
Abstract

Chief Complaint and Presenting Problem
N.
History of Present Illness
N. first came to clinical attention 5 months before his first admission, when his pediatrician referred him to a child and adolescent psychiatrist for self-injury.
N. had a long history of self-injury dating to age 14. The first time he cut he recalled it was at night, and he was on the phone talking to a friend. He became emotional and felt he needed “something strong.” He took a serrated kitchen knife and cut his arm; that action produced a burning sensation, but no blood. Over the next few days, N. repeatedly cut himself harder and harder until he drew blood. He soon discovered his brother's shaving razor and started using it to cut. However, the razor produced more prominent scars, and so, N. started cutting his thighs. He reported that he cut every other day, explaining that the pain would last for 1–2 days at a time. He reported that the intent of cutting was to calm himself down, but stated that sometimes he cut even when not stressed, as “it's just something I have to do.” He did not have a ritualized manner. He reported he told several friends of his cutting but did not like to discuss it with them at length. The deepest he cut was to the superficial fat layer. He had never required suturing at the time of referral.
By the time N. started exhibiting self-injury, he also recalled feelings of frustration and anger in relation to his gender identity. N.’s dissatisfaction with his physical gender started early in childhood. As a late toddler, he never liked to play with dolls. Starting at age 5, he no longer agreed to wear dresses or pink clothing articles. N. wore only pants and liked the color red. At that age, he still dressed as a princess for Halloween, as that was the costume his mother bought him, but when he was in third grade, he told his mother from that point on he refused to be a princess.
When N. was in sixth grade, he reported that he wanted to look like a boy. At that time, he did not know he could take medications or have surgery to transition to a different sex, but merely wanted to change his appearance. At around age 14, feeling guilty about disappointing his parents, N. tried to dress “more femininely” to make them happy, but it only made him feel worse. It was during that period that he cut himself for the first time.
In eighth grade, N. started self-identifying as male. He told a few friends, and he started thinking about names, eventually choosing one that would let him keep the same initials. N. only “came out” to his mother and several other family members a year before his first admission. Since then, N. stated the atmosphere at home had been quite stressful. He reported his mother initially did not take the news very well but had later come to terms with it, and she was the only family member who referred to him by his male name. Other family members, including his father, continued to use his female name and pronouns.
A few months before his hospital admission, N. sent an e-mail to school staff asking to be referred to as male and with a male name. Following that request, many of his classmates did not know how to interact with him, and so, they kept their distance. This was a very isolating experience for N.
When N. was evaluated by the psychiatrist in the outpatient clinic, he was diagnosed with a depressive disorder related to his struggle with gender identity. He was subsequently started on sertraline 50 mg daily. Approximately 2 weeks later, N. experienced fleeting passive suicidal ideation for the first time in his life. He reportedly began to consume increased amounts of alcohol and marijuana, increased self-laceration, and increased absenteeism at school. N. began an escalation of use of alcohol obtained from his parents' home cabinet from a period of intermittent use to nearly daily use. He reported drinking to relieve anxiety. He engaged in intermittent use of marijuana with a similar function. Within a month, N. ingested 70 tablets of aspirin mixed with a pint of liquor with intent to die. N. did not seek medical attention and did not tell anyone of the attempt. N.’s psychiatrist subsequently increased his sertraline to 100 mg; ∼1 week later, N. was hospitalized for the first time when he consumed four 2 mg tablets of alprazolam purchased off the street, a 24 oz beer, a blunt of marijuana, and 1 g of cocaine. He was found unconscious in a park and when asked in the emergency department if he had had suicidal intent, he replied “I don't know.”
During his first hospitalization, N. was continued on sertraline 100 mg and started on aripiprazole 5 mg po qhs to augment the antidepressant and to target symptoms of emotional dysregulation; both served the primary goal of reducing risk for recurrent self-laceration. N. had no symptoms of overt mania; his sleep was intact, his mood was sad, his affect was constricted, and he endorsed multiple dissociative symptoms. There were no signs of psychosis. On day 3, N. requested a rubber band to snap against his wrist to cause pain; when this was declined, he repeatedly rubbed his hand with his thumb, causing skin sloughing and an abrasion.
N. was subsequently placed on constant observation. After a review of calming steps and cognitive behavioral interventions, constant observation was removed. N. was continued on q15m observation without further incident. His sertraline was titrated to 200 mg po and his disposition set to a partial hospitalization (PH) program. His suicidal ideation remained in remission throughout the hospital stay, and he was discharged in stable condition directly to the PH program.
At the program, N. relayed his history of self-injury, a prior suicide attempt, and substance use. N. confirmed that although he had used cocaine only once and alprazolam only a handful of times, he drank alcohol and smoked marijuana every other day to “calm down.” N. could not contract to refrain from use at the program. The PH program decided that N. would not benefit from services and was instead given referral information to a lower level of care in a community substance use clinic for adolescents.
N. reported feeling ashamed by the interaction with staff and his rejection from his planned recovery. He returned home, undressed, went into the shower, and began serially slicing his right thigh with a razor blade. He reportedly lost sense of time in the process, and experienced suddenly realizing that he had induced over a dozen slashes down to the fascia, including one that was over a foot long. He attempted to soak up the blood with a mop pad. He relapsed on alcohol through several cups of hard liquor and woke up the next morning with the pad soaked with blood. He asked his mother to go to the substance use clinic to pursue an appointment with a physician; during the intake, blood was soaking through his jeans and pooling in his chair. His mother walked him to the emergency department where he was readmitted.
The past was notable for an absence of significant anxiety, hyperactivity, impulsivity, and oppositional behavior. N. was reported to have a severe fear of insects since he was a toddler. N. was described as a perfectionist; he would make drawings and then throw them away if they were not good enough. He was reported to be very achievement oriented and would not give up when facing a challenge. In later years, he was reportedly described by teachers as a quiet child who did not voluntarily participate in class, but when asked, would always know the right answer.
Developmental History
N. was an unplanned pregnancy. Mother did not recall any difficulties with the pregnancy aside from nausea and vomiting in the first couple of months and during the last week. During the pregnancy, mother attended all prenatal visits although she did not take any prenatal vitamins. There was no substance exposure in utero. N. was born full term at 39 weeks, in a normal vaginal delivery, and weighed 3.175 kg. There were no peri- or postnatal complications. He met all developmental milestones on time. Mother described N. as a joyful baby, always happy and smiling.
Educational History
N.’s grades were very good, consistently above 95. When N. was in the first grade, he was bullied at school. He was younger, smaller, and of a different ethnicity than that of the other children. In fifth grade, N. was accepted into a gifted and talented class that he attended throughout junior high school. He continued to do well academically despite his psychiatric functional impairments.
Social History
N. was the youngest of three siblings. Mother reported that when she initially found out that she was pregnant, she debated terminating the pregnancy. She decided to keep her baby when she discovered that she was going to have a girl after having two boys (who were 8 and 5 years old at the time). She bought many pink dresses and other girly clothing items.
Parents had immigrated from a different country before N. was born and lived in a neighborhood of transplant first-generation immigrants. Soon after N. was born, father went to work in the country of their family origin, and N. was left in the care of his mother. Father continued to live abroad and was only present at home 2–4 months a year.
N. described having few friends, all of them from school and in the same age group. He denied sexual experience; he was reportedly not attracted to men or women.
Pertinent Family History
There was no known family history of psychiatric disorders.
Medical History
There was no significant medical history. Menarche occurred at age 12; N. recalled feeling upset, as it “took a more gendered meaning” as a feminine physiological process associated with child bearing. He felt his body “betrayed” him.
Medication History
At the time of referral, N. had been on sertraline 50 mg and titrated to 100 mg po at morning by his outpatient psychiatrist. On his first admission, aripiprazole 5 mg po qhs was added, and sertraline was shifted to evening administration. It was subsequently titrated to 200 mg po qam for a final regimen of sertraline 200 mg po qhs and aripiprazole 5 mg po qhs.
Mental Status Examination
On initial interview, N. was neatly groomed. He was generally cooperative, somewhat vague at times. There was a mild psychomotor retardation. His speech was slow but normal in volume. N. described his mood as “okay,” although his affect was constricted. His thought process was linear, goal directed, and coherent. His thought content was notable for thoughts related to dissociative states, “I feel as if I'm in another world.” He endorsed urges to self-injure but denied suicidal ideation. He reported visual hallucinations of flickering lights and shadows, and denied auditory hallucinations. His insight was limited as he was not aware of the damage of self-injury; “I don't see the problem in what I did.” He was unable to commit to refrain from self-injury.
Hospital Course
N. was admitted to the inpatient child and adolescent psychiatry unit under voluntary status on constant observation for his history of self-injury on the unit, indicators of dissociation on his mental status examination, and inability to refrain from engaging in self-injury.
N. underwent a detailed interview, which included administration of the Utrecht Gender Dysphoria Scale (UGDS) (Cohen-Kettemis and Van Goozen 1997) and the Gender Identity/Gender Dysphoria Questionnaire for Adolescents and Adults (GIDYQ-AA) (Deogracias et al. 2007; Singh et al. 2010). N. scored 55 of 60 possible points on the UGDS and 110 of 135 points on the GIDYQ-AA, both signifying an extremely high degree of gender dysphoria. N.’s subscores on the GIDYQ-AA showed high degrees of subjective, somatic, and socio-legal indicators of gender dysphoria.
N. was also asked to draw human figures of a man and a woman (Fig. 1), which showed an absence of any secondary sexual trait details, gendered clothing, or culturally gendered styles despite his great artistic talent in drawing.
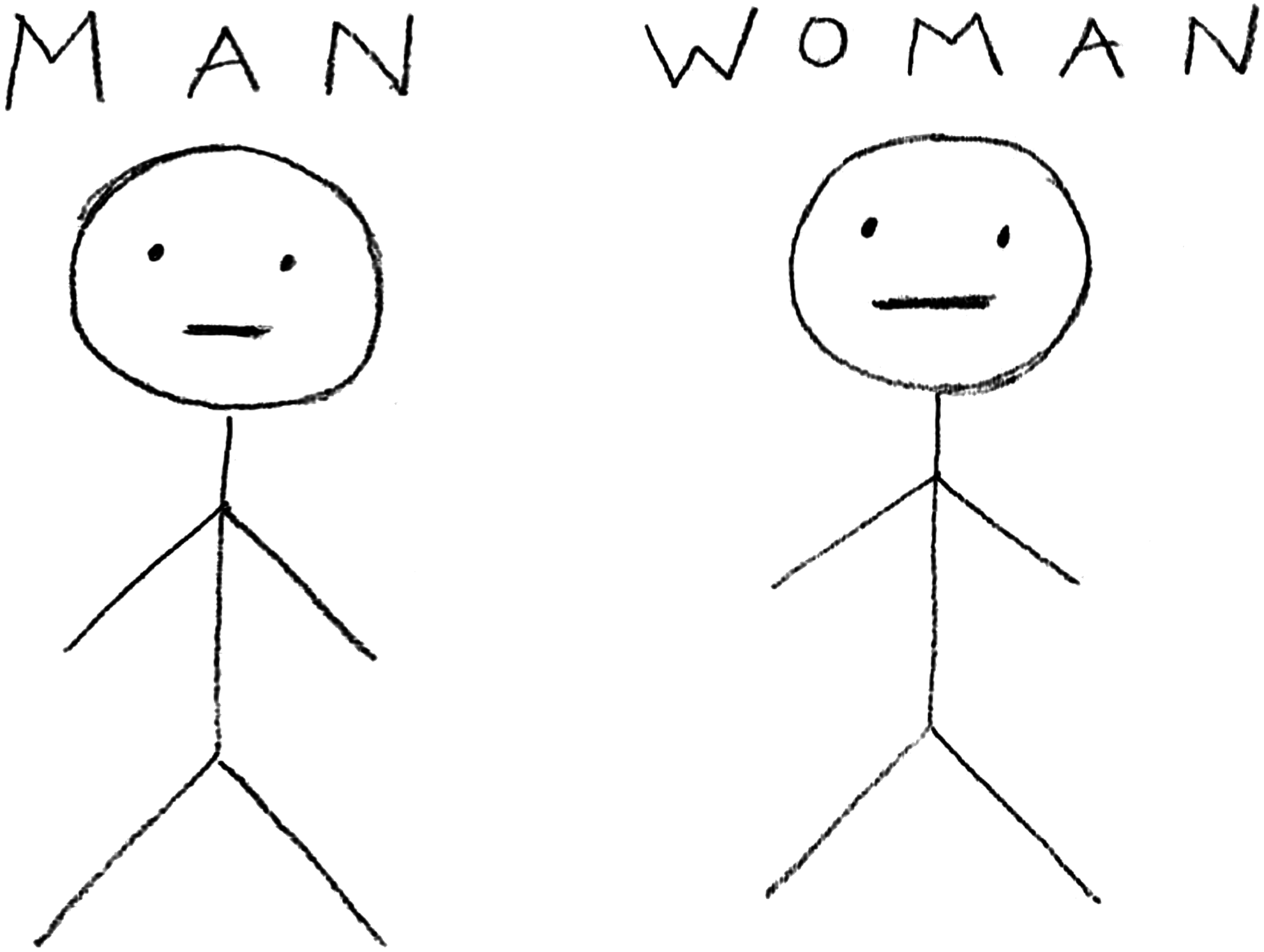
The patient was asked to draw human figures of a man and a woman.
On hospital day 1, aripiprazole 5 mg po at dinner was titrated to 10 mg and then to 15 mg on hospital day 3. N. endorsed a decrease in urges to self-injure and dissociation with this intervention, and was removed from constant observation status. However, on day 4, N. endorsed blurred vision and transient diplopia; tongue fasciculations were observed on physical examination. He received 1 mg benztropine × 1, his aripiprazole was held for one day, and then restarted again at 5 mg po with a full resolution of extrapyramidal signs. On day 6, lithium ER 450 mg po was recommended and started on hospital day 8 after obtaining mother's consent.
N. was engaged in multimodal psychosocial treatment, including individual, group, and milieu planning with a full resolution of his urges to self-harm. As in the prior hospitalization, he was taught to use progressive muscle relaxation, guided imagery, deep breathing techniques, and recourse to squeezing a stress ball. He was encouraged to express negative affect and thought content without self-incrimination. Communications included a neutral, nonjudgmental sharing of joint attention upon his physical wounds during dressing changes, while validating the sadness, isolation, and grief of his mental state associated with cutting.
This intervention was informed by an understanding of common experiences of individuals with gender dysphoria (Lopez et al. 2016) and included a series of interventions that had not been used during the first hospitalization when the significance and severity of gender dysphoria were not yet fully understood. N. was encouraged to identify, label, and share his affective experiences, and he gained some ability to transcend a dissociated relatedness and self-experience.
Despite all interventions described above, N. continued to endorse self-injurious urges and was unable to contract for safety after discharge. After discussing treatment options with N. and his mother, it was decided he would benefit from a longer hospitalization. N. was discharged to a state psychiatric facility on a medication regimen that included aripiprazole 5 mg po qam, sertraline 200 mg po qam, and lithium XR 450 mg po qam.
Brief Formulation
N. was a 16-year-old transgender boy whose most acute symptoms leading to inpatient hospitalization included the escalation of a pattern of self-destructive acts and self-neglect—most acutely, a severe act of dissociated self-injury.
From a biological perspective, N.’s longstanding discomfort with his female body and gender worsened at the time of puberty, and was associated with the onset of self-injury. N. may have been predisposed to his current presentation through time-dependent activation effects of his sertraline pharmacotherapy. There were no known general medical conditions or family history of psychiatric illness that might have contributed to his presentation.
From a psychological perspective, N. had significant discomfort with his gender role and identity. He lacked coping skills and manifested alexithymia. His difficulty in identification as an autonomous individual, distinct from his parents’ wishes for a female child, and his anger over this disconnect may have been a perpetuating psychological factor. His responsivity to psychoeducation and behavioral modeling was a protective factor.
From a social perspective, N. came from a first-generation family that was still undergoing the acculturation process with the associated difficulties, including family isolation, tension between cultures, and a sense of diffused identity in the children. His father's absence during key developmental phases could also have contributed to N.’s presentation. N. was socially isolated and had few close friends. There was a negative or at best neutral response in the community to his coming out as a transgendered individual, as well as within his nuclear family.
Multiaxial Diagnoses
AXIS I: Gender dysphoria
Major depressive disorder, single episode, severe, without psychotic features
Alcohol use disorder, severe
Marijuana use disorder, moderate
AXIS II: Diagnosis deferred
AXIS III: None
AXIS IV: Problems with primary support group. Problems related to social environment
AXIS V: GAF 45
Discussion
Recent literature on the approach to adolescents with gender dysphoria provides strong guidance for working with this population (Leibowitz and de Vries 2016; Lopez et al. 2016). Additional literature guides the pharmacotherapy of severe self-injury in adolescents (Hawton et al. 2012, 2015). However, to date, no studies specifically focus on pharmacotherapy of self-injury in adolescents with gender dysphoria, despite several reports noting high rates of NSSI in this population (Marshall et al. 2016). N.’s history and presentation illustrate that severe self-injury in adolescents with gender dysphoria does occur, and warrants a specific synthesis of knowledge from both bodies of literature.
First, it is important to identify and include gender dysphoria in the diagnostic formulation, as individuals with this condition have significantly different comorbidities from their nonaffected peers, including a 4.3 relative risk of self-harm (Reisner et al. 2015). Nearly half of transgender youths report a history of suicidal ideation, and a quarter report suicide attempts (Grossman and D'Augelli 2007). Among adult transgender individuals, as many as 41% report a history of suicide attempts (compared to 1.6% of the general population), suggesting that, without treatment, advancing age raises these numbers from those seen in adolescent populations (Grant et al. 2010). Prevalence of substance use disorders have also been reported to be higher in transgender individuals compared with the general population (Keuroghlian et al. 2015).
Risk factors for NSSI among transgendered adolescents include impaired interpersonal functioning and low social support (Claes et al. 2015), and they can be targeted for psychosocial intervention. Interventions with parents (Riley et al. 2011) and schools can be beneficial for the transgender individual (Russell et al. 2014). Education for all members of the inpatient treatment team is also important (Chapman et al. 2012). Up to half of all transgender individuals report having to educate their providers on transgender care (Grant et al. 2010), suggesting that this lack of specific knowledge was not unique in N.’s care. The level of N.’s acceptance by his family, school, and healthcare team was addressed to fit the pharmacological intervention undertaken within a socioecological model.
Guidelines on NSSI suggest—but cannot clearly demonstrate—that psychopharmacological intervention for NSSI is effective in the child and adolescent (Hawton et al. 2015) and young adult populations (Turner et al. 2014). Thus, N.’s team decided to apply this scientific evidence to his care (Claes et al. 2015; Aitken et al. 2016; Davey et al. 2016). First, comorbid depression and dissociation were addressed through the titration of the selective serotonin reuptake inhibitor (Claes et al. 2015). Second, the team decided to add a neuroleptic to augment the antidepressant and target deficits in emotional self-regulation, which have been associated with NSSI (Andover and Morris 2014; McKenzie and Gross 2014). However, the onset of extrapyramidal symptoms (partially due to the interaction between sertraline and aripiprazole) foreclosed the possibility of this neuroleptic. Finally, a trial of lithium was undertaken as an agent for refractory self-injury (Smith 2005). The history of potential activation on sertraline monotherapy supported this decision.
Guidelines have been developed for gender dysphoria which incorporate endocrinological interventions to control sexual development (Hembree et al. 2009; Wylie et al. 2016). Young adolescents extremely distressed by pubertal body changes may receive treatment with gonadotropin releasing hormone agonists (GnRHa) to delay puberty (Kreukels and Cohen-Kettenis 2011). This may allow extended time for diagnosis and prevention of untoward clinical outcomes, including suicidality and self-injury. Although positive psychological adjustment has been demonstrated in one study with young transgender adults who had received puberty suppression during adolescence (de Vries et al. 2014), more research about safety, long-term psychological benefits and optimal concurrent medical and mental healthcare of prolonged puberty suppression with GnRHa is required. This intervention was not indicated in N.’s case, because of his developmental stage and psychiatric disorders, which are considered an exclusionary factor by major guidelines (Hembree et al. 2009).
For older adolescents for whom GnRHa therapy is no longer an option, cross-gender hormone therapy can be used to promote secondary sexual characteristics and reduce gender dysphoria. Guidelines that identify eligibility and readiness criteria include (1) persistent, well-documented gender dysphoria, (2) capacity to make a fully informed decision, (3) age of majority, and (4) reasonably well-controlled medical or mental health concerns (Coleman et al. 2012; Leibowitz and de Vries 2016). Taken together, N. did not meet the criteria for this intervention during hospitalization.
Even if coordinated as an outpatient, treatment with sex hormones may have untoward effects. Testosterone therapy for transgender men is a proven treatment (Irwig 2016), but it has been related to physical and psychological adverse effects (Wierckx et al. 2014). When suicidal and violent behavior appears with the use of testosterone, major guidelines recommend deferring therapy until associated comorbid psychiatric illnesses with increased suicide and violence risk are controlled (Rice and Sher 2013, 2015; Sher 2013, 2014; Rice et al. 2015).
In conclusion, this case report draws attention to self-injury in adolescents with gender dysphoria and illustrates an important need for further research on pharmacological interventions for this population.
Footnotes
Acknowledgment
We acknowledge and thank Maxwell Luber for his assistance in the review and preparation of the article.
Disclosures
No competing financial interests exist.