
Abstract
Objectives:
Pharmacotherapy for problematic aggressive and violent behavior disorders in male children and adolescents is associated with significant adverse events. Treatments with more acceptable risk–benefit ratios are critically needed. Micronutrient intervention will be investigated as an alternative to bridge the therapeutic gap in the management of these behaviors.
Methods:
Males aged 4–14 who displayed ongoing violent and aggressive behaviors received micronutrient intervention containing alpha-tocopherol (vitamin E), ascorbic acid (vitamin C), biotin, chromium, pyridoxal-5-phosphate (P5P), pyridoxine (vitamins B6), selenium, and zinc, in a 16-week open-label trial. Plasma zinc, plasma copper, copper/zinc ratio, and urinary hydroxyhemopyrroline-2-one (HPL) tests were conducted at baseline and endpoint. Participants were examined for changes in aggressive and violent behaviors measured using the Children's Aggression Scale (CAS) and the Modified Overt Aggression Scale (MOAS), improvements in family functioning measured using the Family Functioning Style Scale, improvements in health-related quality of life (HRQoL) measured using the Pediatric Quality of Life Inventory (PedsQL) at baseline, 8 weeks, endpoint, and at 4–6-month follow-up.
Results:
Thirty-two male children and adolescents met inclusion criteria. Thirty-one (mean 8.35 ± standard deviation 2.93 years) completed the study, with one participant lost to follow-up. Micronutrient therapy significantly improved parent-reported aggressive and violent behaviors measured using the CAS for all domains except the use of weapons (p < 0.001 to p = 0.02) with medium to large effect size (Cohen's d = 0.72–1.43) and the MOAS (p < 0.001) with large effect size (Cohen's d = 1.26). Parent-reported HRQoL (p < 0.001; Cohen's d = −1.69) and family functioning (p = 0.03; Cohen's d = −0.41) also significantly improved.
Conclusion:
Micronutrient therapy appeared well tolerated, with a favorable side effect profile. It appeared effective in the reduction of parent-reported aggressive and violent behaviors, and showed improvement in family functioning and HRQoL in male youth after 16 weeks. Further research in the form of a double-blinded, randomized controlled trial is required to verify these initial positive observations.
Introduction
C
The global prevalence of CD in 2010 was 3.6% for males and 1.5% for females (Erskine et al. 2014), with males appearing to have an increased frequency and severity of behaviors (Pilling et al. 2013). CD is a heterogeneous condition with sufferers often exhibiting vastly different symptom profiles (Klahr and Burt 2014). Therefore, individualizing treatment for these patients may need to be considered a target of therapy (Hambly et al. 2016). CD is often refractory to first-line interventions (e.g., behavioral, psychosocial, psychotherapeutic, and educational/school-based therapy) and off-label prescription medication is usually required to manage severe cases (Barzman and Findling 2008). There is limited evidence for the safety, efficacy, and impact on quality of life (QoL) for medicines used in children with CD, resulting in a treatment gap and an opportunity to investigate adjunct and novel therapies (Hambly et al. 2016).
There are a multitude of biochemical and neurochemical inductors of aggression reported in the literature. Androgenic, serotonergic, noradrenergic, dopaminergic, GABAergic, and opioidergic mechanisms are involved in the formation of aggressive behavior (Chichinadze et al. 2011). Changes in concentrations of different micronutrients such as zinc and pyridoxal-5-phosphate (P5P), in addition to other organic and inorganic compounds, have been shown to contribute to aggressive behavior (Walsh et al. 1997; Chichinadze et al. 2011). Micronutrients are essential for neurological development, cognition, protection against oxidative stress, and as cofactors for the synthesis of neurotransmitters (Shils et al. 2006; Frazier et al. 2013). It is possible that behavioral problems may be indicative of inborn metabolic insufficiency due to suboptimal availability of micronutrient cofactors (Ames et al. 2002; Kaplan et al. 2007). Raising cellular concentrations of the deficient cofactor through high-dose micronutrient therapy is one approach to target metabolic insufficiency. Micronutrient therapy is aimed at overcoming genetic or acquired abnormalities in neurotransmitter precursors and other important body chemicals (Walsh et al. 2004). Improved metabolic efficiency at the level of neurotransmitters is only one of several mechanisms that have been proposed to explain how micronutrients affect brain function and behavior. Others include enhanced antioxidant activity, improved bioenergetic function, improved methylation, and facilitation of mitochondrial function (Mehl-Madrona et al. 2010).
There has been an increase in literature on the use of micronutrient treatment for behavioral disorders, including violence and aggression. A review of single-nutrient interventions in mood disorders has provided promising results for the use of micronutrients, including zinc, pyridoxine (vitamin B6), alpha-tocopherol (vitamin E), chromium, and selenium (Kaplan et al. 2007). Recent research on micronutrient combinations has also shown promising evidence in a variety of mental health conditions (Mehl-Madrona et al. 2010). A randomized controlled trial (RCT) of 231 young offenders receiving micronutrients containing omega-3 and omega-6 fatty acids showed a 35.1% decrease in disciplinary incidents compared to a reduction of only 6.7% in those receiving placebo (Gesch et al. 2002). Similarly, an RCT of 326 incarcerated male youth receiving micronutrients, fish oil, and evening primrose oil reported a 34% reduction in aggressive incidents in those receiving treatment compared to a 14% increase in incidents in those receiving placebo (Zaalberg et al. 2010). Furthermore, a study of delinquent behavior in 80 schoolchildren aged 6–12 found a 47% lower mean rate of antisocial behavior requiring discipline (e.g., fighting, disorderly conduct, and endangering others) in those taking micronutrients compared to placebo (Schoenthaler et al. 1991; Schoenthaler and Bier 2000).
The ability to individualize therapy based on biochemical profiling and through personalized pharmaceutical compounding may be a novel way to provide better treatment outcomes. Ultimately, it may be that individualized micronutrient dosing is optimal based on detectable genetic variations in micronutrient metabolism, including receptor or transcription factors (Frazier et al. 2013). The majority of published studies include commercial formulations of multiple micronutrients such as EMPowerplus™, which contains a proprietary mix of ingredients, including retinyl palmitate (vitamin A), ascorbic acid (vitamin C), cholecalciferol (vitamin D), vitamin E, thiamine (vitamin B1), riboflavin (vitamin B2), niacin (vitamin B3), vitamin B6, folic acid (vitamin B9), cyanocobalamin (vitamin B12), biotin, pantothenic acid, calcium, iron, phosphorus, iodine, magnesium, zinc, selenium, copper, manganese, chromium, molybdenum, and potassium (Kaplan et al. 2002, 2004; Frazier et al. 2009, 2013; Mehl-Madrona et al. 2010).
To date, no biomarker for CD has achieved the status of clinical utility as a diagnostic tool or as a predictor of treatment outcome. There are reports that explosive anger, aggression, and violence may be associated with a biochemical deficiency of vitamin B6 and zinc, an elevation of free copper levels, and low plasma biotin (Walsh et al. 1997, 2004; McGinnis et al. 2008b). Elevated hydroxyhemopyrroline-2-one (HPL), an oxidative stress-related molecule (Fryar-Williams and Strobel 2015), has also been observed in patients with these behaviors (Walsh et al. 1997, 2004). HPL is an organic pyrrole-containing compound that has been detectable in urine (McGinnis et al. 2008a, 2008b; Walsh 2012). Furthermore, copper and zinc have shown promise with elevated copper/zinc ratios correlating to aggressive and violent behaviors (Walsh et al. 1997, 2004).
Vitamin B6 is required by more than 100 enzymes involved in protein metabolism and is a cofactor for more than 80 biochemical reactions, including the efficient synthesis of the neurotransmitters serotonin, dopamine, and gamma-aminobutyric acid. Deficiency can result in altered levels of these neurotransmitters and may contribute to conditions, including attention-deficit/hyperactivity disorder (ADHD), depression, anxiety, sleep disorders, and mental illnesses (Hvas et al. 2004; Rucklidge and Kaplan 2013; Rucklidge et al. 2015). In the context of violent and aggressive behaviors, vitamin B6 is an understudied micronutrient. Due to the high affinity that HPL has for the aldehyde structure of vitamin B6, further research into the identification of this mechanism and its role in vitamin B6 depletion and behavior is crucially needed (Vucijak et al. 2009).
Zinc is an important cofactor for metabolism of neurotransmitters, prostaglandins, and melatonin and indirectly affects dopamine metabolism (Viktorinova et al. 2016). Zinc protects sulfhydryl groups of proteins and enzymes against free radical attack in the body by acting as an antioxidant (Black 1998). Although its precise role is not fully understood, low zinc levels could alter neuron activity, result in neurological dysfunction, and impact upon the neurodevelopment, intellect, and behavior of children and adolescents (Walsh et al. 1997; Viktorinova et al. 2016). Severe zinc deficiency is uncommon in the developed world, however; marginal zinc deficiency has been identified by a number of studies with clinical implications (Prasad 1996; Ploysangam et al. 1997; Hambidge 2000). Although its prevalence is not reported, marginal zinc deficiency is believed to be widespread (Arnold et al. 2005). Definitive indicators of zinc status are lacking and serum zinc may not be a reliable biomarker for zinc status in humans (Hambidge 2000).
Zinc plays a reciprocal role to copper, competing for the metallothionein binding protein and acting as a defence against copper by inhibiting its absorption from the gastrointestinal tract (Faber et al. 2009; Fryar-Williams and Strobel 2015). The serum copper/plasma zinc ratio has been reported as a promising biomarker for indicating stress in the metallothionein system (Faber et al. 2009). When there is a deficiency of zinc, copper appears to accumulate in the body, which may contribute to violent behavior, hyperactivity, learning disabilities, schizophrenia, and depression (Viktorinova et al. 2016). Studies investigating the ratio of copper to zinc are a contemporary area of interest with a recent article reporting that plasma copper/zinc ratio significantly correlated with teacher-rated inattention in ADHD children and adolescents (Viktorinova et al. 2016). Elevated copper/zinc ratios have also been associated in assaultive young males (Walsh et al. 1997), autism spectrum disorders (ASD) (Faber et al. 2009), and schizophrenia (Fryar-Williams and Strobel 2015).
The use of micronutrients such as vitamin B6, P5P, zinc, biotin, selenium, and vitamins C and E, has been documented to target violent and aggressive behaviors in those with elevated HPL and oxidative stress (Walsh et al. 2004; Walsh 2012). Micronutrient therapy may be an alternative therapy that may be useful in bridging the therapeutic gap in the management of violent and aggressive behaviors in youth without the metabolic, cardiovascular, thyroid, and sedative side effects associated with contemporary pharmaceuticals often used in this population, such as antipsychotics, psychostimulants, anticonvulsants, and mood stabilizers (Hambly et al. 2016). Nonetheless, micronutrient therapy requires further study due to its increasing use in youth without supportive evidence (Frazier et al. 2013).
Methods
The study consisted of a 16-week, single-site, open-label intervention of micronutrient therapy. Participants were seen for a screening visit, at baseline, after 8 and 16 weeks of treatment. Follow-up occurred 6–12 months after discharge from the study. The Griffith University Human Research Ethics Committee provided ethical clearance for the study. Participants were recruited from February 2015 to September 2015 via advertising to schools or clinical referral by medical practitioners, specialists, or social workers. Inclusion criteria were male participants, 4–14 years of age, displaying parent-reported ongoing violent and aggressive behaviors for at least 6 months defined by a T score greater than 60 on the Children's Aggression Scale Parent Version (CAS-P) and/or a positive score on the Modified Overt Aggression Scale (MOAS). Participants had never received or had not recently received (within 4 weeks) micronutrient therapy or prescription medication (elimination kinetics calculated for adequate washout by pharmacist J.L.H.) for their behavior. A screening questionnaire was sent to guardians who had contacted the research team. After completion, potentially eligible participants and their guardian/s were invited for a further screening assessment and provision of oral and written information about the study. They provided written informed consent, urine (APAN Laboratories) and blood samples (Sullivan and Nicolaides Pathology) to screen for any full blood count, plasma zinc, plasma copper, whole blood histamine, and urine HPL abnormalities. Potential participants were excluded if their behavior was secondary to another illness (e.g., physical disability, diabetes, or thyroid dysfunction), had an acute medical condition requiring priority, had severe anemia or vitamin D deficiency, or had a medical condition that may result in severe malabsorption from the gastrointestinal tract (e.g., Crohn's disease or irritable bowel syndrome). Those receiving nonpharmaceutical interventions such as psychological therapy and counseling were allowed to participate provided that treatment was consistent throughout screening to week 16. Guardians completed the CAS-P, MOAS, Family Functioning Style Scale (FFSS), and the Pediatric Quality of Life Inventory (PedsQL). Once pathology and questionnaires were completed, those participants meeting inclusion criteria were invited to participate and were provided with teacher information and consent forms for optional classroom teacher participation. Participating teachers completed the Children's Aggression Scale Teacher Version (CAS-T) and the MOAS at the same time points as participant visits.
We hypothesized that micronutrient therapy would be efficacious after 16 weeks, shown by the primary outcome of a reduction in aggressive and violent behaviors in male children and adolescents aged 4–14 years of age, measured using the CAS-P and MOAS. Secondary outcomes included an improvement in health-related quality of life (HRQoL) measured using the PedsQL, and an improvement in family functioning measured by the FFSS, and that micronutrient therapy would be safe and well tolerated shown by an absence of adverse effects and compliance to the intervention.
Intervention
Participants received capsules that could be swallowed or dispersed in food or drink containing vitamin C, vitamin B6, P5P, vitamin E, biotin, chromium, selenium, and zinc. In general, the strategy of studying several ingredients in combination is unusual, especially given the standard scientific approach of examining the effects of one pharmacologic agent at a time (Kaplan et al. 2002). However, previous studies using micronutrients in combination have been successful (Kaplan et al. 2004), and the use of this combination of micronutrients has reported (Walsh et al. 2004) an anecdotal (Walsh 2012) success for violent and aggressive behaviors in those with elevated HPL. As elevated HPL is associated with oxidative stress and a deficiency in vitamin B6, P5P, zinc, and biotin, these agents were included. Vitamin E was included as a lipid-soluble antioxidant (Niki 2014), vitamin C as a water-soluble antioxidant (Rose 1988), and selenium for its role as a major constituent of many enzymes with antioxidant functions (Prasad 1996). Chromium was included due to its role in neurotransmitter synthesis, fat metabolism, and glucose regulation, where glucose intolerance has been described as a potential exacerbating factor in violent outbursts (Sylvia et al. 2013). The dose of each micronutrient was calculated based on weight. For example, a 25 kg participant received 460 mg of vitamin C, 23 mg of vitamin B6, and 57.5 mg of P5P in the morning; and 460 mg of vitamin C, 34.5 mg of zinc, 368 (international units) IU of vitamin E, 920 (micrograms) mcg of biotin, 46 mcg of chromium, and 11.5 mcg of selenium in the evening. The micronutrients were provided by a compounding pharmacy in Tugun, Queensland, Australia. Both morning and evening capsules were prescribed to be taken with food to minimize any risk of nausea.
Outcome assessments
Assessments were conducted at the screening visit, baseline, 8 weeks, endpoint (16 weeks), and at 4–6-month follow-up. The CAS-P, MOAS, FFSS, and the PedsQL were administered to guardians at the baseline, week 8, week 16, and at follow-up. The CAS-T and MOAS were administered to classroom teachers/aides who consented at baseline, week 8, and week 16. Compliance was recorded via the use of dose administration charts and counting capsules returned to the clinic at 8 and 16 weeks. Primary outcomes were ratings of aggressive behavior, measured using two instruments, the CAS and the MOAS, which have recently been shown to be useful in RCTs, including youth with violent and aggressive behaviors (Hambly et al. 2017).
• The CAS-P and CAS-T Version
The CAS is used to measure the frequency and severity of aggressive acts of noninstitutionalized youth in setting-specific environments (e.g., home or school) (Halperin et al. 2003). The CAS-P features 33 items and the CAS-T features 23. The CAS has five key domains namely verbal aggression, aggression against objects and animals, provoked physical aggression, unprovoked physical aggression, and use of weapons. The parent version has two additional domains, including aggression against family members and aggression against nonfamily members (Halperin et al. 2002). The items in the CAS are weighted depending on the frequency and severity of the act, with higher numerical scores indicating increased frequency and/or severity of aggression (Halperin et al. 2002). A qualitative score is also assigned ranging from “normal range,” “mildly elevated,” “moderately elevated,” to “very elevated.” The CAS has strong psychometric properties in children and adolescents across both the parent and teacher versions (Halperin et al. 2002, 2003).
• The MOAS
The MOAS is a 16-item rating scale that is used to measure the severity of verbal aggression, physical aggression against objects, physical aggression against self, and physical aggression against others (Sorgi et al. 1991). The items of the MOAS are weighted and hand-scored on a five-point Likert scale of increasing severity with verbal aggression assigned the lowest weight and physical aggression the highest (Huang et al. 2009). Scores can range from 0 to 40, with higher scores indicating more severe aggression. The MOAS has been used in many studies with child and adolescent participants (Kronenberger et al. 2007; Blader et al. 2010; Dean et al. 2014). It has reasonable reliability in children (Dean et al. 2014).
Secondary outcomes were HRQoL and family functioning. They were assessed by the following: • The Pediatric Quality of Life Inventory (PedsQL™ 4.0) PedsQL is an instrument used to measure HRQoL in children and adolescents aged 2–18 years. The 23-item PedsQL 4.0 parent report features four domains that are used to assess physical, emotional, social, and school functioning. These four domains comprise the core health dimensions outlined by the World Health Organization (Varni et al. 2002). Scale scores range from 0 (“almost always having a problem”) to 100 (“never having a problem”), with higher scale scores indicating better HRQoL. The PedsQL 4.0 has evidence for reliability, validity, and responsiveness (Varni et al. 2002, 2002). • The FFSS The FFSS is used to assess the extent to which a family member believes his or her family displays different strengths and capabilities namely, interactional patterns, family values, coping strategies, family commitment, and resource mobilization (Trivette et al. 1990). It includes 26 items, each rated on a scale from one (“not at all like my family”) to five (“almost always like my family”), with higher scores indicating better family functioning. The FFSS has evidence for reliability and validity of families of preschool children (Trivette et al. 1990).
Biological testing
Blood samples (nonfasting) were collected via Sullivan and Nicolaides Pathology at the screening visit (full blood count, plasma zinc, plasma copper, whole blood histamine) and at endpoint (16 weeks) (plasma zinc and plasma copper). Urine samples (nonfasting) were collected and measured at APAN Laboratories for HPL at the screening visit and at endpoint (16 weeks). Zinc, copper, histamine, and HPL were investigated for diagnostic purposes. Height and weight were measured at baseline, 8 weeks, and 16 weeks.
Adverse effects
Guardians and participants were requested to report any potential adverse effects occurring during the study. Guardians were advised to monitor for nausea, gastrointestinal upset, and/or a decline in behavior particularly on initiation. Guardians were contacted regularly (weekly on average) throughout the study and any data regarding adverse effects were documented and managed accordingly.
Statistical analyses
Statistical analyses were carried out using Stata® version 14.1 (StataCorp 2015). The sample size estimate was calculated based on the primary outcome of a reduction in aggressive and violent behaviors measured using the CAS due to its valid and reliable psychometric properties and ability to measure the frequency and severity of behaviors. A standard deviation (SD) of 23 was assumed based on total aggression scores reported in a validation study of the instrument in community and clinical samples (Halperin et al. 2002; Halperin 2008). To detect a statistically significant difference between repeated measures, pre- and postintervention, with 90% power and a type I error value of 0.05, 30 participants were required to complete the study. Assuming a 20% drop out, there was a target to recruit 38 participants at baseline.
Continuous measures were described using means and SDs, or medians and interquartile ranges, as appropriate. Nominal variables were described as frequencies and percentages. Paired samples t-tests and effect size (Cohen's d) for changes from baseline to end of week 8 and from baseline to end of week 16 were analyzed for primary and secondary outcome measures. The adequacy of each statistical model for primary and secondary outcomes was assessed by examining residuals for heterogeneity and normality. All tests were two tailed and p-values less than 0.05 were considered statistically significant.
Results
Thirty-one male participants completed the 16-week study (Fig. 1). One-hundred fourteen individuals contacted the recruitment team and 61 children and adolescents were screened for eligibility. Thirty-two participants met inclusion criteria and with their guardian/s providing consent to participate. One participant was lost to follow-up after the initial visit. Thirty-one participants were included in outcome analyses. Characteristics of the population are presented in Table 1. Participants ranged from 4 to 14 years of age (mean 8.35 ± SD 2.93 years) with at least one participant in each year of age. On average, they were considered lean with a mean body mass index of 16.79 ± SD 2.39 (normal range: 18.5–24.9). The population sample predominately consisted of nuclear families (55%), with single-parent and blended families less common in 26% and 19% of the sample, respectively. Of the 31 participants, 20 (65%) resided in metropolitan areas, while 11 (34%) resided in rural or nonmetropolitan areas. Nineteen (61%) participants had been diagnosed with one or more behavioral disorders, including oppositional defiant disorder (16%), ADHD (16%), ASD (34%), and posttraumatic stress disorder (6%), emphasizing the heterogeneity of violent and aggressive behavioral disorders. Twelve (39%) participants had no formal diagnosis, which was expected due to the inclusion criteria for treatment-naive participants. Twenty-two (71%) participants were on previous psychosocial therapy. At baseline, 26 (84%) participants were rated at the highest category of aggression according to CAS-P (i.e., “very elevated” aggression), 4 (13%) were scored as “mild to moderate,” and 1 (3%) participant scored a borderline “normal” aggression rating. All participants returned a positive MOAS score for aggressive behavior at baseline (mean 13.32 ± SD 7.36). Twenty-four participants (77%) were compliant with therapy, defined as adhering to more than 80% of their doses. Teacher response was suboptimal with only two completing questionnaires from baseline to week 16. The mean and SD for baseline, as well as change and effect size from baseline to week 8 and from baseline to week 16, are presented in Table 2.
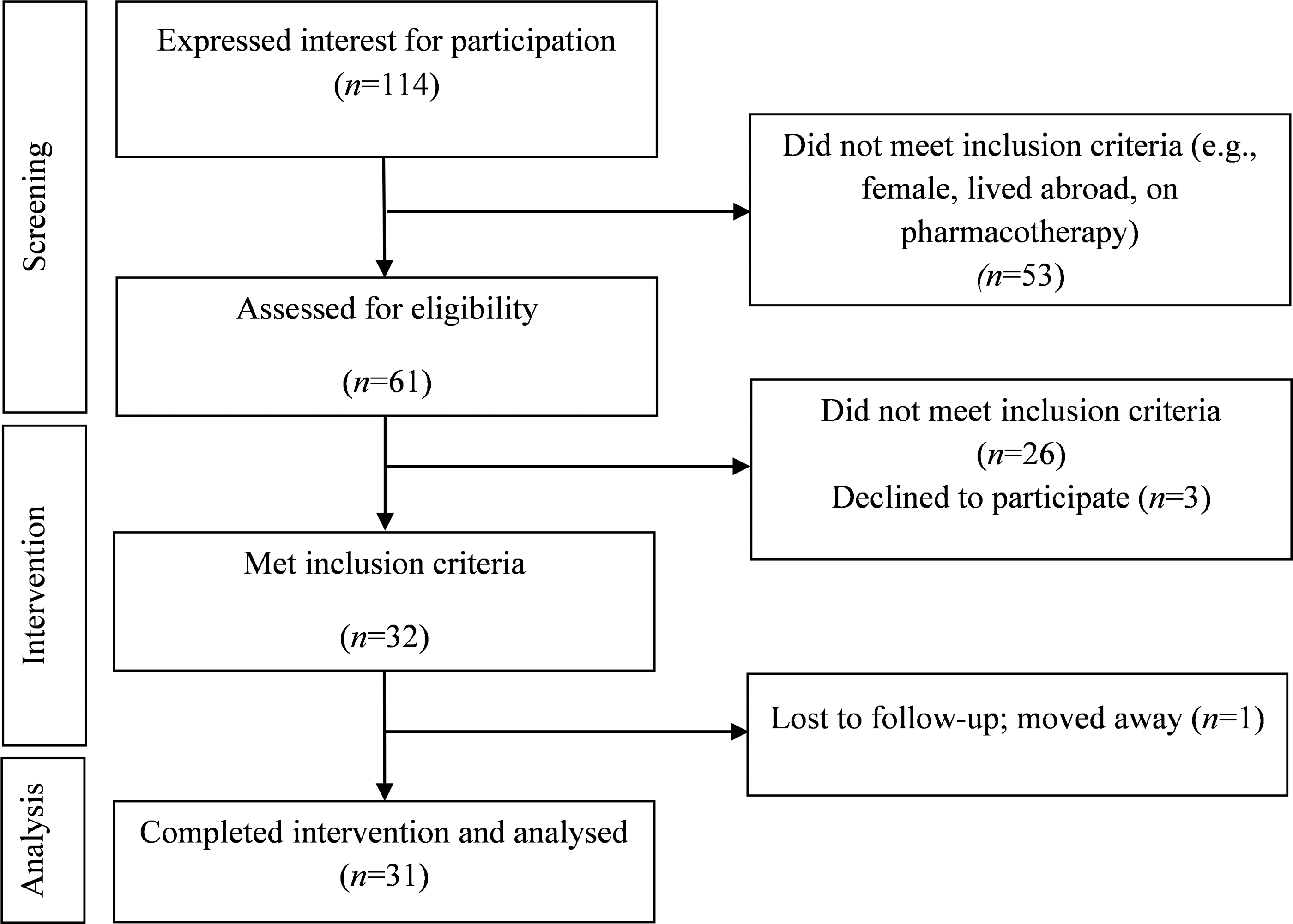
Flowchart of participants through the study. n, number.
BMI, body mass index; CAS, Children's Aggression Scale; SD, standard deviation.
p < 0.001.
p < 0.05.
p >0.05.
CAS, Children's Aggression Scale; HPL, hydroxyhemopyrroline-2-one; FFSS, Family Functioning Style Scale; MOAS, Modified Overt Aggression Scale; O/A, objects/animals; PedsQL, Pediatric Quality of Life Inventory; SD, standard deviation.
Primary outcome: aggression and violent behaviors
Significant improvement in aggression and violent behaviors within 8 weeks was observed for the MOAS (p < 0.001) (Table 2) and the CAS-P (p < 0.001 to p = 0.002) (Table 2 and Figs. 2 and 3). Furthermore, a significant (p < 0.001) improvement with large effect size (Cohen's d = 1.26) in aggressive behavior was observed for the MOAS from baseline to endpoint (week 16). A significant improvement in parent-reported total aggression for all subscales of the CAS-P (p < 0.001 to p = 0.02) was observed from baseline to endpoint (Table 2 and Figs. 2 and 3). Medium to large effect size (Cohen's d = 0.72–1.43) was also observed for all subscales of the CAS-P except the use of weapons subscale (Cohen's d = 0.42) between baseline and endpoint (Table 2). At endpoint, 11 (35%) participants had reached the “normal range” on the CAS-P and 10 (32%) had “mild to moderate” aggression. Ten (32%) participants had “very elevated” aggression at endpoint compared to 26 (84%) at baseline.

Mean change of raw scores of aggressive and violent behaviors measured by the CAS-P at baseline, week 8, and week 16 for verbal, physical, and initiated aggression, aggression against objects/animals, and use of weapons. CAS, Children's Aggression Scale; CAS-P, Children's Aggression Scale Parent Version.

Mean change of aggressive and violent behaviors measured by the CAS-P at baseline, week 8, and week 16 for aggression against family, nonfamily peers, and adults. CAS, Children's Aggression Scale; CAS-P, Children's Aggression Scale Parent Version.
No correlations between behavior in the school environment and any other outcomes were identified from the teacher data. However, parent-reported aggression scores against nonfamily members (p < 0.001, Cohen's d = 1.23) and peers (e.g., those outside the home) measured using the CAS-P over 16 weeks were significant with large effect size (p < 0.001, Cohen's d = 1.24), possibly suggesting improvements in school behavior. Thematically, teacher feedback supported behavioral improvements in those who were identified as displaying violent and aggressive behavior at school. For example, teachers reported for two participants, “He has shown a decrease in aggressive and violent outbursts, and the severity of reactive aggression” and “aggressive and explosive behaviours are not evident, they were prevalent before treatment.”
Four- to 6-month follow-up data showed that of the 20 participants who continued micronutrient treatment after the trial, 7 (35%) had further improvements in their parent-reported MOAS and CAS-P scores. Nine (45%) participants maintained the behavior reached at week 16, and four (20%) deteriorated on the MOAS and CAS-P showing a decline in MOAS and CAS-P scores. Of the four who showed a decline in behavior, all were taking additional supplements or had switched to commercially available formulations with fewer micronutrients. Two (6%) participants did not continue micronutrients after discharge from the study. Of these, one (3%) participant showed a decline in behavior with CAS-P scores returning to moderate aggression after reaching normal levels at week 16 from very elevated at baseline. No differences were observed for the second participant not continuing. Nine participants were lost to follow-up.
Secondary outcome: HRQoL
Mean baseline PedsQL was 56.73 ± SD 11.90 reflecting that participants “often” had problems with emotional functioning and “sometimes” had problems with physical, social, and school functioning. Micronutrient treatment had a significant effect on the PedsQL from baseline to week 8 (p < 0.001) and from baseline to week 16 (p < 0.001) with a large effect size (Cohen's d = −1.69) and an endpoint mean score increasing to 70.93 ± SD 11.70. All four domains (physical, emotional, social, and school) displayed significant (p < 0.001) participant improvement from baseline to endpoint. The most notable improvement was for the social (mean difference −16.45 ± SD 14.45) and emotional (mean difference −16.13 ± SD 15.15) domains, which included questions pertaining to relationships with peers and behavioral issues such as anger, anxiety, depressed mood, and insomnia.
Secondary outcome: family functioning
Mean baseline FFSS was 3.85 ± SD 0.62 reflecting that the strengths and capabilities of the participant's families were present “sometimes” to “usually” out of a five-point scale of “not at all,” “a little,” “sometimes,” “usually,” and “almost always.” Micronutrient intervention had a significant effect on family functioning (p = 0.03) with a mean endpoint FFSS score increased to 4.01 ± SD 0.51, reflecting that families reached the “usually” category. Although a small to medium effect size was observed (Cohen's d = −0.41), it was not expected to see a large effect size or improvement in this outcome due to the adequacy of family functioning at baseline.
Biological testing
In this study, 14 (45%) participants were identified as being deficient or marginally deficient in plasma zinc at baseline (mean = 11.5 ± SD 1.7 μmol/L). Three (10%) participants were considered zinc deficient at baseline (<9 μmol/L), with a further 11 (35%) in the lowest quartile of the reference range (9–11.5 μmol/L). Twenty-nine (94%) participants had an increase in plasma zinc from baseline to endpoint. Compared to baseline measurements, micronutrient supplementation resulted in an expected significant increase in plasma zinc (p < 0.001), where a mean of 14.8 ± SD 3.16 μmol/L was reached at endpoint, consistent with behavioral improvements.
Compared with baseline measurements, micronutrient supplementation resulted in an expected significant decrease in plasma concentrations of copper (p < 0.001). At baseline, four (13%) participants had elevated (>22 μmol/L) plasma copper (mean 18.55 ± SD 3.42), three of whom returned to normal reference range at week 16. Twenty-five (81%) had a decrease in plasma copper levels from baseline to week 16. A decrease in copper levels was expected due to the supplementation with zinc (Faber et al. 2009; Fryar-Williams and Strobel 2015).
At baseline, the mean copper/zinc ratio was 1.64, which decreased to 1.14 at week 16. Twenty-four (77%) participants had an improvement in their copper/zinc ratio after micronutrient intervention.
HPL levels were elevated for all participants at baseline, ranging from 19 to 204.4 μg/dL. No significant (p = 0.90) differences were found between pre- and postintervention urinary HPL with endpoint HPL levels ranging from 4 to 152.9 μg/dL. A significant change in HPL level was expected to be observed in a 16-week period. Despite significant decreases in aggression levels, only 11 (35%) participants had reached “normal” aggression levels at endpoint (16 weeks) as defined by the CAS-P. HPL levels were not available for those participants who continued to improve in their behavior at 6 and 12 months. Furthermore, zinc supplementation can result in copper excretion leading to initial elevated free copper levels due to the dynamic competition and homeostasis between these metals in the body, resulting in increased HPL (Fryar-Williams and Strobel 2015; Viktorinova et al. 2016). To prevent therapy interruption, no washout period was observed before biological testing at endpoint, and therefore, the pathology results may not be true indicators of physiological HPL, zinc, and copper (e.g., elevated zinc levels due to the intervention).
Safety outcomes
No serious adverse events occurred and all reported adverse effects (n = 4) were mild and transient. No participants experienced moderate or severe adverse effects and no participants withdrew due to a study-related adverse event. Four participants reported nausea from their morning dose, which was alleviated by reminding the affected participants to take the intervention with food or to delay their morning dose until a meal had been consumed later in the day.
Discussion
Micronutrient therapy has been evaluated in many clinical studies; however, few studies have focused on violent and aggressive behavioral outcomes. Those studies that do include violent and aggressive children and adolescents are case reports (Kaplan et al. 2002) or case series reports (Kaplan et al. 2004), including the coadministration of prescription medicines, including antipsychotics, psychostimulants, and antidepressants. Individualized micronutrient dosing through biochemical profiling is emerging as a novel method to manage behavioral disorders (Walsh et al. 2004; Rucklidge and Kaplan 2013). Perhaps due to its personalized prescribing, rigorous evidence in the form of RCTs to support efficacy and safety is lacking. This pilot open-label trial is the first, to our knowledge, that has investigated the use of vitamin C, vitamin B6, vitamin E, biotin, chromium, selenium, and zinc as a combination of micronutrients for use in violent and aggressive behaviors in male children and adolescents. This trial provides preliminary data, suggesting that compounded micronutrient therapy may be safe and effective in improving violent and aggressive behaviors, HRQoL, and family functioning in males aged 4–14. Notably, improvements in aggressive and violent behaviors and HRQoL were seen as early as 8 weeks with significant findings across all domains of the CAS-P, MOAS, and PedsQL. Significant improvements across all outcome measures from pre- to post-intervention were observed over 16 weeks. As measured using the CAS-P, the use of micronutrient therapy significantly improved verbal aggression, aggression against objects/animals, physical aggression, initiated aggression, aggression against family and nonfamily members, aggression against peers and adults with an overall large effect size. The micronutrient intervention also improved aggression related to the use of weapons; however, this was less remarkable perhaps due to the study sample having a young mean age (8.35 ± SD 2.93 years) and reduced ability to acquire weapons compared to older counterparts. Scores measured using the MOAS also displayed an improvement in overt aggressive behaviors.
Individuals with developmentally inappropriate negativistic, aggressive, and violent behaviors often have considerable impairments in social, family, and academic functioning (Wehmeier et al. 2011; American Psychiatric Association 2013), resulting in a decrease in their HRQoL and placing burden on their families (Wehmeier et al. 2011; American Psychiatric Association 2013). In this study, significant improvements in HRQoL and family functioning were observed. Although the effect size was small to medium for family functioning, it was efficient at baseline; therefore, we did not expect to observe an improvement after intervention.
With the intervention showing promising results, one of the most notable observations was the enthusiasm of guardians to continue therapy. On completion of the study, families had to fund continuing therapy, consultations, and pathology. The majority (n = 20, 65%) of participants continued the micronutrient intervention with 80% (n = 16) maintaining or having further improvements at 4–6-month follow-up. Given the trajectory of response at endpoint and follow-up, a future study with a longer duration of intervention is suggested for any future double-blind, placebo-controlled study utilizing this intervention.
It is known that childhood aggression is highly situational and the ability to analyze aggression in different contexts (e.g., home, school, siblings, and peers) is useful (Halperin et al. 2003). Teachers of the participants were approached by both the research team and guardians for participation; however, the data collected were not substantial for analysis. Reasons for the lack of teacher questionnaire compliance included workplace leave, school holidays, and/or teachers changing employment sites. Nonetheless, results in parent-reported behavior at school and thematic analysis of parent and teacher commentary suggest improvement in behavior.
Urinary HPL has recently emerged as a legitimate biomarker of oxidative stress in schizophrenia and schizoaffective psychosis (Fryar-Williams and Strobel 2015). It is thought to arise as an abnormal product of heme metabolism under conditions of extreme oxidative stress (Fryar-Williams and Strobel 2015). Elevated HPL has also been associated with a deficiency of other micronutrients, including vitamin B6, P5P, and zinc. Our findings that participants had elevated HPL at baseline support reports that explosive anger, aggression, and violence may be associated with elevated urine HPL (Walsh et al. 1997, 2004; Fryar-Williams and Strobel 2015). Human studies that evaluate the impact of antioxidant or micronutrient intervention on urinary HPL are lacking, and therefore, further investigation is required to determine if HPL can normalize following micronutrient intervention. Micronutrients have an essential role in oxidant and antioxidant mechanisms in the body. Imbalances may result in susceptibility to oxidative damage of important cellular components, which may contribute to violent and aggressive behaviors (Walsh et al. 2004; Viktorinova et al. 2016).
A study conducted by Walsh et al. in 1997 reported a mean serum copper to plasma zinc ratio of 1.4 for assaultive young males aged 3–20 compared to normal behavior controls of 1.02 (Walsh et al. 1997). We observed at baseline that participants had a mean elevated plasma copper/zinc ratio of 1.64, which decreased to 1.14 at week 16.
Conclusion
This is the one of the first studies to evaluate a uniform treatment protocol of individualized micronutrient therapy for violent and aggressive male youth in a clinical trial using valid and reliable psychometric instruments. Results from this open-label pilot study indicated that micronutrient therapy was well tolerated, with a favorable side effect profile. Furthermore, micronutrient therapy appeared effective in the reduction of aggressive and violent behaviors, with improvement of HRQoL and family functioning in male youth after 16 weeks, with significant improvements seen as early as 8 weeks. However, further research in the form of a double-blinded, RCT of sufficient size and extended duration is required to verify these initial positive observations, and to further clarify whether baseline urinary HPL, plasma zinc and copper have potential as biomarkers for diagnostic purposes and to predict treatment responders.
Clinical Significance
Current pharmacotherapy for aggressive and violent behavior associated with behavioral disorders in youth is associated with significant adverse events (Hambly et al. 2016). Treatments with a more acceptable risk–benefit ratio are critically needed (Frazier et al. 2013). Micronutrient interventions may be useful in the management of child and adolescent CDs with favorable side effect profiles. This is one of the first studies exploring the efficacy and safety of micronutrient therapy on violent and aggressive behaviors, HRQoL, and family functioning. A 16-week, open-label study of 31 males receiving a compounded micronutrient supplement containing eight ingredients appeared safe and effective for the reduction of violent and aggressive behaviors and improvement of HRQoL. This research suggests that further, more rigorous investigation is required to determine if micronutrient therapy can continue to show efficacy and safety.
Limitations
Limitations of the current open-label study include the absence of a double-blind placebo-controlled design, inclusion of only male participants, and sparse data from school teachers. While no serious adverse effects were observed, the short duration of the study did not allow for assessment of long-term safety. While this combination of micronutrients was effective in reducing violent and aggressive behaviors, future trials are needed to determine if a more efficient combination of micronutrients will result in the same behavioral change.
Footnotes
Acknowledgments
The authors acknowledge the teachers, parents, guardians, and participants for their valuable time and participation; the clinic staff for their assistance; Prof. Brett McDermott and Dr. William Bor for their feedback; Griffith University, The Menzies Health Institute QLD, and Mater Research—The University of Queensland for their support; Tugun Compounding Pharmacy for providing the intervention; APAN Laboratories for urine analysis and Sullivan Nicolaides Pathology for blood analysis.
Disclosures
No competing financial interests exist.