
Abstract
Objectives:
Suvorexant is the first dual orexin receptor antagonist for treating insomnia. This study aimed to evaluate the tolerability, efficacy, and safety of suvorexant on insomnia in adolescents.
Methods:
Thirty patients (8 male and 22 female; mean standard deviation age: 15.7 ± 2.4 years; range: 10–20) with insomnia were administered suvorexant. Clinical background, persistence rate, the Clinical Global Impression (CGI), and the Athens Insomnia Scale (AIS) were compared between patients who continued and discontinued suvorexant treatment.
Results:
Seventeen patients (56.7%) successfully continued taking suvorexant. Among the 13 patients who did not continue treatment, 5 patients were lost to follow-up. Of the remaining eight who did not continue treatment, four decided to discontinue of their own accord, two decided to discontinue due to lack of effectiveness, and two decided to discontinue due to adverse reaction, namely abnormal dreams. Among patients who completed the study, CGI significantly decreased from 3.6 ± 0.8 to 3.1 ± 0.9 (p = 0.014). The score of sleep quality in AIS was significantly higher among the patients who discontinued suvorexant than those who continued suvorexant (p = 0.02).
Conclusion:
Our results indicate that suvorexant could be considered a treatment option for adolescents.
Introduction
I
The treatment of insomnia starts with a detailed assessment of its cause and triggers; the foundation of insomnia management is sleep hygiene routines. Occasionally, pharmacological treatments for insomnia are needed in addition to behavioral approaches. However, hypnotic agents are not indicated for children and adolescents in most countries. In some cases, the prescription of off-label hypnotic medications is made after careful consideration of the risks and benefits. Most published studies on medication for insomnia in the pediatric population have been done in children with neurodevelopmental disorders, with melatonin being the most common medication studied (Maski et al. 2016). Evidence for the use of hypnotics in the pediatric population is still limited.
Suvorexant is the first reversible dual orexin receptor antagonist released for the treatment of insomnia in November 2014 in Japan and in February 2015 in the U.S. Suvorexant works as a selective antagonist of both orexin receptors, OX1R and OX2R, suppressing the orexin-mediated wakefulness system of the brain (Sakurai et al. 2010; Gotter et al. 2012). Orexin receptor antagonists represent a new class of therapeutic hypnotic medications for the treatment of insomnia. Clinical trials have evaluated the efficacy and safety of suvorexant (Herring et al. 2016; Michelson et al. 2014); however, these trials have only been undertaken with patients aged over 18 years.
The aim of this study was to evaluate the tolerability, efficacy, and safety of suvorexant on insomnia in adolescents to elucidate the possibility of the future use of suvorexant in adolescents.
Materials and Methods
In this study, we included 30 patients (8 male and 22 female; mean standard deviation [SD] age: 15.7 ± 2.4 years; range: 10–20) with insomnia who began taking suvorexant between January and June 2015 at Toyokokeiai Hospital, a psychiatric hospital for adults and children.
The investigators recorded gender, age, inpatient/outpatient status, pattern of insomnia, comorbid psychiatric disorders, mental state using the Children's Global Assessment Scale (CGAS), sleep state according to the Clinical Global Impression (CGI), and medication before the administration of suvorexant. The identified primary patterns of insomnia were difficulty initiating sleep, difficulty maintaining sleep, and waking up earlier than desired. Suvorexant was administered as a new prescription to drug-naive patients, or those switching from or adding on to current hypnotics. Dosage of suvorexant was fixed to 20 mg/day according to the Japanese regulations on the prescription of suvorexant to those younger than 65 years. CGAS and CGI scores were compared before and after the administration of suvorexant. The Athens Insomnia Scale (AIS) (Soldatos et al. 2003; Shahid et al. 2012) was used to assess the severity of insomnia 6 months after starting suvorexant as a posttreatment evaluation. AIS was developed as a brief and easy-to-administer self-assessment questionnaire for estimating the severity of insomnia. The validated Japanese version of the AIS has been established and was regarded as a highly useful instrument in both clinical and research settings (Okajima et al. 2013). Adverse events and reason for discontinuation were identified. This study was approved by the Institutional Review Board of the Toyokokeiai Hospital. This study was conducted according to the principles of the Declaration of Helsinki and informed consent was obtained from all participants.
Data were summarized as means (±SD) for continuous variables. Descriptive statistics were used to describe the distribution of participant characteristics. A chi-square test and a Mann–Whitney U test were employed to compare the results of patients in the continued and discontinued groups. Comparisons of CGI scores at administration of suvorexant and at the maintenance stage were performed using the Wilcoxon signed-rank tests. All tests were two tailed and assumed a 5% significance level. All data were analyzed using the statistical software SPSS Statistics (IBM Corp., Armonk, NY) for Windows, version 22.0.
Results
A flow diagram showing the outcomes for participants is shown in Figure 1. Of 30 patients, 28 patients were diagnosed with 1 or more psychiatric disorders: depression (n = 10), adjustment disorder (n = 8), autism spectrum disorder (n = 7), schizophrenia (n = 6), obsessive-compulsive disorder (n = 1), somatic symptom disorder (n = 1), reactive attachment disorder (n = 1), and conduct disorder (n = 1). Eleven patients had already received another sleep medication (brotizolam (n = 3), zolpidem (n = 3), eszopiclone (n = 2), amobarbital (n = 1), nitrazepam (n = 1), and quazepam (n = 1)). Among the patients taking suvorexant, 17 patients (56.7%) successfully continued the treatment until the postevaluation was conducted. The reason for not-continued treatment was loss of contact in five patients, their own decision to stop taking medication in four patients, lack of effectiveness in two patients, and adverse events in two patients. In 13 patients who did not continue suvorexant, the average duration before stopping was 82.2 days ±67.7 (range; 7–215). In the five patients with whom we lost contact, the durations of suvorexant use were 14, 28, 34, 115, and 128 days. In the four patients who decided of their own accord to discontinue suvorexant, the duration of suvorexant use was 45, 52, 55, and 90 days. In the two patients for whom suvorexant was not effective, the durations of suvorexant use were 7 and 79 days. Two patients who experienced adverse events, namely abnormal dreams, were females aged 16 and 17 with durations of suvorexant use of 207 and 215 days, respectively. In the continued group, a 17-year-old female patient experienced excessive sleep and sleepiness during the day; however, these symptoms were only seen in the first month after administration. No patient showed increased suicidality and suicidal ideations.
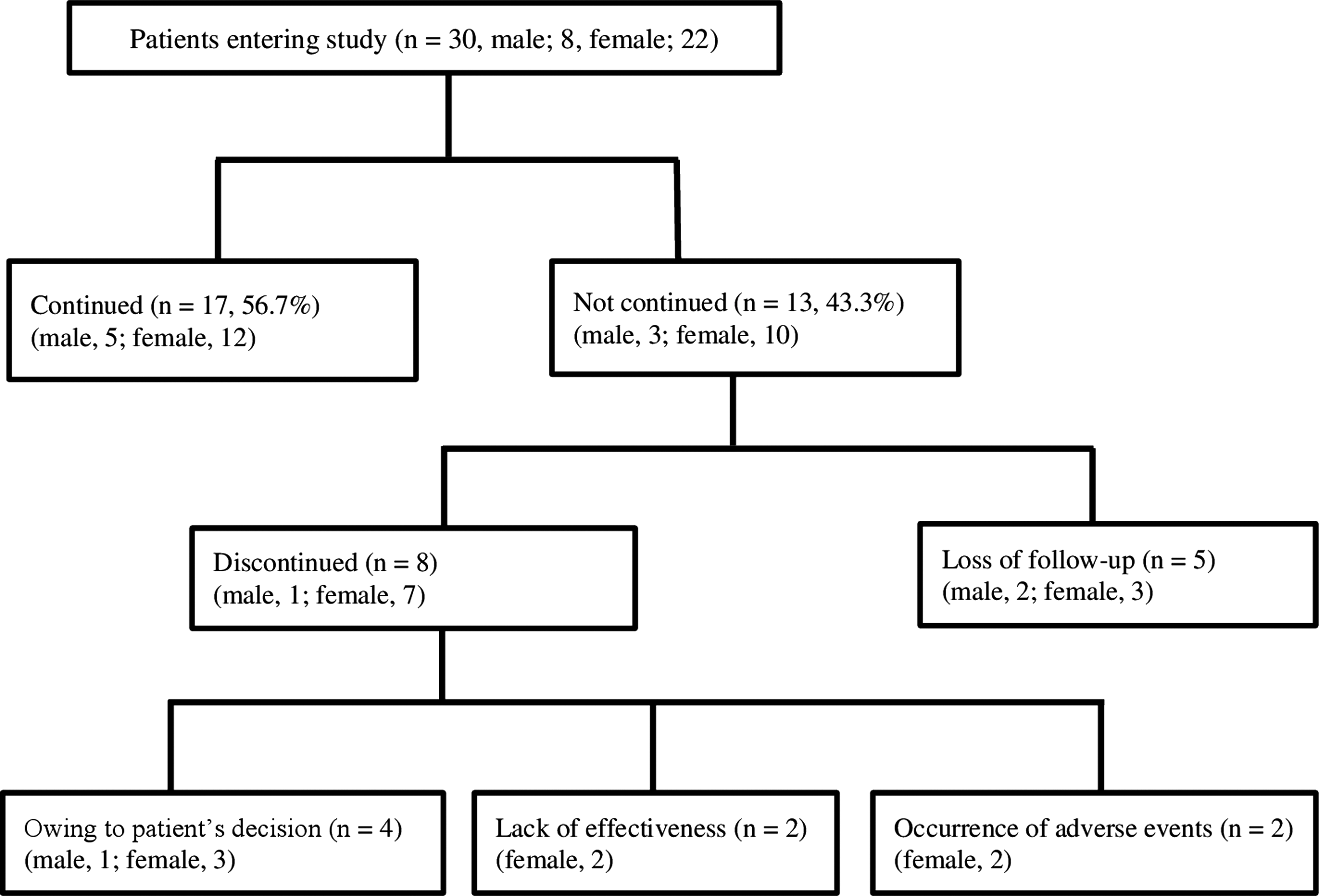
Flow diagram of participants.
The demographic and clinical characteristics of patients are shown in Table 1. Inpatient/outpatient ratio, pattern of insomnia, type of administration, CGAS scores at administration of suvorexant, and CGI scores at administration of suvorexant were not statistically different in the two groups. The posttreatment evaluations of patients are shown in Table 2. CGI scores at the maintenance stage of suvorexant were not statistically different in the continued group and the discontinued group. In the continued group (n = 17), CGI scores were significantly decreased in 6 months after starting suvorexant (before: 3.6 ± 0.8 and after: 3.1 ± 0.9, p = 0.014). Fifteen out of 17 patients who continued suvorexant answered the AIS. Sleep quality scores in AIS were significantly higher in the discontinued group than the continued group. However, the total scores and scores in other sections of the AIS were not statistically different.
Chi-square test.
Mann–Whitney U test.
CGAS, Children's Global Assessment Scale; CGI, Clinical Global Impression–Sleep (1: normal, not ill; 2: minimally ill; 3: mildly ill; 4: moderately ill; 5: markedly ill; 6: severely ill; and 7: among the most extremely ill).
AIS, Athens Insomnia Scale; CGI–Sleep (1: normal, not ill; 2: minimally ill; 3: mildly ill; 4: moderately ill; 5: markedly ill; 6: severely ill; and 7: among the most extremely ill).
Mann–Whitney U test. * p < 0.05.
Discussion
This study aimed to evaluate the tolerability, efficacy, and safety of suvorexant on insomnia in adolescent patients. There is little evidence recommending the use of hypnotic agents in adolescents, mainly due to insufficient evidence on safety and efficacy. The use of hypnotic agents, including suvorexant, is not indicated for children and adolescents in the package insert, therefore careful administration is always required. In general, hypnotics for young patients should always begin with a low initial dose; however, the doses that are acceptable vary from country to country. Suvorexant is available in 15 and 20 mg formulae in Japan, and 15 mg formula is indicated for elderly patients over 65 years. National health insurance system in Japan reimburses the costs of suvorexant for adolescents under the careful prescription by the physician.
In this study, the main outcome was the reduction of CGI scores by prescribing suvorexant in 6 months after starting suvorexant. Our study also shows that 56.7% of adolescents successfully continued taking suvorexant, and the adverse effect that led to discontinuance of suvorexant was abnormal dreams. The most common adverse effect of suvorexant usage established during clinical trials for adults is daytime somnolence (Michelson et al. 2014). One meta-analysis reported that suvorexant causes a higher incidence of abnormal dreams in adults compared to a placebo, despite a small effect size (Kishi et al. 2015). Moreover, nightmares more frequently occurred in participants with insomnia than those without; and nightmare and insomnia are known to be associated with the development of depression (Nakajima et al. 2014). As the prevalence of nightmares was 35.2% in Japanese adolescents, careful consideration is needed before prescribing suvorexant (Munezawa et al. 2011). The meta-analysis also showed that suvorexant was superior to a placebo with regard to subjective total sleep time and subjective time to sleep onset; however, suvorexant was not superior to a placebo with regard to the subjective quality of sleep as assessed by the Insomnia Severity Index score at week 1 (Kishi et al. 2015). The power spectral profile of suvorexant is generally similar to placebo (Snyder et al. 2016). Two large randomized controlled trials (RCTs) (Blumer et al. 2009; Sangal et al. 2014) in pediatric insomnia associated with attention-deficit/hyperactivity disorder were performed in the United States. In these studies, nonbenzodiazepine hypnotics (Z-drugs), such as zolpidem and eszopiclone, failed to reduce latency to persistent sleep on polysomnography, and describe no superiority of Z-drugs to placebo. In this study, the continued suvorexant group showed significantly higher scores on the sleep quality of AIS than the discontinued group at the maintenance phase. Continuous administration of suvorexant might improve patients' perceptions of sleep quality. Although sleep problems were not evaluated by AIS before the administration of suvorexant and the effect on the sleep architecture of suvorexant was not investigated in our study, suvorexant may improve the subjective sleep quality on insomnia in adolescents.
The results of our study must be interpreted in light of a number of limitations. First, the total number of patients included in this study was relatively small and the type of administration was not uniform because it was up to the clinical judgment of the psychiatrists. Second, some patients took suvorexant in addition to another sleep medication. In addition, subjects who participated in this study included patients with comorbid psychiatric disorders. Third, we could not follow 5 out of 13 discontinued patients. These five patients might stop attending hospital because suvorexant was not effective. Use of AIS among adolescent may also have affected the result. Although AIS was reported to be a reliable and valid instrument in adolescents (Chung et al., 2011), AIS is usually used over 18 years of age. Furthermore, further prospective studies with larger samples sizes are needed to elucidate the effectiveness and safety of suvorexant in adolescents.
Conclusion
Suvorexant could improve the subjective sleep quality on pediatric insomnia in a clinical setting, and could be considered a treatment option of insomnia in adolescents.
Clinical Significance
This study adds important new information for the treatment of insomnia in adolescents as follows: (1) evaluate Suvorexant, the first reversible dual orexin receptor antagonist; (2) two female patients experienced abnormal dreams, and discontinued suvorexant; and (3) suggests that suvorexant may improve patients' perceptions of sleep quality as a new and useful hypnotic medication for insomnia in adolescents.
Footnotes
Acknowledgment
The authors thank all the participants who participated in this study.
Disclosures
No competing financial interests exist.