
Abstract
Objectives:
To examine the metabolic profile of adolescents at baseline and to determine the potential predictive power of a 1-month weight gain (WG) on weight changes during longer term second-generation antipsychotic (SGA) treatment.
Methods:
A retrospective chart review study, including patients between 13 and 18 years of age and treated with SGA, was conducted. Available data at baseline, 1, 3, and 12 months of treatment were recorded.
Results:
Four hundred fifty-six patients were included, with a median age of 15 years. Ten percent of the patients were obese (>95th percentile) and abdominal obesity (>90th percentile) was observed in 12% of patients. In a subgroup of 42 patients with both baseline, 1, and 3-month weight data available, WG >4.5% after 1 month was found to be the best predictor (sensitivity: 100; specificity: 66; area under the curve: 83) for a WG >15% after 3 months. After adjusting for potential confounders, a threshold of WG >4% was found as being the best predictor.
Conclusions:
A worrisome prevalence of metabolic disorders was observed in an adolescent psychiatric cohort. In such patients, a WG >4% during the first month of treatment should raise concerns about weight controlling strategies. Further research is needed to confirm the present results and to determine the impact of a 1-month WG on a 1-year weight change.
Introduction
S
Thus, with a two- to four-fold increased prevalence of metabolic complications in psychiatric patients compared with the general population, cardiovascular diseases are one of the major causes of death in psychiatric patients, contributing largely to the observed decreased life expectancy of 12–30 years (Huber-Giseke et al. 2014; Ringen et al. 2014). As in the general population, cardiovascular diseases have probably a multifactorial origin (obesity, sedentary lifestyle, unhealthy food, and/or smoking are common in psychiatric patients) (De Hert et al. 2012). However, the contribution of SGA in the development of metabolic disturbances, principally due to an important WG, is of major concern, with clozapine and olanzapine inducing strong WG, quetiapine and risperidone inducing a medium WG, and aripiprazole, amisulpride, and ziprasidone associated with a lower WG risk (Leucht et al. 2013; Huber-Giseke et al. 2014). WG in pediatric or adolescent patients is of major concern and has also been widely described in the literature because of its life course impact. As in adults, a Bayesian meta-analysis on short-term WG in pediatric patients showed a significant weight increase for clozapine, aripiprazole, quetiapine, olanzapine, and risperidone, in addition to a worsening of metabolic parameters in pediatric patients (Cohen et al. 2012).
Of note, an important interindividual variability of drug-induced WG is observed, explained, in part, by personal risk factors, such as female gender, low baseline body mass index (BMI), younger age, or non-Caucasian ethnicities (De Hert et al. 2012). This underlines the importance of monitoring metabolic parameters during SGA treatment, to rapidly identify patients with a clinically meaningful WG and to initiate as soon as possible effective weight controlling strategies, such as lifestyle change and/or antipsychotic switching if clinically feasible (Citrome and Vreeland 2008).
Post-hoc analysis from clinical trials conducted in adults have shown that a rapid WG during the first weeks of treatment predicts further important WG in patients treated for schizophrenia with olanzapine, ziprasidone, and aripiprazole (Lipkovich et al. 2008; Hoffmann et al. 2010) and in bipolar patients treated with olanzapine (Lipkovich et al. 2006). Moreover, we recently demonstrated that a fast (>5%) WG after 1 month of treatment is the best predictor for an important WG after 3 (>15%) and 12 (>20%) months of treatment (Vandenberghe et al. 2015). However, the study included mainly adult and elderly patients (93% were ≥18 years of age), and we could not determine whether the 5% threshold could also specifically be used for pediatric patients.
Puberty is a developmental period involving a physiological WG related to hormones influencing the distribution of body fat. Adolescents are, for this reason, more sensitive than adults to metabolic effects during SGA treatment (Ratzoni et al. 2002; Safer 2004; Vitiello et al. 2009) and an iatrogenic WG at that developmental stage can be very deleterious on adolescent health (De Hert et al. 2011). In addition, important WG during SGA treatment is associated with poor treatment adherence (Rettew et al. 2015) and may also have strong psychological consequences on adolescent development. Of note, the persistence of obesity at adulthood varies from 20% to 50% when it starts before sexual maturity and from 50% to 70% when arising before puberty (Sweeting 2008; Romualdo et al. 2014). Thus, obese children are at risk for further metabolic complications in adulthood such as dyslipidemia or type 2 diabetes. Predicting important WG during SGA in pediatric patients is therefore of major clinical relevance.
In the present study, we first aimed to have an overview of metabolic parameters in a Swiss adolescent cohort from an adolescent psychiatric hospital, which is the first study in this class of age in Switzerland. Second, we attempted to determine, in a subsample of patients with available longitudinal data, how a weight change after 1 month of SGA treatment could predict a weight change after a longer period of treatment which has, to our knowledge, never been investigated.
Methods
Study design
A retrospective chart review study, including computerized clinical record of hospitalized patients has been conducted between August 2005 and January 2015 in the adolescent psychiatric inpatient clinic of the University Hospital of Lausanne, Switzerland. Inclusion criteria were adolescents between 13 and 18 years of age receiving amisulpride, aripiprazole, clozapine, olanzapine, paliperidone, quetiapine, risperidone, and/or sertindole as treatment. Somatic and psychiatric comedications as well as somatic comorbidities could not be recorded. There were no exclusion criteria.
Demographic data (age, gender, psychiatric diagnosis, number and duration of hospitalizations, and patient height) were recorded at treatment introduction. ICD-10 classification was used to establish psychiatric diagnosis (see Supplementary Data S1 for more information; Supplementary Data are available online at
The study was approved by the Ethics Committee of Lausanne University Hospital. Due to the retrospective noninterventional study design, no informed consent form was requested.
Predictive value of an early WG: exploratory statistics
Due to the important number of missing data at 3 and 12 months, and to consider an eventual dropout bias, baseline demographic was compared between patients with complete (at least baseline, 1 month and 3 or 12 months) and incomplete follow-up data. To assess the predictive value of an early WG during the first month of treatment on 3 and 12 months WG, sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) were calculated using the “pROC” R package (Robin et al. 2011). Sensitivity is defined as the percentage of correctly predicted high-risk patients among all truly long-term high-risk patients. Specificity defines the percentage of patients predicted as low-risk patients among all truly low-risk patients. PPV indicates the percentage of patients with an important 3 months WG and who were classified as having a high first-month WG. NPV indicates the percentage of patients who did not have an important 3 months WG and were classified as having a low early WG (see Supplementary Data S2 for more information).
Predictive value of an early WG: confirmatory analysis
A linear mixed-effects model was fitted on the WG percentage observed at 3 and 12 months after separating patients into two groups based on the best early WG threshold predicting 3 months WG discovered in the exploratory analysis. The “nlme” package of R (Pinheiro et al. 2013) was used to fit a linear mixed-effects model adjusted for baseline BMI, age, gender, and treatment duration (see Supplementary Data S3 for more information).
Results
Baseline demographics
Data were available for 456 patients (56% male, 44% female, Table 1), with a median (interquartile range [IQR]) age of 15 (2) years and with no significant age differences between both genders. Schizophrenia (F20–F29) and mood disorders (F40–48) were the most frequent diagnosis with a significantly higher schizophrenia prevalence among males (28% vs. 13%; p = 0.0001) and inversely a higher prevalence of mood disorders among females (38% vs. 24%; p = 0.003). A small but significant longer hospitalization duration was observed in female patients compared with males (23 vs. 20 days; p = 0.01). The most frequently prescribed SGA were quetiapine (48%), risperidone (35%), and olanzapine (14%), with no prescription of clozapine or sertindole. Except for quetiapine, which was more prescribed among females (53% vs. 41%; p = 0.01), no significant gender difference was found.
p-Values were calculated using Wilcoxon rank-sum tests for continuous variables and Fisher's exact tests for categorical variables between both groups. Significant p-values (p < 0.05) are presented in bold.
Presence of coprescriptions of amisulpride, aripiprazole, olanzapine, paliperidone, quetiapine, or risperidone.
95th BMI percentile and higher.
For children younger than 16 years: presence of abdominal obesity if waist circumference >90th percentile. For children older than 16 years: Presence of abdominal obesity if waist circumference ≥102 cm for males and ≥88 cm for females.
For children younger than 16 years: systolic blood pressure >130 mmHg or diastolic blood pressure >85 mmHg or treatment for hypertension. For children older than 16 years: systolic blood pressure >130 mmHg or diastolic blood pressure >80 mmHg.
For children younger than 16 years: presence of hypo HDL cholesterolemia <1.03 mmol/L. For children older than 16 years: <1.00 mmol/L for males and <1.3 mmol/L for females.
Hypertriglyceridemia: triglycerides ≥1.7 mmol/L.
Hyperglycemia: glucose ≥5.6 mmol/L.
Metabolic syndrome is present if: presence of central obesity and at least two other following factors: hypertension, hypo HDL cholesterolemia, hypertriglyceridemia, or hyperglycemia.
IQR, interquartile range; BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Prevalence of metabolic disorders
A baseline median (IQR) BMI of 20 (4) kg/m2 and a prevalence of obesity of 10% were observed, with a significant higher prevalence among males (14% vs. 7%, p = 0.04). Abdominal obesity was observed in 12% of the patients, without a significant difference between genders. Thirty-one percent of the patients had hypo HDL-cholesterolemia, 4% hypertriglyceridemia, and 9% hyperglycemia, with no gender differences. Of note, a 13-year-old male fulfilled the IDF definition of MetS.
Short-term WG as predictors of long-term WG
After 1 month of treatment, a median WG of 4% (IQR: 5%) was observed. A median weight increase of 8% (IQR: 10%) was measured after 3 months and of 11% (IQR: 19%) after 12 months of treatment. Because of missing data, only patients with available weight at baseline, 1 month, and 3 months (total n = 42) of treatment were included in the analysis for weight predictor (see Supplementary Data S4 for more information). One month WG predicting a WG after 12 months could not be determined due to an insufficient number of data (only 19 remaining patients at 12 months).
The best short term predictor, based on the highest area under the curve (AUC), was found to be a WG of >4.5% after 1 month predicting for WG >15% after 3 months of treatment. This threshold had a sensitivity of 100%, specificity of 71%, NPV of 100% and a PPV of 40% (Table 2). Other short term WG predictors close to the 4.5% threshold were also explored (>3%, >3.5%, >4.5% and >5%). With the exception of the >3% threshold, all other values have an AUC higher than 75, thus clinically relevant for predicting a WG at 3 months of treatment.
NPV, negative predictive value; PPV, positive predictive value; AUC, area under the curve.
Confirmatory analysis of a short-term WG
Generalized linear mixed models integrating age, baseline BMI, gender, and treatment duration as potential confounders were analyzed in four separate models (Table 3). These analyses confirmed the early WG threshold of >4.5% as a significant predictor for a weight change during the first year of treatment ([β]: 3.7%, p adjusted = 0.05). However, using this model adjusted by the same confounders, a value >4% was also found to be the best early WG predictor (β: 4.1%; p adjusted = 0.03) and was thus retained for further analysis. Of note, an increase of weight was also observed in the group of patients with a WG ≤4% after 1 month, 75% of such patients gaining more than 4% after 3 months of treatment (Fig. 1).
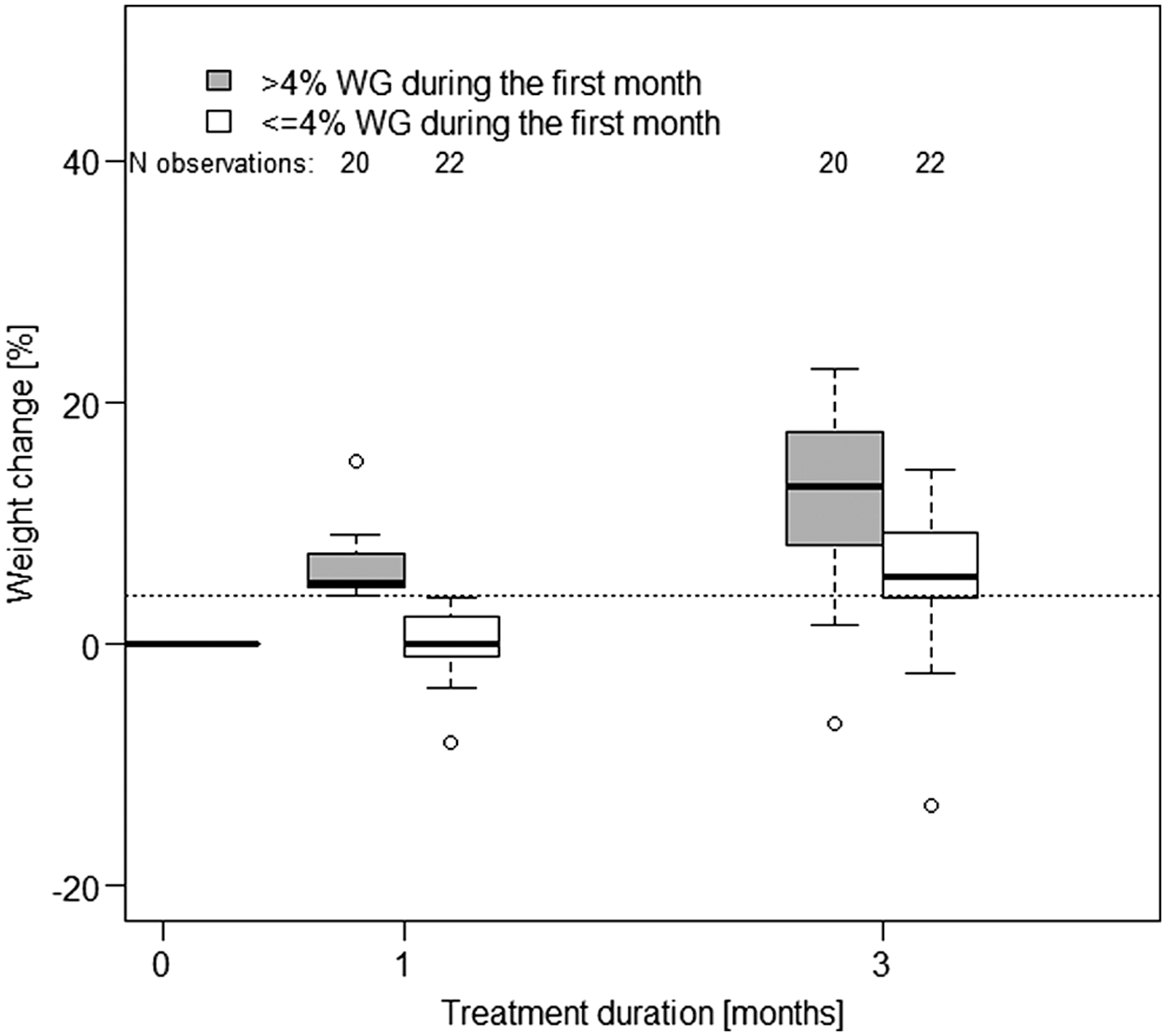
Weight changes at 1 and 3 months. Gray and white box plots (median and interquartile range) represent patients with a first-month weight gain of more than 4% and less or equal to 4%, respectively. Dotted black line represents a 4% weight increase.
Results were obtained by fitting a linear mixed model controlling for age, sex, treatment duration, baseline BMI. One thousand bootstraps were used for the analysis.
BMI, body mass index.
Demographic and metabolic parameters between early and nonearly weight gainers
No significant demographic differences were observed between the groups of patients with a 1-month WG >4% versus ≤4% (Table 4). Metabolic traits such as waist circumference, BMI, or blood pressure, were also found to be identical between the two groups at baseline. However, patients with a WG >4% at 1 month had a significantly lower median (IQR) baseline level of fasting glucose (4.7 [0.5] vs. 5.2 [0.7] mmol/L; p = 0.01).
p-Value were calculated using Wilcoxon rank-sum tests for continuous variables and Fisher's exact tests for categorical variables between both groups. Significant p-values (p < 0.05) are presented in bold.
Presence of coprescriptions of amisulpride, aripiprazole, olanzapine, paliperidone, quetiapine, or risperidone.
95th BMI percentile and higher.
For children younger than 16 years: presence of abdominal obesity if waist circumference >90th percentile. For children older than 16 years: Presence of abdominal obesity if waist circumference ≥102 cm for males and ≥88 cm for females.
For children younger than 16 years: systolic blood pressure >130 mmHg or diastolic blood pressure >85 mmHg or treatment for hypertension. For children older than 16 years: systolic blood pressure >130 mmHg or diastolic blood pressure >80 mmHg.
For children younger than 16 years: presence of hypo HDL cholesterolemia <1.03 mmol/L. For children older than 16 years: <1.00 mmol/L for males and <1.3 mmol/L for females.
Hypertriglyceridemia: triglycerides ≥1.7 mmol/L.
Hyperglycemia: glucose ≥5.6 mmol/L.
IQR, interquartile range; BMI, body mass index; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Discussion
In the present cohort of adolescent psychiatric patients, a worrisome obesity prevalence of 10% was observed at baseline, which is higher than the 3.5% obesity prevalence reported in general pediatric and young populations (age range 15–24) in Switzerland (Swiss Health Survey 2012, Federal Statistical Office 2013). This high prevalence of obesity underlines the higher cumulative risk profile of this adolescent psychiatric population, showing as in adults, the intertwining between mental illness and somatic disorders. Despite this, data on obesity prevalence in psychiatric adolescents similar to the present cohort (e.g., same age range, similar diagnosis) is scarce; prevalence ranging from 6.9% to 16% has been reported by studies with similar mean ages to the present cohort (Fraguas et al. 2008; de Hoogd et al. 2012; Kemp et al. 2013; O'Donoghue et al. 2014).
Hyperglycemia was observed among 9% of patients at baseline, which is higher than the 5.3% prevalence rate observed in a nationwide German obese adolescent cohort (Hagman et al. 2014). Regarding psychiatric patients, a retrospective chart review reported a 7.5% prevalence of hyperglycemia in SGA-naive patients (mean age = 13.9) (Panagiotopoulos et al. 2009), a value closer to the present study, suggesting a higher prevalence rate of hyperglycemia among psychiatric as compared with nonpsychiatric adolescent subjects. Of note, it has been reported that diabetic children have an increased risk of neuropsychiatric disorders, the risk increasing in cases of associated obesity or dyslipidemia (Block et al. 2010). These results are of clinical concern knowing the importance of promoting a healthy state during adolescence to prevent noncommunicable diseases during adulthood. Pediatric psychiatric populations therefore deserve greater medical attention to avoid the development of type 2 diabetes and/or of other metabolic disorders.
Differences of psychiatric diagnoses were observed among genders. Schizophrenia was more prevalent in males (28%) than in females (13%), which could be explained by a later age of onset in females (Szymanski et al. 1995). On the other hand, mood disorders were more frequent among females (38% vs. 24%), confirming previous observations (Birmaher et al. 1996). Off-label use of SGAs in pedopsychiatry is very common and of major concern for patient safety (Winterfeld et al. 2008). In the present study, the most common prescribed antipsychotics were quetiapine and risperidone, both approved for pediatric use by the Swiss Agency for Therapeutic Products (Compendium Suisse des Medicaments 2015). However, 14% of the patients were treated with olanzapine, a drug without indication for pediatric use in Switzerland (2015), and known to induce, like clozapine, an important WG (Leucht et al. 2013). Of note, the prescription rate of olanzapine dropped from 53% (17/32 treatments introduced in 2008) to 8% (3/36 treatments introduced in 2009). This could be explained by the introduction (in 2008) within the University hospital of a department guideline for metabolic follow-up during psychotropic drugs known to induce WG (SGA, valproate, lithium, and mirtazapine) (Choong et al. 2008), resulting in an increased awareness of metabolic disorders induced by psychotropic treatments.
In the longitudinal cohort, a clinically important WG of 8% was observed after 3 months of SGA treatment, which is close to the 11.8% WG reported in a previous study with drug-naive adolescents (mean age = 13) treated with SGAs for the same treatment duration (Roy et al. 2010). These values can also be compared with the nonsignificant weight change (0.65%) in untreated adolescent psychiatric patients (mean age = 15.5) during a clinical follow-up of 3 months (Correll et al. 2009). Of note, a WG of 8.1% after 3 months of aripiprazole was also reported in a pedopsychiatric cohort (mean age = 13.9) (Correll et al. 2009), emphasizing that drugs with low WG-inducing potential in adults can induce strong WG in pedopsychiatric patients. Due to the small cohort size with longitudinal data in the present study, no weight evolution among each SGA could be calculated. Moreover, these results need to be confirmed in a cohort taking into account BMI changes over time.
An early WG of more than 4% after 1 month of treatment with SGA was found to be a good predictor in adolescent psychiatric patients for an important WG (>15%) after 3 months. Patients with >4%WG during the first month had 4.1% more WG over 1 year compared with patients with ≤4% (p adjusted = 0.03). This observation is in line with the previously described 5% WG threshold found to predict an important WG at 3 and 12 months of treatment in a cohort of adult and old age patients (Vandenberghe et al. 2015). Of note, a 7% WG after 6 weeks of treatment was defined as clinically significant by the European Association for Study of Diabetes and the European Society of Cardiology (De Hert et al. 2009). However, this threshold was first chosen for its clinical significance and not for its predictive value. The present result suggests that a rapid weight change of more than 4% after 4 weeks of treatment in pedopsychiatric patients should be a warning for clinicians to further evaluate metabolic consequences of SGA prescription in adolescent patients. Interestingly, baseline BMI and age were found to be similar between patients with more than 4% WG and those with less or equal to 4%, a result which differs from those found in adults patients (Vandenberghe et al. 2015). This difference can probably be explained by the narrow range of age in the present adolescent cohort, as well as a narrower range of baseline weight probably reflecting a lower number of previous treatments as compared with adult psychiatric patients. On the other hand, in agreement with our previous study (Vandenberghe et al. 2015), the type of SGA was not found to influence an early WG.
Several limitations of the study have to be discussed. First, the conclusions are limited by the important amount of missing data during drug treatment after the baseline evaluation, which can be explained by the generally short hospitalization of patients in the ward where this study took place, a strict time inclusion criteria of ±2 days at 1 and 3 months as well as ±7 days at 12 months, and also by the late introduction in this ward of clinical recommendations to monitor metabolic parameters during treatment with psychotropic medication. However, and interestingly, they are in agreement with the results found in our previous study with a much larger adult psychiatric cohort. The important number of missing data at 1 year could explain that no predictor could be found for the 1 year weight change. Future studies should therefore specifically aim to find predictors for long-term WG in pediatric patients starting a SGA treatment. Second, weight changes can be due to physiological adolescent growth. To take into account this effect, calculations should be based on %BMI changes with a height measured at each time point. In the present study, only baseline height was available, thus baseline BMI was integrated as confounder into the validation model and relative WG expressed in % was used as the dependent variable. The absence of recorded height after 3 months of treatment should not influence the present results as this period is too short to produce a significant increase in height. However, we cannot exclude that some patients had an important growth spurt during this period. Third, no information was available concerning previous treatments, and it was thus not possible to identify antipsychotic-naive patient. Fourth, information on SGA dosing was not available. Finally, physical activity, food intake, comorbidities, and somatic medication, which could interfere with metabolic parameters, were not known for the present cohort, and such factors could therefore not be taken into account. Thus, it was not possible to determine if other somatic drugs known to induce WG (e.g., insulin, prednisone) were confounding our results.
Conclusions
The present study confirms the presence of several metabolic abnormalities in this cohort of adolescent psychiatric patients, underlining the importance of a systematic weight and other metabolic parameter monitoring during SGA treatment, but also during treatment with other psychotropic drugs with WG-inducing potential (i.e., some first-generation antipsychotics, mood stabilizers, and antidepressants). To identify patients at risk for important WG, complete metabolic parameters should carefully be monitored at baseline and during the first months of treatment according to previously published guidelines (Pringsheim et al. 2011). Adolescent patients with a weight increase of more than 4% during the first month of treatment appear to be at higher risk for an important (>15%) WG at 3 months. Considering the major impact of obesity and/or of metabolic symptoms on future general health and quality of life, in particular in this young age group, a particular emphasis should be put on patients at risk, using all available options (e.g., behavioral interventions, diet, and physical activity advice), but also possible change in psychotropic medication after a careful reevaluation of the risk/benefit ratio of psychotropic and/or somatic drug prescription.
Clinical Significance
Several metabolic abnormalities were observed in this adolescent psychiatric cohort. A weight gain of more than 4% during the first month of treatment should be used by the clinician as one of the early warning signs to consider those patients as being at higher risk of important weight gain during long-term treatment.
Footnotes
Author Contributions
Study concept and design: C.B.E., A.-E.A.; Acquisition of data: A.N.-G.; Analysis and interpretation: F.V.; Drafting of the article: F.V., A.N.-G.; Critical revision of the article for important intellectual content: all authors; Statistical analysis: F.V.; Obtained funding: A.-E.A., C.B.E., P.C.; Administrative, technical, or material support: all authors.
Disclosures
C.B.E. received honoraria for conferences or teaching CME courses from Astra Zeneca, Forum für Medizinische Fortbildung, Janssen-Cilag, Lundbeck, Merck Sharp and Dohme, Mepha, Otsuka, Servier, and Vifor-Pharma in the past 3 years, and for writing a review article for the journal “Dialogues in clinical neurosciences” (Servier). He received an unrestricted educational research grant from Takeda in the past 3 years. Other authors have no financial disclosures.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.