
Abstract
Objectives:
To describe a cohort of young users of risperidone and quetiapine in the province of Manitoba (Canada) and assess the risk for movement disorders in the two treatments.
Methods:
This was a population-based study conducted on all residents of the province of 19 years of age and younger who received prescriptions for risperidone or quetiapine between April 1, 1996, and March 31, 2011. Incident rates of antipsychotic use were reported. The risk for movement disorders in patients treated with quetiapine compared with those treated with risperidone was assessed by time-to-event analysis using Cox proportional hazards models.
Results:
Between April 1, 1996, and March 31, 2011, 23,888 youth (age ≤19 years) were prescribed an antipsychotic agent. Among them, 8756 were identified as new incident users. After applying exclusion criteria, 2594 individuals comprised the cohort of users of risperidone and quetiapine. The use of quetiapine was associated with a lower risk of extrapyramidal symptoms (EPSs) adverse events. The unadjusted and adjusted hazard ratios (95% confidence interval [CI]) for quetiapine versus risperidone were 0.83 (0.56–1.25) and 0.53 (0.34–0.83), respectively.
Conclusion:
EPS diagnoses have been detected in children treated with quetiapine; however, the risk of movement disorders appears to be higher with treatment with risperidone. Clinicians should always take into consideration the risk–benefit before treating children with antipsychotic medications and should be vigilant of the onset of drug-induced adverse events.
Introduction
C
High rates of prescribing antipsychotics to children and adolescents have been reported in recent years (Alessi-Severini et al. 2012; Patten et al. 2012; Zito et al. 2013; Olfson et al. 2015; Bachmann et al. 2014; Hartz et al. 2016; Huskamp et al. 2016). Official indications of SGAs in pediatric populations vary across countries (Penfold et al. 2013; Bachmann et al. 2014; Huskamp et al. 2016). FDA-approved use for risperidone, olanzapine, quetiapine, and aripiprazole in children and adolescents includes schizophrenia and bipolar disorder; riperidone and aripiprazole are also approved for the treatment of aggressive behaviors in young patients diagnosed with autism spectrum disorder (Penfold et al. 2013; Huskamp et al. 2016). In Canada, only aripiprazole is indicated for adolescents diagnosed with schizophrenia or bipolar disorder (Health Canada 2015); the official product monographs of the other SGAs explicitly state that the safety and efficacy of such products have not been established in children under the age of 18 years (Health Canada 2015). As a result, the use of antipsychotics in pediatric populations has largely been off-label (Alessi-Severini et al. 2012; Murphy et al. 2013; Burcu et al. 2014; Huskamp et al. 2016).
The aims of this study were to describe incidence rates of antipsychotic use in children and adolescents (≤19 years of age) in the province of Manitoba (Canada) and to assess the risk for movement disorders in patients treated with risperidone compared with those treated with quetiapine, which is currently the second most used antipsychotic agent prescribed to children in Canada (Alessi-Severini et al. 2012; Murphy et al. 2013; Pringsheim and Gardner 2014).
Methods
This study was a population-based retrospective cohort of all children and adolescents (age 0–19 years) living in the Canadian province of Manitoba (total population ∼1.2 M) served by a universal healthcare system.
Data were obtained from the administrative healthcare databases of the Manitoba Population Health Research Data Repository housed at the Manitoba Centre for Health Policy (MCHP). The Repository is a comprehensive collection of administrative, registry, survey, and other data relating to virtually all registered residents of the province. All individual contacts with the universal provincial healthcare system, including physician visits, hospitalizations, and pharmaceutical prescriptions, are captured and linkable through the use of one 9-digit identifier, which is scrambled to protect privacy (Brownell et al. 2006; Fransoo et al. 2008). Data are suppressed (not revealed or published) when the number of persons or events involved is five or less. This process of suppressing data is conducted to avoid potential identification of individuals residing in areas of low-density population. Databases accessed and linked included the Manitoba Health Insurance Registry, Drug Program Information Network (DPIN), Hospital Abstracts, Medical Services, Statistics Canada Census, and Vital Statistics.
Incident rates of second-generation antipsychotic use between April 1, 1996, and March 31, 2011, were described. Incident users were defined as individuals ≤19 years of age at the date of their first antipsychotic prescription (no previous use of any antipsychotic in the year prior). Individuals with a pre-existing condition of a movement disorder identified by the appropriate diagnostic codes (ICD-9-332, 333, 781 and ICD-10-G20-G26) or a prescription for a medication to treat the condition were excluded, subjects who spent >25% of the year before cohort entry in hospital were also excluded from the study (as the DPIN database does not include information on prescriptions administered in hospitals). Furthermore, only individuals fulfilling the “persistent use” definition (MCHP Concept Dictionary, 2016), by which prescription refills cover at least 80% of the observation time, were included in the comparison. Individuals were followed for up to 1 year from index date and censored when any of the following occurred: event of interest (diagnosis in medical or hospital records of movement disorders, extrapyramidal symptoms [EPSs]) and end of the last prescription (dispensing date plus days' supply) before a gap of >30 days; switch to another agent; a hospital episode of care lasting >30 days (for the already mentioned reason that medication use in hospital is not captured) unless caused by an event of interest and end of health coverage (e.g., individual leaving the province); death; or end of the study (March 31, 2011). Please note that cohort entry was stopped at March 2010 to allow for the 1 year of observation in individuals entering the cohort in 2010. Please refer to Figure 1 for details on the cohort definition.
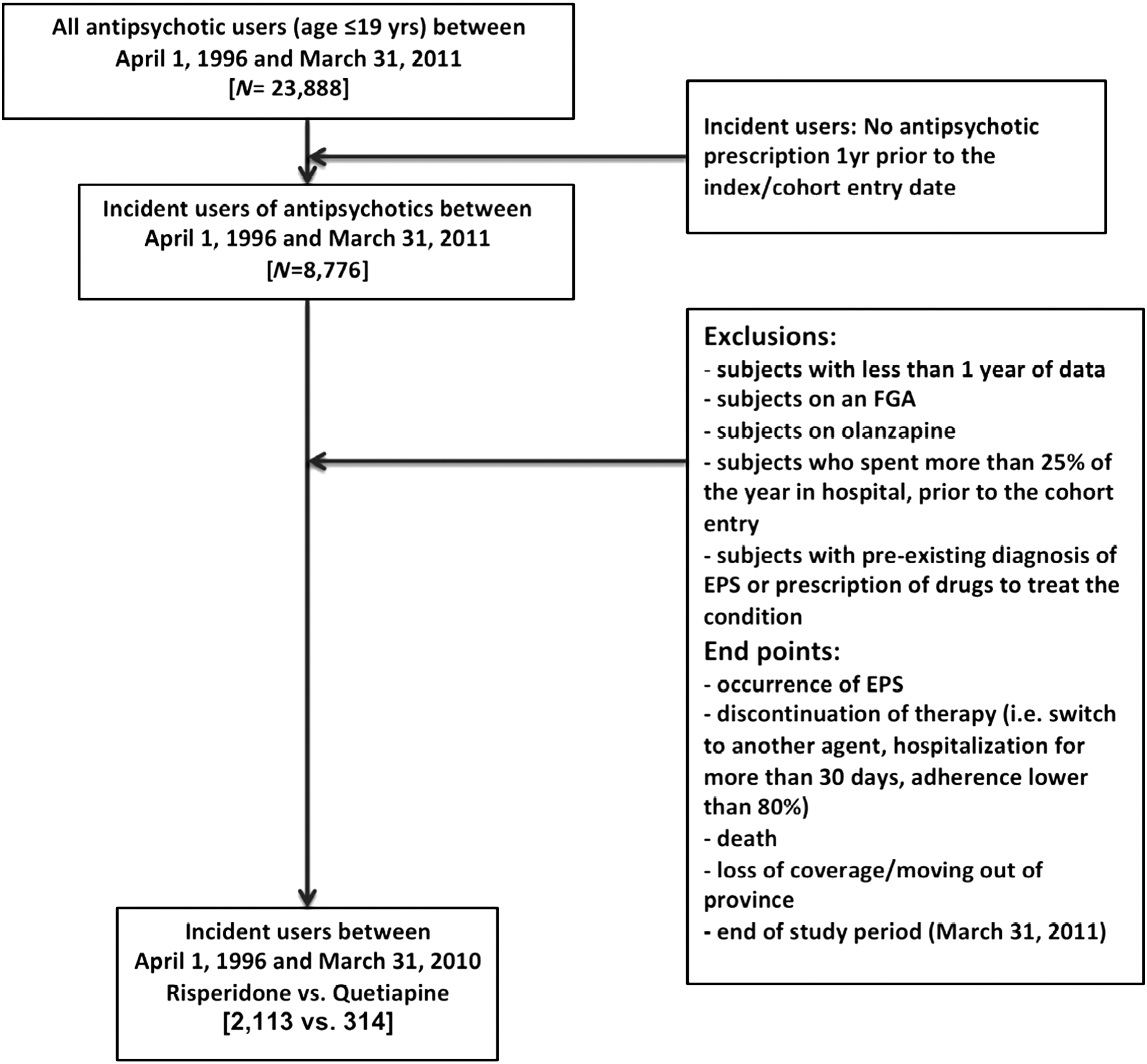
Cohort definition.
Descriptive statistics were used to report incidence rate of antipsychotic use and to characterize the cohort of incident users of risperidone and quetiapine. Time-to-event analysis using Cox proportional hazards models was conducted to compare hazard ratios (HRs) between the two treatment groups. Adjustments for potential confounders such as age, gender, socioeconomic status, and comorbid diseases, identified by the use of Aggregated Diagnosis Groups, ADGs®, part of Johns Hopkins Adjusted Clinical Group® (ACG®) Case-Mix System (software version 9), were conducted. Adjustments were also made for the use of other medications. In particular, adjustments were made for use of medication associated with development of movement disorders (i.e., metoclopramide, tetrabenazine, reserpine, methyldopa, amiodarone, valproate, and lithium). Furthermore, adjustments were made for the index year to control for potential changes in prescribing patterns.
Significance of confounders was determined by t-test and chi-square test and a p-value <0.05 was considered to represent significance. Crude event rates were calculated using the number of events per 100 person-years.
Analyses were performed using SAS statistical software for Windows, version 9.3 (SAS® Institute, Cary, North Carolina). All analyses were conducted from a remote access site of the MCHP located in the College of Pharmacy, University of Manitoba.
This study received ethics approval from the Health Research Ethics Board of the University of Manitoba. It was conducted in compliance with the Personal Health Information Act of Manitoba and was approved by Manitoba's Health Information Privacy Committee.
Results
According to Statistics Canada, the general youth population of Manitoba ranged from 327,796 to 327,551, between 1996 and 2011. From the data available in the Manitoba Population Health Research Data Repository, the total user population, who were prescribed at least one antipsychotic agent between April 1, 1996, and March 31, 2011, included 23,888 youth (age ≤19 years). Among these, 8776 were identified as incident users of an antipsychotic medication. First-generation antipsychotics (e.g., haloperidol and phenothiazines) have not been generally prescribed to children because of the recognized risk for movement disorders; results from this study confirmed a very limited utilization. The only SGAs available on the Canadian market during the study period were risperidone, olanzapine, quetiapine, and clozapine; as expected, utilization of clozapine was negligible in this patient population. Incidence rates of antipsychotic use in the pediatric population of Manitoba for a 15-year period are reported in Figure 2.
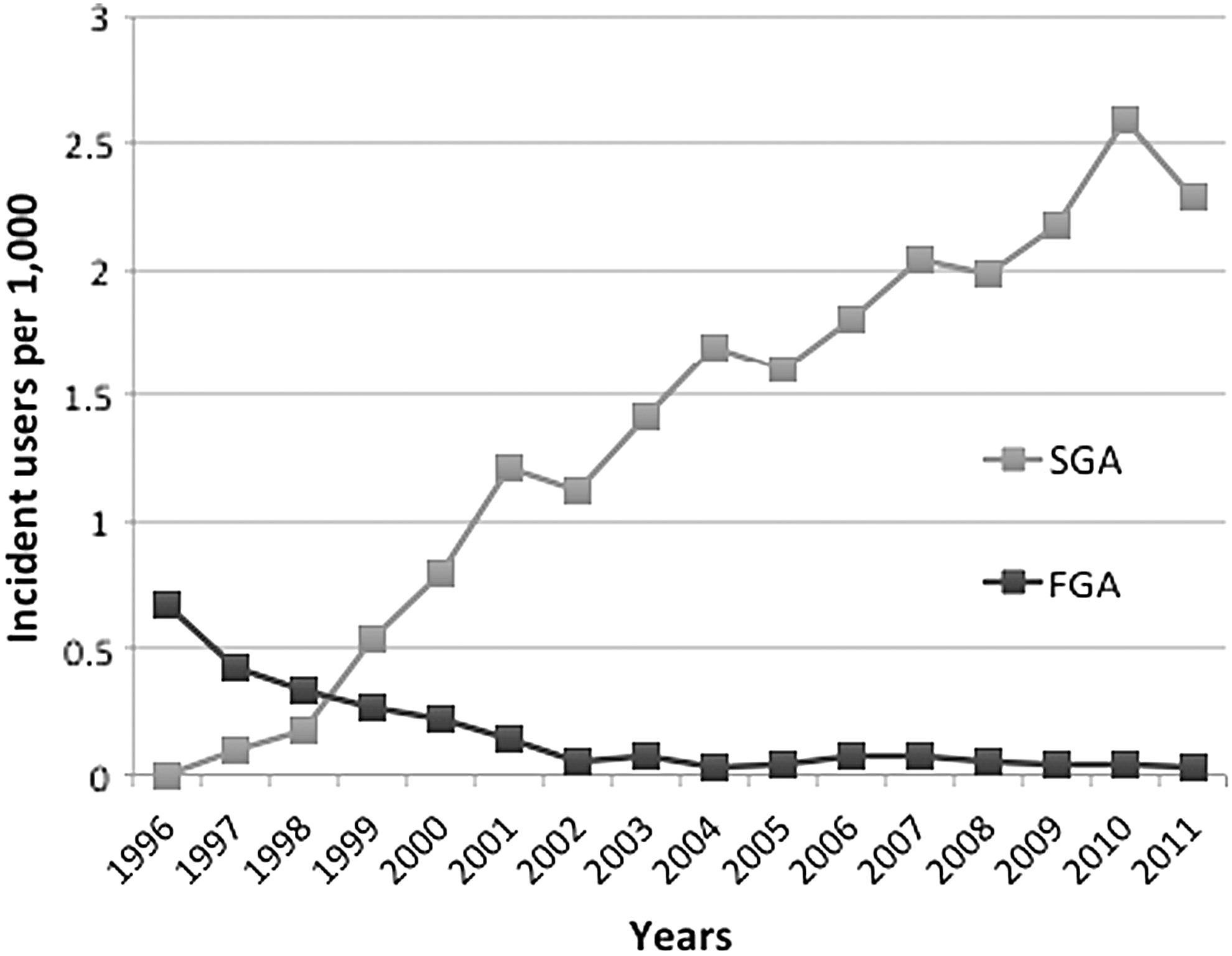
Incident use of antipsychotic agents (1996–2011).
After applying all exclusion criteria, 2427 individuals were selected from the initial cohort of SGA users and were included in the EPS comparison of risperidone with quetiapine (Fig. 1). Baseline characteristics of the two groups are presented in Table 1. Significant differences were observed between the groups in terms of age, gender distribution, income, diagnosis of attention-deficit/hyperactivity disorder, autism, mood disorders, and conduct disorders. Use of additional medications was also significantly different: EPS-inducing agents, anxiolytics, benzodiazepines, anticonvulsants.
NF includes individuals to whom a neighborhood income could not be assigned, that is, residents of personal care homes, psychiatric facilities, and prisons as well as wards of the public trustee and Child and Family Services.
Chi-square (and t-test, where appropriate) test was used to assess the differences. p-value <0.05 represents significance.
Years 1996/97 to 2000/01 were suppressed due to small cell size.
ADHD, attention-deficit/hyperactivity disorder; EPSs, extrapyramidal symptoms; NF, not found; NS, not significant; SD, standard deviation.
The number of EPS-related adverse events, mean length of follow-up, and contributed person-years for risperidone and quetiapine are reported in Table 2. The use of quetiapine was associated with a lower risk of EPS adverse events. The unadjusted and adjusted HRs (95% confidence interval [CI]) for quetiapine versus risperidone (reference) were 0.83 (0.56–1.25) and 0.53 (0.34–0.83), respectively (Table 2). The adjusted analysis reached statistical significance.
CI, confidence interval; HR, hazard ratio; SD, standard deviation.
Discussion
Our study reported the occurrence of EPS adverse events in children treated with either risperidone or quetiapine. As expected, the risk of EPS appears to be lower for children exposed to quetiapine than for children exposed to risperidone with an adjusted HR of 0.53; nevertheless, similar crude rates of EPS events of 10.55 and 8.76 per 100 person-years for risperidone and quetiapine reveal a general significant risk for movement disorders in children treated with SGAs.
At the time of their introduction to the market, SGAs were claimed to be devoid of EPS; however, subsequently EPS events with SGAs have been reported in both adults and children (Derinoz 2013). It is hypothesized that the incidence of EPS is related to the affinity of the antipsychotic for the dopamine D2 receptor. Risperidone has a higher affinity for D2 receptor than quetiapine, which has the least affinity for D2 receptor (Seeman 2006). A meta-analysis of randomized control trials (RCTs) on risperidone suggests that in comparison with placebo, risperidone has significantly higher odds ratio for EPS in children (Pringsheim et al. 2011). Our results provide a real-world comparison of risperidone and quetiapine in children at a population level and show the expected higher risk for risperidone exposure. It needs to be observed that EPS adverse events were observed in both SGAs and it is important to consider that no therapy is without risk. Similar crude rates for EPS events for risperidone and quetiapine support this level of clinical caution. Clinicians should monitor carefully children treated with antipsychotics to avoid the development of serious adverse events.
This population-based study was conducted using the comprehensive administrative health databases of Manitoba (MB). As data come from the entire population, results are free from sampling errors and can likely be generalized to the general youth population of Canada. The DPIN database captures >90% of all prescriptions filled in the community by MB residents (including registered First Nations) without limitations due to age and type of drug coverage; DPIN is one of the few databases in Canada that includes prescription information for children and adolescents.
Despite the strengths described, this study was not devoid of limitations. The effect of dose on the incidence of various adverse events was not measured and the lack of clinical data hampered the opportunity to assess the direct benefit of antipsychotic therapy and/or the quality of life in young users of antipsychotic medications. It is also worth noting that prescription information provided by administrative databases is dispensation records and there is no assurance that the medications prescribed are actually consumed by patients. Lastly, it is recognized that the possibility of unmeasured confounders is always an intrinsic limitation of observational studies. In particular, as risperidone is commonly prescribed for psychotic externalizing disorders (Bachmann et al. 2014) while quetiapine is more commonly prescribed for internalizing disorders (Temmingh and Stein 2015), the two cohorts might present an inherently different risk for movement disorders despite the adjustments made on comorbid conditions.
Furthermore, it is recognized that movement disorders are likely to be underdiagnosed and underreported (Acton 2013), as a result the rates of incident EPS might be underestimated; however, as this would likely occur with the same frequency in both treatment groups, the validity of the comparison would not be affected.
Conclusion
Although quetiapine appears to be associated with a lower risk of movement disorders in children and adolescents than risperidone, EPS diagnoses have also been detected in children treated with quetiapine.
Clinical Significance
Clinicians should always take into consideration the risk–benefit before treating children with antipsychotic medications and should be vigilant of the onset of drug-induced adverse events.
Footnotes
Acknowledgments
The authors acknowledge the Manitoba Centre for Health Policy, University of Manitoba, for use of data contained in the Population Health Research Data Repository under project 2012-150 and derived from data provided by Manitoba Health. The results and conclusions are those of the authors, and no official endorsement by Manitoba Health, Seniors and Active Living (HIPC File No. 2012/2013-16) and the Manitoba Centre for Health Policy, or other data providers, is intended or should be inferred.
Disclosure
S.A.-S. received unrestricted research grants from Pfizer and Merck for projects not related to this project. S.B. received an unrestricted grant from Merck for a project not related to this work. No other competing financial interests exist.