
Abstract
To the Editor:
T
The patient was referred for treatment-resistant vocal and motor tics, hyperactivity, impulsivity, inattention, aggressive, and obsessive–compulsive behavior. Attention-deficit/hyperactivity disorder (ADHD) symptoms began by age 3, obsessive–compulsive behavior by age 5, and tics, including coprolalia and copropraxia, by the age of 7. The parents described worsening of these symptoms in the last 2 months.
He was using haloperidol 15 mg/day and pramipexol 1 mg/day with very little improvement in tics, which included coprolalia, copropraxia, touching and kissing others, licking his fingers and shoulder, echolalia, and facial expressions. His past treatments included adequate doses of various typical and atypical antipsychotics, clonidine, guanfacine, benzodiazepines, anticonvulsants, lithium, selective serotonin reuptake inhibitors, methylphenidate, atomoxetine, hyperbaric oxygen therapy, steroid treatment, plasmapheresis, and all failed to relieve the symptoms. He could not comply with behavioral treatment because of severe ADHD symptoms. He was expelled from school because of unremitting tics and disruptive behavior.
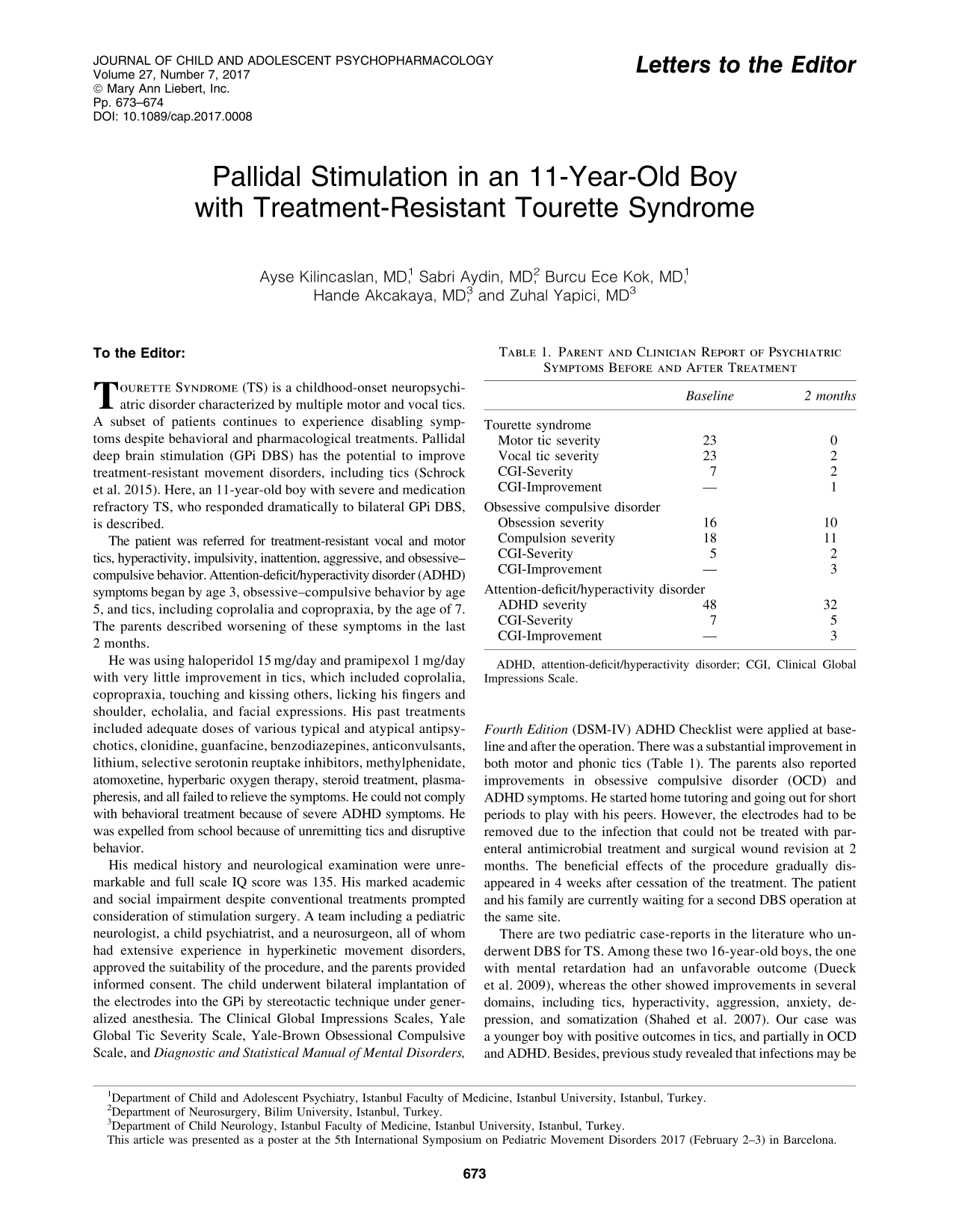
His medical history and neurological examination were unremarkable and full scale IQ score was 135. His marked academic and social impairment despite conventional treatments prompted consideration of stimulation surgery. A team including a pediatric neurologist, a child psychiatrist, and a neurosurgeon, all of whom had extensive experience in hyperkinetic movement disorders, approved the suitability of the procedure, and the parents provided informed consent. The child underwent bilateral implantation of the electrodes into the GPi by stereotactic technique under generalized anesthesia. The Clinical Global Impressions Scales, Yale Global Tic Severity Scale, Yale-Brown Obsessional Compulsive Scale, and Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) ADHD Checklist were applied at baseline and after the operation. There was a substantial improvement in both motor and phonic tics (Table 1). The parents also reported improvements in obsessive compulsive disorder (OCD) and ADHD symptoms. He started home tutoring and going out for short periods to play with his peers. However, the electrodes had to be removed due to the infection that could not be treated with parenteral antimicrobial treatment and surgical wound revision at 2 months. The beneficial effects of the procedure gradually disappeared in 4 weeks after cessation of the treatment. The patient and his family are currently waiting for a second DBS operation at the same site.
ADHD, attention-deficit/hyperactivity disorder; CGI, Clinical Global Impressions Scale.
There are two pediatric case-reports in the literature who underwent DBS for TS. Among these two 16-year-old boys, the one with mental retardation had an unfavorable outcome (Dueck et al. 2009), whereas the other showed improvements in several domains, including tics, hyperactivity, aggression, anxiety, depression, and somatization (Shahed et al. 2007). Our case was a younger boy with positive outcomes in tics, and partially in OCD and ADHD. Besides, previous study revealed that infections may be more common in subjects with TS. Servello et al. (2011) reported that DBS-related infection rates were 18% in TS compared to 3.7% overall (including DBS for Parkinson's disease, dystonia, and essential tremor).
In conclusion, GPi DBS may be a very effective treatment option for the selected children with TS. Psychiatric comorbidities should not necessarily preclude stimulation surgery. However, infections may complicate and cause cessation of the treatment.
Footnotes
Disclosures
Z.Y. is an unpaid researcher in the Phase 3 trial of everolimus in treatment refractory seizures associated with the Tuberous Sclerosis Complex. Other authors have nothing to disclose. The authors received no financial support for the research, authorship, and/or publication of this article.