monitoring may be needed to ensure safety.
Introduction
F
Nosologically, pediatric acute-onset neuropsychiatric syndrome (PANS) (Swedo et al. 2012) and Pediatric Autoimmune Neuropsychiatric Syndrome Associated with Streptococcus (PANDAS) (Swedo et al. 1998a) are subtypes of childhood-onset OCD that begin suddenly often following an infection (although not required for PANS), and have accompanying high rates of comorbidities. Specifically PANDAS is a subset of PANS with an acute onset of OCD that is temporally associated with a group A streptococcal (GAS) infection. In addition to OCD, children with PANS/PANDAS frequently have symptoms of separation anxiety, nightmares, irrational fears, decreased appetite, personality changes, oppositional behavior, tics, hyperactivity, inattention, and deterioration of math skills, and handwriting abilities (Swedo et al. 1998a; Bernstein et al. 2010; Murphy et al. 2012). The immune-driven hypothesis for PANS/PANDAS proposes that antibodies produced in response to an infection cross the blood–brain barrier and interfere with neuronal signaling leading to neuropsychiatric symptoms (Kirvan et al. 2003; Cox et al. 2013; Dileepan et al. 2016; Kim et al. 2016).
Although inadequately examined, the current treatment for youth meeting PANS/PANDAS criteria includes immune therapies, prophylactic antibiotic therapy, and the same standard of care practices for pediatric OCD (i.e., psychopharmacological, cognitive-behavioral treatment) (Murphy et al. 2014). Despite the increasing evidence suggesting immunological disruptions in the pathology of acute-onset OCD and/or tics, the full potential of immune-based therapies for the treatment of acute-onset OCD and/or tics is still relatively uncharted. Using rodent models, Lotan et al. (2014) found not only a direct correlation between GAS infection and behavioral abnormalities, but also an association between antibiotic intervention and behavioral improvement. This study showed a reduction of immunoglobulin G (IgG) deposition in the thalamus with the use of antibiotics.
In a case series, 12 children with acute and severe onset of OCD were positive for GAS tonsillopharyngitis. Symptoms remitted during antibiotic treatment for the infection and symptoms reappeared with a new infection, supporting an association between OCD and GAS infections (Murphy and Pichichero 2002). To date, there are only three clinical trials examining antibiotic treatment for PANDAS or PANS (Garvey et al. 1999; Snider et al. 2005; Murphy et al. 2015a) (Table 1).
OCD, obsessive–compulsive disorder; PANDAS, Pediatric Autoimmune Neuropsychiatric Syndrome Associated with Streptococcus.
In an 8-month, placebo-controlled, crossover trial (N = 37), prophylactic oral penicillin did not effectively reduce episodes of PANDAS when compared with the placebo (Garvey et al. 1999). However, the crossover design used in this study may have introduced some possible confounds such as carry-over and order effects, in addition to the subjects in the placebo arm needing antibiotics for known infections. Additionally, the study did not control for the possibility of infections contracted during one arm and the subsequent symptoms flare that could present in the other arm. Given the potential confounds of this design, a 12-month parallel design examined prophylactic doses of penicillin (N = 11) and azithromycin (N = 12) in participants classified as PANDAS (Snider et al. 2005). During the study year, the mean number of neuropsychiatric exacerbations was reduced from 1.8 to 0.9 (SD = 0.5) and the mean number of streptococcal infections was significantly reduced from 2.4 to 0.1 (SD = 0.3). Both medications showed similar reductions in exacerbations of OCD and tics, without significant differences in side effects between groups. This study was limited by the comparison of retrospective data for the baseline year to prospective data of the treatment year using an active comparator. Additionally, the response to azithromycin or penicillin could be explained by time, as symptoms can remit on their own.
More recently, Murphy et al. (2015a) conducted a placebo-controlled trial examining the preliminary safety and efficacy of a 30-day treatment dose of cefdinir in reducing symptom severity in youth aged 4–13 with a recent onset of OCD and/or tics (N = 28), but not all meeting full PANS/PANDAS criteria. Participants receiving cefdinir exhibited clinical improvements of OCD and tic symptom severity (CYBOCS Cohen's d = 1.22, YGTSS Cohen's d = 0.97); however, these differences failed to meet statistical significance. Collectively, these clinical trials generally suggest some treatment benefit, but difficulties with study design and small sample size limit the influence of their findings (Garvey et al. 1999; Snider et al. 2015; Murphy et al. 2015a).
In light of the paucity of research evaluating PANS/PANDAS phenomenology and response to antibiotic therapy, we aimed to evaluate the feasibility, tolerability, and preliminary efficacy of azithromycin in the treatment of children with acute- and severe-onset OCD. Azithromycin has the advantage of providing defense against GAS and Mycoplasma pneumonia, as well as having reported immune-modulating effects outside of its antimicrobial properties, such as decreasing inflammatory cytokine production (Kanoh and Rubin 2010; Altenburg et al. 2011).
Given previous reports of improvements in neuropsychiatric symptoms of patients presenting with PANDAS following antibiotic treatment (Murphy and Pichichero 2002; Snider et al. 2005; Murphy et al. 2015a) and the immune-modulating properties of azithromycin, we hypothesized that youth with PANS receiving antibiotics would show greater overall improvement in symptom severity (e.g., OCD, tic, and/or associated neuropsychiatric symptom severity) compared with youth receiving placebo.
Methods
Study design and participants
This study was approved by the local institutional review board, and registered with
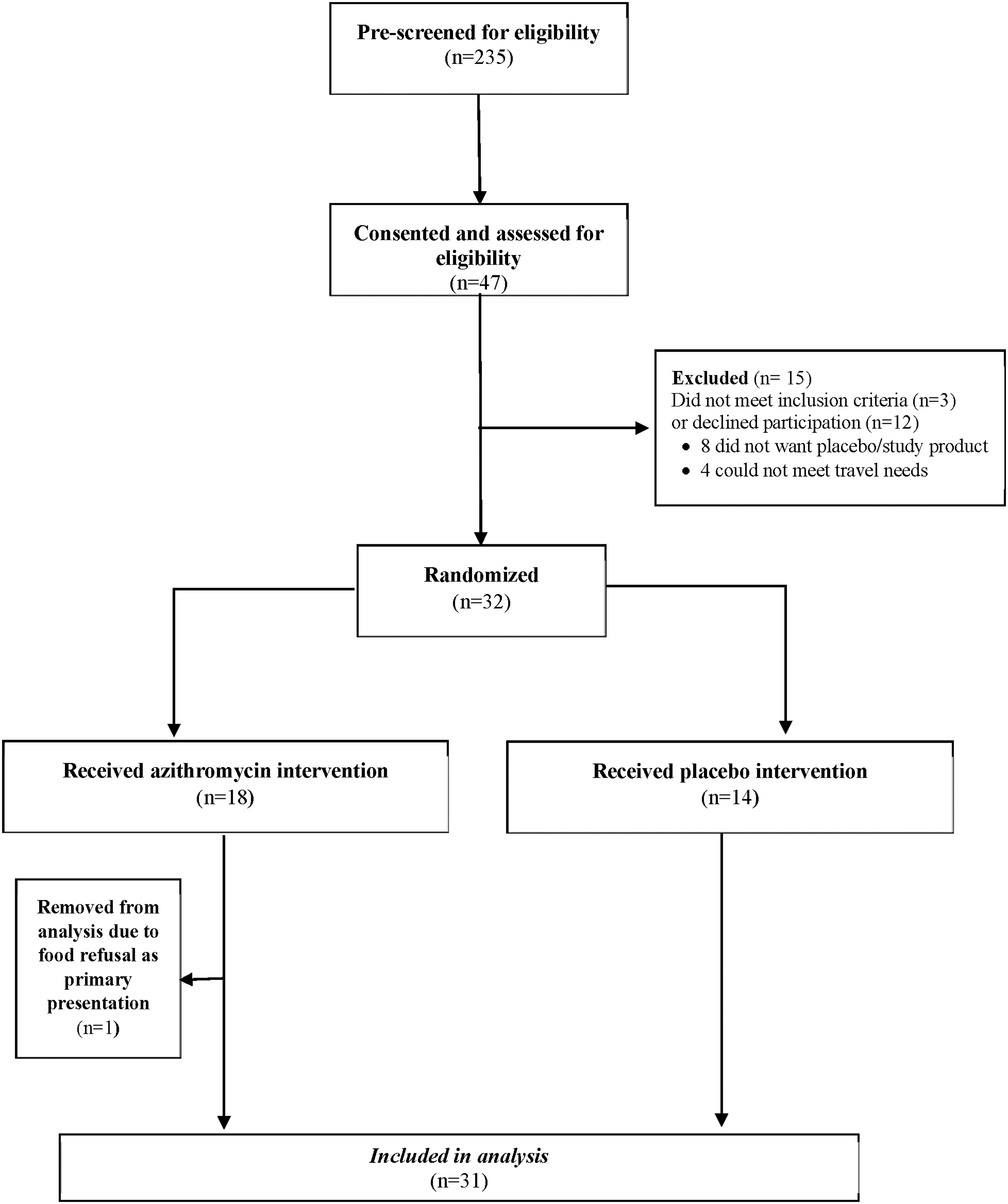
CONSORT diagram depicting recruitment and retention of participants through the study.
Inclusion criteria included, (1) an acute onset or acute relapse within 6 months of evaluation (abrupt, dramatic overnight onset) of moderate or worse OCD symptoms (Children's Yale-Brown Obsessive Compulsive Scale [CY-BOCS] Total Severity Score ≥16, and Clinical Global Impression Severity [CGI-S] ≥4 [Moderate]); (2) presence of a sudden and severe co-occurrence of at least two neuropsychiatric symptoms (e.g., anxiety, emotional lability, tics, frequent urination, and food restrictive symptoms) (Swedo et al. 2012); (3) aged 4 to 14 years (age range was selected to capture primary ages of onset); and (4) medication free or on a stable dose of a neuropsychiatric medication (4 weeks for most medications [including atomoxetine, anticonvulsants, stimulants, and antipsychotics] and 8 weeks for selective serotonin reuptake inhibitors [SSRIs]).
Due to the difficulty of a definitive confirmation of an infectious trigger with each neuropsychiatric onset, we chose to examine youth meeting the PANS criteria assuming that some of the group would have a GAS or Mycoplasma infectious trigger. By meeting inclusion criteria, participants met PANS criteria. Exclusion criteria included (1) gradual onset or duration of OCD symptoms >6 months; (2) receiving extended-course antibiotics (i.e., not a typical treatment course of antibiotics for an infection, or prophylactic antibiotics) and/or other immune therapy for PANS; (3) a primary diagnosis of tics (rather than OCD); (4) receiving exposure-based cognitive behavioral therapy (CBT); (5) a history of nonresponse to a prior antibiotic trial; or (6) a diagnosis of moderate to severe autism spectrum disorder, intellectual disability, and/or chronic neurological disease.
Randomization, masking, and design considerations
Following written parental consent, child assent, and an initial assessment, children were randomized in a one to one ratio to azithromycin (10 mg/kg up to 500 mg per day) or placebo for 4 weeks. Dosing was based on clinical experience of those treating PANS patients, which supported that this regimen was effective and appeared to be safe. For determining the timeline of conditions, clinical experience also suggested that antibiotic response occured after week 2, but before week 4. A longer study would have required the placebo group to not receive active or additional treatments. All physicians and raters, as well as participants and families were blind to assignment. After 4 weeks, participants entered the open-label phase, where all participants received azithromycin. Medication was an oral suspension and placebo was matched for color, taste, and consistency.
Procedures
Participants were evaluated weekly (every 2 weeks in person and other weeks through phone interview). Raters were not involved in medical management (medication side effects, etc.) or other aspects of clinical care. Both arms were provided with twice daily probiotic therapy (Saccharomyces boulardii, Florastor®) to mitigate risk of antibiotic-induced diarrhea.
Infection-related OCD/tic evaluation
The infection-related OCD/tic evaluation (IROTE) is an assessment of infection-triggered symptoms and history of autoimmune illness (Murphy et al. 2004). This clinician-administered questionnaire elicits information germane to the diagnosis of immunological conditions, infections, rheumatic fever, SC, and other movement disorders (Murphy et al. 2012). This instrument also screens for personal and family history of autoimmune illnesses. Infection trigger was determined based on documented infections and/or laboratory results. The screening visit IROTE has a parent version and a clinician version that complement each other (IROTE-PV, IROTE-MD). These instruments collect historical information, whereas the return visit administered IROTE (IROTE-RV) focuses on change in status. A summary sheet with PANS criteria is included to document PANS caseness. The IROTE-RV was administered at every visit.
Outcomes
Primary outcomes
Children's Yale-Brown Obsessive Compulsive Scale
The CY-BOCS is a clinician-rated, semistructured interview for rating the severity of OCD (Scahill et al. 1997). Participants were rated on the CY-BOCS at every visit.
Clinical Global Impression-Severity Scale
The CGI-S scale is a seven-point clinician rating of severity of psychopathology. Severity ratings range from 1 (no illness) to 7 (extremely severe). This instrument has been successfully used in treatment studies (Cook et al. 2001; Storch et al. 2007). This rating was performed separately to assess the severity of OCD, tic, mood, and neurocognitive symptoms. The mood symptom CGI-S encompassed sadness/irritability/rage symptoms, and the neurocognitive CGI-S encompassed attention-deficit/hyperactivity disorder, memory, and school performance symptoms. Participants were rated on the CGI-S at every visit.
Secondary outcomes
Clinical Global Improvement Scale
The Clinical Global Improvement (CGI-I) scale (Guy 1976) is a 7-point rating system of treatment response anchored by 1 (very much improved) and 7 (very much worse). This rating was performed separately to assess the severity of OCD, tic, mood, and neurocognitive symptoms. Participants were rated on the CGI-I at every study visit following baseline. Participants who scored ≤2 on the CGI-I OCD at the end of week 4 were considered responders.
Child Global Assessment Scale
The Child Global Assessment Scale (CGAS) (Sorensen et al. 1982; Shaffer et al. 1983; Green et al. 1994) is used for assessing a child's overall level of functioning. Based on clinical information from the parent and child, the clinician rates the overall psychological functioning on a scale of 0–100. Participants were rated on the CGAS at every visit.
Yale Global Tic Severity Scale
The Yale Global Tic Severity Scale (YGTSS) is a clinician-rated, semi-structured interview for rating tic symptom severity according to number, frequency, intensity, complexity, and interference (Leckman et al. 1989; Storch et al. 2005). The YGTSS has excellent interrater agreement and good psychometric properties (Storch et al. 2005). Participants were rated on the YGTSS at every visit.
Swanson, Nolan, and Pelham–IV Parent Scale
The psychometrically sound, parent-rated Swanson, Nolan, and Pelham–IV Parent Scale (SNAP-IV) provides a dimensional scaling of the DSM items for inattention, impulsivity, hyperactivity, and oppositionality (Swanson 1992). Symptoms are scored by assigning a severity estimate for each item on a four-point scale. The SNAP-IV was administered at every visit.
Children's Affective Lability Scale
The Children's Affective Lability Scale (CALS) (Gerson et al. 1996) is a 20-item parent report measure developed to assess affect regulation in children aged 6–16. Internal consistency, 2-week test–retest reliability, and construct validity are excellent (Gerson et al. 1996). The CALS was administered at every visit. This measure is not validated for use in 4–5 year olds.
Screen for Childhood Anxiety-Related Emotional Disorders
The Screen for Childhood Anxiety-Related Emotional Disorders (SCARED) is a 41-item parent and participant-completed tool used to measure symptoms of anxiety, including the most common symptoms of panic/somatic, generalized anxiety, separation anxiety, social phobia, and school phobia. The child and parent versions of the SCARED have moderate parent–child agreement and good internal consistency, test–retest reliability, and discriminant validity; it is also sensitive to treatment response (Birmaher et al. 1999). The target population for this rating is 8–18 years of age (Birmaher et al. 1997). The parent and child version of the SCARED were administered at every visit. This measure is not validated for use in 4–7 year olds.
Biological measures
At the screening visit, all participants underwent a physical examination. Electrocardiography (ECG) measurements, temperature, pulse rate, blood pressure, height, and weight were obtained at each visit. ECGs were interpreted by Pediatric Cardiology. Adverse effects (AEs) were monitored at each visit by checklists and interviews with the physician.
Anti-deoxyribonuclease B (anti-DNase B), anti-streptolysin O (ASO), M. pneumonia immunoglobulin (IgG/IgM), antinuclear antibody (ANA), Raji cell (C3d-bound circulating immune complexes), C1q, quantitative immunoglobulins, comprehensive metabolic panel, complete blood count (CBC), and urinalysis were performed at a clinical laboratory (LabCorp). ACMP and CBC were repeated at the end of week 4 as part of safety monitoring.
Statistical analysis
The primary analyses were conducted as intent to treat and included all randomized participants. Compliance with trial procedures, dropouts, and reason for participant withdrawal were carefully tracked throughout the study. To evaluate medication tolerability, adverse events were compared between the placebo and azithromycin groups through Fisher's exact tests. Baseline group differences were evaluated using independent samples, t-tests for continuous variables, and Fisher's exact tests for categorical variables as appropriate. Changes in pulse, weight, and ECG QTc from baseline to week 4 within the azithromycin group were examined using paired t-tests. Group differences in the change in pulse, weight, and ECG QTc from baseline to end of week 4 were examined using t-tests. The CGI-S OCD and the CY-BOCS were chosen as primary outcomes a priori. The CGI-I, CGAS, YGTSS, SNAP-IV, CALS, and SCARED were chosen as secondary outcomes.
To evaluate between-group treatment outcomes on continuous outcomes, mixed-effect models were used including random effects for intercept, and fixed effects for time, group, and their interaction. To evaluate treatment response, CGI-I scores reflecting “much improved” or “very much improved” or ≥30% reduction on the CY-BOCS from baseline to end of week 4 were considered to reflect treatment responder status, whereas all other cases were considered nonresponders (Storch et al. 2010). Group comparisons of response rates (i.e., a categorical outcome) were evaluated through a Fisher's exact test. To examine whether change in OCD symptom severity (as measured by the CGI-S OCD and CY-BOCS) was moderated by tic severity (measured by the YGTSS), we used mixed model analyses. Missing data were minimal, with no more than two cases with missing data on any measure (2.16% of all data points) and no missing data on measures of primary outcome. Mixed model analyses allow all available data to be included in analyses, with missing data excluded pairwise in other analyses.
Results
Clinical characteristics for 43 of the 47 screened participants were previously described (Murphy et al. 2015b). Table 2 summarizes the demographic characteristics of the 31 randomized participants. Twenty-four participants (77.42%) were on medications at baseline with no differences between groups (p = 1.000). Three subjects were receiving SSRIs at baseline, all of which were indicated for OCD. The most common trigger/associated infection in the participants' current episode at study entry was GAS (n = 19, 61.29%) and upper respiratory infections (URIs; n = 13, 41.94%) (Table 3). The number of GAS triggers is greater if elevated ASO titers or Anti DNase B titers (n = 26, 83.87%) at baseline were considered as additional evidence for GAS trigger.
Based on medical record review and parent report.
Urinary tract infections, gastrointestinal illnesses, exposure to undiagnosed illness in sibling.
Based on laboratories reported at baseline visit.
Preeclampsia, induction, prenatal exposures, postnatal complications, abnormal Apgar scores.
IgG, immunoglobulin G.
One participant in the placebo group did not complete week 4 due to desire to receive additional treatment. One participant in the azithromycin group briefly discontinued azithromycin for 1 week during week 3, during which time the participant took cephalexin due to a GAS infection before resuming azithromycin again at the start of week 4. Symptoms were already improved and this subject did not experience an exacerbation with the GAS infection. It does suggest that this subject may have had an azithromycin-resistant GAS. It is unclear whether the participant had positive levels of azithromycin during the time they were receiving cephalexin. Due to the long half life of azithromycin, it is presumed that the participant had some continued level of azithromycin while receiving cephalexin.
There were no group differences on any demographic measure. Similarly, the groups did not differ in terms of baseline clinical characteristics, with the exception that youth in the azithromycin group showed higher baseline anxiety severity on the SCARED (M = 31.82, SD = 5.75; M = 20.43, SD = 15.30; p = 0.051; Table 4). Twenty-six of the 31 enrolled (83.87%) presented during their first PANS episode and were considered new onset, whereas five (16.13%) presented during a recurrent PANS episode (had a previous but remitted OCD episode). Descriptive statistics for symptom change over the course of treatment for the placebo and azithromycin groups are summarized in Table 4.
Effect size calculated using the difference between baseline and week 4 and dividing by the pooled standard deviation.
Effect size calculated by taking the difference in means at endpoint and dividing by the pooled standard deviation at baseline.
p < 0.01.
CGAS higher score is an improved score.
M, mean; SE, standard error; ES, effect size.
Compliance with study medication was good, based on parent report and confirmed by measuring returned study product, with only one participant in the azithromycin group and one participant in the placebo group reporting less than 100% compliance (96.45% and 96.45% compliance, respectively). Each missed two doses. However, compliance with probiotic was fair, with only 64.29% (n = 9) of those in the placebo group and 71.43% (n = 10) of those in the azithromycin group reporting 100% compliance. The difference in compliance of study medication and probiotic between groups was not significant.
Figure 2 and Table 4 report intent to treat (ITT) analyses, and indicate that the azithromycin group showed a superior reduction in OCD severity on the CGI-S OCD in comparison to the placebo group by the end of week 4 (p = 0.003). Based on those who completed treatment, youth in the azithromycin groups showed an average of 21.76% (SD = 22.21) reduction in symptoms compared with 0.95% (SD = 17.08) in the placebo group (p = 0.008), with significantly more participants in the azithromycin condition meeting treatment responder criteria on the CGI-I OCD at the end of week 4 (41.18%, n = 7) in comparison to the placebo group (7.2%, n = 1; p = 0.045).
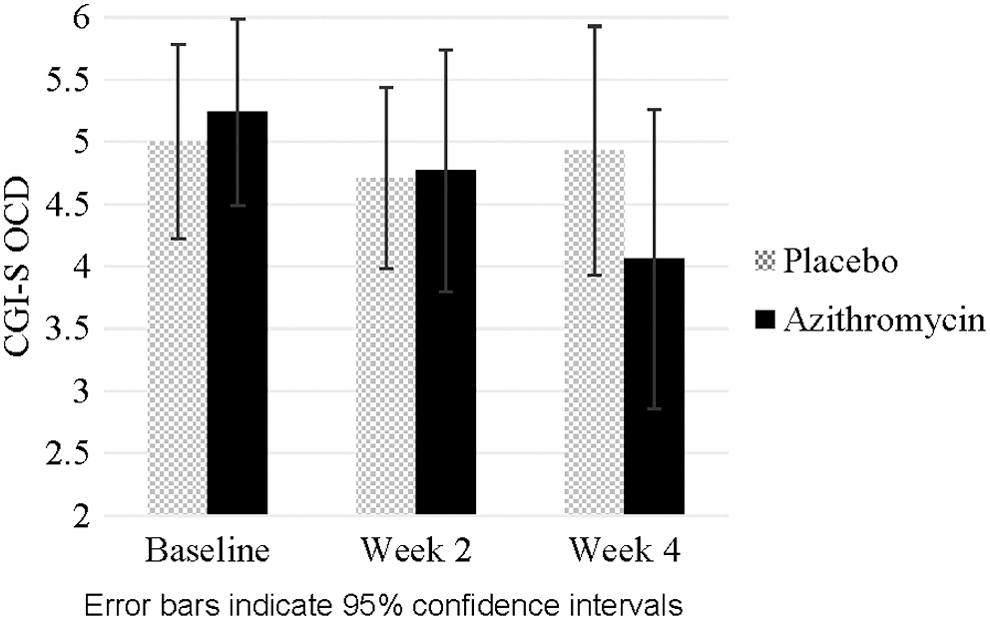
Change in obsessive–compulsive symptom severity over first 4 weeks of treatment. Error bars indicate 95% confidence intervals.
There was no significant group by time interaction on the CY-BOCS and no significant difference in the percent reduction in symptoms, with the azithromycin groups showing an average reduction of 30.52% (SD = 33.28) versus 17.20% (SD = 20.68) in the placebo group (p = 0.203). There was no significant group difference in the proportion of treatment responders (defined as a reduction of 30% reduction on the CY-BOCS; p = 0.258), despite there being more treatment responders in the azithromycin group (47.06%, n = 8) compared with the placebo group (21.43%, n = 3). At the end of week 4, 52.95% (n = 9) of participants in the azithromycin arm met treatment responder criteria based on CYBOCS or CGI-I OCD (≥30% CYBOCS reduction from baseline and/or 1 or 2 on CGI-I OCD).
When assessing reduction in tic severity, there were no group differences on the YGTSS or CGI-S Tic (Table 4). Results were the same when assessing treatment outcome among only those participants who experienced tics at baseline (n = 12 in the placebo group and n = 12 in the azithromycin group), with no significant group by time interaction on the YGTSS and CGI-S Tic (p = 0.667 and, p = 0.257 respectively). For the overall sample, 41.18% (n = 7) of the azithromycin group met treatment responder criteria on the CGI-I Tic compared with 42.86% (n = 6) in the placebo group; this difference was not statistically significant (p = 0.606). This was the same when examining group differences in only the sample of children who experienced tic symptoms, with 58.33% (n = 7) of children meeting responder criteria in the azithromycin group, compared with 50.00% (n = 6) in the placebo group (p = 0.500).
Cognitive function did not appear to change over treatment, with no significant group by time interaction for any of the SNAP subscales or for the CGI-S Neurocognition. Three participants (17.65%) in the azithromycin group were rated as “much improved” or “very much improved” on the CGI-I Neurocognition, in comparison to none (0.00%) in the placebo group (p = 0.607).
There was no group by time interaction on the CGI-S Mood (F = 2.68, p = 0.077); however, significantly more participants in the azithromycin group were rated as much improved or very much improved on the CGI-I Mood at the end of week 4 (n = 7; 50.00%) in comparison to none (0.00%) in the placebo group (p = 0.006). There was no group difference when examining changes in anxiety on the SCARED or affective lability on the CALS. Similarly, there was no group difference in improvement in global functioning on the CGAS.
To examine whether change in OCD symptom severity (as measured by the CGI-S OCD and CY-BOCS) was moderated by tic severity, we used mixed model analyses. Primary group by time interactions have been reported above. The three-way interaction between group, time, and baseline YGTSS score was significant in predicting change in OCD symptoms on the CGI-S OCD (p = 0.023), suggesting that baseline YGTSS severity had a greater impact on treatment response in the azithromycin group in comparison to the placebo group (Fig. 3). In the azithromycin group, treatment response differed depending on the level of baseline tic severity on the YGTSS. Figure 3 shows patterns of response for youth with average levels of tic severity on the YGTSS at baseline, and for those who scored one standard deviation above and below the mean.
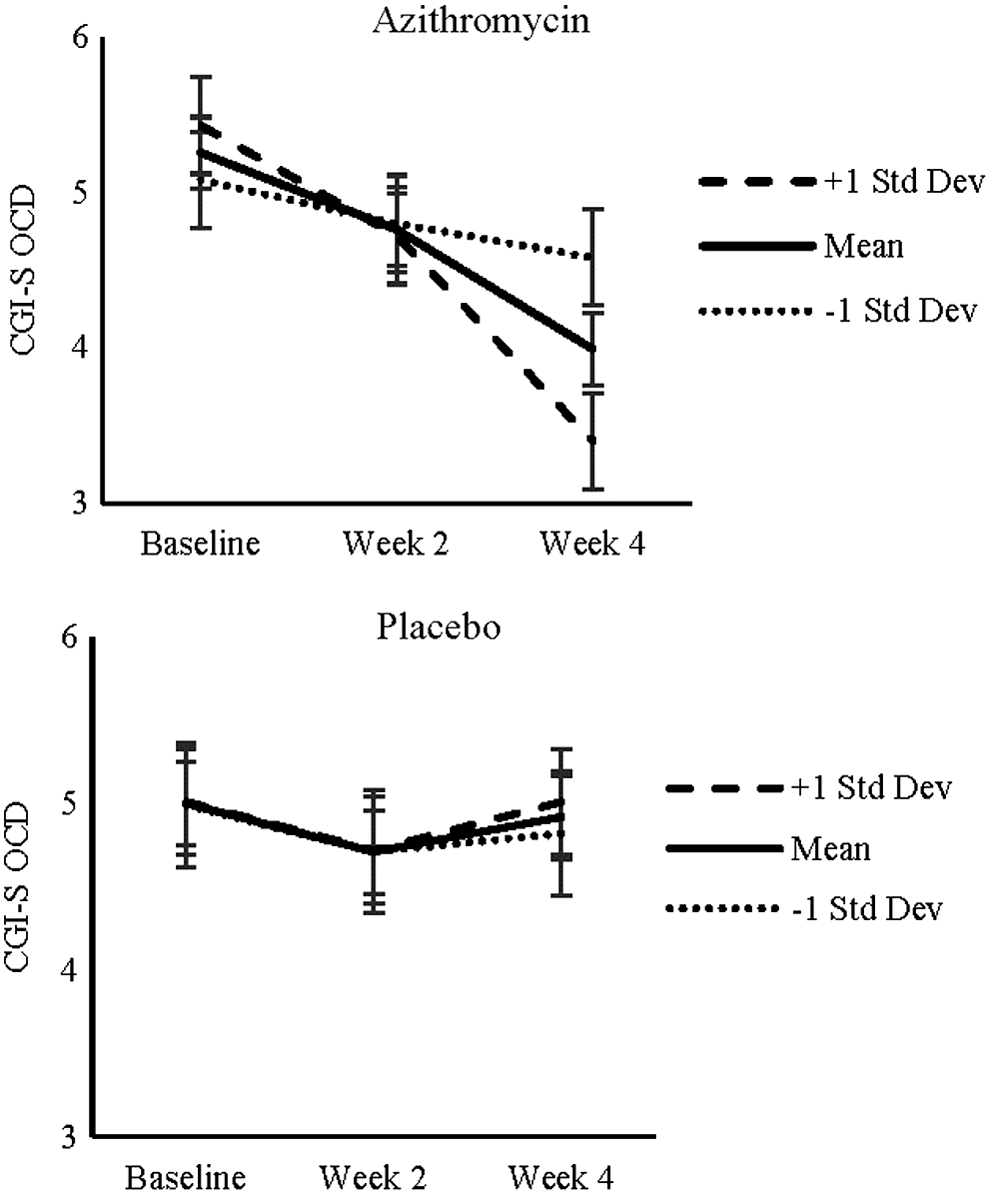
Impact of tic severity on treatment outcome in PANDAS children with tics. PANDAS, Pediatric Autoimmune Neuropsychiatric Syndrome Associated with Streptococcus.
With average levels of baseline tic severity, youth in the azithromycin group showed a significant improvement on the CGI-S OCD at the end of week 2 (p = 0.020) and week 4 (p < 0.001). This pattern was even stronger for youth with higher levels of baseline tic severity (p = 0.030 and p < 0.001 respectively). Youth who scored one standard deviation below the mean on baseline YGTSS showed a poorer response, with no significant improvement at the end of week 2 (p = 0.324) or week 4 (p = 0.084). Baseline YGTSS did not moderate outcome in the placebo group (all p-values >0.228). Similar to the primary outcome analysis, the three-way interaction between group, time, and baseline YGTSS score was not significant in predicting outcome on the CY-BOCS (p = 0.385).
Treatment responders and nonresponders within the azithromycin group were compared to examine clinical differences. There were few demographic or clinical differences between treatment responders and nonresponders. Participants were considered treatment responders if they had a ≥30% reduction on CYBOCS from basline to end of week 4 or scored as very much or much improved on the CGI-I OCD at end of week 4. Although not significant, fewer treatment responders in the azithromycin group (22.22%, n = 2) presented with psychotic features in comparison to nonresponders (50.00%, n = 4; p = 0.247). Seven of nine responders (77.78%) were reported to have a GAS trigger, three of which also had evidence of URI and one who also had M. pneumonia (Table 5). For nonresponders in the azithromycin group, 37.50% (n = 3) had a GAS trigger, 12.50% (n = 1) with a GAS and URI trigger, 37.50% (n = 3) with a URI trigger, and 12.50% (n = 1) with a M. pneumonia trigger.
Participants were classified as a responder if they were either “much improved/very much improved” on CGII OCD OR 30% reduction on CY-BOCS.
Based on medical record review and parent report.
IgG, immunoglobulin G; GAS, group A streptococcal; OCD, obsessive–compulsive disorder.
There was not a significant difference in study medication (p = 0.337) and probiotic (p = 0.526) compliance between treatment responders (M = 100.00, SD = 0.00, and M = 97.45, SD = 4.82) and nonresponders (M = 99.49, SD = 1.34, and M = 94.28, SD = 11.73).
The symptoms of seven of the nine azithromycin responders and three nonresponders were considered to be new onset, first episode. The symptoms of one responder and four nonresponders were considered to be a relapse of previously resolved symptoms, and one responder and one nonresponder symptoms were considered to have an acute and severe exacerbation of previous subclinical symptoms. There was no significant differences between responders and nonresponders in terms of onset characteristics (p = 0.187). No characteristics were found to influence outcome (Table 5).
There was no significant differences in demographics or presentation of symptoms between responders and nonresponders in the placebo group. Two out of the three placebo responders (66.67%) had a GAS trigger. Of the 11 nonresponders in the placebo group, 6 (54.55%) had a GAS trigger and 2 (18.18%) had a mycoplasma trigger. There was not a significant difference in study medication (p = 0.341) and probiotic (p = 0.244) compliance between placebo responders (M = 100.00, SD = 0.00, and M = 100.00, SD = 0.00) and nonresponders (M = 99.68, SD = 1.06, and M = 92.17, SD = 10.75). The symptoms of all three of the responders in the placebo group and 9 of the 11 nonresponders were considered to be new onset, first episode. The symptoms of two nonresponders were considered to be an acute exacerbation of previously subclinical symptoms. There were no significant differences between responders and nonresponders in terms of onset characteristics (p = 0.604).
Tolerability
Azithromycin was well tolerated, with few group differences in reported AEs (Table 6). There was significantly higher incidences of loose stools in the azithromycin group in comparison to the placebo group (52.94% compared with 7.14%, p = 0.009), and significantly lower levels of constipation (0.00% compared with 35.71%, p = 0.012).
p < 0.05.
There were no significant group differences in reference to the change in pulse (p = 0.647) or weight (p = 0.347), but a trend toward significance in reference to change in ECG QTc (p = 0.060) from baseline to week 4. Mean pulse increase from baseline to end of week 4 was not significantly different between groups (azithromycin group M = 5.65, SD = 13.76; placebo group M = 8.46, SD = 11.51). Nine participants (29.03%; 4 in the azithromycin group, 3 in the placebo group) had heart rates above 100 beats per minute at baseline. At the end of week 6, six of the nine (one in the azithromycin group, five in the placebo group) with elevated heart rate at baseline continued to have elevated heart rate at end of week 4 and five participants who did not have elevated heart rate at baseline had elevated heart rates at the end of week 4 (four in the azithromycin group, one in the placebo group).
When examining the within group effect, participants in the azithromycin group did not show any significant change in weight (p = 0.344); however, they did show a trend toward an increase in pulse from baseline to week 4 (90.47, SD = 15.22 to 97.23, SD = 12.76; p = 0.058), and a significant increase in ECG QTc (414.59, SD = 19.39 to 427.65, SD = 16.32; p = 0.007). Four participants in the azithromycin group had QTc 440–460 ms at end of week 4, which is considered to be borderline (Moss 1993), two of whom presented with borderline QTc at baseline. One participant in the placebo group was considered to have a borderline QTc at end of week 4, but also presented with a borderline QTc at baseline. No participants had >460 ms QTc at any point. ECGs did not control for diurnal variations or time from last dose received. All AEs were mild and did not require study medication discontinuation.
Discussion
This pilot trial examined the efficacy and safety of azithromycin to treat acute-onset pediatric OCD. As previously reported on most of this sample (Murphy et al. 2015b), characteristics of these youth highlight the severity and impairment of the presenting OCD with multiple domains affected, including movement, sensory, mood, feeding, and cognition (Murphy et al. 2015b). This study did not require an infectious trigger, but many (61.29%) reported GAS as a trigger and inasmuch would meet the criteria for PANDAS.
OCD severity (as measured by the CGI-S) showed improvement with separation from the placebo arm occurring after end of week 2. Mood improvement was also observed. No group differences in other measures were observed in this 4-week trial. Tic severity appeared to moderate treatment outcome for azithromycin, with youth who presented with average to higher tic severity showing enhanced treatment response in comparison to those with minimal tic symptoms. OCD with a higher tic severity may represent a more treatment-responsive phenotype that deserves further study; however, it is too soon to suggest treatment recommendations based on this preliminary observation.
Both study arms showed improvement over this 4-week randomized trial, with a greater reduction in OCD symptoms and greater number of responders in the azithromycin group. At least three potential mechanisms may explain the improvement in the placebo arm. One possibility is the traditional placebo response. Pediatric OCD SSRI studies report placebo response rates typically around 25%–41% with a pooled difference of four points on the CYBOCS (Geller et al. 2003), highlighting that placebo response rates are not low in pediatric OCD. The second possibility is that the natural course of acute-onset OCD may be more episodic or waxing and waning than chronic OCD. Our subjects were young (mean age 8.26, SD = 2.78) and had a very short duration of illness (mean duration of illness 9.76 weeks, SD = 6.65) by the time of study enrollment, especially in the placebo group. Even before study enrollment, some participants reported symptom improvement from time of onset, with the worst-ever symptoms typically occurring 3 days after the acute onset with some degree of improvement over the next week or so. The third possibility is that since both groups received a probiotic twice daily, the probiotic may have provided some therapeutic benefit. Some studies suggest that probiotics may decrease anxiety (Neufeld et al. 2011; Mayer et al. 2014), however, the influence on OCD severity has not been evaluated.
Although the study was limited in determining if onset characteristics determined response, there was a suggestion that subjects with new-onset, first-episode OCD may have been more likely to respond than those with a recurrent OCD episode. Those with recurrent OCD may need longer or additional treatment compared with new-onset subjects. This will be interesting to examine in the future.
Azithromycin was well tolerated with minimal complaints of AEs. Higher rates of loose stools were reported, but none at a severe level. One report of possible bacterial resistance was noted during the study, but antimicrobial resistance was not studied at a laboratory level. Although patients with PANS have not been documented to later develop rheumatic carditis, macrolide resistance could have the serious consequence of acute rheumatic fever, therefore, this possibility should be monitored (Logan et al. 2012). One primary concern is that the azithromycin group showed an average QTc increase of 13.06 ms (range −28 to 48) on the end of week 4 ECG. All ECGs were reviewed by Cardiology and were considered to be clinically normal.
Generalizability of findings may be limited by inclusion and exclusion criteria that are too specific as few individuals met critera for inclusion. While the present is a small pilot study, limited by power, the results provide some support for the benefit of antibiotic therapy in the treatment of OCD and mood in youth with PANS/PANDAS. However, youth receiving long-term treatment with azithromycin should be monitored to address possible QTc prolongation. Additionally, no correction for the number of statistical tests conducted were made, as such, the risk of a type 1 error is inflated.
Due to inherent issues with the CY-BOCS rating in young children, we did not find this rating as sensitive as the CGI-S for assessing severity. Many children went from 8 hours or more per day involved in obsessions and compulsions to perhaps 3–4 hours per day with little changes in CY-BOCS scores. Most young children made no effort to control or resist symptoms and these items alone account for 16 points of the 40-point maximum score for the CY-BOCS. We saw some evidence that neurocognitive symptoms respond more slowly to treatment, but this will need further investigation in a larger study. In addition, the CALS and SCARED are not validated for use in 4–5 year olds and 4–7 year olds, respectively, which may have impacted findings.
Conclusion
Within these limitations, these data provide support for the feasibility and preliminary efficacy of azithromycin treatment for youth with acute-onset OCD meeting PANS criteria, especially those with elevated levels of both OCD and tic symptoms. Further testing in a fully powered trial that is able to examine treatment moderators is warranted.
Clinical Significance
Given that the treatment with azithromycin of acute-onset OCD appeared safe and well tolerated, and preliminary data found responders at week 4 (52.9% of the active group vs. 21.4% in the placebo group), antibiotic therapy may be a useful option for those with recent-, acute-, and severe-onset OCD. Risks should be weighed against benefits until utility of this treatment option is comprehensively examined.
Contributors
T.M. is the lead investigator, designed the study, oversaw trial implementation and data interpretation, is the principle writer of the article, and is the lead investigator on the grant; E.B. was responsible for implementing trial details, and contributed to writing and critical review of the article; C.J. was responsible for primary data analysis, produced the figures, interpreted the data, and contributed to writing and critical review of the article; C.P.A. contributed to writing and critical review of the article; B.M. was responsible for data analysis, and critically reviewed the article; A.B.L., critically reviewed the article; and E.A.S., critically reviewed the article.
Footnotes
Acknowledgments
The authors thank Laura Rodriguez, Priyal Patel, Allison Kennel, Henry Storch, MD, and Camille Hanks for providing research assistance.
Disclosures
Dr. Murphy reports grants from Auspex Pharmaceuticals, grants from National Institute of Mental Health, Shire Pharmaceuticals, Pfizer, Inc., F. Hoffmann-La Roche Ltd., AstraZeneca Pharmaceuticals, Centers for Disease Control, Massachusetts General Hospital, Sunovion Pharmaceuticals, Neurocrine Biosciences, Psyadon Pharmaceuticals, and PANDAS Network, and personal fees from International OCD Foundation, Tourette Syndrome Association.
Dr. Storch receives research support from NIH, Agency for Healthcare Research and Quality, International OCD Foundation, and All Children's Hospital Research Foundation. He has received royalties from Elsevier Publications, Springer Publications, American Psychological Association, Wiley, Inc., and Lawrence Erlbaum. He is a consultant for Prophase, Inc. and Rijuin Hospital, China. Dr. Storch is on the Speaker's Bureau and Scientific Advisory Board for the International OCD Foundation. He receives research support from the All Children's Hospital Guild Endowed Chair.
Dr. Lewin receives research support from All Children's Hospital Research Foundation, the Centers for Disease Control and Prevention, and the International OCD Foundation. He is on the speaker's bureau for the Tourette Association of America and the International OCD Foundation. He has received travel support from Tourette Association of America, American Psychological Association, Anxiety and Depression Association of America, NIMH, and the American Board of Professional Psychology. He has received consulting fees from Bracket and Prophase, Inc. He receives book royalties from Springer, and has received honoraria from Oxford University Press, Children's Tumor Foundation, and University of Central Oklahoma. Dr. Lewin is on the Scientific & Clinical Advisory Board for the International OCD Foundation and the Board of Directors for the Society for Clinical Child and Adolescent Psychology and the American Board of Clinical Child and Adolescent Psychology. Ms. Brennan, Dr. Parker-Athill, Dr. Johnco, and Dr. Miladinovic report no financial disclosures.