
Abstract
To the Editor:
S
Case Report
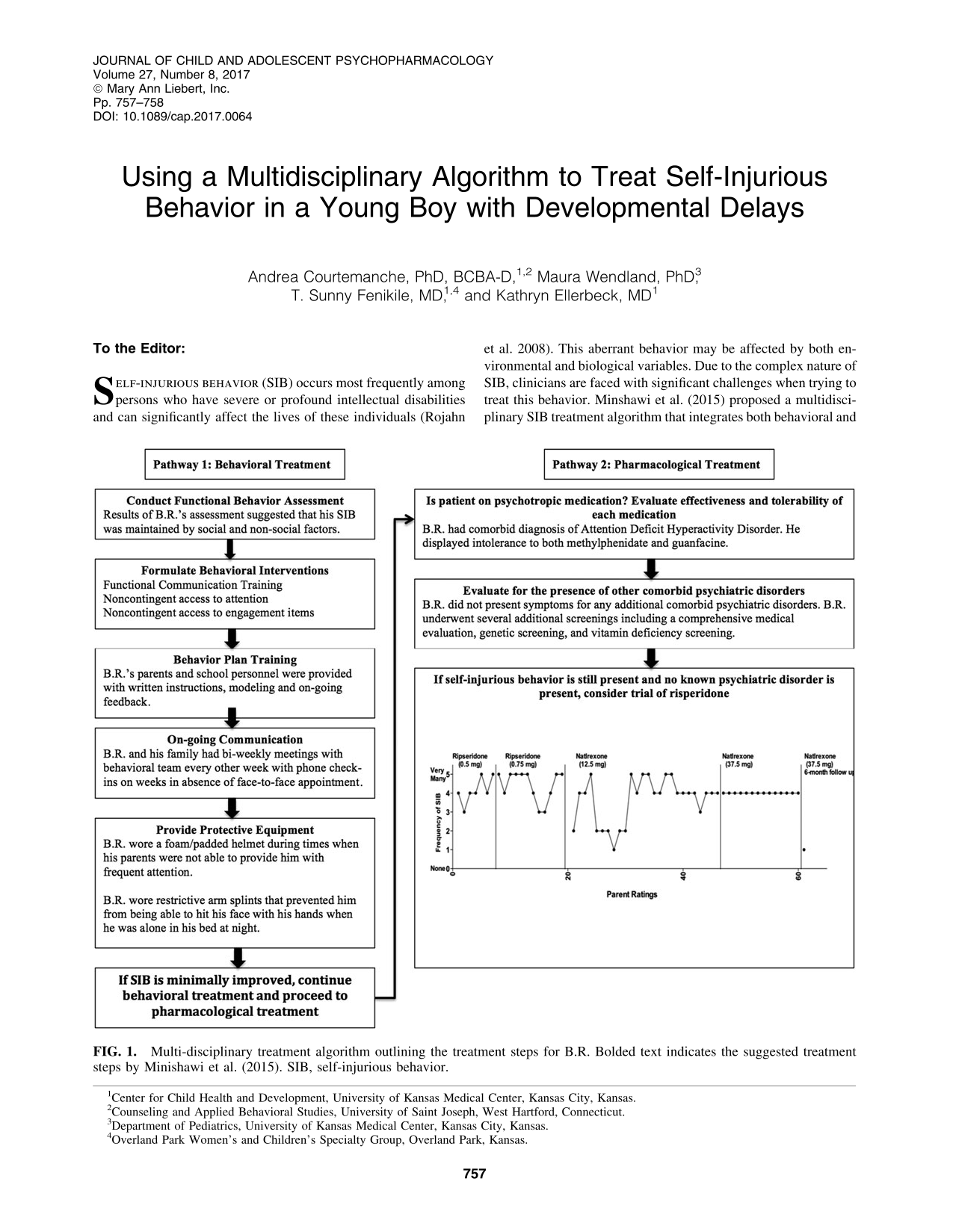
B.R. was a nonverbal, 6-year-old male born with a chromosomal deletion (9p13.3–13.1) and presented with a global developmental delay. B.R. was referred to a developmental pediatrician at a university-based child development center because of his high rates of self-injurious (i.e., head hitting, head banging, elbow and knuckle banging, eye poking, tongue pulling, and self-biting), repetitive, and hyperactive behavior. In addition to the developmental pediatrician, B.R. and his family participated in an outpatient problem behavior clinic at the same center. The treatment algorithm and specific treatment steps for this case are presented in Figure 1.
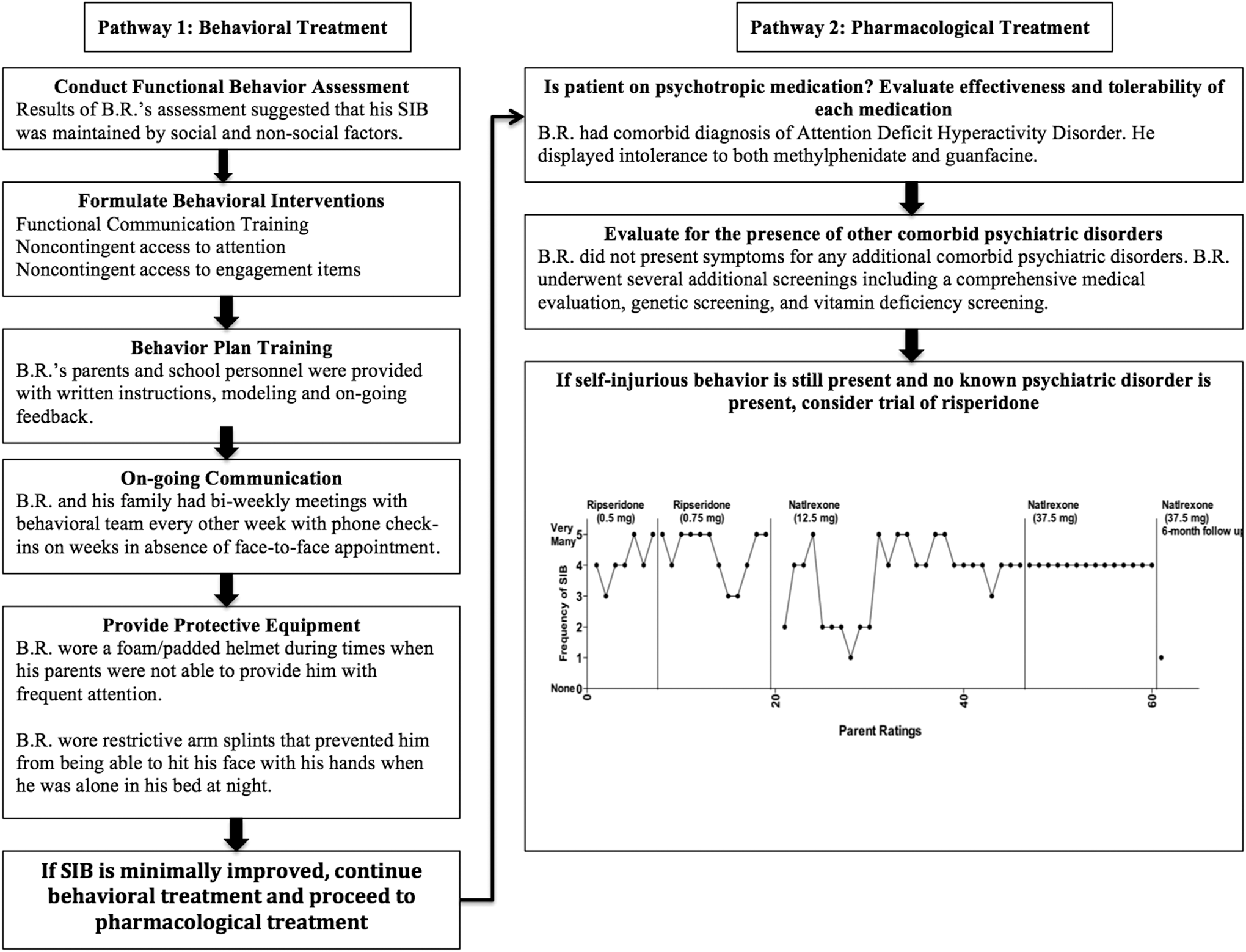
Multi-disciplinary treatment algorithm outlining the treatment steps for B.R. Bolded text indicates the suggested treatment steps by Minishawi et al. (2015). SIB, self-injurious behavior.
Discussion
After conducting a functional behavior assessment, B.R.'s SIB appeared to be maintained by both social (e.g., receiving attention contingent on SIB) and nonsocial consequences (e.g., self-stimulation). Based on observations and parental report, the function-based behavioral intervention (i.e., functional communication training and noncontingent reinforcement) was moderately effective at reducing overall rates of SIB. In conjunction with the behavioral intervention, the effects of two different medications were also evaluated: risperidone and naltrexone. Based on daily parental ratings, risperidone, at all doses, exacerbated SIB and was discontinued. In the first 2 weeks after starting naltrexone (12.5 mg), based on parental ratings, there was a dramatic reduction in the frequency of SIB. B.R.'s parents also reported observing increases in expression of pain-related behaviors after he engaged in SIB. Individuals with chronic SIB may have elevated opioid activity that may produce a chronic state of analgesia (Sandman and Kemp 2011). Due to the antagonistic action of naltrexone, opioids cannot bind to the receptors, increasing the likelihood of experiencing the painful effects of SIB. After 2 weeks of taking naltrexone, the parental ratings of the frequency of SIB increased. The dose of naltrexone was increased (37.5 mg) and the ratings of the frequency of the SIB remained stable at “many” instances each day. At a 6-month follow-up with B.R.'s family, they reported the overall frequency of B.R.'s SIB was “few.”
In conclusion, this case study describes the decision-making process for the treatment of frequent SIB in a young child with developmental delays. The multidisciplinary treatment algorithm proposed by Minishawi et al. (2015) may be a helpful guide for other clinicians confronted with treating frequent and severe SIB. Lastly, treatment providers should collaborate across disciplines to create the most comprehensive treatment plan, including both behavioral and pharmacological treatments.
Footnotes
Disclosures
No competing financial interests exist.