
Abstract
Introduction:
Pediatric Acute-onset Neuropsychiatric Syndrome (PANS) is characterized by the sudden onset of severe obsessive-compulsive symptoms and/or eating restriction along with at least two coinciding neuropsychiatric symptoms. When associated with group A Streptococcus, the syndrome is labeled Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal infections (PANDAS). An abnormal immune response to infection and subsequent neuroinflammation is postulated to play an etiologic role. We evaluated the impact of nonsteroidal anti-inflammatory drug (NSAID) treatment on flare duration in PANS/PANDAS.
Methods:
Patient inclusion criteria: Patients were included if they had at least one neuropsychiatric deterioration (“flare”) that met strict PANS/PANDAS research criteria and for which flare duration could be assessed. Flare inclusion criteria: Any flare that started before October 15, 2016 was included and followed until the flare resolved or until the end of our data collection (November 1, 2016). Flare exclusion criteria: Flares were excluded if they were incompletely resolved, treated with aggressive immunomodulation, or treated with NSAIDs late (>30 days of flare onset). Ninety-five patients met study inclusion criteria and collectively experienced 390 flares that met flare criteria. Data were analyzed using multilevel linear models, adjusting for demographics, disease, and treatment covariates.
Results:
NSAID use was associated with a significantly shorter flare duration. Flares not treated with NSAIDs had a mean duration of approximately 12.2 weeks (95% CI: 9.3–15.1). Flares that occurred while the child was on NSAID maintenance therapy were approximately 4 weeks shorter than flares not managed with NSAIDs (95% CI: 1.85–6.24; p < 0.0001). Flares treated with NSAIDs within 30 days of flare onset were approximately 2.6 weeks shorter than flares not managed with NSAIDs (95% CI: 0.43–4.68; p = 0.02). Flares treated prophylactically and those treated early with NSAIDs did not differ in duration (p = 0.26). Among the flares that received NSAID treatment within the first 30 days, earlier intervention was modestly associated with shorter flare durations (i.e., for each day that NSAID treatment was delayed, flare duration increased by 0.18 weeks; 95% CI: 0.03–0.33; p = 0.02), though it was not statistically significant after controlling for covariates (p = 0.06).
Conclusion:
NSAIDs given prophylactically or within 30 days of flare onset may shorten neuropsychiatric symptom duration in patients with new-onset and relapsing/remitting PANS and PANDAS. A randomized placebo-control clinical trial of NSAIDs in PANS is warranted to formally assess treatment efficacy.
Introduction
P
The Stanford PANS Program, created to research the etiology of and treatment for this disorder, conducts a community-based interdisciplinary clinic that is designed to evaluate and treat youth with suspected PANS or PANDAS. Our program accepts patients who live locally (83% live within 90 miles). For our local cohort, we require frequent follow-up visits (every 1–2 weeks during flare and every 4–12 weeks during remissions).
In our clinic, patients' PANS symptoms often relapse and remit. Relapses (acute deteriorations in neuropsychiatric symptoms, referred to as “flares”) can be severely debilitating, often lasting weeks to months. As a flare resolves, neuropsychiatric symptoms improve; however, patients often report persistent fatigue, pain, and arthritis, similar to what is noted in other inflammatory conditions, including systemic lupus erythematosus (Benseler and Silverman 2007; Petri et al. 2016).
Treatment of PANS flares includes eliminating associated factors contributing to inflammation (e.g., infection), cognitive behavioral therapy (CBT), psychiatric medications, and addressing inflammation itself. Consensus guidelines for immunomodulatory interventions have been developed, recommending therapies depending on disease severity and course (Frankovich et al. 2017). The use of nonsteroidal anti-inflammatory drugs (NSAIDs) is included in these recommendations which are based on clinical experience, as there are limited reports on the efficacy of NSAIDs in PANS (Spartz et al. 2017).
When our PANS clinic opened in September 2012, clinicians initially prescribed NSAIDs for arthritis and pain, as this is the standard of care for juvenile arthritis. Interestingly, in addition to improvement in joint pain, temporal associations between NSAID introduction and psychiatric symptom improvement were noted (Spartz et al. 2017). These observations are congruent with burgeoning anecdotal experiences shared between parents of affected youth in online PANS/PANDAS forums.
To further investigate the link between NSAID use and PANS flare characteristics, we designed this retrospective case review with the following two aims (developed a priori): (1) to assess the impact of NSAID treatment on flare duration in patients with new-onset PANS and relapsing/remitting illness (primary analysis); (2) to evaluate the impact of timing of NSAID introduction on flare duration.
Methods
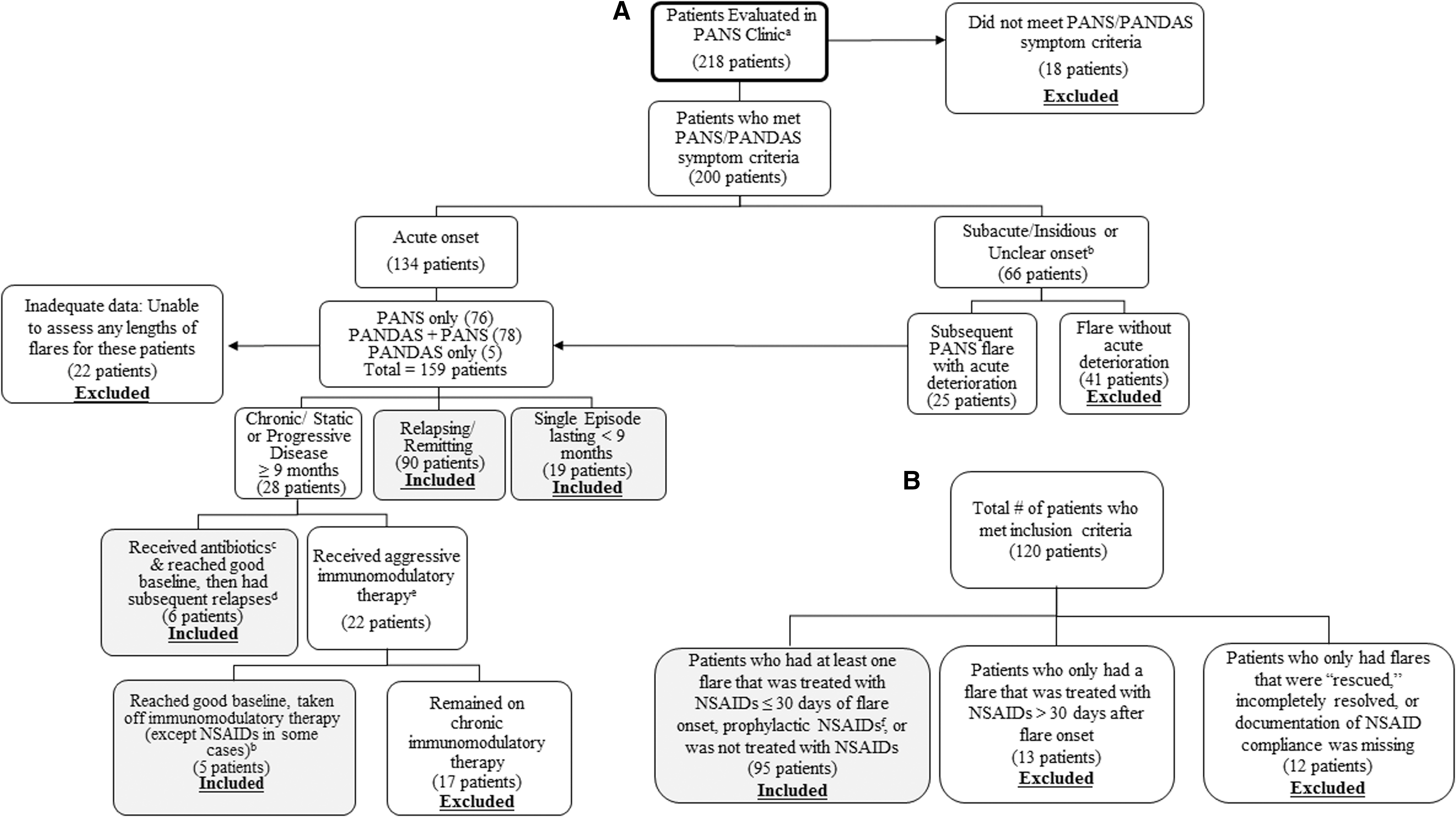
We reviewed clinical electronic medical records (EMR) of 218 consecutive patients of the Stanford PANS Clinic between September 1, 2012 and October 15, 2016 or by our PANS psychiatrist (MT) before starting the formal multidisciplinary clinic (Fig. 1A). Patients were prescreened before registering with our clinic to increase the probability that patients seen would meet criteria for PANS or PANDAS. The Stanford Panel on Human Subjects Institutional Review board approved this study. All definitions, inclusion criteria, exclusion criteria, statistical methods, and covariates listed later were developed a priori.
Definitions of clinical course
Relapsing/remitting course is defined as an abrupt onset of symptom relapses (“flares”) followed by an approximate return to 90%–95% of preflare baseline functioning without the need for aggressive immunomodulatory therapy (e.g., intravenous immunoglobulin [IVIG], mycophenolate mofetil, plasma exchange, rituximab, etc.). Chronic-static course is defined as a course with persistent unchanging PANS symptoms lasting at least 9 months. Progressive disease is a chronic course in which PANS symptoms worsen in intensity over time.
Patient inclusion criteria
Patients were included in the analysis if they had at least one acute neuropsychiatric deterioration (“flare”) that strictly met both research criteria for PANS or PANDAS (Swedo et al. 1998, 2012; Chang et al. 2015) and flare inclusion criteria; and for which there was adequate documentation to assess flare duration (Fig. 1A). Patients with a single flare or relapsing/remitting course were included in the analyses (Fig. 1A). As noted in Figure 1A, eleven patients with chronic-static or progressive disease were included in the study because they eventually returned to their pre-PANS baseline without requiring chronic immunomodulatory therapy. These patients experienced subsequent deteriorations, which were included in the flare analyses.
Patient exclusion criteria
Patients were excluded if they required aggressive disease-modifying therapies such as rituximab, cyclophosphamide, mycophenolate mofetil, and/or chronic immunomodulatory therapy to sustain baseline functioning (i.e., monthly IVIG and/or monthly intravenous [IV] methylprednisolone pulses). Patients who remained chronic-static or progressive were excluded from the study (Fig. 1).
Study entry date
Study entry begins at the time of the first clearly documented neuropsychiatric deterioration (“flare”) that meets strict PANS/PANDAS research criteria and flare inclusion criteria. This “first flare” may have occurred before entry/registration in our PANS clinic. Study entry is therefore not necessarily coterminous with entry/registration in the PANS clinic.
Definition of flare duration
A flare is defined as an acute neuropsychiatric deterioration that meets strict PANS or PANDAS research criteria. Flares and flare durations were identified by using our standard psychiatric and neurological clinical assessments (documented in the EMR), our PANS questionnaires, which are based on tracking forms used in the recent PANDAS clinical trial (Williams et al. 2016), the PANS Global Impairment Scale, and documented communications (emails and phone calls) between parents and providers. The PANS Global Impairment Scale was developed by Dr. James Leckman and colleagues and the National Institute of Mental Health (personal communication). A flare was considered resolved when the patient was functioning at or near their preflare baseline based on clinician documentation, patient questionnaires, and parent recall.
Flare inclusion criteria
Any flare that started before October 15, 2016 was included and followed until the flare resolved or until the end of our data collection (November 1, 2016). Included flares could have occurred either during treatment in our PANS clinic or before clinic entry if there was adequate historical documentation to determine flare duration (weeks). Historical documentation reviewed includes medical records, therapy records, and patient questionnaires.
Flare exclusion criteria
We created exclusion criteria for individual patients and for individual flares. For example, a patient could have been eligible for study inclusion, while one or more of the patient's flares were excluded.
“Rescued” flares
“Rescued” flares are those that were severe enough to be treated with IVIG, high-dose IV methylprednisolone (30 mg/kg, maximum: 1 g/dose), or plasma exchange, in addition to NSAIDs, oral corticosteroids, and/or antibiotics. “Rescued” flares were excluded from the analyses because they required escalating immunomodulatory treatment to achieve resolution and were therefore clinically distinct from other flares (n = 61).
Incompletely resolved flares
Flares that were unresolved before a subsequent deterioration were excluded (n = 14).
Late NSAID-treated flares
When the initiation of NSAID treatment for a flare was more than 30 days after the flare onset, the flare was excluded (n = 44). These flares were not included in the analysis for two reasons: First, the amount of time until NSAID initiation is linearly related to flare duration. Therefore, flares with late NSAID use would likely last longer than other flares for reasons that are inconsequential to the analysis. Second, we hypothesized that flares treated in the late phase of disease may not be as responsive to NSAIDs, a phenomenon seen in other inflammatory diseases such as juvenile arthritis (Wallace 2006).
Other excluded flares
Flares that occurred fewer than 50 days after a single treatment with IVIG, a pulse of high-dose IV methylprednisolone (30 mg/kg), or plasma exchange were excluded. This time-frame was chosen for two reasons. First, we expected that these medications may exert effects for 50 days based on the following logic: (1) the half-life of immunoglobulin G levels in healthy patients is 3–4 weeks, but longer for other disorders (Silvergleid and Ballow 2016) and (2) methylprednisolone pulse effects often last 2–6 weeks in other autoimmune conditions, which is why many rheumatologic protocols use monthly methylprednisolone pulse regimes (Barile-Fabris et al. 2005; Then Bergh et al. 2006; Huber et al. 2012; Li et al. 2012). Second, many patients in our clinic experience a recrudescence of symptoms approximately 3–4 weeks after IVIG and/or IV methylprednisolone. It was unclear whether recrudescence of symptoms during this 50 day period was due to medication waning or a new onset flare, and we therefore excluded these flares.
Lastly, eight flares were excluded because the timing of NSAID initiation was not recorded, and three flares were excluded because patient compliance with NSAID prescription was not documented.
Definition of time since onset of PANS illness
Time since onset of PANS illness is defined as the number of weeks since the onset of the patient's initial neuropsychiatric deterioration that met PANS or PANDAS symptom criteria. For 79 out of 95 (83%) patients included in the study, the initial neuropsychiatric deterioration met strict PANS or PANDAS onset criteria (acute onset ≤72 hours). For the remaining 16 patients, the acuity of their initial flare onset was unclear. These 16 patients were still included in the study because they experienced a future flare that clearly met strict PANS or PANDAS research criteria.
Definition of NSAID treatment
NSAID treatment is defined as the use of NSAIDs that was started after the flare onset date and was prescribed for at least 7 days during a PANS flare. Prophylactic NSAID treatment is defined as the use of NSAIDs before the flare onset date, with subsequent use throughout the duration of the flare. Early NSAID treatment describes the introduction of NSAIDs within 30 days of the flare onset.
NSAID treatment protocol
PANS clinic patients are evaluated and treated for underlying infections on presentation to the clinic, in accordance with PANS consensus diagnostic guidelines (Chang et al. 2015) and PANS infection treatment guidelines (Cooperstock et al. 2017). Before January 2015, our clinicians did not routinely prescribe NSAIDs for treatment of PANS flares, but rather offered them to treat arthritis and/or pain. Starting January 2015, clinicians routinely recommended NSAIDs to treat new-onset PANS or PANS flares. Clinicians also offered NSAIDs for treatment of arthritis, pain, or residual neuropsychiatric symptoms. Naproxen was dosed at 10 mg/kg every 12 hours (maximum: 500 mg/dose). Ibuprofen was dosed at 10 mg/kg every 6–8 hours (maximum: 600 mg/dose). Sulindac was dosed at 2–4 mg/kg every 12 hours (maximum: 6 mg/kg/day, adult maximum dose = 400 mg/day divided twice a day). Celecoxib was dosed at 50–100 mg twice a day. These are the same dosage regimens used by pediatric rheumatologists to treat other inflammatory disorders. Many of our patients with PANS have fluid restriction (as determined by clinical history, high specific gravity on urine analyses, and/or high BUN/Cr ratio). With these patients, we reduced the dose or withheld NSAIDs. We monitored for headaches, allergic reactions, bruising, gastrointestinal side effects, transaminitis, renal function, and hematuria. Liver enzymes, renal function tests, and urinalysis were obtained every 3–6 months for patients on chronic NSAIDs.
Statistical analyses
For analyses that use data with repeated observations on the same patient (Table 3), we employed a multilevel linear model that accounts for within-subject correlation. For analyses with no repeated measures (i.e., one flare per patient; Table 4), we used a standard general linear model. We report the results of an initial model in which the target variable(s) of interest are evaluated without covariates, as are the results with the full complement of putative covariates. Both the multilevel linear and standard general linear models were adjusted for the following covariates: sex, age at flare onset, weeks since onset of PANS illness, antibiotic treatment during flare, prophylactic antibiotics on board before flare, previous flare treated with immunomodulation (IVIG, IV methylprednisolone, and/or plasma exchange), oral corticosteroids, number of psychiatric medications, and use of CBT during flare. Results of the models are presented as the regression parameter estimate and 95% confidence interval (CI); this is interpreted as the change in the dependent variable associated with a one-unit increase in the independent variable. Given that maximum likelihood estimation cannot be relied on to accommodate missing X-side data, multiple imputation routines in Mplus software (Muthén and Muthén 2012) were used to generate pooled results across 20 datasets, accounting for the multilevel structure of the data and the distribution of the variables. Given the exploratory nature of the analyses, p-values were not adjusted for multiple comparisons.
Results
Of the 120 eligible patients (Fig. 1B), 95 patients met all inclusion criteria and were included in the current analyses (Table 1). Thirteen patients were excluded because they received only late NSAID treatment, and 12 patients were excluded because the flares were “rescued,” the flares were incompletely resolved, or documentation of NSAID use was missing or unclear (Fig. 1B).
Some missing data: eating restriction and behavioral regression, n = 1. Academic deterioration, n = 4.
Mood dysregulation, including depression and/or emotional lability.
PANS, Pediatric Acute-onset Neuropsychiatric Syndrome; NSAIDs, nonsteroidal anti-inflammatory drugs; NP, number of patients; NF, number of flares.
Of the 517 eligible flares, 390 met flare inclusion criteria and were included in the current analyses (Table 2). The majority of flares were not treated with NSAIDs (n = 271), followed by prophylactic NSAID treatment (n = 76) and early NSAID treatment (n = 43). Accounting for multiple observations per individual, there were some significant differences (p < 0.05) among flare groups in covariates (Table 2).
Significant differences between groups are demarcated by [group 1]:[group2], for example, P:N indicates that the Prophylactic and Not Treated groups differed significantly.
High-dose IVIG, intravenous methylprednisolone pulse(s) (30 mg/kg), or plasma exchange.
Common infections treated during flare include group A Streptococcus, sinusitis, otitis media, Mycoplasma pneumoniae, etc.
Contents of table are estimated values (with standard errors in parentheses) for the repeated-measures models, accounting for multiple observations per subject.
SE, standard error; P, prophylactic NSAIDs; E, treated with NSAIDs early (≤30 days of flare onset); N, not treated with NSAIDs; IVIG, intravenous immunoglobulin.
Both prophylactic and early NSAID treatment were associated with a significantly shorter flare duration than no NSAID use. Flares not treated with NSAIDs lasted approximately 12.2 weeks (95% CI: 9.3–15.1 weeks). Prophylactically treated flares were about 4 weeks shorter than flares not treated with NSAIDs (95% CI: 1.85–6.24, p < 0.0001), and early treated flares were about 2.5 weeks shorter (95% CI: 0.43–4.68, p = 0.018) (Table 3). Flare duration did not significantly differ between prophylactically and early treated NSAID flares (p = 0.26).
High-dose IVIG, intravenous methylprednisolone pulse(s) (30 mg/kg), or plasma exchange.
Common infections treated during flare include group A Streptococcus, sinusitis, otitis media, Mycoplasma pneumoniae, etc.
p < 0.01, * p < 0.05
Results are from a multilevel model; the unstandardized B value is interpreted as the expected change in flare duration, with a one-unit change in the independent variable. For NSAID use, this is interpreted as the difference between the level of NSAID use (Early or Prophylactic) and the None category, which is the reference. For other categorical variables, the second category is the reference. For example, in the final model, early NSAID use is associated with a duration that is 2.56 weeks shorter than when no NSAID was used, whereas prophylactic NSAID use is associated with a duration that is 4.05 weeks shorter. Prophylactic and Early treatment did not differ from one another in flare duration: Final model, B(SE) = 1.49 (1.32), p = 0.26.
B, beta; CI, confidence interval.
Given that early NSAID treatment is associated with shorter PANS flares, we hypothesized that a relationship may exist between the timing of NSAID introduction and flare duration. Among the early treated flares (within 30 days of flare onset, nf = 43), the majority of patients had only one flare (np = 36). Thus, the first flare for each patient was selected, resulting in a sample of 36 flares from 36 individuals. Within these early treated flares, the timing of NSAID was significantly associated with flare duration, such that each day that NSAID initiation was delayed was associated with an increase in flare duration of 0.18 weeks (95% CI: 0.03–0.33, p = 0.02) (Table 4). When all of the covariates were added to the model, this relationship became nonsignificant (p = 0.06). However the magnitude of the relationship remained unchanged, suggesting inadequate power due to the relatively small sample. When only covariates with at least marginal significance (p < 0.20) were retained, the effect of NSAID timing was again of a similar magnitude, but it was statistically significant (p = 0.016).
Number of days from flare onset to NSAID initiation.
High-dose IVIG, intravenous methylprednisolone pulse(s) (30 mg/kg), or plasma exchange.
Common infections treated during flare include group A Streptococcus, sinusitis, otitis media, Mycoplasma pneumoniae, etc.
p < 0.05
Results are from a standard general linear model with no repeated observations; the unstandardized B value is interpreted as the expected change in flare duration, with a one-unit change in the independent variable. For example, in the final model, for every day that NSAID initiation is delayed, the flare duration increases by 0.17 weeks. For categorical variables, the second category is the reference.
Of the 57 patients included in the analysis who had at least one flare treated with NSAIDs that met flare inclusion criteria, 11 (19%) patients had transient side effects. No patients developed clinically significant side effects. Side effects included abdominal pain (n = 5), skin rash (n = 1), bruising (n = 1), proteinuria (n = 3), and clinically insignificant transaminitis (n = 1). Abdominal pain self-resolved after stopping or reducing NSAID doses in four of the five patients; of these four, two patients tolerated NSAIDs when given to treat a subsequent PANS flare. The patient whose abdominal pain did not resolve after NSAID removal was believed to have abdominal pain amplification; when reintroducing the NSAID, the abdominal pain did not worsen. Skin rash and bruising self-resolved after stopping or reducing NSAID doses, and both of these patients tolerated NSAIDs when given to treat a subsequent PANS flare. Of the three patients with proteinuria, one had elevated urine protein/creatinine ratio (0.3) on a morning void, which resolved after removal of NSAIDs. In the other two patients, it is unclear whether the mild proteinuria (+1) observed on afternoon urinalyses was due to NSAIDs or orthostatic proteinuria. In one of these patients, the proteinuria resolved despite continued NSAID use. The other patient was lost to follow-up. One patient developed mildly elevated liver enzymes while on NSAIDs (AST = 53, normal range for age <50; ALT = 67, normal range for age <60); this patient had a concurrent viral illness that was believed to contribute to the transaminitis. The transaminitis self-resolved despite continued NSAID use.
Discussion
This is the first study to assess the impact of NSAIDs on flare duration in patients with PANS and/or PANDAS. Approximately one-third of the flares included in this study were treated with NSAIDs early or prophylactically. PANS flares treated with NSAIDs early or prophylactically appear to resolve more quickly than flares not treated with NSAIDs. Furthermore, earlier NSAID introduction was associated with faster improvement. This effect was not significant after entering covariates, which is likely a result of inadequate power; regardless of this, the effect was small, perhaps due to the restricted range of time to initiation (up to 30 days). Together, these data suggest that NSAID treatment may be superior to nontreatment and earlier initiation may be beneficial. Our findings have clear clinical importance since patients often present to specialty clinics several days to weeks after symptom onset, and they may still benefit from NSAID treatment.
Flare duration did not differ between flares treated with prophylactic NSAIDs and those treated with NSAIDs within 30 days of flare onset. It is unclear from this analysis whether this is a consequence of statistical power, or whether these results suggest that both treatment approaches may be similarly effective. In addition, it is likely that patients who received prophylactic NSAIDs were in a different disease state than those who received the NSAID after the flare began (i.e., those receiving prophylactic NSAID may have had arthritis or had a history of deteriorating after NSAIDs were stopped).
No patients developed clinically significant side effects; however, 19% reported transient side effects from NSAIDs. Many of the patients who did not tolerate NSAIDs tolerated a subsequent NSAID trial given for a future PANS flare. Therefore, an initial intolerance for NSAIDs should not dissuade NSAID use to treat a future PANS flare.
Wide variability in flare duration was observed in this study, which may be explained by the heterogeneity of the patient and flare groups with respect to disease severity, disease trajectory at the time of NSAID introduction, and flare trigger (i.e., bacterial, viral, etc.). Some patients in our clinic experience a dramatic and rapid response to NSAIDs, whereas others exhibit no response to NSAIDs (Spartz et al. 2017). Variability in response is also observed within individual patients; an individual may exhibit little-to-no response to an initial NSAID trial, but may respond to NSAIDs in a future milder flare (Spartz et al. 2017). These clinical observations, coupled with our current findings that prophylactic NSAIDs are associated with shorter flares, suggest that failure to have an initial response should not dissuade NSAID use for future flares. However, formal clinical trials are required to identify the predictors of response and to evaluate the risk-to-benefit ratio systematically.
Inflammation may play a role in triggering and/or exacerbating PANS/PANDAS symptoms in individuals. Animal and human research suggests that the adaptive immune response (autoantibodies and Th17 cells), neuroinflammation, and microglial activation all may contribute to the pathogenesis of poststreptococcal neuropsychiatric diseases (Kirvan et al. 2003, 2006a, 2006b; 2007; Hoffman et al. 2004; Yaddanapudi et al. 2010; Brimberg et al. 2012; Cox et al. 2013; Lotan et al. 2014; Kumar et al. 2015; Macrì et al. 2015; Williams and Swedo 2015; Xu et al. 2015; Carapetis et al. 2016; Cutforth et al. 2016; Dileepan et al. 2016). In addition, a positron emission tomography (PET) imaging study found greater microglial activation in patients with PANDAS compared with controls (Kumar et al. 2015). Another study found an association between the tumor necrosis factor (TNF)-α gene −308G/A polymorphism and patients with PANDAS (Luleyap et al. 2013). A recent animal model designed to evaluate the relationship between nasopharyngeal infection and neuroinflammation showed that multiple intranasal infections with live GAS generate GAS-specific Th17 cells that migrate along olfactory sensory axons into the brain. Migration of Th17 cells into the brain was associated with neurovascular damage, including increased blood-brain barrier (BBB) permeability and neuroinflammation (Dileepan et al. 2016). NSAIDs inhibit the cyclooxygenase (COX) enzyme, which influences multiple inflammatory mechanisms. Notably, human, postmortem, and animal studies show that NSAIDs can affect all the inflammatory pathways mentioned earlier, including reducing the Th17 response (Chizzolini et al. 2008; Napolitani et al. 2009), reducing TNF-α (Iñiguez et al. 1999, 2010), reducing microglial activation (Mackenzie and Munoz 1998; Klegeris et al. 2004), and reducing BBB permeability (Candelario-Jalil et al. 2007; Brooks et al. 2008). Of importance, we do not know whether shortened PANS flare durations associated with NSAIDs are direct effects (due to the anti-inflammatory properties of NSAIDs on neuroinflammation) or indirect effects (due to reduction in BBB permeability, thus reducing autoantibody access into the central nervous system).
Interestingly, NSAIDs have been observed to be beneficial in other psychiatric conditions. Two clinical trials in adult patients with OC disorder showed celecoxib to be helpful in reducing OC symptoms (Sayyah et al. 2011; Shalbafan et al. 2015). In addition, clinical trials have suggested some benefit of NSAIDs in depression, bipolar disorder, and schizophrenia (Müller et al. 2004; Abbasi et al. 2012; Arabzadeh et al. 2015).
Within our PANS cohort, we previously reported a high rate of arthritis and inflammatory back pain in our PANS cohort (Frankovich et al. 2015; Brown et al. 2016), for which NSAIDs are the cornerstone treatment. For these conditions, NSAIDs are the most effective when they are used early in the disease course and in milder disease. NSAIDs are also used for a number of inflammatory diseases, including juvenile arthritis, systemic lupus erythematosus, Behçet's disease, etc., but they are often used in the context of milder disease and in patients with concurrent arthritis and/or myalgia (Sirnsek et al. 1991; Lander et al. 2002; Wallace 2006). In juvenile arthritis, NSAIDs are often extended beyond the resolution of arthritis by 3–6 months to avoid the recurrence of arthritis that is associated with early discontinuation (Wallace 2006). We have found that in some patients with PANS, arthritis, pain, and psychiatric symptoms relapse after NSAIDs are removed, and they resolve when NSAIDs are reintroduced (Spartz et al. 2017).
As in other inflammatory diseases, more aggressive induction regimens and maintenance immunomodulatory therapy are often necessary to achieve durable remissions in PANS patients, especially in patients with moderate-to-severe disease, chronic-static or progressive courses, or frequent relapses. This study excluded patients who had a chronic-static or progressive disease (i.e., those who required aggressive immunomodulatory regimens). Thus, our results are not generalizable to these patient subgroups. However, NSAIDs may be an important adjunct therapy in these groups as they are often used in combination with other anti-inflammatory medications in more advanced juvenile arthritis.
Limitations
The design of this study was a retrospective chart review, which has several attendant limitations that we attempted to ameliorate with clear reporting of our decisions to include and exclude patients and flares. One major difficulty with this type of design is variability in the quality of documentation; many of the flares treated in the early days of our clinic did not have clear records of start and end dates. In addition, we failed to capture some data when patients did not follow up with our clinic regularly, or when they had flares between clinic visits that lacked proper documentation. However, we expect that the most clinically significant flares resulted in clinic visits, as the majority of our patients (83%) live within 90 miles of the clinic. Although many of these flares/patients were excluded (per flare criteria), flares meeting criteria but that had missing data were retained. The statistical methodology we selected is robust to the influence of these missing data.
Other limitations include the current absence of reliable and validated psychiatric assessment instruments that are specific to PANS. No single measure adequately reports impairment in all of the psychiatric domains affected in PANS and PANDAS. Although derived from validated instruments, the PANS Global Impairment Score has not been validated. Therefore, our primary analysis focused on flare duration rather than symptom level, an approach used in Sydenham's chorea, another poststreptococcal neuropsychiatric disease (Barash et al. 2005; Paz et al. 2006; Walker et al. 2007). Parent questionnaires, clinic visit data, email, and phone communications (recorded in the EMR and personal communication) were used to help inform the outcome variables. Another limitation is that the research assistant (KB) who conducted the retrospective chart review was not blinded to treatment status.
This study under-reports the true NSAID side effect rate since only patients who tolerated NSAIDs for a minimum of 7 days were included in this study, thus eliminating patients who may have had side effects in the first week of NSAID therapy. The true NSAID side effect rate may be as high as 33% (Spartz et al. 2017), but the vast majority of these side effects are clinically insignificant, transient, and self-resolved.
Conclusions
Our results suggest that NSAIDs given prophylactically or early in the disease flare are associated with shorter flare durations in patients with new-onset and relapsing/remitting PANS and PANDAS. Earlier treatment with NSAIDs for a PANS flare may lead to a faster remission. These findings are consistent with the impact of NSAIDs in other inflammatory diseases, including juvenile arthritis. A randomized placebo-control clinical trial of NSAIDs in PANS is warranted to formally assess NSAID treatment efficacy.
Clinical Significance
The results of this retrospective, observational study warrant a randomized, placebo-control trial to definitively evaluate the impact of NSAIDs treatment and prophylaxis on PANS symptoms and subsequent flares, and to systematically evaluate predictors of response. The high rate of relapse observed in patients on prophylactic NSAIDs calls for identification of other treatments or adjunct treatments that may result in a more durable remission. As in other inflammatory disorders, clinicians may consider adjunctive therapies such as corticosteroid bursts (Brown et al. 2017), daily low-dose corticosteroids (as with other inflammatory diseases such as lupus and asthma), hydroxychloroquine, and other corticosteroid-sparing agents in combination with NSAIDs. This study demonstrates that for PANS and PANDAS initial flares and relapses, NSAIDs are associated with shorter neuropsychiatric symptom duration when given early in disease flare or prophylactically. In the absence of clinical trial data, NSAIDs are recommended to treat mild-to-moderate PANS flares, with periodic trials off and side-effect monitoring to evaluate for efficacy in alleviating symptoms (Frankovich et al. 2017).
Footnotes
Acknowledgments
The authors would like to acknowledge Dr. Susan Swedo, MD, The National Institute of Mental Health, the PANDAS Physicians Network, Dr. Kiki Chang, MD, SPARK Translational Research Program, and all the staff and faculty at Lucille Packard Children's Hospital and Stanford PANS Clinic who make caring for these children possible. This work was supported (in part) by the Intramural Research Program of the National Institute of Mental Health and the PANDAS Physician Network.
Disclosures
No competing financial interests exist.