
Abstract
Objectives:
Assess agreement between self-ratings via the adult attention-deficit/hyperactivity disorder (ADHD) Self-Report Scale (ASRS)-v1.1 Symptom Checklist and clinician ratings via the adult ADHD Investigator Symptom Rating Scale (AISRS) expanded version using DSM-5 adult ADHD patients (referred sample) and ADHD controls (recruited from a primary care physician practice).
Methods:
The ASRS v1.1 Symptom Checklist was administered to measure self-reported ADHD symptoms and impairment, the Adult ADHD Clinical Diagnostic Scale v1.2 was used to establish an adult ADHD diagnosis and the childhood and adult/current sections of the scale were used to provide scores to measure symptoms of childhood ADHD and recent symptoms of adult ADHD, the AISRS to measure ADHD current symptom severity.
Results:
Participants (n = 299; range 18–58), of which 171 were ADHD+ and 128 ADHD−. ASRS and AISRS total scores and individual subsections examining inattention, hyperactivity, emotional dysfunction (EF), and emotional dyscontrol (EC) were all significantly correlated (Spearman's ρ’s = 0.78–0.89, ps < 0.01). Correlations remained significant when controlling for demographic factors and psychiatric conditions.
Conclusions:
The ASRS (self) and AISRS (clinician rated) scales have high agreement. This agreement extended not only the to the core 18 DSM symptoms, but also to the additional 13 symptoms that examine EC and EF.
Introduction
A
The Adult ADHD Self-Report Scale version 1.1 Screener (ASRS v1.1) was developed by the workgroup on adult ADHD for the World Health Organization (Kessler et al. 2005). ASRS v1.1 comprises an 18-item Symptom Checklist (corresponding to the 18 symptoms found in the DSM) to reflect adult presentation of ADHD, and a 6-item screener (items extracted from the symptom checklist) to help identify adults at risk of ADHD. The screener and the symptom checklist were not designed to diagnose adults with ADHD; rather, they are employed to increase identification of possible ADHD cases and increase diagnosis accuracy.
The ASRS was been expanded to include 13 additional symptoms intended to assess executive dysfunction and emotional dyscontrol (Ustun et al. 2017). Executive dysfunction is a deficit of higher order cognitive processes that control self-regulation, ability to prioritize, and to plan multiple tasks. Emotional dyscontrol includes symptoms of irritability, affective lability, and emotional overreactivity. Executive dysfunction and emotional dyscontrol have been debated in the literature as possibly being core symptoms of adult ADHD rather than associated features (Faraone 2000; Biederman et al. 2006c, 2015; Brown 2006; Barkley and Murphy 2010; Kessler et al. 2010).
The Adult ADHD Investigator Symptom Rating Scale (AISRS) is a clinician-administered scale that assesses each of the DSM-5 symptoms of ADHD (Spencer et al. 2010). The AISRS not only uses the adult ADHD prompts from the clinician-administered diagnostic scale the Adult ADHD Clinical Diagnostic Scale (ACDS) v1.2, but each of the stem questions are designed to better capture symptoms of the disorder as they present in adulthood. It has been used and validated many times in a variety of clinical drug trials (Biederman et al. 2006d; Adler et al. 2009; Spencer et al. 2010; Arnold et al. 2014; Adler and Gorny 2015; Goodman et al. 2017).
There have been many studies looking at the convergence of child and parent or other reports for childhood ADHD and a few that looked at the convergence of self and parent or self and partner convergence. Unfortunately, only a few studies have looked at the concordance between self-report and clinician ratings of adult ADHD. Adler et al. (2008) looked at the concordance between the Conners Adult ADHD Rating Scale (CAARS) self and investigator report and found that agreement was generally high at baseline, endpoint, and change scores, with intraclass r ranging between 0.51 and 0.87. Similarly, Kooij et al. (2008) found intraclass correlation coefficients ranging from 0.348 to 0.440 using ADHD-RS self and investigator ratings. Self-ratings at primary care physician (PCP) office would be useful in screening for those with ADHD if these ratings are highly concordant with investigator ratings. This study takes another look at concordance of self-report and investigator ratings of ADHD symptoms using the ASRS and the AISRS (see Table 1 for a comparison of the ADHD symptom language of the two scales).
Organized by ASRS v1.1 Symptom Checklist order.
© Reproduced with permission of World Health Organization (2003).
AISRS symptom domains are listed, not the full stem question or prompts.
ADHD, attention-deficit/hyperactivity disorder; ASRS, Adult ADHD Self-Report Scale; AISRS, Adult ADHD Investigator Symptom Rating Scale.
Methods
Participants
Two samples were pooled together from a larger study whose aim was to update the ASRS Screener for DSM-5: (1) a referred sample of adults who had been recruited as part of the NYU Adult ADHD Program and (2) patients screened for ADHD at a PCP practice in the New York area (Ustun et al. 2017).
The referred sample
This was composed of adults (ages 18–54, inclusive) recruited as part of the NYU Adult ADHD Program (Adler et al. 2017; Ustun et al. 2017). The participants in this sample were administered the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR; American Psychiatric Association 2000) Axis I Disorders (SCID), the ACDS v1.2 to evaluate for DSM-5 ADHD and the ASRS v1.1 Symptom Checklist expanded version to measure self-reported adult ADHD symptoms. Participants self-reported medical history, psychiatric history, and demographics. A subset of participants (n = 85) were administered the AISRS-expanded version as well. These recruitment and consent procedures were approved and a HIPAA waiver granted by the Institutional Review Board of NYU Langone School of Medicine.
The PCP sample
This sample was composed of adults (18–58, inclusive) who were screened at a PCP practice in the New York area associated with NYU Langone Medical Center for ADHD. Participants were invited to complete the ASRS v1.1 Screener in the PCP office to screen for adult ADHD. Those who screened negative for adult ADHD, yet endorsed at least one ASRS symptom, were invited for further assessment at a later time on the telephone (see Fig. 1 for a full description of the recruitment procedures and final number of participants from that study included in this assessment).
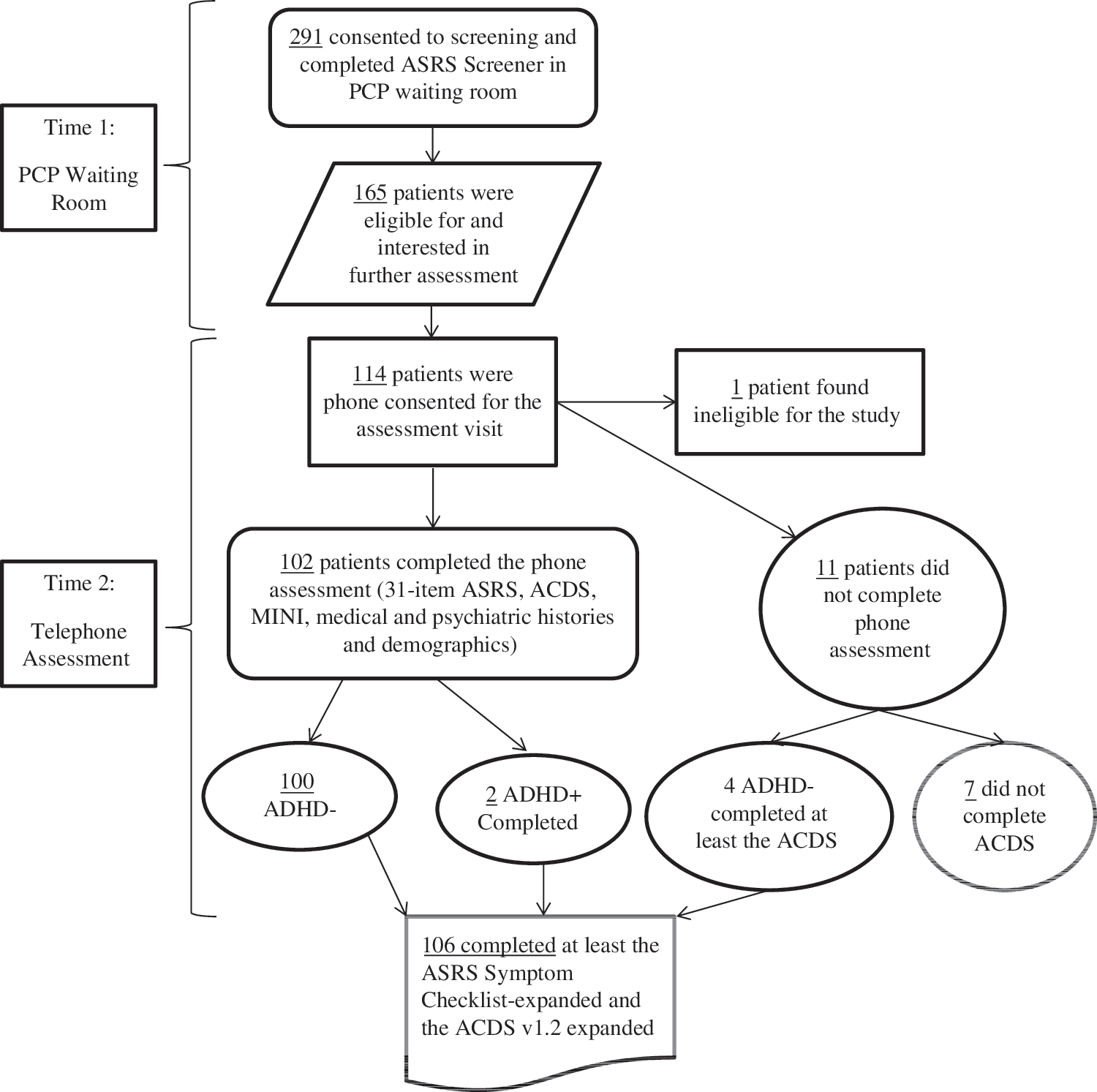
Flow diagram of PCP ADHD control subjects study recruitment. ADHD, attention-deficit/hyperactivity disorder; ASRS, Adult ADHD Self-Report Scale; PCP, primary care physician; ACDS, Adult ADHD Clinical Diagnostic Scale; MINI, Mini-International Neuropsychiatric Interview.
After the initial screening at the PCP practice, participants were contacted via phone by trained research staff between 0 and 21 days. Phone assessments included ASRS v1.1 Symptom Checklist expanded version, the Mini International Neuropsychiatric Interview 7.0 (MINI) to screen for DSM-5 psychiatric comorbidities, and the ACDS v1.2 to confirm lack of current DSM-5 adult ADHD diagnosis. Demographics, medical and psychiatric histories were also collected. Participants were compensated $45 for completing all assessments. The present analysis included 106 patients from the PCP sample, with 100 ADHD− and 2 ADHD+ subjects who completed all T1 and T2 assessments and 4 ADHD− subjects who did not complete all of the T2 assessments but completed at least the T2 ASRS and ACDS.
All recruitment and consent procedures for this sample were approved and a HIPAA waiver granted by the Institutional Review Board of NYU Langone School of Medicine. For the PCP sample, participants were also required to sign a release of protected health information allowing research staff to contact the participants' primary care doctor regarding any new diagnoses that arose during the clinical interview. Participants who refused to sign this form were excluded from the study.
Rating scales
To screen for adult ADHD in the waiting room (for the PCP sample) and to assess current ADHD symptoms (for both samples), the ASRS v1.1 6-item Screener version and the expanded Symptom Checklist, respectively, were used. The ASRS v1.1 was developed to ease identification of adult ADHD in primary care settings (Adler et al. 2012). The Screener was developed by extracting the six questions that psychometrically best predicted Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV; American Psychiatric Association, 1994) ADHD from the 18 item ASRS Symptom v1.1 Checklist, corresponding to the 18 DSM-IV/5 adult ADHD criteria (nine hyperactive [HI] and nine inattentive [IA]). The ASRS v1.1 has been shown to be a useful tool in identifying adult ADHD, with a positive predictive value of 0.94 and a negative predictive value 0.24 (Kessler et al. 2007). The Screener and the Symptom Checklist use a 5-point Likert scale to rate ADHD symptomatology (0 = Never, 1 = Rarely, 2 = Sometimes, 3 = Often, and 4 = Very Often). Depending on the item, “sometimes,” “often,” and “very often” suggests clinical impairment for that specific item. This self-administered scale has been translated into over 20 languages and has shown to have very good operating characteristics (e.g., sensitivity, specificity, total classification accuracy) in general population surveys both in the United States (Kessler et al. 2005, 2007, 2013) and internationally (Yeh et al. 2008; Zohar and Konfortes 2010; Kim et al. 2013). The ASRS Screener's relatively low negative predictive value is acceptable for the scale is designed to identify potential adult ADHD cases, and casts a wide net to prevent false negatives.
Adult ADHD was assessed in this study with version 1.2 of the ACDS (Adler and Cohen 2004; Adler et al. 2015), a semi-structured research diagnostic interview used in multiple studies of adult ADHD (Spencer et al. 1995, 1998, 2001; Fayyad et al. 2017). The interview begins with a retrospective assessment of all symptoms of childhood ADHD and then assessed an expanded set of recent (past year) symptoms including all DSM-5 Criterion A1 and A2 symptoms.
The ASRS, ACDS, and AISRS each have an expanded version that contains 13 non-DSM symptoms believed by the authors to be relevant to adult ADHD based on clinical experience and the research literature, including deficits in higher-level executive function (nine items) and emotional control (four items). These additional items were established by a steering committee of clinical experts in adult ADHD assembled by the World Health Organization (Kessler et al. 2005). They are similar to symptoms proposed in the Utah Criteria (Wender 1998), and were developed by examining other scales that measure ADHD non-DSM symptoms, including the Brown Attention Deficit Disorder Scale and the CAARS-Self-report: Long Version (Brown 1996; Conners et al. 1998). Specific prompts have been written to help guide the rater to explore the full manifestations of adult ADHD symptoms in an adult with ADHD for each of the ACDS and the AISRS items. All raters for the clinical assessment were trained per standard rater training procedures before initiation of trial (Adler et al. 2005).
The AISRS expanded version is described above. The prompts for the ACDS and the AISRS are the same, except that the AISRS was conducted asking for a retrospective reporting of the 2 weeks and the ACDS past year.
Psychiatric comorbidities were assessed using the SCID for the referred sample and the MINI for the PCP sample (Sheehan et al. 1998; First et al. 2002). The SCID, which in this study used to evaluate for Axis 1 psychiatric comorbidities, is a widely used clinical interview to measure psychiatric comorbidities and has been used for many adult ADHD studies [e.g., (Kessler et al. 2004; Adler et al. 2008)]. The MINI is a short structured clinical interview that can be used to evaluate for DSM-5 psychiatric comorbidities. It has been well-validated and is widely used to evaluate for psychiatric comorbidities in research studies, including ADHD studies (Spencer et al. 2006; Priebe et al. 2010; Yoshimasu et al. 2016).
While all evaluations for the referred sample were conducted in-person, most of the assessments for the PCP sample where conducted via telephone. PCP subjects were obtained by completing the ASRS v1.1 Screener in the PCP waiting room and then the full evaluation, including administration of the MINI, ACDS v1.2, and ASRS Symptom Checklist, was conducted on the phone. Each of these three scales has been validated for phone assessment (Adler and Cohen 2004; Cohen et al. 2006; Kessler et al. 2007; Gray et al. 2014). The referred sample interviews were administered by two clinical psychology trainees (a PhD candidate with an MA and an MA candidate with a BA) and the PCP sample interviews were administered by two coordinators with experience in adult ADHD (one with a BA and one with a BS). The clinical interviewers for both samples were trained by one of the investigators (L.A.A.). Validity of the referred sample interviews was established by regular direct observation of interviews. Calibration meetings were held between the coordinators to prevent rater drift and consistent ratings and validity of these interviews was established by meetings with one of the investigators (L.A.A.).
Data analysis
All statistical analyses were conducted using SPSS Version 22. Internal consistencies for the ASRS, AISRS, and ACDS were all calculated with Cronbach's alpha (α). For participants who only had an ACDS (n = 214) and did not have an AISRS, AISRS scores were extracted from the ACDS ratings. The AISRS and ACDS have the same prompts and same 4-point rating scale (“none/never,” “mild,” “moderate,” and “severe,” with the latter two being the threshold for clinical impairment for each item). Therefore, we did not require any transformations of the ACDS ratings to extract AISRS scores for each subject. To justify the AISRS score extraction, the relationship between the AISRS and ACDS scores for the 85 patients who had both clinician-administered tests was analyzed. Spearman correlations (Spearman's ρ) were calculated to examine the correlation between ACDS and AISRS 18-item, IA and HI total score ratings. Cohen's κ coefficients of agreement were calculated to examine item-by-item agreement on each of the 18 core DSM ADHD items for the two scales. To further examine possible influences using extracted scores, Poisson regression analysis was conducted (using the entire sample) with ASRS total score as the dependent variable, AISRS as the independent variable, and controlling for AISRS score being an actual AISRS or AISRS extracted from ACDS score.
The correlations between AISRS and ACDS scores were high and significant for the total 18 ADHD item score, as well as IA and HI scores (all Spearman ρ’s = 0.88, ps < 0.001). Additionally, item-by-item inter-rater agreement between the AISRS and ACDS items were all high and significant for all 18 ADHD items (Cohen's κ coefficients between 0.83 and 0.92, ps < 0.001; Table 2). The Poisson regression analysis examining the association between the ASRS and the ACDS/AISRS remained significant when adjusting for the fact that some people were administered the ACDS and some the AISRS, p < 0.001. These findings consistently support the strong relationship between AISRS and ACDS ratings and the validity of using ACDS ratings in place of AISRS ratings when AISRS ratings were not present for some subjects. Although the patients who received only ACDS assessment and not an AISRS assessment were somewhat, but significantly older than those who received an AISRS, t(177) = 2.50, p = 0.013, the composition of the samples were marginally different with regards to gender, χ 2 (1) = 3.44, p = 0.064, and did not significantly differ by race, χ 2 (4) = 6.95, p = 0.139, or Latino status, χ 2 (1) = 0.07, p = 0.795. Therefore, all subsequent discussion of AISRS data will refer to the combination of the AISRS scores obtained from the actual scale and the extracted scores from the ACDS.
Organized by ACDS/AISRS order.
All ps < 0.001.
ADHD, attention-deficit/hyperactivity disorder; ACDS, Adult ADHD Clinical Diagnostic Scale; AISRS, Adult ADHD Investigator Symptom Rating Scale.
Spearman correlations (Spearman's ρ) were calculated to examine relationship between ASRS and AISRS scores. Since the ASRS is rated on a 5-point Likert scale and the AISRS and ACDS are rated on 4-point Likert scale, for all of the analyses, never and rarely were combined and treated as one rating, as has been previously done in a similar analysis examining ASRS-clinician rated agreement (Adler et al. 2012). This relationship was further examined by stratifying the sample by a variety of demographic factors, past major depressive disorder (MDD) and current generalized anxiety disorder (GAD). We specifically examined MDD and GAD due to the higher prevalence rates for these comorbidities in adults with ADHD and because MINI does not capture past GAD (Kessler et al. 2006; Schatz and Rostain 2006). As the referred sample was a convenience sample, we did not collect overall prevalence rates for any DSM diagnosis. Cohen's κ coefficients of agreement were calculated to examine item-by-item agreement between each of the 31 ASRS v1.1 and AISRS items.
All tests were two-tailed and used a significance level of p < 0.05, unless indicated.
Results
Demographic characteristics of the samples
Data from 299 subjects were analyzed for this study. The mean age of the total sample was 32.0 ± standard deviation 10.5 years; 44.5% (n = 133) male and 55.5% (n = 166) female. Seventy-one percent of the total sample self-identified as Caucasian, 13.4% as African American, 10.7% as Asian, .3% as Native Hawaiian/Pacific Islander, and 4.7% unknown/other. Approximately 13.4% of the participants self-identified as Hispanic. Pearson χ 2 tests demonstrated that the composition of the samples did not differ by race, χ 2 (4) = 3.90, p = 0.42, or Latino status, χ 2 (1) = 0.44, p = 0.51. There were significantly more women in the PCP sample compared to the referred sample, χ 2 (1) = 6.10, p = 0.01. See Table 3 for a full presentation of demographics, organized by recruitment site and ADHD status.
ADHD, attention-deficit/hyperactivity disorder; PCP, primary care physician; IA, ADHD, predominately inattentive type; HI, attention-deficit/hyperactivity disorder, predominantly hyperactive-impulsive type; Comb, attention-deficit/hyperactivity disorder, combined type; ADHD, OTH/UNS, ADHD, other or unspecified type; SD, standard deviation; GAD, generalized anxiety disorder; MDD, major depressive disorder.
Internal consistency
Internal consistency of the ASRS v1.1 and AISRS items were all high. The Cronbach's α for the ASRS-v1.1 was 0.95 for the core 18 ADHD items and individual subscale coefficients ranged from 0.84 to 0.94. Cronbach's α for the AISRS was 0.97 for the core 18 ADHD items and individual subscales α ranged from 0.85 to 0.96.
Concurrent validity
The correlations between the ASRS v1.1 and AISRS were all high and significant (Spearman's ρ’s between 0.79 and 0.90, ps < 0.01; Table 4). This correlation remained significant when stratifying the sample by mean age (greater vs. lesser than mean age), gender, race and ethnicity, past MDD, and current GAD (all ps < 0.01, except for “other” race p < 0.05). The item-by-item analysis between the scales found moderate agreement for all individual items (% agreement: 46.1%–64.9%) and statistically significant κ coefficients (all ps < 0.001; Table 5).
All ps < 0.01.
Presented in ASRS v1.1 Symptom Checklist order, see Table 1 for corresponding items.
All ps < 0.001.
ADHD, attention-deficit/hyperactivity disorder; ASRS, Adult ADHD Self-Report Scale.
Discussion
Our analyses of self and clinician reports of adult ADHD symptoms in two samples, those from a primary care population and those referred to an adult ADHD clinic, show high agreement between self-reported symptoms on the ASRS v1.1 and clinician elicited symptoms from the AISRS. This was true for total scores and for individual items. These results support the utility of self-ratings in busy clinician settings such as PCP practices. Both samples included ADHD positive and ADHD negative adults as diagnosed via the ACDS v1.2. The ASRS and AISRS assessments were each found to be internally consistent with Cronbach αs ranging between 0.84 and 0.97, replicating earlier findings (Kessler et al. 2007; Adler et al. 2010). Furthermore, there were high and significant correlations between the ASRS and AISRS, which remained significant when controlling for age, gender, race, ethnicity, and major comorbid psychiatric diseases.
The analyses here also show that each of the subscales of the ASRS and AISRS had high and significant agreement with each other, although the original 18 symptoms in the DSM-5 subscales showed similar consistency with the executive dysfunction subscale (Spearman ρ of 0.89–0.90), while the emotional dyscontrol subscale showed a lower correlation (ρ of 0.79). Previous studies looking at emotional dyscontrol have had trouble clarifying its role as a possible core symptom of ADHD, possibly due to the wide range of definitions used for this construct. In contrast, behavioral measures of executive dysfunction have been consistently found to be highly correlated with the original 18 symptoms in the DSM (Brown 2006; Barkley and Murphy 2010; Kessler et al. 2010; Adler et al. 2014, 2017). Psychometric assessments of executive dysfunction are less well correlated with ADHD symptoms possibly due to the intrusion of state effects during assessments (Biederman et al. 2008).
The findings of high correlation between self versus clinician ratings but only moderate item-by-item agreement mirror that which has been found in the depression literature (Svanborg and Asberg 2001; Bernstein et al. 2007). Rush et al. (2006) found high correlations between a self and clinician rated depression total scores, but only moderate item-by-item agreement. While some depression scale researchers have explained this trend may be due to different scale constructs (Cuijpers et al. 2010), different scale content, or a variety of different causes, since the ASRS and AISRS are the same scale constructs, the moderate ASRS–AISRS item-by-item agreement may be due to external factors such as clinician and/or patient bias, limited insight, or psychiatric comorbidities. Future studies ASRS–AISRS agreement should attempt to tease out the nature of the moderate item-by-item agreement, which may improve our ability to more accurately measure adult ADHD symptomology.
Limitations of our study include significantly higher prevalence of female subjects in the primary care population than the referred sample. A further limitation is that while our data support the utility of self-report scales in busy practices, only approximately a third of the sample (but nevertheless substantial amount of participants) was recruited from a PCP setting. Limitation was the large number of subjects who did not complete the AISRS, but only completed the ACDS. Nonetheless, we found very high agreement between similar symptoms on the AISRS and ACDS, ranging from 0.82 to 0.93. This is not surprising, considering the prompts from the AISRS are identical to those employed in the ACDS, except with a differing time frame of 2 weeks versus 1 year; this differing time frame did not have a significant effect on the results. Another limitation is the comparison of frequency based ratings in the ASRS Symptom Checklist and severity based ratings in the AISRS; the use of frequency based ratings in patient reports was by design based on the belief that patients would be more reliable reporters of “how often” symptoms occur, as compared to evaluating the overall impact (severity) of their symptoms (Kessler et al. 2005). This supposition is why clinician based ratings are generally the gold standard in clinical trials (Adler et al. 2015).
Conclusions
We found high levels of agreement between clinician and patient ratings of ADHD symptoms, not only for IA/HI but also for symptoms of emotional dysfunction (EF) and emotional dyscontrol (EC), in a fairly large sample of referred adults and adults seen in a PCP practice. Extending these findings to the non-DSM, but associated symptoms of EF and EC is important given the recent findings of the high loading of EF symptoms, along with the differential loading of EC symptoms in adults with ADHD (Adler et al. 2017; Ustun et al. 2017). These results also highlight the potential utility of self-ratings in busy clinical settings where clinician ratings, which may require training or more extensive time of administration, may not be feasible.
Clinical Significance
Considering the high concordance between self and investigator ratings, primary care offices can utilize the ASRS as a self-assessment and for screening purposes before referral for further evaluation of ADHD by a psychiatrist.
Disclosures
M.J.S. and S.A. have no conflicts of interest to disclose.
In the past two years, Dr. L.A.A. received research support or was a consultant from the following sources: Sunovion Pharmaceuticals (Advisory Board, Consultant and Grant Support), Purdue Pharmaceuticals (Grant Support), Enzymotec (Advisory Board, Consultant and Grant Support), Shire Pharmaceuticals (Advisory Board, Consultant and Grant Support), Lundbeck (Grant Support), Alcobra (Advisory Board and Consultant), National Football League (Advisory Board and Consultant), Major League Baseball (Advisory Board and Consultant), Rhodes Pharmaceuticals (Advisory Board and Consultant), and NYU (Royalties).
Additionally, in the past five years, Dr. L.A.A. has received research funds from Purdue Pharmaceuticals, Theravance, and the Department of Veterans Affairs, and served as a consultant for Theravance, Neurovance and Novartis Bioventures.
In the past year, Dr. S.V.F. received income, potential income, travel expenses continuing education support, and/or research support from Lundbeck (advisory board, travel) Rhodes (consulting), Arbor (research grant) KenPharm (advisory board, travel), Ironshore (stock, consulting, advisory board, travel) Shire (research grant, advisory board, travel) Akili Interactive Labs (consulting, travel), Alcobra (advisory board, consulting fee, travel) VAYA (consulting) Sunovion (research grant), Neurovance (advisory board, travel), CogCube (advisory board, stock), NeurolifeSciences (advisory board), Neurovance (advisory board), and Genomind (consulting). With his institution, he has United States patent US20130217707 A1 for the use of sodium-hydrogen exchange inhibitors in the treatment of ADHD. In the previous 3 years, he received support from: Shire, Neurovance, Alcobra, Otsuka, CogCubed, McNeil, Janssen, Novartis, Pfizer, and Eli Lilly. Dr. S.V.F. receives royalties from books published by Guilford Press: Straight Talk about Your Child's Mental Health, Oxford University Press: Schizophrenia: The Facts and Elsevier: ADHD: Non-Pharmacologic Interventions. He is principal investigator of
Dr. S.V.F. does not stand to benefit from the material success of the ASRS. He does consult to companies that might have an interest in the ASRS so that could change his consulting opportunities. He currently has pending a grant request to Shire to fund an accredited Continuing Medical Education program about the ASRS. S.V.F., PhD served as statistical consultant for this study.
Dr. T.J.S. received research support or was a consultant from the following sources: Alcobra, Avekshan, Heptares, Impax, Ironshore, Lundbeck, Shire Laboratories, Inc., Sunovion, VayaPharma/Enzymotec, the FDA and the Department of Defense. Consultant fees are paid to the MGH Clinical Trials Network and not directly to Dr. T.J.S. Dr. T.J.S. has been on an advisory board for the pharmaceutical company Alcobra. Dr. T.J.S. received research support from Royalties and Licensing fees on copyrighted ADHD scales through MGH Corporate Sponsored Research and Licensing. Through MGH corporate licensing, Dr. T.J.S. has a United States Patent (#14/027,676) for a nonstimulant treatment for ADHD and a patent pending (#61/233,686) for a method to prevent stimulant abuse.
Dr. J.B. is currently receiving research support from the following sources: AACAP, The Department of Defense, Food and Drug Administration, Headspace, Lundbeck, Neurocentria, Inc., NIDA, PamLab, Pfizer, Shire Pharmaceuticals, Inc., Sunovion, and NIH.
Dr. J.B. has a financial interest in Avekshan LLC, a company that develops treatments for attention-deficit/hyperactivity disorder (ADHD). His interests were reviewed and are managed by Massachusetts General Hospital and Partners HealthCare in accordance with their conflict of interest policies.
Dr. J.B.'s program has received departmental royalties from a copyrighted rating scale used for ADHD diagnoses, paid by Ingenix, Prophase, Shire, Bracket Global, Sunovion, and Theravance; these royalties were paid to the Department of Psychiatry at MGH.
In 2017, Dr. J.B. is a consultant for Akili, Guidepoint, and Medgenics. He is on the scientific advisory board for Alcobra and Shire. He received honoraria from the MGH Psychiatry Academy for tuition-funded CME courses. Through MGH corporate licensing, he has a United States Patent (#14/027,676) for a nonstimulant treatment for ADHD, and a patent pending (#61/233,686) on a method to prevent stimulant abuse.
In 2016, Dr. J.B. received honoraria from the MGH Psychiatry Academy for tuition-funded CME courses, and from Alcobra and APSARD. He was on the scientific advisory board for Arbor Pharmaceuticals. He was a consultant for Akili and Medgenics. He received research support from Merck and SPRITES.
In 2015, Dr. J.B. received honoraria from the MGH Psychiatry Academy for tuition-funded CME courses, and from Avekshan. He received research support from Ironshore, Magceutics, Inc., and Vaya Pharma/Enzymotec.
In 2014, Dr. J.B. received honoraria from the MGH Psychiatry Academy for tuition-funded CME courses. He received research support from AACAP, Alcobra, Forest Research Institute, and Shire Pharmaceuticals, Inc.
In previous years, Dr. J.B. received research support, consultation fees, or speaker's fees for/from the following additional sources: Abbott, Alza, APSARD, AstraZeneca, Boston University, Bristol Myers Squibb, Cambridge University Press, Celltech, Cephalon, The Children's Hospital of Southwest Florida/Lee Memorial Health System, Cipher Pharmaceuticals, Inc., Eli Lilly and Co., Esai, ElMindA, Fundacion Areces (Spain), Forest, Fundación Dr. Manuel Camelo A.C., Glaxo, Gliatech, Hastings Center, Janssen, Juste Pharmaceutical Spain, McNeil, Medice Pharmaceuticals (Germany), Merck, MGH Psychiatry Academy, MMC Pediatric, NARSAD, NIDA, New River, NICHD, NIMH, Novartis, Noven, Neurosearch, Organon, Otsuka, Pfizer, Pharmacia, Phase V Communications, Physicians Academy, The Prechter Foundation, Quantia Communications, Reed Exhibitions, Shionogi Pharma, Inc., Shire, the Spanish Child Psychiatry Association, The Stanley Foundation, UCB Pharma, Inc., Veritas, and Wyeth.