
Abstract
Objective:
An extended-release amphetamine (AMP) oral suspension has been developed to facilitate medication ingestion and dose titration. This study sought to determine the pharmacokinetic (PK) profile of this new formulation in children with attention-deficit/hyperactivity disorder (ADHD).
Methods:
This was an open-label, single-period, PK study in 29 pediatric participants with ADHD. Participants were stratified into age groups 1 (6–7 years), 2 (8–9 years), and 3 (10–12 years), and dosed with 15 mL extended-release AMP liquid suspension (equivalent to 30 mg mixed AMP salts) after an overnight fast. Blood samples were collected at prespecified time points and analyzed for
Results:
All participants completed the study. As age increased, mean maximum and total exposure to AMP decreased; weight-normalized CL/F slightly increased, resulting in decreasing T1/2 values with age. For
Conclusions:
Exposure (Cmax, AUCinf, and AUClast) to AMP decreased with age, possibly as a result of the 30-mg/15-mL fixed dose across a range of weights (20–57 kg) and the consequent lower dose per kilogram in older participants, as well as the slight increase in clearance with age.
Introduction
A
The first-line pharmacological therapy for ADHD is stimulant medication, either methylphenidate or amphetamine (AMP) (Wolraich et al. 2011a; Rabito-Alcon and Correas-Lauffer 2014). While both stimulants are available in immediate-release and extended-release formulations, the majority of stimulants prescribed for ADHD are extended release, because their release profile allows for once-daily dosing, continued treatment coverage during the day, reduced stigma associated with dosing during school hours, and potentially improved medication adherence (Olfson 2004; Cascade et al. 2008; Feldman and Belanger 2009; Buitelaar and Medori 2010).
ADHD practice guidelines recommend treatment individualization for patients (Wolraich et al. 2011b). This requires clinicians to consider multiple factors when choosing medications for a given patient—a medication class and a dose regimen with a high likelihood of treatment success and tolerable side effects, along with a formulation that meets the needs of the individual patient (Wolraich et al. 2011b; Lopez and Leroux 2013). As part of treatment individualization, dosing flexibility is often necessary to achieve an optimized dose (Wolraich et al. 2011b). In addition, patients may experience swallowing difficulties or prefer not to swallow intact capsules or tablets (Marquis et al. 2013). A recent survey demonstrated that swallowing difficulties affected 12.9% of children and 12.8% of adults with ADHD, leading to significant medication discontinuation (Childress, 2016). To ease medication ingestion and to fulfill the need for treatment individualization, the ADHD treatment arsenal should include a variety of medications and formulations.
A new AMP formulation, extended-release AMP oral suspension, has recently been developed for the treatment of ADHD. This formulation provides a once-daily dosing regimen, eliminates the need to swallow intact tablets or capsules, and allows for dosing flexibility. Extended-release AMP oral suspension is produced using a cation exchange technology. During the manufacturing process,
As part of the development program, clinical studies have assessed the pharmacokinetic (PK) properties of this new formulation in adults. Extended-release AMP oral suspension was shown to be bioequivalent to a commonly prescribed extended-release AMP medication, Adderall XR® (Shire US, Inc., Lexington, MA), under fasted conditions, confirming its extended-release profile. In addition, the presence of food had no significant impact on the PK profile of extended-release AMP oral suspension. The objective of this study was to determine the PK profile of the extended-release AMP oral suspension in children with ADHD under fasted conditions.
Methods
Study design
This single-dose, single-period, one-treatment, PK study was approved by the institutional review board (IRB; Copernicus Group IRB, Durham, NC). The study was conducted in accordance with the United States Investigational New Drug regulations (21 CFR 50, parts 54, 56, and 312), International Conference on Harmonisation (ICH) guidelines, and the most recent guidelines of the Declaration of Helsinki. Written informed consent/assent from both the parent/legal guardian and child was obtained before performing any study-related procedures. The nature, duration, and purpose of the study, and the action of the drug were explained orally and in writing in the IRB-approved informed consent form and assent form, in such a manner that the subject and parent/legal guardian were aware of the study procedures and potential risks associated with participation in the study. They were informed that the subject could withdraw from the study at any time and received all information that was required by federal regulations and ICH guidelines.
The study was conducted at two clinical sites (Atlanta Center for Medical Research, Atlanta, GA, and MRA Clinical Research, South Miami, FL). Enrolled participants were male and female children between 6 and 12 years of age, who had a diagnosis of ADHD based on Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR; American Psychiatric Association, 2000) (combined, predominantly inattentive, or predominantly hyperactive-impulsive subtype, as established by Kiddie Schedule for Affective Disorders and Schizophrenia-Present and Lifetime Version), a history of positive response to AMP treatment for at least 1 month before screening (had been on treatment for at least 3 months), and a body mass index (BMI) for age <95th or >15th percentile as per the Center for Disease Control BMI sex-specific charts.
Exclusion criteria included adverse reactions or allergy to AMP or any components of the study drug; a history or presence of suicidal ideation or suicidal behavior as assessed by the Columbia Suicide Severity Rating Scale (C-SSRS, Pediatric Baseline Version and Pediatric Since Last Visit Version); tic disorder or Tourette's syndrome; seizure disorder; clinically significant cardiovascular, cerebrovascular, renal, hepatic, gastrointestinal, pulmonary, immunological/oncological, dermatological, hematological, endocrine, neurological, or psychiatric disease, or any other condition that may have jeopardized the safety of the participant or the validity of the study results; positive results at urine drug screen; or clinically significant abnormal finding on physical examination, medical history, electrocardiogram (ECG), or laboratory results at screening. In addition, participants were not permitted to take any over-the-counter medications, consume alcohol or tobacco products, or engage in strenuous exercise during the study. Concomitant prescription medications were not recommended during the study. In cases where concomitant medications were necessary, the use of the medications needed to be approved by the investigator and documented.
Participants were stratified into three age groups: 6–7 years old, 8–9 years old, and 10–12 years old. After screening for eligibility, enrolled participants first entered a 4-day washout period during which they discontinued their previously prescribed AMP medications (study days 1–4). Participants were admitted to the research center the evening before study drug administration to ensure a minimum 10-hour fast. On study day 5, participants were dosed with 15 mL of extended-release AMP oral suspension (equivalent to 30 mg mixed AMP salts [MAS]) without water. Food was not permitted until 4 hours postdose, and water was not permitted from 1 hour predose to 1 hour postdose. To closely monitor for potential adverse events (AEs) associated with drug administration, participants were instructed to stay in their seats for the first 4 hours after dosing. Thereafter, participants remained in-house until the completion of the 12-hour blood sampling. Various activities (e.g., videos, reading, arts and crafts, and games) were offered to the participants to occupy their time at the clinical sites. Participants returned to the research center for an outpatient visit ∼24 hours postdose. After the final blood sample collection at the outpatient visit, participants were permitted to resume their usual ADHD medications.
PK sample collection and analysis
A total of eight blood samples for PK assessment were collected at 0 (predose), 0.75, 2, 3.5, 5.5, 8, 12, and 24 hours postdose. Of these samples, seven were collected in-house, and the last one was collected at the final outpatient visit. Plasma from blood samples was analyzed at Worldwide Clinical Trials (Austin, TX) for
PK parameters
Concentration–time data were analyzed by noncompartmental methods using Phoenix™ WinNonlin® Version 6.3 (Certara USA, Inc., Princeton, NJ). The following PK parameters were determined: maximum plasma concentration (Cmax), time to maximum plasma concentration, elimination half-life (T1/2), area under the plasma concentration–time curve from time 0 to the last quantifiable concentration (AUClast), area under the concentration–time curve from time 0 extrapolated to infinity (AUCinf), oral clearance (CL/F), and volume of distribution in the terminal phase (Vz/F). Weight-normalized (by kg) CL/F, Vz/F, and AUClast were also calculated.
Statistical methods
Statistical analyses were performed using SAS® for Windows® Version 9.3 (SAS Institute, Cary, NC). The PK parameters for
The study had a planned sample size of 30 participants, which was determined based on the number of participants needed to complete the PK analysis. Regulatory guidelines require at least four participants in each age group to complete the PK analysis. From a statistical perspective, assuming a 20% intersubject variability estimated from previous PK studies of AMP in children with ADHD (Ermer et al. 2010), eight completed participants in each age group should provide 80% power to target a 95% CI within 60% and 140% of the geometric mean estimates of clearance and volume of distribution, in accordance with the Food and Drug Administration guidance, General Clinical Pharmacology Considerations for Pediatric Studies for Drugs and Biological Products (Food and Drug Administration 2014). Accounting for a 10% attrition rate, 10 participants per age group were planned for enrollment to ensure that eight of them would provide evaluable PK data. Combining all three age groups, a total of 30 participants were required for the study.
Safety assessments
Safety assessments consisted of physical examinations, ECGs, C-SSRS Pediatric Baseline Version and Pediatric Since Last Visit Version, vital signs, and routine laboratory tests, including a urine drug screen and a urine pregnancy test (for females who were postmenarche), and monitoring for AEs. Physical examinations, laboratory tests, and ECGs were performed at screening and the 24-hour postdose outpatient visit. Adverse events were assessed throughout the study period, and participants' parents or legal guardians were instructed to contact the site for any AE that was not reported at the previous visit. The final safety assessment took place at the end-of-study outpatient visit.
Results
Participant disposition and baseline characteristics
A total of 29 participants were enrolled, all of whom completed the study and were included in the PK analysis (22 male participants and 7 female participants). There were nine participants (31.0%) in the 6–7-year age group and 10 participants (34.5%) each in the 8–9-year and 10–12-year age group. Participants' BMI ranged from 14.6 to 23.8 kg/m2, and the majority of the participants were black/African American. No participant used concomitant medications during the study. Detailed participant demographic information and baseline characteristics are shown in Table 1.
BMI, body mass index; N, number of participants; SD, standard deviation.
PK assessments
After a single oral dose of extended-release AMP oral suspension, plasma concentrations of
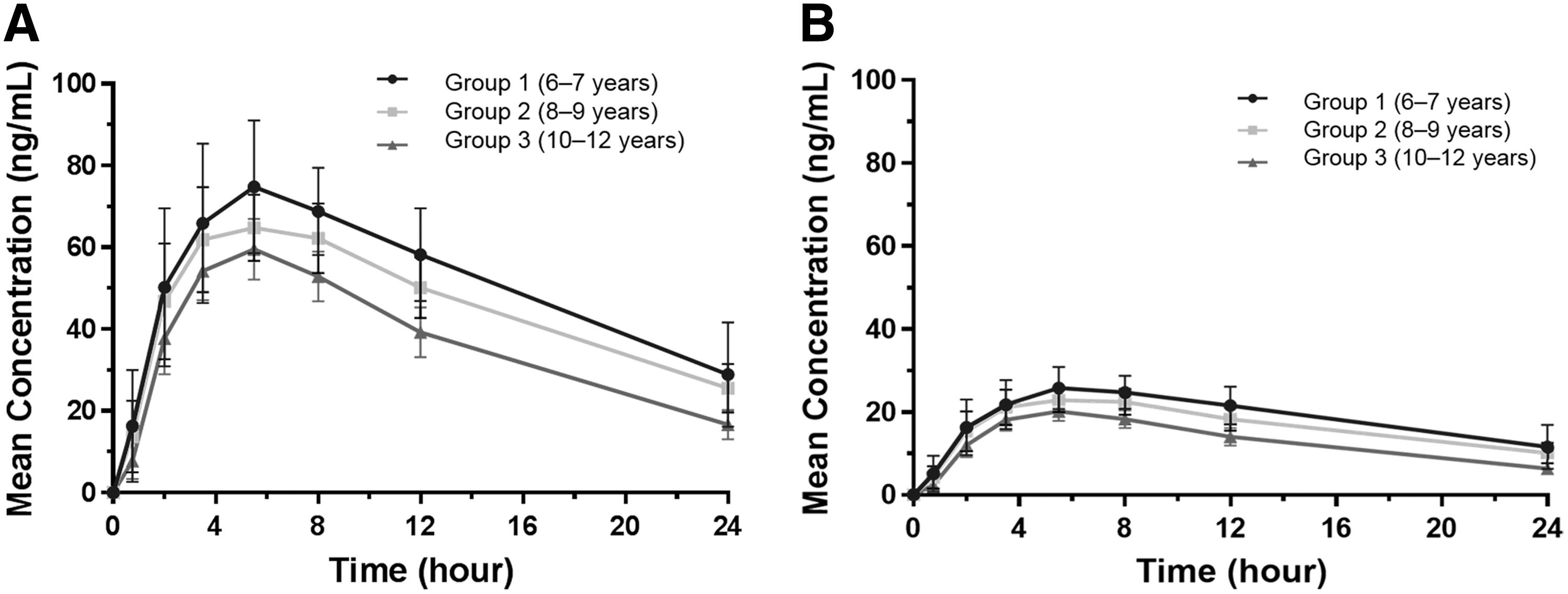
Mean concentration–time profiles of
Following a single dose of extended-release AMP oral suspension, plasma concentrations of
AUCinf, area under the concentration–time curve from time 0 to infinity; AUClast, area under the concentration–time curve from time 0 to last quantifiable concentration; CL/F, oral clearance; Cmax, maximum plasma concentration; h, hours; SD, standard deviation; T1/2, elimination half-life; Tmax, time to maximum plasma concentration; Vz/F, volume of distribution in the terminal phase.
Regarding the statistical analysis of the weight-normalized PK parameters, the 95% CIs for the geometric means of CL/F/kg, Vz/F/kg, and AUClast/kg for
CI, confidence interval.
Safety assessments
Over the course of the study, 12 participants (41.4%) experienced 14 treatment-emergent AEs (TEAEs): sinus tachycardia (determined based on the investigator's judgment; 10 participants [34.5%]), vomiting (three participants [10.3%]), and nausea (one participant [3.4%]). All TEAEs were resolved by the end of the study. There were no serious AEs, deaths, or discontinuations due to TEAEs. Of the 14 TEAEs, 12 were assessed by the investigator to be treatment related, including nine sinus tachycardia events (nine participants [31.0%]), two vomiting events (two participants [6.9%]), and one nausea event (one participant [3.4%]).
There were no abnormal laboratory results, physical examination findings, or ECG results assessed by the investigator as clinically significant. A total of 10 participants had abnormal vital signs that were considered clinically significant and recorded as TEAEs of sinus tachycardia. All these events were mild and resolved by the end of the study. C-SSRS assessment demonstrated that no participant exhibited suicidal ideation or suicidal behavior at any time point during the study.
Discussion
This study assessed the PK profile of a new extended-release AMP oral suspension formulation in children across a range of ages and body weights. The results demonstrated that mean maximum and total exposure to
These results are generally consistent with the findings from studies of other extended-release AMP products. A pediatric PK model for Adderall XR suggested that age and weight were significant factors contributing to intersubject variability in exposure to
The 95% CIs for the geometric means of CL/F/kg, Vz/F/kg, and AUClast/kg for
Residual plasma
Despite the residual AMP 24 hours postdose, drug accumulation in systemic circulation is primarily dependent on the elimination rate and dosing frequency. In this study, T1/2 was in the general range of immediate-release AMP products (e.g., AMP mixed salts tablets [Adderall], 9.11–11.0 hours for
Extended-release AMP oral suspension was well-tolerated in children. All TEAEs during the study were mild and resolved by the end of the study. Reported TEAEs were consistent with the safety profile of other extended-release AMP medications. There were no deaths or discontinuations due to TEAEs. Taken together, extended-release AMP oral suspension may represent an alternative treatment option for ADHD by providing a once daily-dosing regimen with dosing flexibility.
Conclusion
A pharmacokinetic study in children ages 6–12 was performed for a newly developed extended-release AMP oral suspension. Differences in PK parameters between age groups were consistent with studies of other extended-release AMP products. Exposure to AMP decreased with age. This was possibly due to a slight increase in clearance with age and to a lower dose per kilogram in older participants that resulted from the 30-mg/15-mL fixed dose given across a range of weights (20–57 kg). All TEAEs and abnormal vital signs resolved by the end of the study.
Clinical Significance
Extended-release AMP is an effective first-line treatment for children with ADHD, however, some children may have difficulty with oral forms of medication. This study showed that an extended-release AMP oral suspension was well-tolerated in children from 6 to 12 years with ADHD, and overall exposure to AMP decreased with increasing age when a single 15 mL dose was given. This AMP formulation was designed to provide a once-daily dosing option for practitioners to individualize a patient's ADHD treatment.
Disclosures
All authors analyzed the data and provided critical review and editing of all drafts of the article. Liqing Xiao, a medical writer of AlphaBioCom, LLC, wrote the article. R.L.M. is an employee of Neos Therapeutics, Inc. with stock options. Dr. J.G.S. is an employee of Worldwide Clinical Trials. D.E. is an employee of Neos Therapeutics, Inc. with stock options. Dr. C.R.S. is an employee of Neos Therapeutics, Inc. with stock options in Neos Therapeutics, Inc., and stock in Pfizer.
Footnotes
Acknowledgments
This study was sponsored by Neos Therapeutics, Inc. Medical writing assistance was provided by Liqing Xiao, PhD, of AlphaBioCom, LLC.