
Abstract
Objectives:
The increased number of adolescents diagnosed with attention-deficit/hyperactivity disorder (ADHD) in recent years has raised concerns regarding diversion and misuse of prescription stimulant medications. As prescribers of these medications, physicians must be prepared to educate patients on these issues. This is the first study to evaluate physician training and qualification to educate adolescent patients on stimulant diversion and misuse.
Methods:
A questionnaire was developed and mailed to a national sample of child and adolescent psychiatrists (CAPs), child neurologists (CNs), and developmental-behavioral pediatricians (DBPs) in the United States. In addition to descriptive statistics, multivariable regressions (log-binomial and ordinal logistic) were performed to identify differences between subspecialists.
Results:
The final sample consisted of 826 physicians who currently prescribe stimulants. Only 48% of physicians reported receiving formal training on prescription drug diversion (PDD) in medical school, residency, and/or fellowship. Twenty five percent and 48% of physicians felt inadequately qualified to educate patients on the health and legal consequences, respectively, of stimulant misuse and diversion. CAPs were more likely to have received formal training and felt better qualified to educate patients than CNs and DBPs. Physicians who received formal training were 2.4 times more likely to feel adequately qualified to educate patients on these issues. Only 58% of physicians correctly answered a legal question relating to stimulant diversion.
Conclusions:
Most physicians have not received formal training on PDD and many feel inadequately qualified to educate patients on the health and legal consequences of stimulant misuse and diversion. Increased training is needed so physicians can effectively educate patients with ADHD.
Introduction
I
Recent studies have found that a significant number of adolescents misuse stimulants (Poulin 2001, 2007; McCabe et al. 2004; Wilens et al. 2008; McCauley et al. 2010; Viana et al. 2012; Cottler et al. 2013; McCabe and West 2013), highlighting the importance of increased focus on this issue. One literature review found 5%–9% of grade and high school-aged children reported nonmedical stimulant use in the past year (Wilens et al. 2008), and a study of high school seniors found 9.5% had ever misused stimulants (McCabe and West 2013). Many students who misuse stimulants obtain them from peers with ADHD who divert their medication (Poulin 2001, 2007; McCabe et al. 2004, 2011; McCabe and Boyd 2005; DeSantis et al. 2008; Garnier-Dykstra et al. 2012; Rabiner 2013); one study found 26% of adolescent students prescribed methylphenidate diverted their medication (Poulin 2007). These studies focused on adolescents accompany many studies documenting an even greater prevalence of stimulant misuse and diversion in the college-aged population (Hall et al. 2005; Teter et al. 2006; White et al. 2006; DeSantis et al. 2008; Wilens et al. 2008; Rabiner et al. 2009; Garnier-Dykstra et al. 2012; Rabiner 2013).
This mounting evidence of stimulant misuse and diversion, in conjunction with the rise in stimulant prescriptions, suggests an urgent need for effective prevention efforts aimed at youth with ADHD. Although physicians are in a unique position to educate patients on the health risks and legal consequences that result from improper use and unlawful distribution of controlled medications, only a few studies have evaluated stimulant diversion and misuse from a physician's perspective. One study found that 19% of physicians were concerned about diversion when prescribing ADHD medications, but it was published >10 years ago and did not ask further about diversion (Stockl et al. 2002). In another study, Hellerstein et al. reported that physicians rated “abuse potential” as their highest concern when prescribing methylphenidate, but did not provide further information on physician perceptions of stimulant misuse (Hellerstein and Biedermann 2003).
To our knowledge, only one research report has evaluated physician training and qualification regarding diversion of controlled prescription drugs (The National Center on Addiction and Substance Abuse at Columbia University, 2005). In this unpublished survey, a minority of physicians received instruction in identifying diversion of controlled medication (including opioids, depressants, and stimulants) in medical school (19.1%), residency (39.2%), and continuing medical education (34.2%). And although more physicians received training on prescription drug abuse, less than a quarter of physicians felt “very qualified” to diagnose prescription drug abuse, and only 11.5% believed they were “very knowledgeable” about controlled substance laws (The National Center on Addiction and Substance Abuse at Columbia University, 2005). Unfortunately, this study has several limitations: it was conducted in 2004, did not include many physicians who have expertise in childhood ADHD, and was not focused on stimulant medication.
The objective of our study was to determine to what extent pediatric subspecialists with expertise in the treatment of ADHD have received prior training about prescription drug diversion (PDD) and to assess these physicians' perceived and actual qualifications to educate patients with ADHD about stimulant misuse and diversion.
Methods
Study design
A questionnaire on stimulant diversion and misuse by high school students was created and mailed to child and adolescent psychiatrists (CAPs), child neurologists (CNs), and developmental-behavioral pediatricians (DBPs). Mailing labels for CAPs (n = 3021) and CNs (907) were obtained from the American Medical Association; labels for DBPs (n = 579) were obtained from the Society for Developmental and Behavioral Pediatrics. In total, questionnaires were sent to 4507 pediatric subspecialists in the United States. The study received approval from the North Shore-Long Island Jewish Institutional Review Board.
Measures
The four-page questionnaire assessed physicians' demographic characteristics, perceptions of pervasiveness of stimulant diversion and misuse, training and qualification to educate on this issue, patient education practices, and specific strategies employed to prevent diversion. This article focuses on physician training and qualifications to educate patients on stimulant misuse and diversion. All of the questionnaire items included in these analyses are listed in Figure 1.
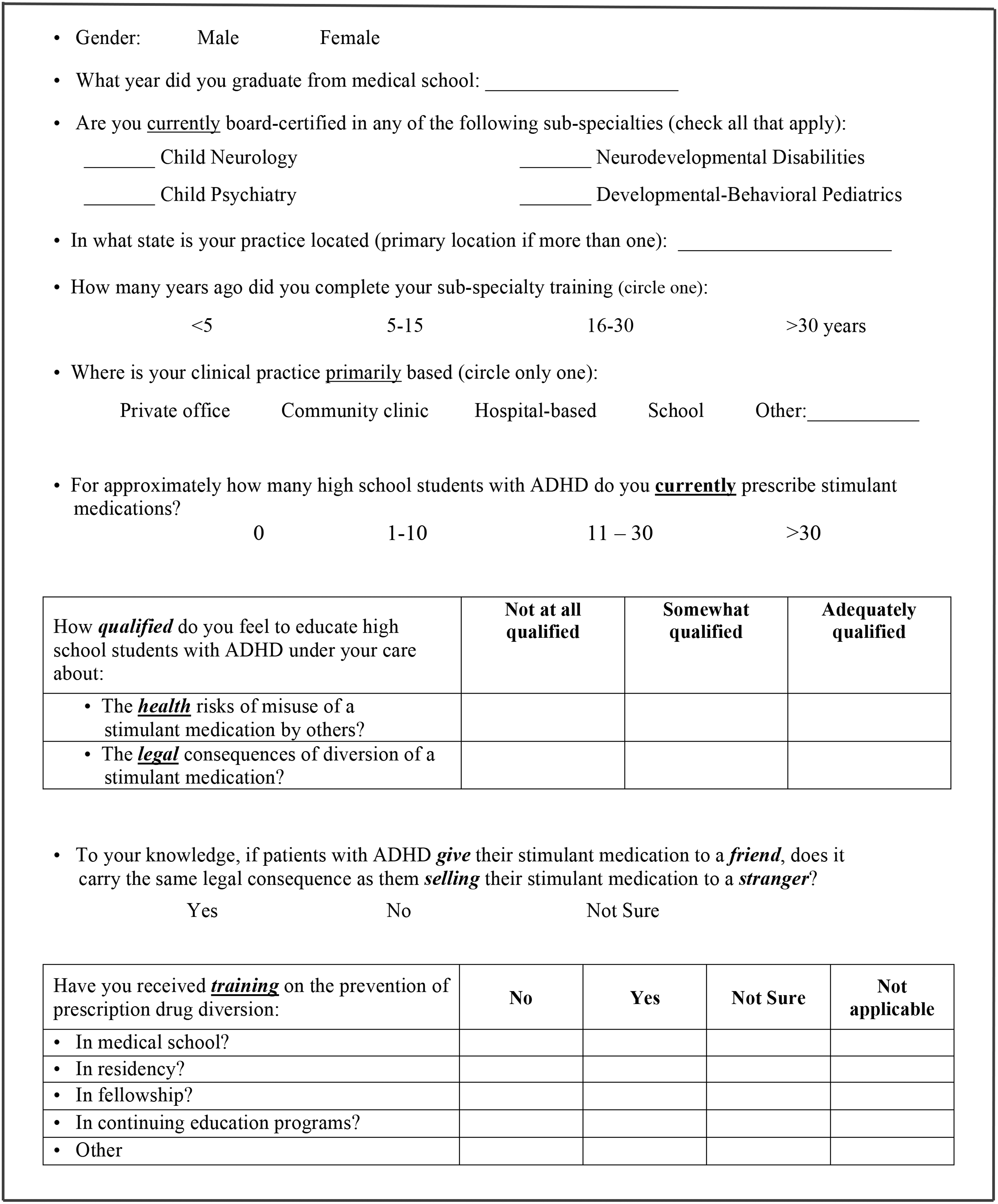
Items from the “Diversion of Stimulant Medication” Physician Questionnaire.
Data analysis
Responses were compiled and coded in a Microsoft Excel document. Distributional assumptions of variables were checked using histograms, q-q plots, and Shapiro–Wilks tests before conducting statistical analysis. Differences in sample characteristics between groups were examined using chi-square analysis for categorical variables. Multivariable regression (log-binomial and ordinal logistic) was used to generate risk ratios (RRs), odds ratios (ORs), and their confidence intervals (CIs) to study the associations between training and perceived qualification and actual knowledge of the legal consequences of stimulant diversion. Potential covariates were first examined for effect measure modification by testing interaction terms in the models; no variables were significant effect measure modifiers. Confounding variables were identified a priori from hypothesized relationships among the variables of interest; these were included in regression models to produce adjusted effect estimates, including adjusted risk ratios (aRRs) and adjusted odds ratios. SAS statistical software (9.3) was used for analyses.
Results
In total, 894 healthcare professionals completed questionnaires, but only responses from Board-certified pediatric subspecialists who currently prescribe stimulant medications and whose subspecialty was clearly identifiable were included in the analysis. The final sample consisted of 826 physicians: 579 CAPs, 106 CNs, and 141 DBPs, with an overall response rate of 18%. Physicians in 49 states were represented in the sample, with a mean medical school graduation date of 1991 (standard deviation (SD): 10; range: 1957–2012). By subspecialty, CAPs had a mean graduation date of 1992 (SD: 8; range: 1974–2012); CNs, 1987 (SD: 12; range: 1959–2007); and DBPs, 1986 (SD: 12; range 1957–2010). Table 1 includes additional sample demographics.
p-values reflect chi-square comparisons between CAPs, CNs, and DBPs.
Responses were missing from one physician.
Responses were missing from 11 physicians.
CAPs, child and adolescent psychiatrists; CNs, child neurologists; DBPs, developmental-behavioral pediatricians.
One-fourth (25%) of all physicians did not feel adequately qualified to educate patients about the health risks of stimulant misuse, and 48% did not feel adequately qualified to educate patients about the legal consequences of stimulant diversion. Subspecialists differed in their perceived qualifications (Fig. 2). After adjusting for confounding variables, ordinal logistical regressions revealed CAPs were more likely to perceive themselves as well qualified to educate patients—both on the health risks of stimulant misuse (compared with CNs and DBPs) and legal consequences of stimulant diversion (compared with CNs) (Table 2).
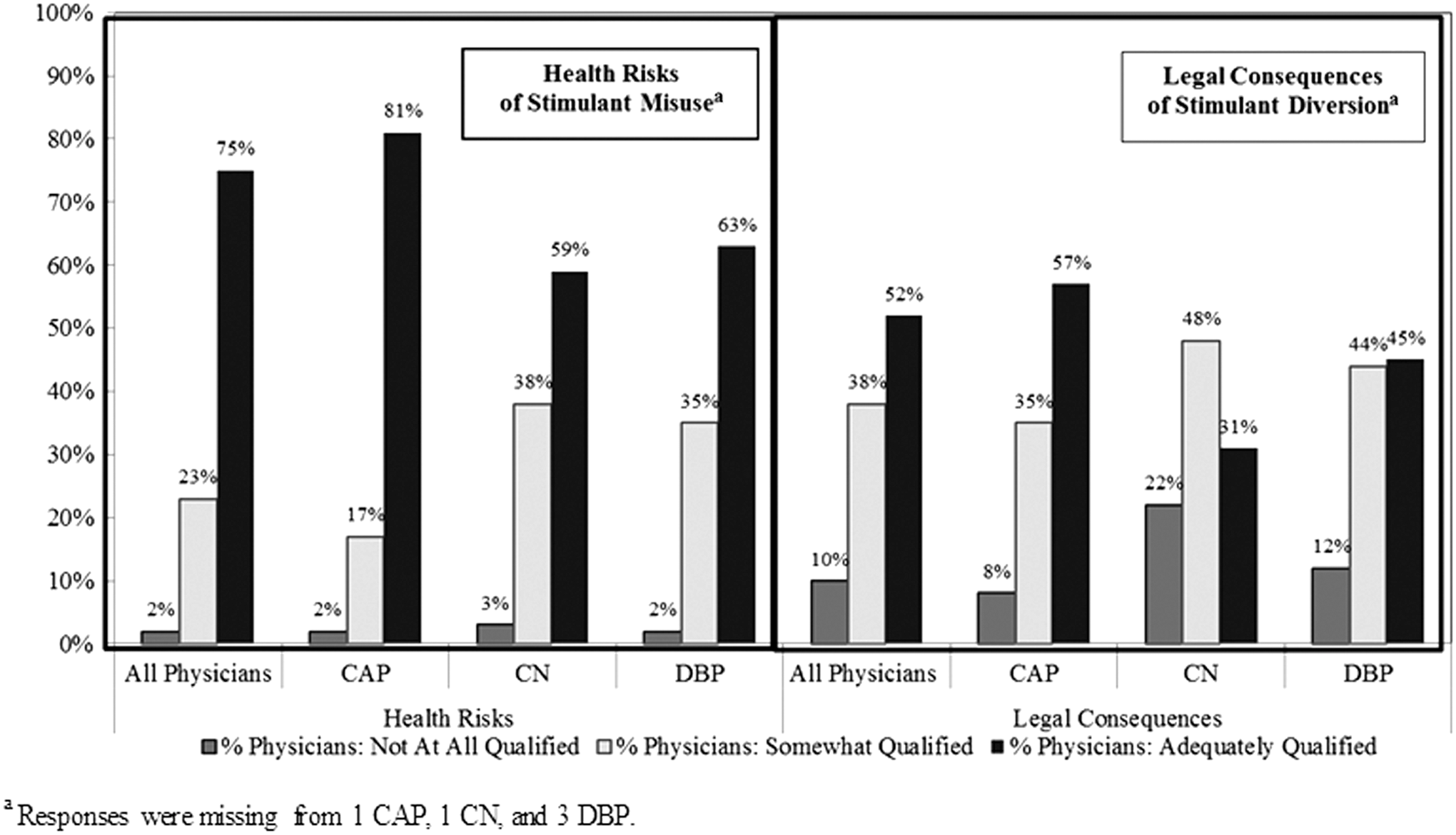
Perceived qualification of CAPs, CNs, and DBPs to educate patients about the health risks of stimulant misuse and the legal consequences of stimulant diversion. CAPs, child and adolescent psychiatrists; CNs, child neurologists; DBPs, developmental-behavioral pediatricians.
Responses were missing from one CAP, one CN, and three DBPs.
Adjusted odds ratios included variables for prescription volume, recency of subspecialty training, and whether the physician received training in any formal domain on prescription drug diversion. Responses were missing from 11 physicians for recency of subspecialty training variable and 26 physicians for any formal domain training variable.
CAP subspecialists were considered as the reference group for these analyses.
OR, odds ratio; CI, confidence interval.
To assess physician knowledge of the legal consequences of stimulant diversion, physicians were asked whether giving away one's stimulant medication carries the same legal consequence as selling one's medication. Only 58% of physicians answered correctly (“Yes”); 11% answered incorrectly (“No”), and 31% were unsure. Fifty seven percent of CAPs, 64% of CNs, and 56% of DBPs answered the question correctly; CNs (RR = 1.12, 95% CI: 0.95–1.32) and DBPs (RR = 0.99; 95% CI: 0.84–1.17) were no more likely than CAPs to answer the question correctly compared with CAPs. Only 68% of all physicians who felt “adequately qualified” to educate patients on legal consequences answered the legal question correctly. By contrast, this question was answered correctly by 50% of physicians who felt “somewhat qualified” and 33% who felt “not at all qualified” to educate on legal consequences. Physicians who felt adequately qualified were 1.5 times more likely to answer the question correctly compared with those who perceived themselves as “not at all” or “somewhat” qualified to educate on this issue (RR = 1.46, 95% CI: 1.29–1.65).
Forty eight percent of physicians had received training on PDD in at least one “formal domain” (i.e., medical school, residency, or fellowship). Specifically, 18% of physicians received training regarding this issue in medical school, 35% in residency, and 42% in fellowship. Fifty two percent were educated about PDD in continuing medical education. Taken together, 67% of physicians (70% CAPs, 58% CNs, and 63% DBPs) received formal training on PDD at some point in their professional training.
Training differences existed across subspecialties (Table 3). Fifty three percent of CAPs had received training on PDD in at least one formal domain compared with 34% of CNs and 36% of DBPs. CAPs were also more likely to have received PDD training specifically in residency and fellowship. Training differences were also observed in relation to recency of physicians' completion of subspecialty training (Table 4). Sixty six percent of physicians who completed subspecialty training <5 years ago received PDD training in any formal domain, while those who completed subspecialty training 5 or more years ago were significantly less likely to have received this training when controlling for gender and subspecialty. Notably, the difference in training was most pronounced between those who graduated <5 years ago and those who graduated >15 years ago (aRR = 0.52; 95% CI: 0.43–0.62). Conversely, compared with physicians who completed subspecialty training <5 years ago, physicians who completed subspecialty training 5 or more years ago were more likely to receive PDD training in continuing education programs.
Any formal domain includes medical school, residency, and/or fellowship.
Responses were missing from 6 CAPs, 5 CNs, and 15 DBPs.
Responses were missing from 24 CAPs, 5 CNs, and 11 DBPs.
Responses were missing from 15 CAPs, 4 CNs, and 10 DBPs.
Responses were missing from 11 CAPs, 6 CNs, and 17 DBPs.
Responses were missing from 22 CAPs, 4 CNs, and 7 DBPs.
CAP subspecialists were considered as the reference group for these analyses.
RR, risk ratio.
Any formal domain includes medical school, residency, and/or fellowship.
Responses were missing from 6 CAPs, 5 CNs, and 15 DBPs.
Responses were missing from 24 CAPs, 5 CNs, and 11 DBPs.
Responses were missing from 15 CAPs, 4 CNs, and 10 DBPs.
Responses were missing from 11 CAPs, 6 CNs, and 17 DBPs.
Responses were missing from 22 CAPs, 4 CNs, and 7 DBPs.
Responses were missing from 11 physicians on recency of subspecialty training.
Adjusted risk ratio (aRR) models included variables for gender and subspecialty type. Responses were missing from one physician for gender variable.
Physicians who completed their subspecialty training <5 years ago were considered as the reference group for these analyses.
Physicians who received formal PDD training were increasingly likely to perceive themselves as being qualified to educate on the health risks of stimulant misuse (OR = 2.43, 95% CI: 1.73–3.41). Fifty three percent of physicians who received this training felt adequately qualified to educate on this topic compared with 47% of physicians who did not receive or were unsure whether they had received formal PDD training. Physicians who received formal PDD training were also increasingly likely to perceive themselves as being qualified to educate on the legal consequences of stimulant diversion (OR = 2.43, 95% CI: 1.84–3.20). Fifty eight percent of physicians who received PDD training felt adequately qualified to educate on legal consequences compared with 42% of physicians who did not receive or were unsure whether they had received this training.
Discussion
This is the first study to assess physician training and perceived qualification to educate patients about diversion and misuse of prescription stimulants. A quarter of physicians did not feel adequately qualified to educate patients on the health risks of stimulant misuse, and almost half of physicians did not feel adequately qualified to educate on the legal consequences of stimulant diversion. To the extent that stimulants, if misused or diverted, can have serious health (Brunton et al. 2011) and legal implications (CriminalDefenseLawyer), these findings are quite concerning. All physicians who prescribe stimulants should feel qualified to educate their patients about these issues.
In addition to perceived qualification, this study assessed the actual qualification of physicians to counsel patients about the legal consequences of stimulant diversion by asking a basic yet key legal question. When asked whether giving away a stimulant medication carries the same legal consequence as selling it, only a slight majority of physicians provided the correct answer. This was particularly important because evidence suggests that physicians may have a limited ability to accurately self-assess their own competence (Davis et al. 2006). In addition, other studies have also found that physicians lack adequate knowledge about relevant healthcare laws (Darvall et al. 2001; Rock and et al. 2003).
The positive association between physicians receiving formal training on PDD and feeling well qualified to educate patients reinforces the importance of physician training. Physicians themselves recognize the potential benefits of PDD training; 75.5% of physicians in one survey believed that more training would improve their ability to prevent prescription drug abuse and PDD (The National Center on Addiction and Substance Abuse at Columbia University, 2005). Although there was indeed a direct association between physicians' perceived and actual qualification, it must be noted that one legal question may not adequately reflect physician knowledge. In addition, the fact that many physicians could not answer this question correctly provides further evidence that physicians are not adequately prepared to educate patients about diversion of stimulant medication.
This study highlights the need for additional physician training regarding PDD. One-third of physicians in this study of pediatric subspecialists who prescribe stimulants for ADHD could not affirm that they had ever received PDD training. An unpublished survey performed almost a decade earlier similarly reported on the lack of physician training on this issue (The National Center on Addiction and Substance Abuse at Columbia University, 2005). Although differences in sample composition and questionnaire wording preclude comparison between studies, our more recent findings on physicians' lack of PDD training given to physicians are very concerning given the growing evidence of stimulant misuse (Wilens et al. 2008; McCabe and West 2013) and diversion (Poulin 2007; DeSantis et al. 2008; Garnier-Dykstra et al. 2012; Rabiner 2013) by adolescents. In addition, the rising prevalence of children and adolescents receiving prescription stimulants (Visser et al. 2014) has created an even greater need for physicians to receive comprehensive training on these issues.
CAPs were most likely to have received formal training on PDD. Differences in patient populations may explain these differences, since CAPs are more likely to treat patients with co-occurring conduct disorder and substance use disorder. Wilens et al. (2006) found that every ADHD subjects who diverted stimulants had comorbid conduct disorder or substance use disorder, and 83% of ADHD subjects who reported misused stimulants met criteria for one of these disorders. It is possible that CAPs training programs reflect the fact that patients treated by CAPs are more likely to be at risk for stimulant misuse and diversion. Nevertheless, these training differences between subspecialists are problematic as all physicians who prescribe stimulant medication should receive adequate education on PDD.
This is not the first publication to suggest that physicians should receive better training on substance abuse. A recent editorial on stimulant misuse and diversion asserts that CAPs and pediatricians must receive better training on addiction so they can develop better evaluation, prevention, and treatment skills (Kaminer 2013). Another study recommends that clinicians receive formal training in the assessment of substance use disorders and master at least one screening tool and comprehensive assessment instrument (Winters and Kaminer 2008). Fiellin et al. (2002) further suggest modification of physicians' licensing examinations to include content on counseling methods to prevent the development of substance use disorders. Our findings strengthen these recommendations by providing evidence of the lack of training received by practicing physicians.
In addition, these findings are important to understand in the context of other research evaluating physician perspectives and practices regarding stimulant misuse and diversion. Recent studies that analyzed this same sample of pediatric subspecialists found that 59% of physicians suspected one or more of their youth patients with ADHD had diverted stimulants in the past year, and almost three-fourths believed they had evaluated one or more patients who was feigning symptoms for an initial ADHD diagnosis (Colaneri et al. 2016). The fact that the majority of pediatric subspecialists in our sample suspect stimulant misuse and/or diversion among their own patients emphasizes the importance of providing adequate training to these subspecialists. Furthermore, with regard to physician practices, less than half of physicians educate patients “often” or “very often” regarding the health and legal consequences of stimulant misuse and diversion (Colaneri et al. 2017a). In addition, >80% of physicians “rarely” or “never” implement prevention practices like using medication contracts or distributing print materials, and almost half do not often refer patients to drug counseling or substance abuse treatment when they suspect misuse and/or diversion (Colaneri et al. 2017b). A comprehensive training program for physicians would ideally emphasize the importance of educating patients and implementing prevention practices as needed.
Optimistically, it seems the medical community has started to incorporate PDD into training programs. Physicians who completed their subspecialty training <5 years ago were more likely to have received formal PDD training. Nonetheless, it is still concerning that many prescribing physicians who completed their training recently did not receive formal training on PDD, highlighting the continued need to incorporate this issue into formal medical education. Another encouraging finding is that physicians were most likely to receive continuing education on PDD if they completed subspecialty training >15 years ago. Although it appears that physicians who trained many years ago may be taking initiative to become educated on this issue, clearly this is not universal. PDD must be included in formal training so that all physicians who prescribe controlled medications receive comprehensive education on this issue.
Although these findings have important clinical implications, several methodological weaknesses and limitations must be noted. First, the psychometric properties of the questionnaire developed for this study need to be more formally assessed; although all items were assessed for clarity and revised as needed before distribution of the questionnaire, additional validation studies are warranted. Second, our overall response rate was somewhat low—potentially limiting the generalizability of our findings. However, physician surveys tend to have lower response rates (VanGeest et al. 2007), and the response rate in this study is similar to that noted in other recent studies (Bonevski et al. 2011). Also, since our data were based on self-report, physician estimates of past training are subject to recall and response bias. Finally, this study focused on pediatric subspecialists, thus, our results cannot be generalized to primary care practitioners who treat youth with ADHD.
Conclusions
Many pediatric subspecialists who treat youth with ADHD have not received formal training on PDD, and a significant number of practicing physicians are not adequately prepared to educate about the health risks and legal consequences of diversion of stimulant medications. Future studies should examine the availability and effectiveness of medical education curriculum related to PDD, as well as the effectiveness of physician counseling on a patient's decision to divert or misuse stimulants. With a greater understanding of these issues, it is hoped physicians will be able to better counsel and caution patients appropriately with the goal of decreasing the prevalence of stimulant misuse and diversion.
Footnotes
Clinical Significance
Given the rise in ADHD diagnoses and stimulant prescriptions in recent years, it is important that physicians educate patients about stimulant misuse and diversion. This study finds that many physicians have not received formal training about prescription drug diversion and many do not feel adequately qualified to educate patients about misuse and diversion. Increased training is needed so physicians can effectively educate patients with ADHD and prevent stimulant misuse and diversion.
Acknowledgments
The authors wish to thank Majnu John, PhD, and Sujit Vettam, MS, for their assistance with preliminary data analysis.
Disclosures
No external funding was received for this article. No competing financial conflicts of interest exist.