
Abstract
Introduction:
A wide range of psychiatric disorders are common in young children, especially in those at high risk because of a parent with a unipolar or bipolar mood disorder in the United States. Yet in part because most children are seen in primary care, these illnesses are often not recognized or treated in a timely fashion. To begin to address this problem, we started the Child Network.
Methods:
The Child Network is for parents of children age 2–12 with mood or behavioral symptoms or at high risk for them. The parents rate the severity of symptoms of depression, anxiety, attention-deficit/hyperactivity disorder (ADHD), oppositional behavior, and mania on a once a week basis on a secure website under a Johns Hopkins Intramural Review Board (IRB)-approved protocol. These ratings can then be printed out along with any treatments given to aide in visualization of symptom course. A demographics form, which includes diagnoses given to the child in the community, and a symptom checklist are filled out upon Network entry. We report on the retrospective diagnoses and prospective treatment of the first 65 parents to join the Network.
Results:
The most common diagnoses were anxiety disorders and ADHD followed by disruptive behavioral disorders and bipolar spectrum disorders. Prospective ratings of two or more consecutive weeks of moderate to severe rating in any of the five symptom domains paralleled these diagnoses given in the community. Atypical antipsychotics, anticonvulsant mood stabilizers, and medications for ADHD were among the most widely used drugs. An illustrated example of symptom course is presented.
Discussion:
Many children continued to show substantial symptom severity despite treatment with an average of 2.2 medications. The Child Network provides a useful longitudinal approach to visualize the course of symptoms, which should help lead to earlier and more effective treatment.
Introduction
T
In an effort to begin to address the issue of fostering earlier recognition and treatment in the community, we developed the Child Network (Post 2016a, 2016b). The Child Network is for parents of children age 2–12 to rate on a weekly basis their child's mood and behavioral symptoms on a secure website, accessed at
In this article, we present an example of the ratings of a highly symptomatic child despite the variety of treatments utilized. We also give a preliminary view of the diagnoses at entry and treatments received during Network participation in most of the first 65 children to be registered in the Network.
Methods
We illustrate the graphic depiction of the course of symptoms in a child who was rated weekly by his parents for 1 year in the Network. The course of each of the five symptoms is plotted along with the delineation of pharmacological and psychosocial treatments given.
Diagnoses of the child already made in the community were elicited from the parent on a questionnaire, which listed 23 diagnoses of common psychiatric disorders of childhood. Parents rated each diagnosis as follows: not diagnosed, possibly, likely, or definitely diagnosed, and we considered ratings of likely or definitely as positive.
The mean number of diagnoses of the children enrolled was 2.6 ± 0.35. Forty-three percent had not previously received any diagnosis. Six percent of the children each received one, two, three, and four diagnoses respectively, 15% received five diagnoses, 8% had six diagnoses, and 10% had seven or more diagnoses made in the community. Forty-nine of the 64 children (77%) were from the United States, and no more than three children were from any other country.
Results
ADHD was the most prevalent community-based diagnosis with 32% of the children positive for it. Generalized Anxiety Disorder (GAD) was next highest at 28% and the other six anxiety disorder diagnoses ranged from 20% for separation anxiety to 8% for school phobia and panic disorder, such that any anxiety disorder was present in 44.6% of the children. Bipolar not otherwise specified (BP-NOS) was diagnosed in 18% of the children, while 11% had a diagnosis of BP I, 5% BP II, and 2% cyclothymia. Oppositional defiant disorder was diagnosed in 23%, intermittent explosive disorder in 9%, and severe mood dysregulation or dysphoric mood dysregulation disorder occurred in 8%, while conduct disorder was seen in only one individual (2%), yielding a total of 27.7% of the children having any of these disruptive behavioral disorders. Bipolar disorder was diagnosed in one parent in 50.8% of the participants, and in both parents in 3.4%. However, the mean number of diagnoses was lower (at the trend level p = 0.053) in the children of a parent with bipolar disorder (2.18) compared to those without a bipolar diagnosis (3.59).
Of the children who had longitudinal ratings of at least 4 weeks, the percent who had ratings of two consecutive weeks of moderate or severe for each symptom was as follows: anxiety in 48.5%; depression in 24.2%; ADHD in 63.6%, oppositional behavior in 63.6%, and mania in 39.4.
Figure 1 illustrates one of the several of the children in the Network showing a difficult poly-symptomatic presentation and the relatively inadequate response to multiple agents and therapies that had been utilized during naturalistic treatment in the community. Despite continued treatment with lamotrigine and the addition of three different atypical antipsychotics and several different types of psychosocial interventions, substantial degrees of dysfunction in each symptom domain remained.
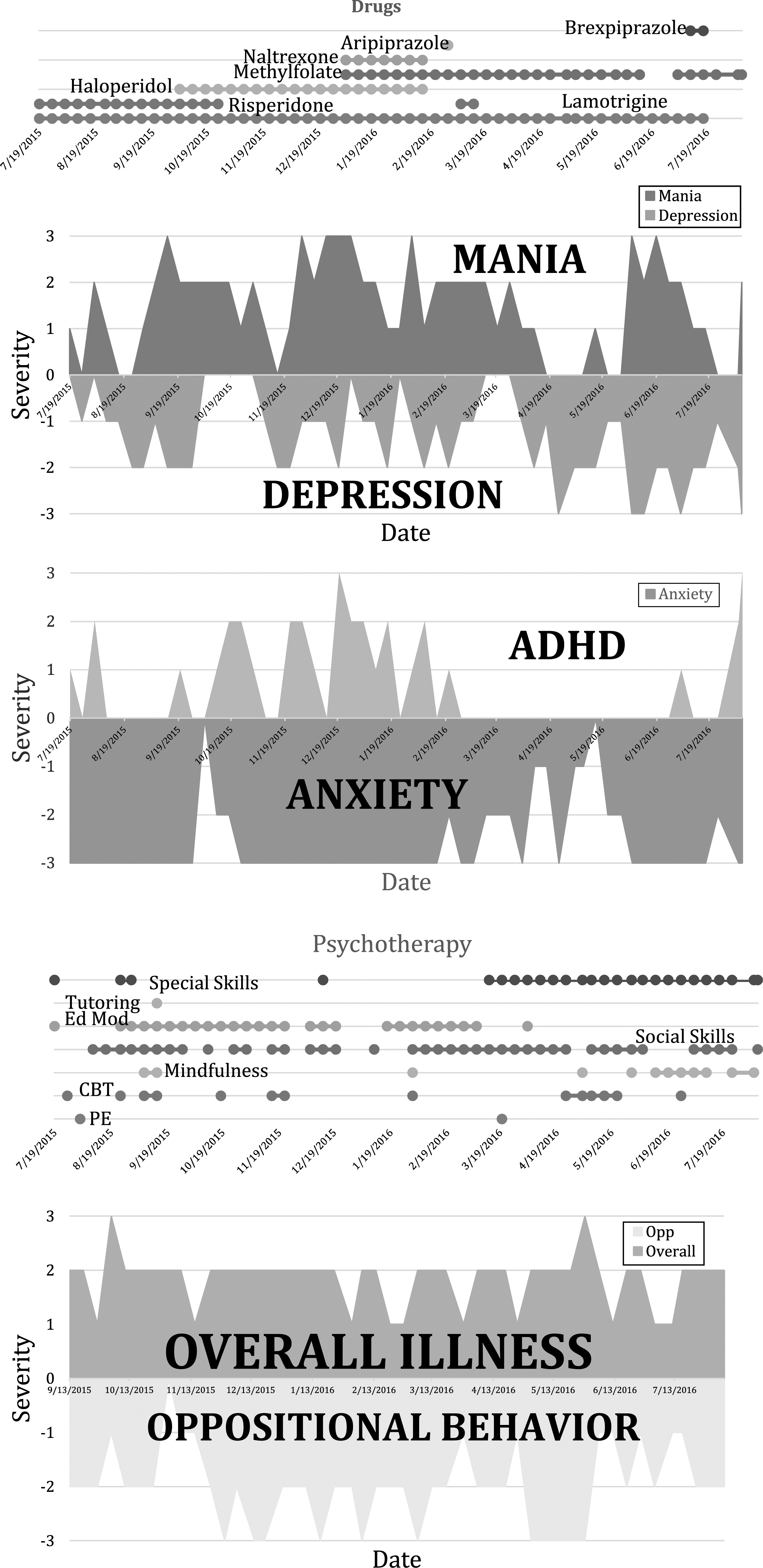
Ratings of each of the five symptoms were on a scale of 1, mild dysfunction; 2, moderate dysfunction; 3, severe dysfunction on a weekly basis from June 2015 to June 2016. Medications utilized are listed above the ratings; therapies are listed above the ratings of overall illness. CBT, cognitive behavioral therapy; Ed Mod, educational modifications; PE, psychoeducation.
Discussion
As might be expected in children age 2–12 (average age 7.8) ADHD and anxiety disorders were the most frequent diagnoses of the children of parents enrolled in the Child Network. Many children continued to be symptomatic (moderate or severe ratings) despite treatment with an average of 2.2 medications/day, and multiple types of medications as illustrated in the figure.
The diagnoses made in the community are consistent with the high prevalence of ADHD, anxiety disorders, depression, and disruptive behavioral disorders in this age range in clinical- or population-based samples (Birmaher et al. 2009; Merikangas et al. 2010; Axelson et al. 2015; Gleason et al. 2016; Mesman et al. 2016). The large percentage of children remaining moderately to severely impaired despite multimodal treatment is particularly noteworthy.
This small sample needs to be expanded before statements can be made about treatment patterns in those with different diagnoses and dysfunctional symptoms, but the preliminary data are already suggestive of the greater need in the community for better recognition and treatment of common diagnoses in children. In particular, those children at increased risk for a psychiatric diagnosis because of a positive family history of bipolar disorder or depression deserve greater attention and treatment if necessary.
Axelson et al. (2015) indicated that 74% of the offspring of a parent with bipolar disorder would have a lifetime psychiatric diagnosis upon 6.7 years of follow-up. In that high-risk study, anxiety disorders, depression, ADHD, and disruptive behavioral disorders were more common than a diagnosis of a bipolar spectrum disorder (which occurred in about 20% of the children). Likewise, Weissman et al. (2006) in a 20-year follow-up study, reported an 80% incidence of a lifetime psychiatric diagnosis in the offspring of a parent with unipolar depression. Strikingly, in the studies of Axelson et al. (2015) and Weissman et al. (2006), ∼50% of the offspring of the community controls also had received a similar range and relative proportion of lifetime psychiatric diagnoses, indicating a very high incidence of illness in the United States even in those not at risk because of a positive family history of a mood disorder (Post et al. 2017).
As the size of the Network increases, it will offer other assets. We will be able to see how common illnesses in very young children are actually being treated in the community. This is of importance as there are no Food and Drug Administration-approved drugs for children under 10 years of age with the exception of those for ADHD. We will also be able to preliminarily describe how apparently effective different agents are for the different conditions, and how well they are tolerated (Post 2016a, 2016b). This will allow assessment of the major gaps in the literature on treatment effectiveness and relative tolerability that then might inform and stimulate more systematic and controlled clinical trials to begin to close these gaps.
As illustrated in the figure, multiple drugs are often used in combination in an effort to bring highly symptomatic children into remission. Particularly, in children with bipolar disorder who have many psychiatric and medical comorbidities the literature supports the view that combination treatment is more effective than monotherapy. However, the systematic treatment literature rarely goes beyond the exploration of two drug combination therapy, and how to use which drugs in which sequences for the treatment refractory patient has not been studied. An expansion of the Child Network and an extension into a clinical trials network in clinical practice settings would do much to begin to address the deficits in the systematic treatment literature on childhood bipolar disorder and related syndromes.
Conclusion
In addition to the presence of mood disorders in the parents, a history of a range of psychiatric difficulties in the grandparents appears to contribute to the risk of multiple psychiatric illnesses in the offspring (Post et al. 2015a, 2015b, 2016). Therefore, a two generation family loading for psychiatric illness, taken in conjunction with a history of adversity in a child's early life should heighten awareness of a range of psychiatric disorders in the offspring (Post et al. 2013). The additional presence of prodromal symptoms occurring in the child would further increase the risk for a major psychiatric illness (Post et al. 2013). Ratings in the Child Network would be an ideal way of assessing of subsyndromal symptoms in both high risk and normal risk children.
Longitudinal ratings by parents of highly symptomatic children (as in Fig. 1) would be helpful to clinicians making decisions about need for treatment and treatment revision. Pediatricians and other primary care physicians who now see the majority of children with psychiatric illness (Anderson et al. 2015) are encouraged to be increasingly actively involved in the assessments, referrals, and treatment of these children (Shonkoff and Garner 2012; Gleason et al. 2016).
The weekly ratings of depression, anxiety, ADHD, oppositional behavior, and mania in the Child Network provide for a longitudinal view of the symptoms present in many of the most common diagnoses of childhood psychiatric illness. While not a formal diagnostic instrument, the printouts of the weekly ratings in the Child Network provide clinicians and physicians a unique longitudinal perspective on the trajectory of the symptoms involved and their improvement or not in the face of psychosocial or pharmacological treatment. In particular, given the high risk for psychiatric illness in offspring of a parent with a mood disorder in the United States (Weissman et al. 2006; Axelson et al. 2015), parents of children at high risk for or already having psychiatric difficulties could be encouraged to join the Child Network (available at
Clinical Significance
Most children with psychiatric difficulties in the United States are seen by primary care providers. Parents' weekly ratings of depression, anxiety, ADHD, oppositional behavior, and mania on a secure website can assist clinicians in early recognition and treatment of a wide range of common psychiatric disorders of childhood.
Footnotes
Acknowledgments
We thank the parents who have joined the Child Network and provided the data for this report.
Disclosures
R.M.P. has been a speaker for and received honoraria from Astra Zeneca, Sunovion, Validus, Teva, Tekada, and Nestle-Pamlabs. R.F., M.R., and D.K. have no conflicts of interest to declare.