
Abstract
Objective:
Only little is known about antipsychotic (AP) off-label use (OLU) in pediatric populations. It was the aim of this study to examine the frequency as well as the risks of off-label AP use in underaged patients.
Methods:
To calculate the frequency of off-label AP prescriptions for the years 2004–2011, we used claims data of more than two million minors aged 0–17 years. Off-label prescriptions were analyzed with regard to type of OLU, physician specialty, and underlying diagnoses. Incidence rates of selected adverse events were calculated for on-label as well as for OLU. The risk of poisoning associated with on- or OLU was assessed in a nested case-control study.
Results:
The annual share of pediatric AP users with off-label prescriptions varied between 52.3% and 71.1%. OLU by indication (42.8%–66.5%) was the most common type of OLU. Of the subjects with OLU by indication, 52.5% had a diagnosis of hyperkinetic disorder. Adverse events were scarce (incidence rates between 0.8 and 8.6 per 10,000 person-years), and no significant difference was observed between on- and OLU.
Conclusion:
Because of their frequent use in hyperkinetic disorder patients, APs are commonly prescribed off-label for minors. Since OLU by contraindication was rare and the risk of the adverse events under study was similarly small for on- and OLU, this is not necessarily an indication for inappropriate treatment. It rather indicates that further randomized studies are needed to examine efficacy and safety of pediatric AP use in this indication.
Introduction
D
Antipsychotics are used for the treatment of disorders like schizophrenia and bipolar mania. Because of their sedative effects, APs are also used for the treatment of restlessness and agitation, anxiety, and sleep disorders (Preston et al. 2013). Despite the risk of adverse events like hyperlipidemia, marked weight gain, and extrapyramidal side effects, including tardive dyskinesia (Preston et al. 2013; Correll and Blader 2015), increasing pediatric (atypical) AP use has been observed in several countries, including Germany (Schubert and Lehmkuhl 2009; Zoega et al. 2009; Alexander et al. 2011; Pringsheim et al. 2011; Alessi-Severini et al. 2012; Olfson et al. 2012, 2015; Ronsley et al. 2013; Bachmann et al. 2014; Steinhausen and Bisgaard 2014; Abbas et al. 2016), with rates of OLU between 36% and 94% (Zoega et al. 2009; Alexander et al. 2011; Olfson et al. 2012; Baeza et al. 2014; Rodday et al. 2014; Carton et al. 2015). However, these studies varied methodologically and were limited to small sample sizes (Zoega et al. 2009; Baeza et al. 2014; Rodday et al. 2014), short observation periods (Zoega et al. 2009; Baeza et al. 2014; Rodday et al. 2014), and single drug classes (Rodday et al. 2014), or they did not examine OLU sufficiently (Zoega et al. 2009; Alexander et al. 2011; Olfson et al. 2012; Baeza et al. 2014; Rodday et al. 2014). Beyond that, the risks of off-label AP use in pediatric patients have not been sufficiently investigated yet.
We therefore assessed changes in the extent of off-label AP use over time and, for the first time, provided detailed analyses of OLU stratified by sex, age, drug class, the prescribing physicians' specialty, and type of OLU, using data from a representative sample of minors in Germany. In addition, we compared the risks of off-label and on-label AP use.
Methods
Data source
We used data from three German statutory health insurance (SHI) providers that are part of the German Pharmacoepidemiological Research Database (GePaRD). GePaRD comprises demographic data, diagnoses, hospitalizations, and outpatient prescriptions of more than 20 million individuals (Pigeot and Ahrens 2008). Diagnoses are coded according to the International Classification of Diseases, 10th Version, German Modification (ICD-10-GM). Among others, outpatient care data cover diagnoses (related to a quarter of a year), procedures, and drug prescriptions. Outpatient prescription data include the date of prescription and dispensation, the Anatomical Therapeutic Chemical (ATC) code, the defined daily dose (DDD), and the prescribing physician's specialty. Hospitalization data cover admission and discharge dates with corresponding diagnoses. GePaRD has been shown to be representative for the German population with regard to age and sex distribution, region of residence, number of hospital admissions, and drug use (Schink and Garbe 2010a, 2010b).
Study design
The study population comprised minors (0–17 years) who were insured in one of the three SHIs between 2004 and 2011. The study cohort was built in two steps. First, the share of outpatient (off-label) AP prescriptions was assessed in annual cross-sectional analyses. All persons with continuous insurance time either (a) during the whole study year, or (b) from birth until death in the study year, or (c) from birth in the study year until the end of the study year, or (d) from start of the study year until death in the study year were included.
Second, a cohort was defined, which included all subjects with at least one outpatient AP prescription during the study period, who had a baseline period of at least 6 months of continuous insurance coverage before the prescription and no concurrent on- and off-label AP prescriptions. The association between AP use and metabolic/endocrine events, extrapyramidal events, malignant neuroleptic syndrome, and poisoning by APs was examined in this cohort. The date of the first outpatient AP prescription was defined as cohort entry. Subjects were followed until the first of the following events: (a) end of study period; (b) end of insurance (including death); (c) interruption of insurance coverage for more than 14 days; (d) December 31st of the year in which the subject turned 17; or (e) date of occurrence of the outcome.
For the outcome with the highest number of events (poisoning by APs), we were able to investigate the risk of OLU compared to on-label use, additionally in a nested case–control study. Up to five controls were matched by sex, age group at the index date (0, 1–2, 3–5, 6–11, 12–14, 15–17 years), and SHI to each case, using risk set sampling.
Drug exposure
Since GePaRD does not contain information on inpatient drug use, only outpatient prescriptions could be assessed. All APs with an ATC code starting with N05A and the ATC code N05CM22 (for promethazine) were included in the analyses and categorized into typical or atypical APs.
The DDD and the amount of the prescribed drug were used to calculate the duration of drug exposure.
In the nested case–control study, current use was defined as AP treatment overlapping the date of the adverse event. Recent use ended 1–30 days before the event. Subjects with a treatment not classified as current or recent were categorized as past users.
Covariates
Diagnoses were identified using inpatient and outpatient data. All approved indications of the prescribed APs and also other diagnoses of diseases of the nervous system (ICD-10-GM: G00-G99) and of mental and behavioral disorders (F00-F99) were considered covariates in the nested case–control study and also when examining the most frequent diagnoses among AP users. Besides, in the nested case–control study, antiepileptics (N03A), additional APs (N05A, N05CM22), anxiolytics (N05B), antidepressants (N06A), and psychostimulants (N06B) were included as comedications. Covariates and comedications were ascertained in the baseline period.
Off-label use
OLU was examined using information from the Summaries of Product Characteristics (SPCs) on the approved indications, contraindications, and the licensed age. If no diagnosis of an approved indication was coded in the quarter of the prescription or in the preceding or following quarter, a prescription was off label by indication. If there was a contraindicated medication overlapping the AP prescription or any diagnosis of a contraindication in the quarter of the AP prescription, a prescription was off label by contraindication. If the age of the child was not in accordance with the licensed age of the drug, a prescription was off label by age. If the licensed age varied by indication or if SPCs of generic preparations gave inconsistent information, the lowest age limit was used. All approved indications and contraindications were assigned to generic drugs if the SPCs of generic drugs did not list all of them.
Outcome definition
Malignant neuroleptic syndrome (ICD-10-GM: G21.0), extrapyramidal events (G21.1, G24.0, and G25.1), poisoning by AP drugs (T43.3, T43.4, T43.5, and T43.9), and metabolic/endocrine events were considered outcomes. A metabolic/endocrine event was defined by at least three out of the five following diagnoses in a subject: (a) obesity (E66); (b) diabetogenic effects (R73, E11-E14); (c) hypertension (I10); (d) hyperglyceridemia (E78.1, E78.2); and (e) hypercholesterolemia (E78.0, E78.2). All outcomes were identified using inpatient main discharge and secondary diagnoses.
Statistical analysis
The prevalence of outpatient AP prescriptions was analyzed stratified by age, sex, on-/ OLU, and drug class with corresponding 95% confidence intervals (CI) using the substitution method (Daly 1998). Off-label prescriptions were further analyzed regarding underlying diagnoses, the prescribing physician's specialty, and type of OLU.
In the study cohort, incidence rates (IR) of the outcomes were calculated per 10,000 person-years (py) with corresponding 95% CIs, stratified by on- and off-label use.
Conditional logistic regression was used to obtain confounder-adjusted odds ratios (ORs) with corresponding 95% CIs in the nested case–control analysis. The risk of poisoning by APs associated with current OLU, simultaneous off- and on-label use, recent use, and past use of any AP was compared to current on-label use of any AP (reference group). Prior history of poisoning was forced into the model and a backward selection (Wald test with p < 0.05 for staying in the model) was performed for further covariates.
All statistical analyses were conducted using SAS statistical software version 9.3.
Ethics
The Code of Social Law (SGB X) regulates the use of SHI data for scientific research in Germany. All involved SHIs and their governing authorities approved the use of the data for this study. Approval by an ethics committee and informed consent were not required.
Registration
The study was registered in the register of studies of the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (
Results
Study population
The study populations of the annual cross-sectional studies comprised between 1,993,994 (2004) and 2,160,541 (2009) minors with mean age between 8.8 and 9.0 years. Throughout the study period, the proportion of boys was slightly higher compared with girls (51% vs. 49%). We identified between 4309 (2006) and 5459 (2011) minors with outpatient AP prescriptions (prevalence between 0.2% and 0.3%).
Extent of OLU
The total number of outpatient AP prescriptions increased from 12,595 in 2004 to 24,309 in 2010 and decreased to 21,951 in 2011. The share of off-label prescriptions varied between 61.0% (2004) and 69.5% (2009). In 2004, 52.3% of all AP users had at least one off-label AP prescription. This proportion increased to 71.1% in 2009 and decreased to 62.7% in 2011, with 63.0% for males and 61.8% for females. OLU was more common among users of atypical than typical APs, especially in the earlier study years (Fig. 1). In 2011, the lowest rate of subjects with off-label prescriptions was observed in the group of 3–5-year olds (46.2%) (Fig. 2).
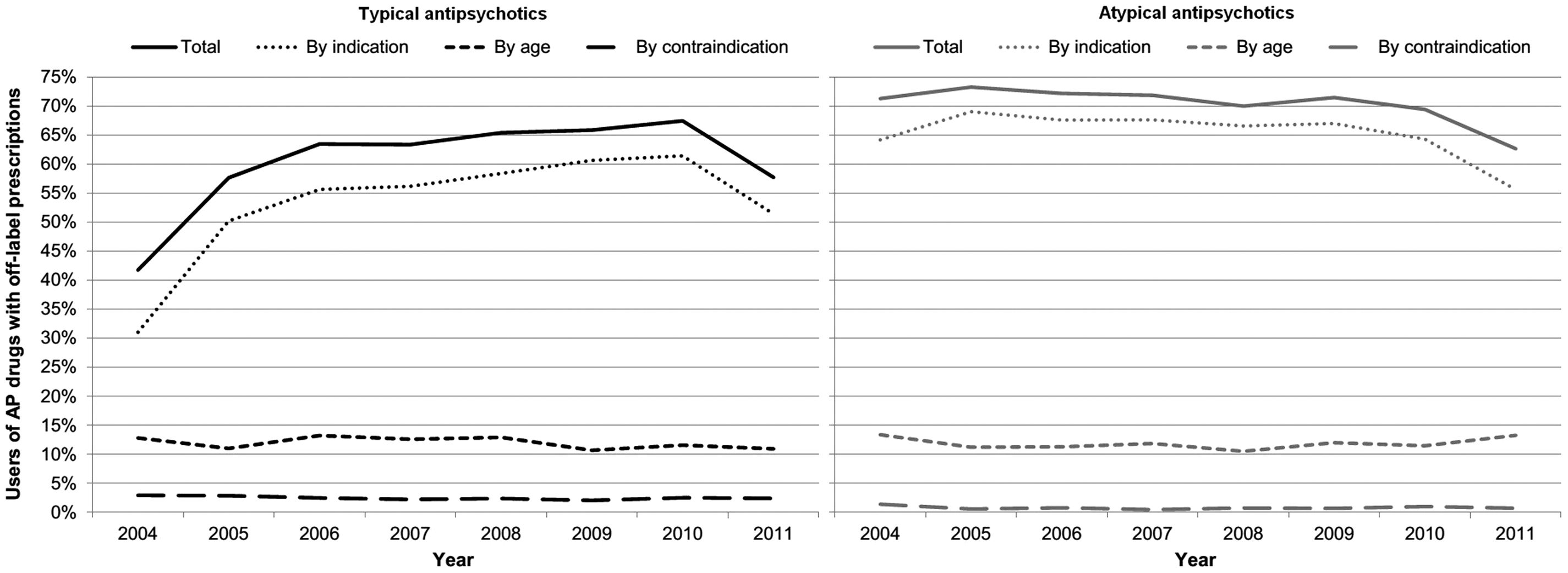
Share of users of typical (left, black) and atypical (gray, right) antipsychotics with off-label prescriptions. One patient can contribute to more than one type of off-label use. AP, antipsychotic.
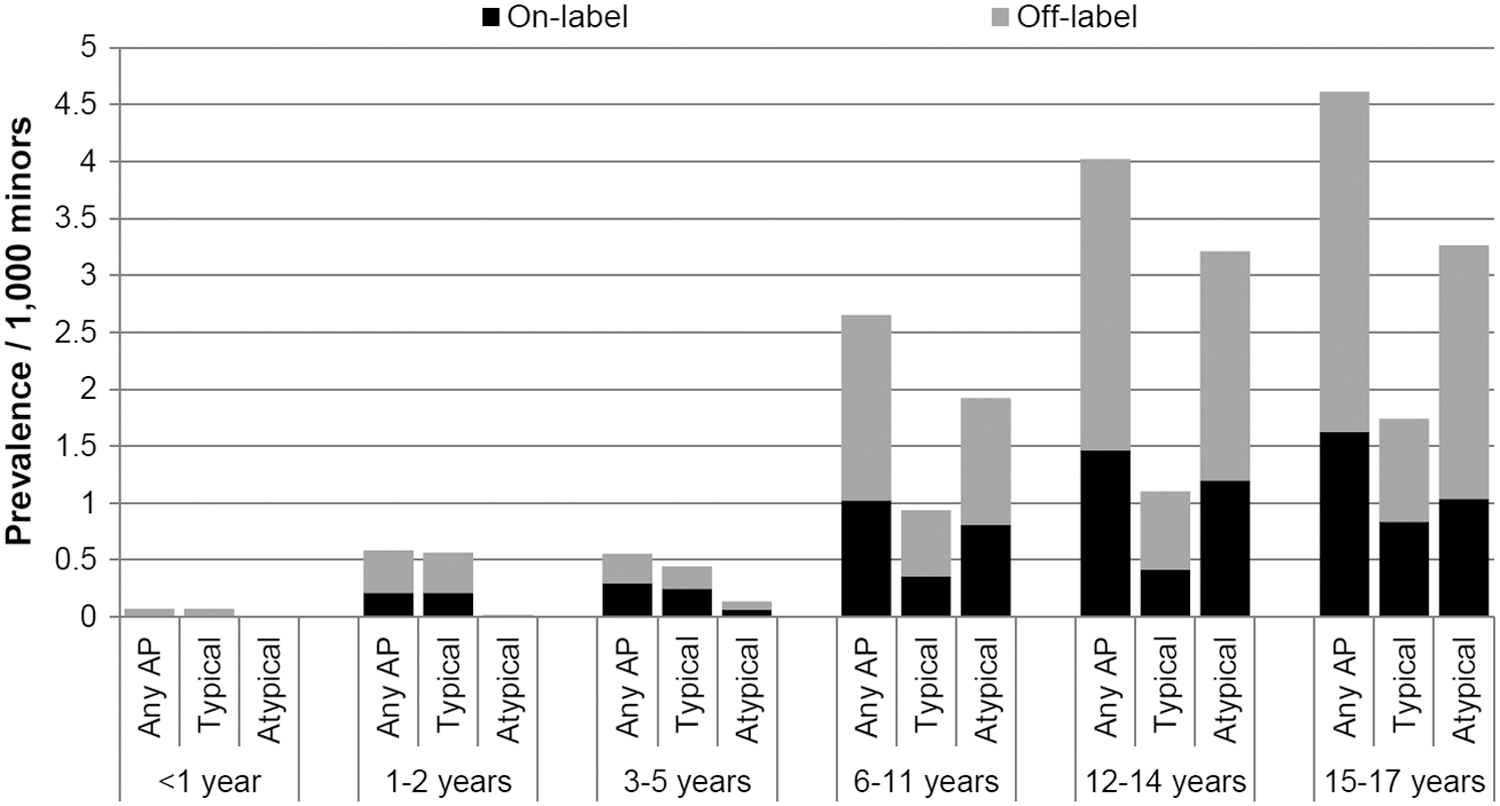
Prevalence of prescriptions of on- and off-label (all types) antipsychotics in 2011 by age group and drug class.
Throughout the study period, OLU by indication was the most common type of OLU, ranging from 42.8% to 66.5% of all AP users having a prescription off label by indication. The proportion of AP users with prescriptions off label by age varied from 11.5% to 13.5%, while the share of AP users with prescriptions off label by contraindication decreased from 2.5% to 1.4%. Off-label prescriptions by indication occurred more frequently among users of atypical APs, while off-label prescriptions by contraindication were more common among typical AP users (Fig. 1).
Of the 3055 AP users with a prescription off label by indication in 2011, 52.5% had a diagnosis of hyperkinetic disorder (ICD-10: F90), 19.2% a diagnosis of pervasive developmental disorder (F84), 15.7% a diagnosis of tic disorder (F95), 15.4% a diagnosis of other behavioral and emotional disorders (F98), and 13.6% a diagnosis of specific developmental disorders of speech and language (F80) during the quarter of the prescription. The mean age of AP users with a prescription off label by age was 12.3 years (SD = 5.0, median = 14).
Pediatricians issued 30.1% of the 21,955 AP prescriptions in 2011, followed by child and adolescent psychiatrists (27.6%), physicians for internal and general medicine (13.3%), and general practitioners (3.9%). The specialty of the prescribing physician was unknown/not reported for 15.9% of all AP prescriptions. The remaining 9.2% were prescribed by physicians with various other fields of specialties. Of the APs prescribed by general practitioners, 65.0% were prescribed off label (Table 1).
Risks of OLU
The AP user cohort (2004–2011) included 21,779 subjects (at cohort entry, 8759 on-label users and 13,020 off-label users), of whom 64.1% were male (Table 2). Of the on-label users, 6.8% switched to OLU during their follow-up time (3.4% from off- to on-label use). The share of males was slightly lower in the group of on-label users (62.3% vs. 65.3%). On- and off-label users were similar regarding age, length of follow-up, and prevalence of most comorbidities and comedications during the 6-month baseline period.
The date of the first prescription of an antipsychotic drug.
Among the analyzed covariates.
The 6 months before cohort entry.
Columns add up to more than 100% because one patient can contribute to more than one line.
In brackets: Diagnostic code according to the International Classification of Diseases, 10th Version, German Modification (ICD-10-GM).
In total, we observed 52 cases of poisoning by APs, 14 extrapyramidal events, 7 metabolic/endocrine events, and 5 cases of malignant neuroleptic syndrome. The corresponding IRs, stratified by on- and off-label use, are shown in Table 3.
The nested case–control analysis showed no significantly increased risk of poisoning by APs for current OLU, combined current off- and on-label use, and recent or past use of any AP compared to current on-label use (Table 4). Use of antidepressants increased the risk of poisoning, while use of psychostimulants had a protective effect.
Reference group = current on-label use.
Adjusted for all covariates shown in the table.
During the 6-month baseline period before the first prescription of an antipsychotic drug.
Discussion
Our findings showed a high rate of off-label AP prescriptions (mostly off-label by indication) among pediatric AP users. However, OLU was not associated with a higher risk of the adverse events under study.
Throughout the study period, off-label AP use in minors occurred frequently. As reported previously, hyperkinetic disorder was by far the most frequent diagnosis among AP users in Germany (Schröder et al. 2017). Our work shows that this diagnosis was even more frequent among those with an AP prescription off label by indication. As there is no licensed AP for the treatment of hyperkinetic disorder, the high share of off-label AP prescriptions is not surprising. Antipsychotics are frequently used to manage aggressive and impulsive behavior in patients with hyperkinetic disorder, although their efficacy in this regard has not been sufficiently investigated (Linton et al. 2013). This is also the reason why the German guideline for the treatment of hyperkinetic disorders states that the risks of AP use might be greater than its benefits and consequently recommends cautious use of APs (German Society of Child and Adolescent Psychiatry Psychosomatics and Psychotherapy 2007a).
In Germany, haloperidol is the only AP approved for the treatment of tic disorder patients older than 2 years. However, the German guideline (German Society of Child and Adolescent Psychiatry Psychosomatics and Psychotherapy 2007b) recommends the use of tiapride and risperidone, and according to a German study (Bachmann et al. 2015), the APs most frequently prescribed for the treatment of tic disorders are tiapride, risperidone, pipamperone, and aripiprazole. Thus, medical treatments of pediatric tic disorder patients largely follow guideline recommendations, but are off label to a large extent as well.
OLU by contraindication can be regarded as the most dangerous type of OLU since it entails the highest risk of adverse events. Therefore, the small fraction of AP prescriptions off label by contraindication, reported in this study, is quite gratifying from the drug safety perspective.
The majority of APs was prescribed by pediatricians and child and adolescent psychiatrists, showing that most AP users were treated by physicians specialized in the treatment of pediatric patients. There were no striking differences regarding the rate of off-label prescriptions between different groups of prescribers. This is in contrast to findings by Carton et al. (2015) reporting that the highest share of off-label AP prescriptions in minors was found for physicians not specialized in child psychiatry.
International comparisons of OLU are difficult due to differences in healthcare systems and the licensing of drugs. Accordingly, studies from different countries (using different methods) showed proportions of AP OLU in minors between 36% and 94% (Zoega et al. 2009; Alexander et al. 2011; Olfson et al. 2012; Baeza et al. 2014; Rodday et al. 2014; Carton et al. 2015).
Between 2004 and 2011, we observed only a small number of reported adverse events, suggesting a rare occurrence of these events in treating minors with APs. However, due to the small number of events, we were only able to examine one outcome (poisoning by APs) in more detail using a nested case–control design. There, we found no significant difference in the risk of poisoning by APs between on- and off-label use. It is known, mostly from case reports, that poisoning by APs can occur in both minors and adults, but no reliable data on the incidence in pediatric patients have been reported (Gajre et al. 2012; Toepfner et al. 2013; Hitosugi et al. 2014). Referring to a report from the American Association of Poison Control Centers, poisoning by APs is quite common with more than 43,000 calls to U.S. Poison Centers in 2009, only regarding atypical APs (Minns and Clark 2012). Since this number is not restricted to minors and based on self-reports with an unknown extent of underreporting or overreporting, it is, however, not comparable with our results.
A prior diagnosis of mental retardation was associated with a lower risk of poisoning in our study. Minors with such a diagnosis probably do not have direct access to the medication as their parents will manage the drug intake. A prior use of antidepressants was associated with a higher risk of poisoning by APs. In addition, in the unadjusted analysis (data not shown), we observed an increased risk for patients with a history of mood disorders [OR = 2.6 (95% CI 1.3–5.5)]. Although these patients might also include an unknown number of individuals suffering from bipolar affective disorder, who could tend to poison or harm themselves during a manic episode, these two findings indicate that some poisoning cases were associated with a depressive disorder and possibly had a suicidal background.
The consequences of poisoning by APs include sedation, tachycardia, hypotension, extrapyramidal symptoms, neuroleptic malignant syndrome, seizures, coma, and even death (Isbister et al. 2005; Minns and Clark 2012; Toepfner et al. 2013; Hitosugi et al. 2014). Regarding the atypical APs clozapine, olanzapine, quetiapine, and risperidone, the most frequent symptoms are minor reductions in vigilance, miosis, and mild tachycardia (Meli et al. 2014), which might not always lead to physician visits. Even if weaker symptoms lead to physician visits, they might not always be coded as cases of poisoning. Therefore, milder cases of poisoning are likely to be underestimated in our study.
A major strength of this study is the size of the database used. We describe real-world drug utilization patterns in a population representative for the German general population (Schink and Garbe 2010a, 2010b). Investigating drug exposure with pharmacy dispensing data is considered the gold standard in pharmacoepidemiological research since recall bias can be ruled out (Schneeweiss and Avorn 2005). In addition, it is known that drug dispensation data give valid information on drug use in Germany (Hoffmann et al. 2008; Schink and Garbe 2010b).
We were only able to assess outpatient AP treatment since GePaRD does not include information on inpatient AP use. However, the database should provide valid and comprehensive information on outpatient AP use in minors since all examined APs are available by prescription only. Compared to primary data collections based on interview data, there is only low potential for misclassification of drug exposure, since GePaRD contains the exact date when the patient received the medication from the pharmacy. Yet, there is no information on patients' adherence to prescriptions. And since the database does not provide information on the prescribed daily dose, we were not able to investigate associations between drug dosage and the frequency of adverse events. Furthermore, we had to use information on the prescribed amount and the DDD to estimate the time period of drug exposure.
Some misclassification is possible with regard to the underlying diagnoses for AP prescriptions since outpatient diagnoses in GePaRD are only related to a quarter of a year. This is also the reason why we were not able to use outpatient diagnoses for the identification of adverse events, which might have contributed to the small number of identified cases. If an outpatient diagnosis and AP prescription occurred in the same quarter, it is impossible to ascertain whether the outcome followed the exposure or vice versa. Finally, being limited to ICD-10 codes, we were not able to assess the cause behind an identified case of poisoning, which can include an adverse drug reaction as well as an overdose.
Conclusions
Antipsychotic OLU in minors, especially OLU by indication, occurs frequently. Our results show that most off-label AP prescriptions are issued to hyperkinetic disorder patients. This is not necessarily an indication for inappropriate drug use as shown by the low proportion of prescriptions off label by contraindication and by the fact that the risk of adverse events was similarly small for on- and off-label use. It rather indicates the need for further randomized studies investigating the efficacy and safety of APs in managing impulsive and aggressive behavior in minors suffering from hyperkinetic disorder. Such studies might lead to further regulatory approvals and consequently to decreasing OLU.
Clinical Significance
The reasons for and the risks of pediatric off-label use of antipsychotic drugs have not been sufficiently investigated yet. This study showed that antipsychotics are frequently prescribed off label for children and adolescents (mostly for patients diagnosed with hyperkinetic disorders). However, off-label use does not entail a higher risk of adverse events than on-label use.
Footnotes
Acknowledgments
The authors would like to thank all statutory health insurances, which provided data for this study, namely the AOK Bremen/Bremerhaven, the DAK-Gesundheit, and the Techniker Krankenkasse (TK).
The authors would also like to thank Dr. Heike Gerds for proofreading the final article.
Disclosures
C.S., B.K., T.B., and O.R. are working in departments that occasionally perform studies for pharmaceutical industries as indicated below. Until October 2014, M.D. worked at the same institute, and until August 2015, E.G. was head of a department there. The pharmaceutical companies include Bayer, Celgene, GSK, Mundipharma, Novartis, Sanofi, Sanofi Pasteur MSD, and STADA. E.G. has been a consultant to Bayer, Nycomed, Teva, GSK, Schwabe, Astellas, Takeda, and Novartis on issues unrelated to the subject of the study. R.W.D. has received compensation for serving as consultant or speaker, or he or the institution he works for has received research support or royalties from the following companies or organizations indicated: EU (FP7 Programme), US National Institute of Mental Health (NIMH), German Federal Ministry of Health/Regulatory Agency (BMG/BfArM), German Federal Ministry of Education and Research (BMBF), German Research Foundation (DFG), Volkswagen Foundation, Boehringer Ingelheim, Ferring, Janssen-Cilag, Lilly, Lundbeck, Otsuka, Servier, Shire, Sunovion/Takeda, and Theravance. R.W.D. owns Eli Lilly stock.