
Abstract
Objectives:
To assess the impact of antipsychotic tapering and discontinuation on measures of metabolic functioning and psychiatric symptom severity in severely impaired youth hospitalized in a psychiatric state hospital.
Methods:
The study examined psychiatric and metabolic measures in 67 hospitalized children and adolescents (mean age 10.0; 56 with discontinued use of antipsychotics, 10 with continued use of antipsychotics, and 1 started on an antipsychotic) from admission to discharge.
Results:
Upon admission, 56 youth were tapered off of antipsychotic medications, started on other forms of pharmacotherapy (92.9% were started on medications used to treat attention-deficit/hyperactivity disorder), and received evidence-based behavioral programming and were ultimately discharged from the hospital. The mean duration of treatment was 228 days for the discontinuation group and 204 days for the continuation group. Significant decreases in body mass index [BMI; t(53) = 7.12, p = 0.0001] and BMI percentile [t(53) = 6.73, p = 0.0001] were found from admission to discharge in the antipsychotic discontinuation group. Changes in BMI, BMI percentile, or systolic blood pressure were not found in the group (n = 10) who were maintained on antipsychotics. Both groups experienced a significant increase in their Global Assessment of Functioning score [t(52) = 19.98, p = 0.0001 for discontinued; t(8) = 5.092, p = 0.001 for maintained]. Psychiatric symptom severity scores significantly improved in many subscales relevant to disruptive behaviors and mood disorders for those who were removed from the medications. For those maintained on the antipsychotics, there were fewer changes in psychiatric symptom scores.
Conclusion:
Discontinuation of atypical antipsychotic medications in conjunction with tailoring treatment to presenting diagnoses resulted in metabolic and psychiatric symptom improvement among severely impaired state hospital inpatient youth. These results serve as a feasibility demonstration that discontinuation of antipsychotics does not provoke psychiatric destabilization, particularly among disruptive behavior disordered youth.
Introduction
T
When AAPs are used for off-label purposes in youth, they are most commonly used to address aggressive or disruptive behaviors, in the context of attention-deficit/hyperactivity disorder (ADHD), oppositional defiant disorder (ODD), or conduct disorder (CD) diagnoses (Matone et al. 2012; Penfold et al. 2013; Olfson et al. 2015). In fact, those with ADHD appear to be the largest consumers of AAPs (Matone et al. 2012), and the likelihood of a youth being prescribed an AAP increases as behavior problems increase (Rawal et al. 2004). Medications such as AAPs are often one of the first-line treatment options for an individual demonstrating violence or aggression (Baeza et al. 2013), particularly when evidence based behavioral interventions, which can be costly to implement (Kieling et al. 2011), are scarce (McHugh and Barlow 2010).
Despite high rates of AAP prescriptions, there is limited high quality evidence (e.g., sufficiently powered randomized controlled trials, augmentation studies, and so on) examining efficacy in disruptive behavior disorders (Pringsheim et al. 2015). One notable exception is the Treatment of Severe Childhood Aggression (TOSCA) study which added risperidone to a regimen of stimulant+parent training in children with residual severe aggression in the context of ADHD-CT and ODD/CD (n = 168; Aman et al. 2014). The addition of risperidone improved social competence (through improvements in reactive aggression), although no difference was present between groups in overall clinical global impression. As anticipated, participants taking risperidone had increases in prolactin levels and gastrointestinal symptoms. Of note, at 52 weeks follow-up, there was no difference in behavioral outcomes between groups, although treatment adherence was relatively low in both groups (36%–43%) (Gadow et al. 2016).
Clinical practice guidelines for the treatment of ADHD, as well as the use of antipsychotics, are currently in development by the American Academy of Child and Adolescent Psychiatry (AACAP). AACAP notes that existing practice parameters are out of date at present, as they were developed more than 5 years ago. Compounding the problem of an overall lack of research, youth routinely recruited into clinical trials and other clinical research studies are typically much higher functioning than many youth treated in real-world settings (Southam-Gerow et al. 2003). Thus, there is a paucity of research on children with complex needs who would otherwise be excluded from clinical trials, yet these youth are being treated in large numbers in the community (Blader 2011).
Of additional concern, AAPs are associated with high rates of adverse effects, including extrapyramidal symptoms and metabolic (e.g., weight gain, dyslipidemia) and cognitive symptoms (Longden and Read 2016). Children and adolescents have been shown to be more susceptible to the adverse effects of AAPs than adults (Correll and Carlson 2006; Vitiello et al. 2009). Hospitalized children with exposure to antipsychotics have thrice the prevalence of overweight compared to national norms (Patel et al. 2007). The risk of diagnosis with type 2 diabetes mellitus is twice as high when a child is prescribed an AAP (Sohn et al. 2015). Metabolic changes can begin to manifest quite rapidly during the first few months of treatment (Moreno et al. 2010; Ebert et al. 2014), even if the AAP is only used for a short time (Liao and Phan 2014).
In addition to efficacy and safety concerns outlined in this study, augmentation with an AAP has been shown to be associated with more healthcare utilization, as well as higher healthcare costs (Lachaine et al. 2014). One study found that patients with an ADHD diagnosis and a prescription claim for an AAP (vs. those taking other treatments) had higher rates of medication augmentation, inpatient admissions, emergency department visits, and outpatient visits, in addition to obtaining higher medical costs (Sikirica et al. 2014).
Inpatient psychiatrists are the most likely to prescribe AAPs, likely due to increased severity of symptoms and illnesses in the patients they treat (Rodday et al. 2014; Mann et al. 2016). Psychotropic medications, mainly stimulants and AAPs used in inpatient settings, are most often used for off-label usages or at off-label dosages (Akram 2015). “Violence” or “aggression” at admission was correlated with AAP prescriptions during the hospitalization, in one study (Weber et al. 2016). For those patients taking AAPs for aggression, discontinuation of the medications has been reported to be associated with fears of provoking aggressive acting out or even violence (Weber et al. 2016). Despite frequent use, there are still only limited studies evaluating medication use for aggression in pediatric inpatient settings (Deshmukh et al. 2010; Teixeira et al. 2013). Thus, inpatient admissions are a likely time when children and adolescents may first or repeatedly encounter AAP prescriptions.
Beyond concerns of monotherapy with an AAP, polypharmacy using an AAP plus other psychotropic medications has also increased (Kearns and Hawley 2014; Kreider et al. 2014). However, this complex treatment option appears to be occurring even in individuals who are less psychiatrically impaired (Kreider et al. 2014). This practice raises multiple concerns, among them drug–drug interactions may arise when using more than one psychotropic medication (Mojtabai and Olfson 2010). Off-label use and polypharmacy suggest that (1) prescribers are unfamiliar with the prescribing evidence base, (2) prescribers are encountering pediatric patients who appear to fall outside this base, and (3) limited data does suggest that AAP may improve disruptive behavior symptoms, at least in the short term. Thus, in this study we aim to examine AAP prescribing and subsequent deprescribing in a real-world sample of youth needing the highest level of psychiatric care available.
We hypothesized that (1) youth who experienced AAP discontinuation would show improved metabolic vital signs and electrocardiogram (EKG) metrics (Lindsay et al. 2004; Correll et al. 2009; Moreno et al. 2010; Calarge et al. 2014), (2) some youth would experience a worsening of psychiatric/behavioral symptoms with AAP discontinuation as these medications have been shown to have some efficacy in reducing psychiatric symptoms in disruptive behavior disorders (Troost et al. 2005; Jensen et al. 2007; Loy et al. 2012; Aman et al. 2014), and (3) youth treated according to best practice standards, including AAP discontinuation in combination with optimization of a different pharmacologic regimen, would benefit on metabolic, as well as psychiatric indices (Mortimer 2011).
To test these hypotheses in a severely affected sample, we reviewed treatment records from admission to discharge on youth hospitalized in an Indiana State Operated Facility (i.e., “state psychiatric hospital”).
Methods
A retrospective chart review was conducted of all 74 consecutive youth patients who were on psychotropic medications and admitted to the Evansville Psychiatric Children's Center (EPCC) between January 1, 2010 and December 31, 2012. EPCC is a small state-operated hospital in Evansville, Indiana for children aged 5 to 16 with Severe Emotional Disturbances which have not been successfully addressed in a less intensive environment.
A “gatekeeper” (the patient's local Community Mental Health Center) refers children who need this level of care, usually due to unmanageable aggression, from all over the state of Indiana. To qualify for admission, these children have failed to achieve sustained or adequate improvement after multiple forms of outpatient treatment, several acute psychiatric hospitalizations, and other (months long) residential treatments. A referring physician must certify that the child requires this level of care. Exclusionary criteria for the program include intellectual disability or known autistic spectrum disorder.
The treatment program uses the Boys and Girls Town Psychoeducational Treatment Model (PEM) as its primary behavior modification tool, but also utilizes individual, group, occupational/sensory, and recreational therapy modalities regularly. PEM trains staff and youth to recognize antecedents and triggers for aggressive behavior, promotes de-escalation techniques, implements a motivational system, and encourages staff-to-youth relationship building skills (Larzelere et al. 2001). PEM has been shown to decrease seclusion and restraint in residential settings (O'Brien 2004) and has promoted placement in less restrictive environments (Daly et al. 1998).
All staff at EPCC are also trained in Trauma Informed Care. The patient's diet plan consists of three meals and three snacks per day following National School Lunch Program guidelines. We speculate that the children typically experience relatively less screen time and more physical activity opportunities than they did in their home communities or prior placements.
Psychiatric assessment was completed by the staff child psychiatrist upon admission, although a structured diagnostic tool was not used. Intelligent quotient (IQ) testing was completed on 59.5% of the sample, by a licensed psychologist at EPCC. IQ testing was not completed when it was felt that testing done before admission was adequate. Psychiatric symptoms were additionally assessed at admission and discharge by master's level mental health clinicians at EPCC using the Child and Adolescent Needs and Strengths (CANS) tool (Anderson et al. 2003; Dilley et al. 2007) in all cases.
The CANS is a comprehensive assessment tool completed by trained clinicians that rates the severity of a range of mental health symptoms and life experiences. The CANS was developed to support care planning as each item may translate into different service plans or actions; it has also been used to monitor outcomes of services over time or over the course of treatment (Lyons 2009).
CANS scales used in this study are: Level of Need (LON); possible scores of 0–5, where a higher score signifies the need for a more intensive placement; Child Behavioral/Emotional Needs Domain, possible scores from 0 to 30 (each item rated 0–3), where a higher score signifies greater mental health problems, consisting of psychosis, impulsivity/hyperactivity, depression, anxiety, oppositional, conduct, adjustment to trauma, anger control, substance use, and eating disturbance items; and Child Risk Behaviors Domain, possible scores from 0 to 30 (each item rated 0–3), where a higher score signifies a history of more risky behaviors, consisting of suicide risk, self-mutilation, other self-harm, danger to others, sexual aggression, delinquency, fire setting, intentional misbehavior, and bullying.
Available metabolic and clinical metrics were noted for each of the youth at the time of admission and the time of discharge at EPCC. Demographic and historical information provided at admission was gathered from all available documents and in person reports presented at an admissions conference. Reporters vary for each child, but typically include biological, adoptive, or foster parents, community mental health center representatives, and personnel from the Department of Child Services, if relevant.
Data from the medical chart of each patient were collected from paper records and transposed into a Microsoft Excel spreadsheet that had been deidentified by investigators who had not been involved in evaluation or treatment of the patients. Demographic variables included gender, race, ethnicity, IQ scores, and age. Medical variables included body mass index (BMI; normed for age and gender), BMI percentile, height, weight, laboratory values (glucose, blood urea nitrogen, creatinine, sodium, potassium, high density lipoproteins, low density lipoproteins, total cholesterol, triglycerides, aspartate aminotransferase, alanine aminotransferase, thyroid-stimulating hormone, and hemoglobin), EKG reports (QTc interval), and vital signs (systolic blood pressure, diastolic blood pressure, and heart rate) and ratings of abnormal involuntary movements.
A screening EKG was collected at admission for each child. Youth whose EKGs had abnormal findings received adjustment of the medications and then a repeat EKG. Psychiatric variables included numbers of and types of Diagnostic and Statistical Manual of Mental Disorders IV-TR (DSM-IV-TR) (APA 2000) diagnoses, prescribed medications, and CANS scores.
EPCC attempted to collect postdischarge follow-up information for each patient. A “gatekeeper” representative from the local community mental health center who handled the discharge placement completed a brief questionnaire about the clinical status of the child, 6 months after discharge from EPCC. The gatekeeper noted whether or not the child was still receiving mental health services, whether or not they were still living at home, and whether or not they were doing “reasonably well.” They also provided comments in a free text area.
For clarity in presenting tabular data and to correctly classify the entire sample, youth were divided into four groups as follows: (1) those who were discontinued (DISC) from AAPs after admission, (2) those who were admitted and maintained on AAPs (continued; CONT), (3) youth who were started on AAPs during the course of admission, and (4) youth who never took an AAP. Because of small sample sizes in several of the groups (i.e., three and four) no between-group comparisons were undertaken. Instead, admission and discharge variables were compared using two-tailed, paired sample t-tests within the two largest groups, specifically those who experienced AAP discontinuation (DISC) and those who were maintained on the antipsychotics (CONT). Statistical significance was set at p < 0.05, uncorrected, given the exploratory nature of the study. Missing data were coded as such. Individuals missing crucial information, such as diagnosis or medications, were excluded. The study protocol was approved by Indiana University Institutional Review Board and was exempted from informed consent.
Sample characteristics
Of the 74 youth records assessed, 67 took AAPs during the study's observational period. Fifty-six were discontinued from AAP at some time after admission (typically shortly after), 10 were maintained on AAP since admission, and 1 was started on an antipsychotic during the course of their admission. Two youth lacked sufficient data and were therefore excluded from the analyses. Demographic variables are presented in Table 1 and Supplementary Table S1 (Supplementary Data are available online at
IQ, intelligent quotient; SD, standard deviation.
The mean (±standard deviation [SD]) age of the sample was 10.0 years ±2.37 (range: 5–14 years); 52 (74.29%) were children (<12 years) and 18 (25.71%) were adolescents (≥12 years). Fifty-four (75%) of the subjects were male. The mean (±SD) length of stay was 218.66 days ±124.12 (range: 52–619 days). Sixty-eight percent of the sample was exposed to “regular or problematic” use of tobacco, alcohol, illicit drugs, or prescription drugs of abuse. Seventy-six percent was reported to have experienced traumatic conditions (e.g., substantiated neglect, physical abuse, sexual abuse, and domestic violence).
The sample was reasonably healthy, with 39 (53%) individuals having some form of mild, comorbid medical condition. Most conditions were noted to be mild and included vision problems (N = 11), allergic rhinitis (N = 6), and asthma (N = 6). However, some of the conditions present were more serious in nature, such as chronic hepatitis (N = 1), epilepsy or another seizure disorder (N = 5), or allergic angioedema (N = 1). In addition, there were five congenital conditions present, such as secundum atrial septal defect or congenital limb malformation.
Upon discharge from the state hospital, 66% of the sample (48/74) was discharged to a family setting with relatives (e.g., parents, other relatives), and 25% (19/74) was discharged to a family setting with nonrelatives (e.g., foster home, adoptive home, nonrelative guardian). Nine youths (12.5%) were discharged to an institutional setting (eight to a Psychiatric Residential Treatment Facility and one to a juvenile justice setting).
Results
Psychiatric diagnoses
Participants averaged of 3.00 ± 1.02 diagnoses per individual after the admission assessment (Supplementary Table S2 and Fig. 1). The most common diagnoses made were ODD (N = 64; 88.9%), ADHD combined type (ADHD-CT; N = 40; 55.6%), and Anxiety Disorder Not Otherwise Specified (NOS; N = 41; 56.9%). Of note, most of the anxiety disorder NOS diagnoses were given for cases where some criteria of PTSD were met, but DSM-IV criterion C symptoms (i.e., avoidance and numbing) were absent. At admission, there were three (4.17%) individuals with an Axis II diagnosis of Borderline Intellectual Functioning (BIF) and 47 (65.28%) with a deferred diagnosis (Supplementary Table S2).
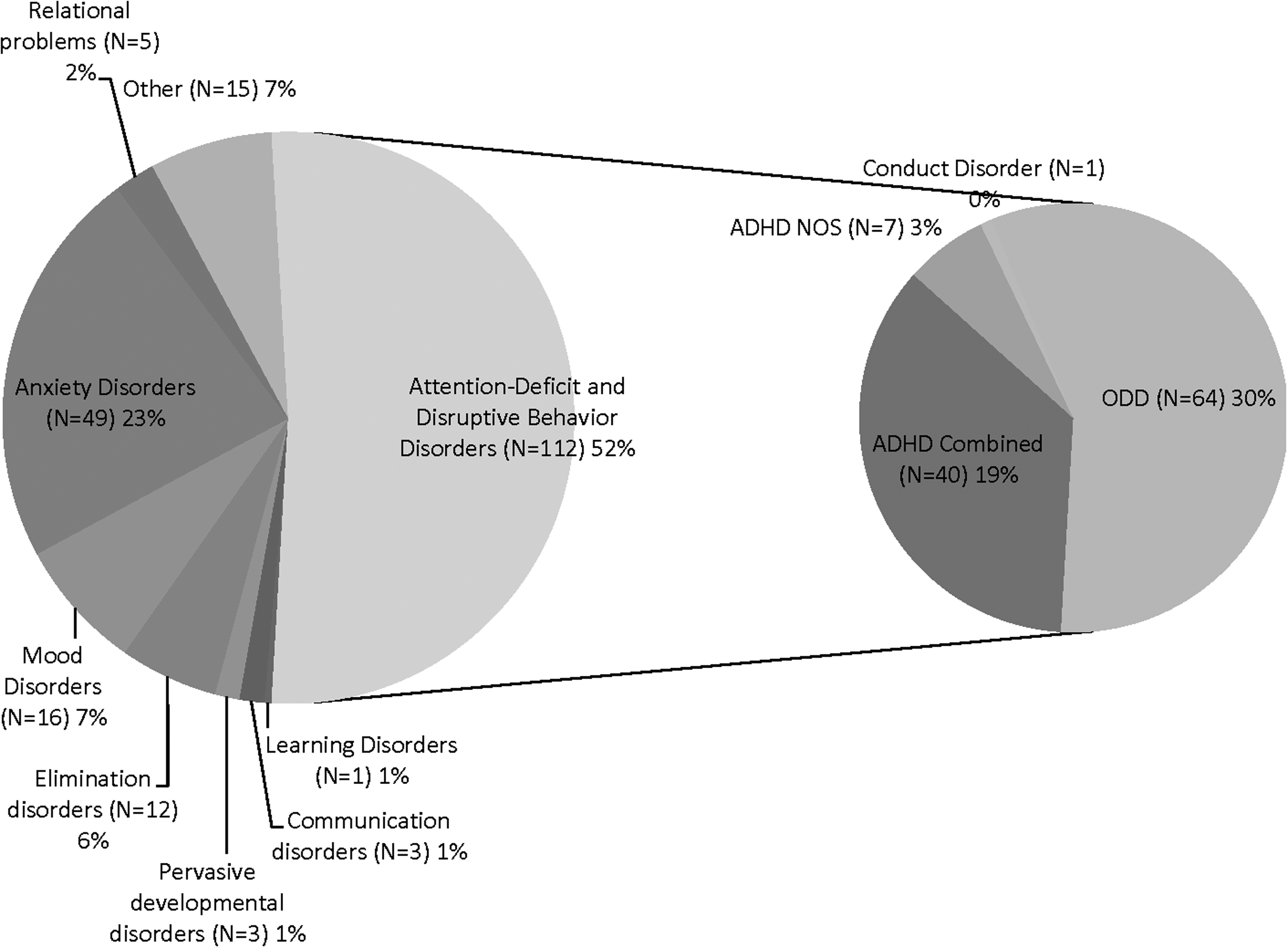
Total number of diagnoses by category given at admission. Individual diagnoses in the Attention-Deficit and Disruptive Behavior Disorders category are given in the chart to the right.
At discharge, there were 3.18 ± 1.09 diagnoses per individual (Supplementary Table S3 and Fig. 2). Again, the most common discharge diagnoses were ODD (N = 53; 73.6%), ADHD-CT (N = 47; 65.3%), and anxiety disorder NOS (N = 60; 83.3%). It was discovered during the hospital stay that additional children met criteria for an intellectual disability, such that six (8.33%) individuals had an Axis II diagnosis of BIF, seven (9.72%) had an Axis II Mild Mental Retardation (MR) diagnosis, and five (6.94%) had a deferred Axis II diagnosis (Supplementary Table 3). Of the 47 individuals with a deferred Axis II diagnosis at admission, 35 ultimately were not diagnosed with an Axis II diagnosis, 5 met criteria for Mild MR, and 2 were categorized as BIF; 5 remained deferred.
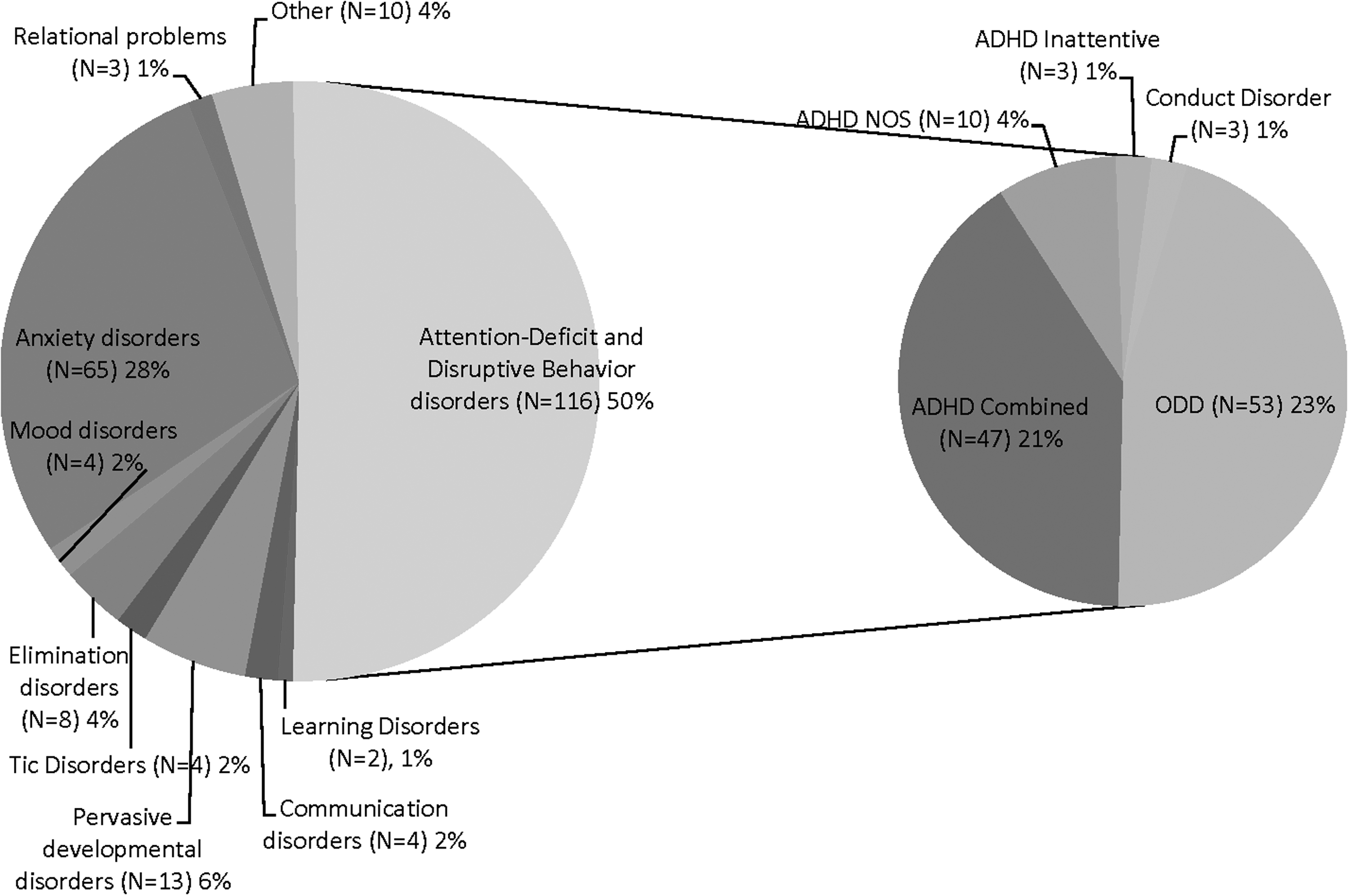
Total number of diagnoses by category at discharge. Individual diagnoses in the Attention-Deficit and Disruptive Behavior Disorders category are given in the chart to the right.
Average (±SD) change in diagnoses from admission to discharge was 0.764 ± 0.760. Thirty-three (45.8%) individuals had a change in number by 1 diagnosis, 10 individuals (13.9%) had a change in number of 2 or more diagnoses, and 29 individuals (40.3%) maintained the same number of diagnoses. Of the 29 that maintained the same number of diagnoses, only 15 (51.7%) were completely unchanged in the specific diagnoses given. Fifty-two diagnoses were removed in total, the most common being ODD with 13 instances. Sixty-five diagnoses were added, with the three most common being Anxiety Disorder NOS (with 14 instances), ADHD (with 18 instances total for all 3 types), and Asperger's/Pervasive Developmental Disorder (with 9 instances). Some diagnoses were made that were more specific than what the patients had when they entered the facility. There were 22 of this type with the most common changes occurring in the mood disorder, NOS, and the specific type of ADHD.
Psychotropic medications
At admission, there were a total of 232 unique psychotropic medications being prescribed, with an average of 3.22 ± 1.14 medications per individual. Of the 72 individuals described at admission, 66 (91.7%) were on antipsychotics, 31 (43.1%) on stimulants, 24 (33.3%) on antidepressants, 30 (41.7%) on mood stabilizers, and 53 (73.6%) on a nonstimulant therapy for ADHD (i.e., alpha-agonist, a serotonin and norepinephrine reuptake inhibitor (SNRI), or atomoxetine; Supplementary Table S4 and Fig. 3). Nineteen individuals (26.4%) were on two or more medications in the same class (see Supplementary Table S5 for breakdown). When the children were admitted, 88 of the 232 psychotropic medications (37.9%) were being prescribed in accordance with FDA indications (Table 2).
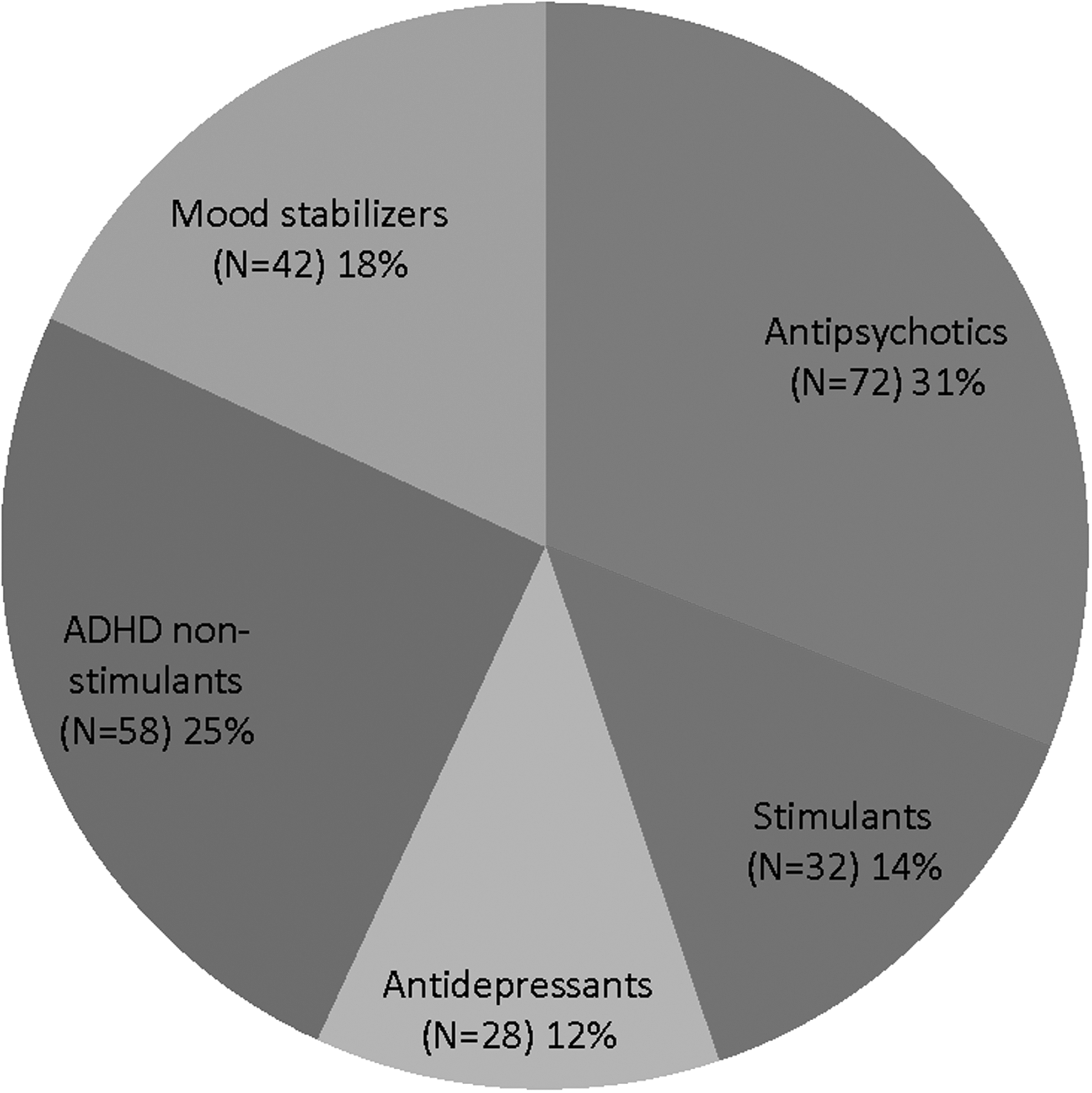
Total number and distribution of medications by class at admission (N = 232).
Cells represent numbers out of the total number of unique medications per category.
ADHD, attention-deficit/hyperactivity disorder; FDA, Food and Drug Administration.
At discharge, there were a total of 194 psychotropic medications being prescribed, with an average of 2.69 ± 1.03 medications per individual. Of the 72 individuals described at discharge, 11 were on antipsychotics, 44 were on stimulants, 48 on antidepressants, 10 on mood stabilizers, and 62 on adjunctive therapy for ADHD (Supplementary Table S4 and Fig. 4). Eighteen individuals took two or more medications in the same class. At discharge, 156 of the 194 psychotropic medications (80.4%) were being prescribed in accordance with an FDA indication (Table 2).
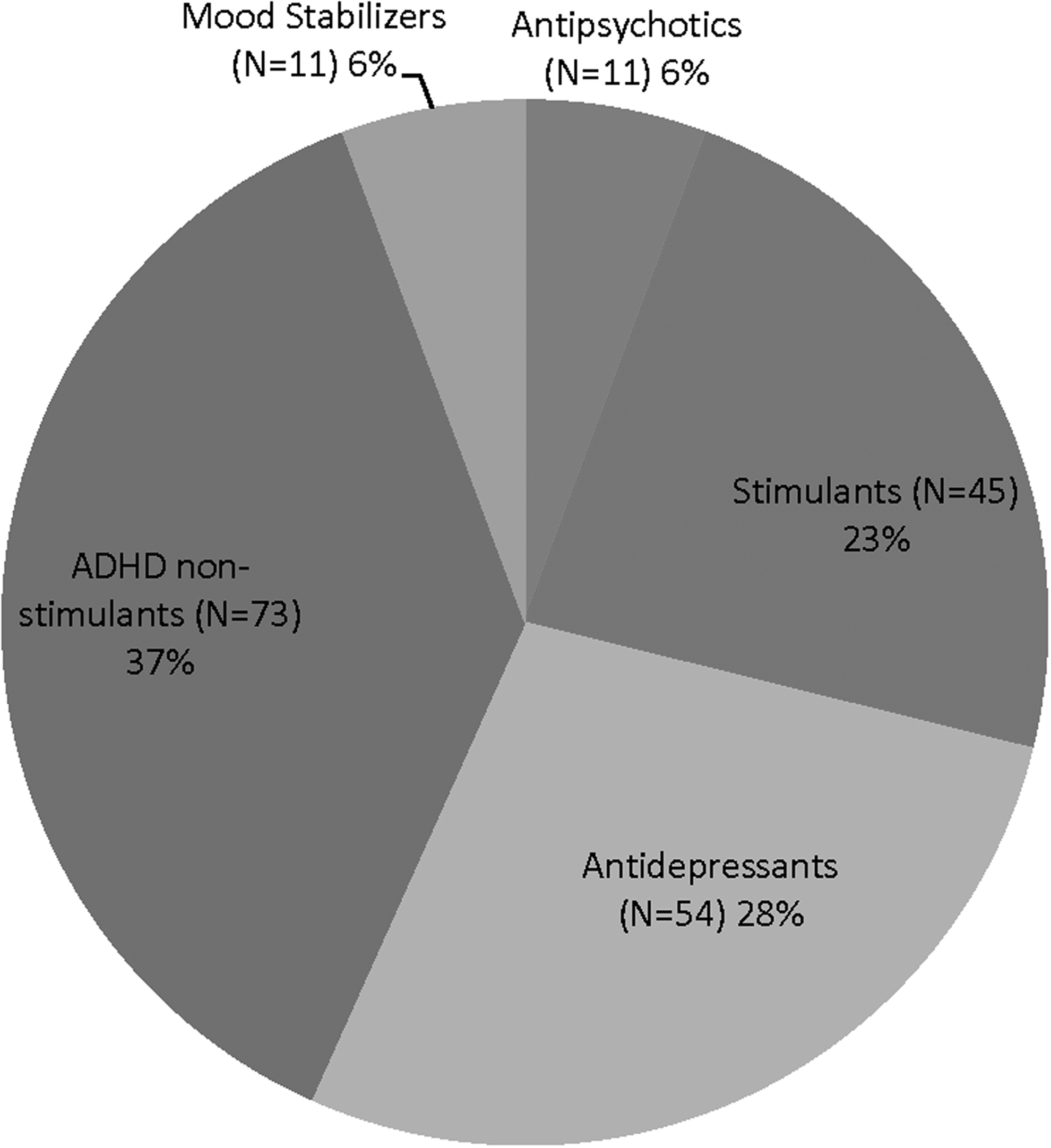
Total number and distribution of medications by class at discharge (N = 194).
Medical variables
At admission, 3 (4.17%) individuals were underweight, 23 (31.94%) were considered to be a healthy weight, 15 (20.83%) were at risk of being overweight, and 31 (43.06%) were overweight. By discharge, 5 (6.94%) were underweight, 41 (56.94%) were a healthy weight, 12 (16.67%) were at risk of being overweight, and 12 (16.67%) were overweight (Table 3).
Laboratory, EKG, and vital sign information is presented in Table 4. Of the 74 cases reviewed, 20 required repeat EKGs, due to some type of abnormality noted on the cardiologist's report for the baseline admission EKG (12 in DISC; 8 in CONT). QTc interval duration did not decrease significantly with repeat EKGs. Of note, each of those 20 youths took antipsychotics (5 risperidone, 5 olanzapine, 4 quetiapine, 3 ziprasidone, 1 haloperidol, 1 iloperidone) with 1 youth taking 2 antipsychotics (risperidone plus quetiapine) at admission. Multiple other medications were also taken with the antipsychotics. Changes from baseline to repeat EKG are reported in Table 4. There were not enough complete data to run paired sample t tests for the laboratory values or the values from the EKG for the CONT group, although it is worth noting that most EKG abnormalities theoretically would have been addressed by AAP discontinuation.
N represents number of individuals with admission and discharge measurements. Paired sample t tests were run only for pairs that contained at least 10 variables. Admission and discharge mean for N smaller than 10 are representative of all values present, including those without a pair. Baseline EKGs were obtained for all youths, but only the number indicated had repeated EKGs.
A1C, glycated hemoglobin; AIMS, Abnormal Involuntary Movement Scale; ALT, alanine transaminase; AST, aspartate transaminase; BMI, body mass index; BP, blood pressure; BUN, blood urea nitrogen; EKG, electrocardiogram; HDL, high density lipoproteins; K, potassium; LDL, low density lipoproteins; Na, sodium; SD, standard deviation; TSH, thyroid-stimulating hormone.
There were no significant differences in laboratory values in the DISC group from the time of admission to the time of discharge, except for the triglyceride levels [t(15) = 2.384, p = 0.032], which improved. Vital signs and BMI for DISC were all significantly improved across admission, (p ≤ 0.001) except for diastolic blood pressure [t(54) = 0.695, p = 0.490], which was unchanged. In contrast, for the CONT group, the only vital sign or BMI variable that changed across admission was height, which increased [t(10) = −3.860, p = 0.004]. Of note, diastolic blood pressure, heart rate, and weight were unchanged from admission to discharge for the CONT group, as opposed to the decrease found in the DISC group.
Psychiatric symptom severity
The CANS LON decreased in the DISC group [t(35) = 6.898, p = 0.0001], suggesting that a decreased level of care was needed at the time of discharge. In contrast, the CANS LON was unchanged in the CONT group [t(8) = 2.308, p = 0.054], suggesting that an ongoing high level of care was needed. Disruptive behavior ratings generally improved, with the DISC group showing significant improvements in 6 out of the 10 categories (all p ≤ 0.001), while the CONT group showed significant improvements in only 3 out of the 10 categories (all p ≤ 0.029). Psychosis scores decreased significantly for both groups [DISC: t(52) = 2.672, p = 0.010; CONT: t(9) = 2.449, p = 0.037].
For the two anxiety-related subscale scores, the DISC group showed significant decreases in both, while the CONT group did not show any changes. The DISC group showed significant decreases in all of the five subscales related to mood disorders (p ≤ 0.01), while the CONT group showed no significant changes in any of the five subscales. Neither group showed significant changes relating to substance use disorders likely due to the low baseline diagnostic rate (Table 5).
SD, standard deviation.
At admission, both the DISC and CONT groups had an average (SD) Global Assessment of Functioning (GAF) score in the 20 seconds (DISC = 23.92 ± 8.06; CONT = 20.89 ± 12.78), which indicates serious impairment in communication or judgment or an inability to function in almost all areas. By discharge, both groups had an average (SD) GAF score in the 40 seconds (DISC = 48.42 ± 6.87; CONT = 45.22 ± 5.17), indicating serious symptoms or impairment in social, occupational, or school functioning. Both groups experienced a significant increase in their GAF score during the hospitalization [DISC: t(52) = 19.98, p = 0.0001; CONT: t(8) = 5.092, p = 0.001].
When looking at individual CANS scores, compared to the entire population means, it is worth noting that some individuals in both groups still experienced either some psychiatric symptom worsening (DISC: 6.14% had worsening CANS; CONT: 9.60% had worsening CANS) or no improvement in an already elevated score (DISC: 20.4% had no change; CONT: 19.7% had no change; Supplementary Table S6).
Postdischarge follow-up
Six-month follow-up forms were completed by the child's mental health center for 44 out of 74 youths (59%). Of those with follow-up information provided, 70% were still in treatment with outpatient providers, 75% were still living “at home,” and 54% were “doing reasonably well.” Examples of comments included: “parent didn't follow through with treatment, pediatrician referred to psychiatry, unstable household, etc.” Four youths (9%) originally placed at home had been admitted to a residential placement (two of those noted to be placed due to lack of available foster care placement). In addition, two youths (4.5%) required a psychiatric admission, in the 6-month interval after discharge from the state hospital.
Discussion
The primary finding of this study is that a subset of youths, largely with disruptive behavior disorder diagnoses, hospitalized in the most restrictive, high needs environment (i.e., most psychiatrically ill) actually benefited from AAP discontinuation, when treated instead with a structured behavioral model, coupled with pharmacotherapy which more closely adhered to best practice standards (vs. pharmacotherapy present at admission). These benefits were found in behavioral, as well as medical, domains.
We had hypothesized that metabolic parameters would improve, but anticipated that behavioral worsening might occur fairly commonly. In fact, we found that only 6% of youths who experienced AAP discontinuation had a worsening of psychiatric symptom severity ratings. It is worth noting that to qualify for admission to the hospital reported on here, youth must have therapeutically failed multiple inpatient hospitalizations and, typically, multiple residential psychiatric placements. Thus, based on their treatment histories, the number of diagnoses, and the number of medications taken on admission, this appears to be a highly impaired sample. Youth with such severe impairments may be viewed, by prescribers, as too complex for the evidence base to apply and worthy of escalation to less tested agents, such as AAPs.
In this study, we demonstrate that even among such highly impaired youths, AAP discontinuation does not appear to precipitate an increase in symptoms in most youths, at least when assessed at the end of a long-term hospitalization. At least within the immediate postdischarge and 6-month follow-up periods, most youth were able to be discharged to home (vs. institutional) settings.
Psychiatric diagnoses and psychotropic medications
Many of the individuals in this study came into the psychiatric hospital with a large number of diagnoses and most were admitted for primary complaints of aggressive behavior. These children were individually taking a large number of medications at admission, likely with the intention of treating each individual diagnosis with a separate medication (Kearns and Hawley 2014), as well as controlling the aggression, despite the limited evidence that complex regimens improve care (Deshmukh et al. 2010; Baeza et al. 2013). With the extended length of stay, the staff child psychiatrist, utilizing results from psychological testing and incorporating input from all disciplines, attempted to clarify the children's diagnoses. This actually led to an increased number of diagnoses at the time of discharge overall.
Even in individuals without a change in the number of diagnoses, the diagnoses themselves were often changed. In particular, the number of diagnoses of anxiety disorders increased, while the numbers of psychotic disorders decreased. Consistent with other reports, this suggests that in disruptive youth, anxiety may be under-recognized (Bubier and Drabick 2009), while psychosis may be overreported (Biederman et al. 2004). Our work suggests, unsurprisingly, that an extended length of stay, with multiple family contacts, may enhance the ability of the provider to obtain a clear diagnostic picture.
Despite the overall increase in number of diagnoses from admission to discharge, the overall number of psychotropic medications actually decreased, on average. The majority of those youths admitted on AAP were weaned off and were placed on other psychotropic medications, such as stimulants, antidepressants, or adjunctive therapy for ADHD, given that most youths did not appear to have true psychosis.
Medical variables
At admission, a substantial proportion of the sample (63.9%) was either at risk for being overweight or were already overweight. We speculate that by weaning most individuals off of the AAPs (and other weight promoting medications) and starting individuals on a structured exercise regimen and, in some cases, medications that promote weight loss, only 33.3% were at risk of being overweight or were overweight at discharge. It is worth noting that the diet plan at EPCC was generous in the frequency of provided food and the amount of calories in the food offered. In addition, 56.9% were discharged with BMIs within healthy limits (vs. 31.9% at admission).
Surprisingly, laboratory values for the DISC group did not show significant improvement from admission to discharge, except for triglyceride levels. This is actually an important finding as disturbances in lipid metabolism can occur before the weight gain that occurs with AAP treatment (Cai et al. 2015). We conjecture that lipid related abnormalities may take more time to normalize.
The QTc interval was found to be elevated in a number of youths, all taking AAPs, at the time of admission. This is important as QTc interval prolongation has been associated with AAPs (Chohan et al. 2015; Barbui et al. 2016). QT prolongation can lead to ventricular tachycardia torsade de pointes (TdP), which may lead to sudden cardiac death (Nielsen et al. 2011). This group change in QT interval is noteworthy, as none of the individual children were noted by the referring physicians to have QT abnormalities at the time of admission.
Vital signs all significantly improved for the DISC group from admission to discharge, except diastolic blood pressure, which did not change. Many youths were changed to other psychotropic medications which can also impact weight, heart rate, and blood pressure, so the effects are not likely isolated to the AAP discontinuation alone. For the CONT group, height was the only significant change from admission to discharge, likely due to the extended length of stay for growing children. Unsurprisingly, BMI significantly decreased in the DISC group. However, for the CONT group, the average BMI percentile did not decrease and remained above the 85th percentile, indicating that these individuals were still overweight at discharge, despite the structured exercise regimen.
Psychiatric symptom severity
Oppositional behavior, anger control, and social behavior (or intentional misbehavior) ratings significantly improved in both groups of individuals across their hospitalizations. Both groups showed significant decreases in the symptom severity of some disruptive behaviors; however, delinquency, fire setting, and bullying showed no changes across either group. Psychosis scores decreased significantly for both DISC and CONT groups from admission to discharge, despite the DISC group being taken off medications that would, in theory, reduce psychosis symptoms.
There were a large number of anxiety disorders that were diagnosed during the inpatient stay. Because medications were tailored to treat overall diagnoses, including anxiety disorders, anxiety scores significantly decreased for the DISC group; however, there were no significant changes for the CONT group. For the mood-related behaviors, the DISC group saw significant decreases in all five categories, while the CONT group saw none and, in fact, saw slight increases in depression, eating disturbances, and suicide risk.
Limitations
Several limitations of this study are worth noting. This is a naturalistic study, including youth who would likely not qualify for routine clinical trials given their comorbidities and unstable life circumstances. Our design was not able to prospectively evaluate symptoms, with validated assessments, nor were we able to control for the heterogeneous medication regimens and diagnoses. The sample was relatively small, preventing valid between-group comparisons; and prescribing and diagnosing were subject to the biases of the psychiatrist, as a structured diagnostic instrument was not used. We also note that CANS scores, our primary outcome measure, can be biased by the clinical rater at the time of discharge, in particular, if a child is in need of a relatively high level of care (e.g., residential placement), to assist in acquiring that placement. These findings would be enhanced by data examining rates of return to AAPs once placed in less restrictive settings, but those data are not available for this sample.
Conclusion and Clinical Significance
This study longitudinally examined psychiatric and medical outcomes in a sample of youth with severe psychiatric symptoms at admission and at discharge from a long-term, state psychiatric hospital. Most youths were admitted for disruptive behavior and were taking AAPs at the time of admission. Most AAPs were discontinued as behavioral and other psychopharmacological treatments were optimized according to their diagnoses. Most youths were able to transition back to home-based, rather than inpatient, settings.
Unsurprisingly, a number of medical outcomes such as BMI and vital signs improved in youths who experienced AAP discontinuation. Psychiatric symptom severity ratings also improved in the discontinuation group. Unexpectedly, psychiatric symptom worsening was rare with AAP discontinuation. This study suggests that AAP discontinuation may be beneficial to highly impaired youths with disruptive behavior disorders who are treated in a structured environment. Systematic controlled studies are needed to further inform clinical practice of AAP discontinuation.
Disclosures
L.H. serves as a medical consultant to Indiana's Family and Social Services Agency which operates EPCC. However, L.H. was neither involved in the clinical care of any of the children in this study nor did she influence the clinical practice of S.J., as the study period occurred before the time of the consultancy. All other authors have no competing financial interests.
Footnotes
Acknowledgments
The authors acknowledge the AACAP's Campaign for America's Kids (CFAK) for the Summer Medical Student Fellowship in Child and Adolescent Psychiatry given to S.P. The authors thank Dustin Craney for his assistance with data collection.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.