
Abstract
Objectives:
Providing novel treatments for autism has been a subject of long-standing research. Based on etiopathological findings, we aim at assessing potential therapeutic effects of statins, here simvastatin, on autism symptoms for the first time.
Methods:
In this randomized, double-blind, placebo-controlled, parallel-group 10-week clinical trial, 70 drug-free children aged 4 to 12 years old with diagnosis of autistic disorder based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision, who had an Aberrant Behavior Checklist-Community (ABC-C) scale irritability subscale score of ≥12, were equally randomized to receive either simvastatin (20–40 mg/day) or placebo as an adjunct to risperidone (1–2 mg/day) whereas administration of both drugs was started simultaneously from baseline. Patients with comorbid psychiatric disorders, active medical conditions, severe intellectual disability, seizure disorders, history of any treatments for autism in the past 6 months, or history of current anti-inflammatory drug consumption were excluded. Primary outcome was defined as the difference in mean change of the ABC-C scale irritability subscale score from baseline to the endpoint (
Results:
Significant differences in change of the ABC-C scale irritability (mean difference [95% confidence interval (CI)] = −3.45 [−5.37 to −1.54], p = 0.001; Cohen's d = 0.89) and hyperactivity/noncompliance (mean difference [95% CI] = −4.27 [−6.69 to −1.86], p = 0.001; Cohen's d = 0.87) subscales scores were detected between the two arms. No significant difference was detected in case of the other three subscales.
Conclusions:
This study provides preliminary evidence for potential therapeutic effects of simvastatin in the treatment of autism that warrants further investigations.
Introduction
T
Effective treatment of autism has been a concern since the core symptoms have remained relatively resistant to different therapeutics (Ji and Findling 2015; DeFilippis and Wagner 2016), and autism prevalence has increased dramatically in recent decades (Christensen 2016). Meanwhile, several promising potential treatments have been proposed for autism-associated symptoms, especially irritability and hyperactivity, whether as single therapies or as an adjunct to the risperidone and aripiprazole, as the only medications approved by the food and drug administration (FDA) for the treatment of irritability symptoms in autism (Masi et al. 2015). In pursuit of novel therapeutics, the etiopathological findings from studies on neurobiology of autism have been the mainstay of ideas.
Autism is a disorder of an unclear origin integrating both genetic and environmental factors, which together converge on aberrancy in three main domains of excitatory/inhibitory balance of neurotransmission, lipid metabolism, and immune/inflammatory responses. Numerous studies have demonstrated an alteration of excitatory/inhibitory balance in autism; however, they have remained inconclusive regarding the direction of this imbalance and the suggestion of potential therapeutics (Dickinson et al. 2016). Meanwhile, potential therapeutics have been proposed based on the consistently documented importance of different lipid molecules, including prostaglandin E2 (Wong et al. 2015), cholesterol (Wang 2014), and polyunsaturated fatty acids (van Elst et al. 2014), in autism. In addition, a strong role for immune/inflammatory elements is also assumed in autism regarding the evidence of brain-specific patterns of increases in oxidative stress (Rossignol and Frye 2014), autoantibodies, pro-inflammatory cytokines, and microglial activation as well as increased rates of autoimmune disorders, increased levels of peripheral pro-inflammatory cytokines, decreased levels of peripheral anti-inflammatory cytokines, and defective systemic cell-medicated immunity (Estes and McAllister 2015; Young et al. 2016).
Considering neurobiological findings in autism, statins appear to be interesting candidates for further investigations. Widely used as cholesterol-lowering agents, statins have gained attention in brain research in recent years. They are suggested to influence the central nervous system (CNS) in both a cholesterol-dependent and -independent fashion. They inhibit the synthesis of cholesterol as well as downstream isoprenoids and influence the regulation of some key signaling proteins in CNS (van der Most et al. 2009; Ling and Tejada-Simon 2016). They also decrease lipid peroxidation, production of reactive oxygen species, leukocyte infiltration capability, antigen presentation to T-cells, and pro-inflammatory cytokine levels, while increasing anti-inflammatory cytokines and inhibiting microglial activation (van der Most et al. 2009).
In addition, statins showed promising results in a number of neuropsychiatric conditions that are hypothesized to share some underlying mechanisms with autism. These include lovastatin for aberrant behavior in children with Fragile X syndrome (Çaku et al. 2014); lovastatin but not simvastatin for cognitive deficits in children with neurofibromatosis type 1 (Krab et al. 2008; Acosta et al. 2011); fluvastatin for motor symptoms in animal models of Rett syndrome (Buchovecky et al. 2013); and simvastatin but not lovastatin or pravastatin for negative symptoms in patients with schizophrenia (Ghanizadeh et al. 2014; Vincenzi et al. 2014; Tajik-Esmaeeli et al. 2017).
Overall, simvastatin and lovastatin are the most studied statins in brain research due to their lipophilic structure, which enables them to cross the blood-brain barrier (Ling and Tejada-Simon 2016). Meanwhile, simvastatin demonstrated superiority in neuroprotection when comparing several statins in a single study based on a combination of different factors, including capacity to penetrate the blood-brain barrier, decrease cholesterol in CNS, induce direct neuroprotection, and cause less adverse events (Sierra et al. 2011).
This is the first study to report the potential effects of statins, here simvastatin, as an adjunctive therapy to risperidone on irritability symptoms in children with AD, as measured by the difference in the Aberrant Behavior Checklist-Community (ABC-C) scale irritability subscale score changes between the simvastatin and placebo arms from baseline to the endpoint.
Materials and Methods
Trial design and study settings
In this randomized, double-blind, placebo-controlled, parallel-group 10-week clinical trial, children with AD were selected from the specialty outpatient autism clinic at Roozbeh Psychiatry Hospital, Tehran University of Medical Sciences (TUMS), Tehran, Iran, between February 2016 and December 2016. The trial was carried out in accordance with the World Medical Association (Declaration of Helsinki, as revised in Seoul 2008) code of ethics after protocol approval by the Institutional Review Board (IRB) of TUMS (Code No. IR.TUMS.REC.1394.1602) and registration at the Iranian Clinical Trials Registry (IRCT Registration No. IRCT201602041556N86;
Participants
Participants were selected from male and female children aged 4 to 12 years old with the diagnosis of AD based on the DSM-IV-TR criteria (American Psychiatric Association 2000), and the ABC-C scale irritability subscale score of ≥12. It was required that the participants endorse at least six of the DSM-IV-TR criteria for AD diagnosis confirmed by a pediatric psychiatrist according to a semi-structured interview with the parents or guardians as well as behavioral observations of the patient. The diagnosis was then confirmed again by a second experienced pediatric psychiatrist by using Autism Diagnostic Interview-Revised (Lord et al. 1994). It was also required that the patient present with severe disruptive symptoms of autism as the chief complaint, which would indicate treatment intervention with risperidone.
Children with any of the following conditions were excluded from the study: concomitant DSM-IV axis I or II disorders as well as active medical conditions, severe intellectual disability making the diagnosis inconclusive based on prior records and clinical judgment, seizure disorders, history of alcohol/drug abuse, tardive dyskinesia, or history of antipsychotic medication or behavior therapy within the past 6 months before the trial. Also, it was required that the participants do not use potent inhibitors of the cytochrome P450 isoform 3A4 (CYP3A4), or systemic anti-microbial/anti-inflammatory drugs. Due to raised ethical concerns, it was not possible to change or discontinue prior medications of patients. Instead, participants were selected from those who were drug free due to other reasons, including discontinuation of treatment by parents.
Intervention
Participants were randomized to receive risperidone (Risperdal; Janssen Pharmaceuticals, Belgium) plus either simvastatin (Osveh, Iran) or placebo for 10 weeks, while starting both drugs simultaneously from baseline. Risperidone starting dose was 0.5 mg/day in 0.5 mg tablets, and in the absence of clinically significant adverse effects it was increased by 0.5 mg per week to the target dose of 1 mg/day for children weighing <20 kg and 2 mg/day for those weighing ≥20 kg. Simvastatin or placebo was administered in the form of a 20 mg tablet per day for children <10 years of age and a 40 mg tablet per day for those ≥10 years of age. Treatment adherence was monitored during the study by using a pill count and checking with parents. It was required that no other psychosocial therapies or medication be administered during the trial.
Outcome
The ABC-C scale was used for the measurement of treatment efficacy in this study (Aman et al. 1985b), which has been proved to be a valid and reliable tool for research purposes (Aman et al. 1985a; Kaat et al. 2014) and has been widely used in autism research, including clinical trials of autism in the Iranian population (Ghaleiha et al. 2015, 2016; Nikoo et al. 2015). As a rating scale designed for assessment of disruptive behaviors, the ABC-C scale is composed of 58 items and five behavioral abnormality subscales; three subscales for core deficits of autism, including “lethargy/social withdrawal,” “stereotypic behavior,” and “inappropriate speech”; and two subscales for associated disturbances, including “irritability” and “hyperactivity/noncompliance.”
An independent rater asked parents to complete the ABC-C scale according to standardized instructions at baseline, week 5, and week 10. The primary outcome of interest was the difference in mean change of the ABC-C irritability subscale score from baseline to the endpoint between the simvastatin and placebo arms. The secondary outcomes were defined as the differences in mean change of the ABC-C other subscale scores as well as time × treatment interaction for all subscale scores between the two treatment arms. Also, response to treatment rate was compared between the two arms for those subscales with a significant difference in score changes while considering partial response and complete response, respectively, as ≥25% and ≥50% reduction in the subscale score.
Safety and adverse events
Parents were informed about the potential adverse events and were asked to report incidence of any unexpected signs/symptoms in their child immediately. In addition, adverse events were checked at week 1 of the study through a phone call and at week 2 through a home visit, as well as other visits at the outpatient clinic during the trial using open-ended questioning followed by a comprehensive 25-item checklist (Akhondzadeh et al. 2008). Different raters were responsible for behavior appraisal and adverse events. Extrapyramidal Symptoms Rating Scale (ESRS) (Chouinard and Margolese 2005) was used for assessment of extrapyramidal symptoms at each visit, which has been used in previous trials in the Iranian population as well (Ghaleiha et al. 2015, 2016; Nikoo et al. 2015). Further, risperidone active fraction plasma levels were measured at weeks 5 and 10 to monitor simvastatin potential effect on increasing risperidone levels in participants' blood. Each participant was also subject to thorough clinical examination as well as laboratory testing for liver diseases. An expert child psychiatrist was responsible for making decisions immediately regarding dose adjustment or discontinuation of treatments in case of adverse events.
Sample size
Based on results from a similar recent study (Ghaleiha et al. 2016), a difference of 4 in mean score change of the ABC-C irritability subscale between the two treatment arms, a standard deviation (SD) of 4.5, a type I error of 0.05, and a power of 90% were considered for estimation of sample size. A final overall sample size of 70 was calculated while assuming a primary sample size of 54 (27 participants in each arm) and a potential attrition rate of 30%.
Randomization, allocation concealment, and blinding
Using a computerized random number generation, participants were randomized to simvastatin and placebo arms in a 1:1 ratio. Sequentially numbered, sealed, opaque envelopes were used for treatment allocation concealment from patients and physicians. Different entities were responsible for random allocation and rating. Simvastatin and placebo tablets were identical in shape, size, texture, color, and taste, and they were dispensed in identical containers by an investigational drug pharmacist. During the trial, the physicians, other healthcare personnel, participants, and parents were blinded to treatment assignments.
Statistical analyses
The IBM SPSS Statistics 19.0.0 (IBM Corporations) was used for all the analyses. Mean (SD) and number (%) formats were used in reporting continuous and categorical data, respectively. Mean (95% confidence interval [95% CI]) and Cohen's d (95% CI) formats were used in reporting the difference in mean change of the ABC-C subscale scores between the two treatment arms, and the effect size of this difference, respectively. The last observation carried forward method was used to deal with missing data for the intention-to-treat analysis. After application of the two-way repeated-measure analysis of variance (ANOVA) for the assessment of time × treatment interactions in each subscale, Greenhouse-Geisser's correction was considered in cases that sphericity assumption was violated according to Mauchly's W test result. After application of the independent-samples t-test for a comparison of continuous data, including mean change in the ABC-C subscales scores from baseline to each time point between the two treatment arms, corrected degrees of freedom (df) and p-values were considered in cases that equality of variances assumption was violated according to Levene's test result. Freeman-Halton extension of Fisher's exact test was used to compare partial/complete response to treatment between the two treatment arms. P-values of <0.01 in comparison of ABC-C subscale scores changed from baseline to endpoint, and p-values of <0.05 in all other analyses were considered significant. Two-tailed p-values were reported.
Results
Participants and baseline characteristics
Primarily, 90 patients were screened, out of whom 70 participants were randomized equally to simvastatin and placebo arms. A total of 66 participants (33 in each arm) were visited at week 5, continued to the endpoint, and were analyzed (Fig. 1).
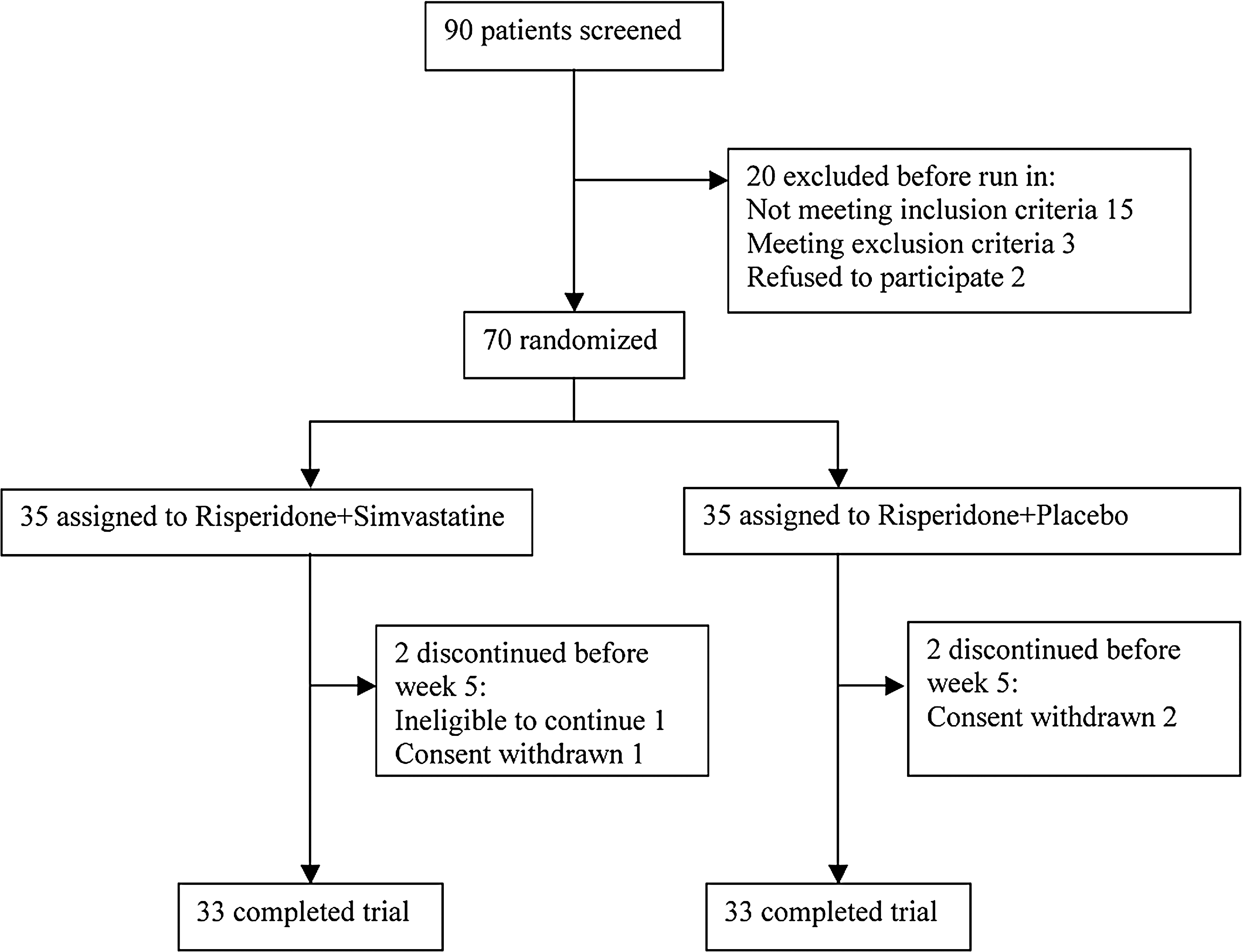
Flow diagram of patients with autistic disorder.
There was no significant baseline difference between the two treatment arms in terms of distribution of demographics, ESRS scores, or the ABC-C subscale scores. Throughout the study, risperidone was administered with mean (SD) doses of 1.51 (0.47) mg and 1.54 (0.39) mg in simvastatin and placebo arms, respectively, with no significant difference. Risperidone active fraction plasma levels in the respective simvastatin and placebo arms were 29.3 (13.2) ng/mL and 29.1 (12.4) ng/mL at week 5, and 30.1 (13.0) ng/mL and 29.7 (13.8) ng/mL at week 10 with no significant difference at any of the two time points (Table 1).
Independent-samples t-test or Fisher's exact test is applied where appropriate.
ABC-C, Aberrant Behavior Checklist-Community; ESRS, Extrapyramidal Symptoms Rating Scale; SD, standard deviation.
ABC-C irritability subscale score
As the primary outcome, there was a significantly higher reduction in the ABC-C irritability subscale score in the simvastatin arm compared with the placebo arm by the endpoint at week 10 (Table 2). There was also a significant time × treatment interaction between the two treatment arms [two-way ANOVA sphericity assumed: F (df, mean square) = 6.44 (2, 49.27), p = 0.002]. Participants in the simvastatin arm were subject to a significantly higher rate of complete response to treatment compared with the placebo arm by the endpoint (Table 3) (Supplementary Data; Supplementary Data are available online at
df and concordant p-values were calculated based on the results of Levene's test for assessment of equality of variances in independent-samples t-test.
CI, confidence interval; df, degrees of freedom; SD, standard deviation.
Freeman-Halton extension of Fisher's exact test is used for calculation of two-tailed p-values.
Complete, score reduction ≥50% of baseline score; Less than partial, score reduction <25% of baseline score; Partial, score reduction ≥25% of baseline score; SD, standard deviation.
ABC-C lethargy/social withdrawal subscale score
There was no significant difference in mean change of the ABC-C lethargy/social withdrawal subscale scores between the simvastatin and placebo arms by the endpoint (Table 2). Also, there was no significant time × treatment interaction between the two treatment arms [two-way ANOVA with Greenhouse-Geisser correction: F (df, mean square) = 0.52 (1.57, 3.48), p = 0.555] (Supplementary Data).
ABC-C stereotypic behavior subscale score
There was no significant difference in mean change of the ABC-C stereotypic behavior subscale scores between the simvastatin and placebo arms by the endpoint (Table 2). Also, there was no significant time × treatment interaction between the two treatment arms [two-way ANOVA with Greenhouse-Geisser correction: F (df, mean square) = 2.28 (1.33, 8.33), p = 0.127] (Supplementary Data).
ABC-C hyperactivity/noncompliance subscale score
There was a significantly higher reduction in the ABC-C hyperactivity/noncompliance subscale scores in the simvastatin arm compared with the placebo arm by the endpoint (Table 2). There was also a significant time × treatment interaction between the two treatment arms [two-way ANOVA with Greenhouse-Geisser correction: F (df, mean square) = 9.16 (1.60, 96.45), p = 0.001]. Participants in the simvastatin arm were subject to a significantly higher rate of partial and complete response to treatment compared with the placebo arm by the endpoint (Table 3) (Supplementary Data).
ABC-C inappropriate speech subscale score
There was no significant difference in mean change of the ABC-C inappropriate speech subscale scores between the simvastatin and placebo arms by the endpoint (Table 2). Also, there was no significant time × treatment interaction between the two treatment arms [two-way ANOVA with Greenhouse-Geisser correction: F (df, mean square) = 1.58 (1.52, 1.30), p = 0.214] (Supplementary Data).
Adverse events
There were no significant differences between the simvastatin and placebo arms in terms of incidence of adverse events (Table 4). Also, there was no significant difference in mean change of the ESRS scores between the simvastatin and placebo arms by the endpoint [mean difference (95% CI) = 0.06 (−0.13 to 0.25), t (df) = 0.63 (64), p = 0.534] (Supplementary Data).
Fisher's exact test is used, two-tailed p-values are presented.
Discussion
We found that there were dramatically higher reductions as well as strong time × treatment interactions in the ABC-C irritability and hyperactivity/noncompliance subscale scores in the simvastatin arm compared with the placebo arm by the end of the trial. Further, patients in the simvastatin arm experienced higher partial and complete response rates based on change in the ABC-C irritability and hyperactivity/noncompliance subscale scores. None of these findings were replicated for any of the three other subscales of the ABC-C scale.
To the best of our knowledge, this is the first report of a statin in the treatment of patients with AD or any of the conditions meeting the criteria for ASD. However, our findings can be partially appraised in the context of autism trials that used medications with potential biologic effects comparable to statins. In this manner, most of the published randomized clinical trials of autism on medications with anti-inflammatory properties demonstrated beneficial effects for irritability symptoms and in some cases for other autism-associated symptoms as well whereas the core symptoms remained relatively unchanged. These medications include minocycline (Ghaleiha et al. 2016), pioglitazone (Boris et al. 2007; Ghaleiha et al. 2015), celecoxib (Asadabadi et al. 2013), pentoxiphyline (Akhondzadeh et al. 2010), N-acetylcysteine (Hardan et al. 2012; Ghanizadeh and Moghimi-Sarani 2013; Nikoo et al. 2015), and intravenous immunoglobulin (Boris et al. 2005).
The results of few other clinical trials are inconsistent with our study. A trial of oral human immunoglobulin (IGOH) did not improve behavioral symptoms, including irritability, compared with the placebo in autistic children with chronic persistent GI disturbances; however, IGOH was supposed to mainly result in local gastrointestinal mucosal effects rather than systemic effects (Handen et al. 2009). Adrenocortocotrophic hormone (ACTH) administration also did not make an improvement in the ABC-C subscales, including irritability, in two trials of autism (Buitelaar et al. 1990, 1992) where it was supposed to induce anti-inflammatory/immunosuppressive effects indirectly through increasing synthesis of corticosteroids.
Although the neuroprotective effects of statins, especially simvastatin, are well documented through numerous studies on several pathologic conditions to date, the available evidence is inconclusive regarding their exact mechanism of action in each condition (van der Most et al. 2009; Ling and Tejada-Simon 2016). Here, we hypothesize their potential mechanisms of action in autism based on available literature. Statins inhibit the synthesis of cholesterol and downstream isoprenoids through the mevalonate pathway (van der Most et al. 2009; Ling and Tejada-Simon 2016). Altered cholesterol synthesis is highly implicated in autism (Wang 2014). It seems that statins reduce insoluble Aβ peptide levels and Aβ plaque load through cholesterol-dependent mechanisms (van der Most et al. 2009; Ling and Tejada-Simon 2016), whereas dysregulation in the amyloid precursor protein (precursor to Aβ peptide) biochemical pathway is documented in autism (Westmark et al. 2016). Further, statins influence regulation of the Wnt/β-catenin signaling pathway, brain-derived neurotrophic factor, and nuclear factor kappa B (Ling and Tejada-Simon 2016), all of which are proposed as important molecules in the neurobiology of autism (Young et al. 2011; Das 2013; Willsey and State 2015). Statins also have anti-inflammatory/immune modulatory effects. They reduce lipid peroxidation, production of reactive oxygen species, and nitric oxide (van der Most et al. 2009), whereas increased oxidative damage and reactive oxygen species are detected in brains of individuals with autism (Rossignol and Frye 2014). In addition, they reduce leukocyte infiltration capability, interfere with antigen presentation to T cells, decrease pro-inflammatory cytokine levels, increase anti-inflammatory cytokines, and inhibit microglial activation (van der Most et al. 2009), which are especially important while considering the evidence of immune/inflammatory changes in autism, including variations in genes coding for cell surface proteins that are important in antigen presentation (e.g., HLA genes), increased levels of pro-inflammatory cytokines (e.g., IL-1, IL-6, TNF-α) in brain specimens and cerebrospinal fluid, decreased levels of anti-inflammatory cytokines (e.g., IL-10, TGFβ), and enhanced microglial and astrocytic activation (Estes and McAllister 2015; Young et al. 2016).
This study is subject to some limitations. First, the results should be interpreted with caution in terms of generalizability, considering that all of the participants were treated with the same anti-psychotic (i.e., risperidone) and among the four conditions meeting the criteria for ASD, only those children with AD were included. However, these two factors together reduced unwanted bias. Second, the trial duration was not enough for assessment of simvastatin long-term beneficial effects and adverse events. Third, ethical considerations made it impossible to use simvastatin and placebo as single treatments in participants. In fact, although we found no reports of interaction between risperidone and simvastatin, in one study risperidone demonstrated anti-inflammatory effects by reducing pro-inflammatory cytokines (MacDowell et al. 2013), which implies the probability of a synergism between simvastatin and risperidone toward greater symptom improvement in the simvastatin arm. Fourth, although we checked for history of autoimmune diseases in participants, we did not carry out a biological assessment of immune/inflammatory states. It is plausible that a subgroup of patients with prominent immune dysregulation/inflammation may improve more significantly in response to medications such as statins. Meanwhile, a sample size of 66 with a power of about 90% is among the strengths of this study.
Conclusion
Overall, this was the first study to provide evidence for the potentially beneficial effects of simvastatin in the treatment of children with autism. Future investigations are warranted with the same medication as well as other statins such as lovastatin to both confirm the results and scrutinize exact mechanisms of action.
Clinical Significance
Our data favor greater improvement of irritability and hyperactivity symptoms in children with autism who received simvastatin compared with placebo. Meanwhile, simvastatin failed to improve core symptoms of autism, which is a major challenge in the treatment of autism. This was a preliminary study of simvastatin in autism and is subject to some limitations as discussed earlier, which warrants future investigations before considering statins as plausible medications in autism. Future clinical trials may not provide additional data about the applicability of statins in autism unless biological measurements are recruited and long-term effects are evaluated.
Footnotes
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.