
Abstract
Objective:
Sleep disturbance is often a problem for children with either autism spectrum disorder (ASD) or attention-deficit/hyperactivity disorder (ADHD). Psychostimulant medications used to treat ADHD symptoms can exacerbate this problem. For children with ASD and ADHD, atomoxetine (ATX) is a viable alternative to psychostimulants. We investigated the effects of ATX and a manualized parent training (PT) program targeting noncompliance, on the sleep quality of children with ASD and ADHD.
Methods:
Participants in a randomized clinical trial were treated with ATX + PT, ATX alone, PT alone, or placebo (PBO) alone, for 10 weeks. Fifty-four of 128 (42%) caregivers completed the Children's Sleep Habits Questionnaire (CSHQ) at baseline and endpoint. Analysis of covariance was used to investigate possible differences between treatment groups.
Results:
There were no significant differences between treatment groups, including PBO on the CSHQ 33-Item total score, total hours of sleep per day, and total minutes awake after sleep onset at the study endpoint.
Conclusion:
ATX appears sleep neutral. Clinicians who treat ADHD symptoms in children and adolescents with ASD may prefer ATX over psychostimulants when sleep disturbance is an issue.
Introduction
S
Stimulant medication is often prescribed for treating ADHD symptoms in individuals with ASD (Mandell et al. 2008; Coury et al. 2012), despite variable treatment effects and frequent side effects (Research Units on Pediatric Psychopharmacology 2005; Aman et al. 2008). One commonly reported side effect of psychostimulants is sleep disturbance. Although findings on stimulant use and sleep in children with ADHD have been mixed, a recent meta-analysis of randomized clinical trials (RCTs) examining sleep and stimulant use concluded overall that sleep is worse in children taking stimulant medication than placebo (PBO) (Kidwell et al. 2015).
Stimulant use was related to shorter sleep duration, longer sleep onset latency, and poorer sleep efficiency (Kidwell et al. 2015). Higher stimulant dose was also related to longer sleep onset latency, perhaps reflecting later daily dosing in children receiving multiple doses. These findings are of particular concern because sleep disturbances are already common in unmedicated children with either ADHD (Herman 2015) or ASD (Cortesi et al. 2010). As a result, prescribers often seek alternatives for treating ADHD symptoms.
In their review of eight RCTs, Garnock-Jones and Keating (2009) reported that children with ADHD who received atomoxetine (ATX) showed a smaller increase in sleep onset latency than those who received methylphenidate, indicating that ATX may be more tolerable for children and adolescents with ADHD who are often vulnerable to sleep disturbance. However, little information is available on the effects of ATX on sleep in children who have intellectual and developmental disabilities (IDD) such as ASD, along with ADHD. Aman et al. (2014) identified 11 studies using ATX to treat ADHD in children with iIDD. Sleep problems were reported as adverse events in three of nine open-label studies and in one of the two, double-blind PBO-controlled trials. Early morning awakenings were reported more often in the ATX group when compared with PBO (p = 0.027) (Harfterkamp et al. 2012).
Given the limited research in this area, there are lingering concerns about how ATX might impact sleep. The Children with Hyperactivity and Autism Research Treatment Study (CHARTS) examined the effects of ATX, administered either as a solo treatment or in combination with parent training (PT) in behavioral strategies, to reduce ADHD and behavioral noncompliance.
CHARTS was a RCT conducted with 128 youth with ASD, age 5–14 years, at three sites: the University of Pittsburgh Medical Center, the Ohio State University's Nisonger Center, and the University of Rochester Medical Center. Individually, both ATX and PT significantly improved ADHD symptoms, but when combined they were not significantly better than ATX alone. Also, ATX, both alone and combined with PT, significantly decreased behavioral noncompliance. Additionally, although ATX was associated with fatigue and decreased appetite, it was otherwise well tolerated (for more information see Silverman et al. 2014; Handen et al. 2016; Smith et al. 2016; Tumuluru et al. 2017).
Midway through the study, CHARTS added a standardized measure of sleep quality (Owen 2000). Using CHARTS data, our primary aim in the current report was to increase knowledge regarding the effects of ATX on patterns of sleep quality over time, in a sample of children and adolescents with ASD and ADHD. We tested whether ATX altered the quantity and quality of sleep over the 10-week RCT. We hypothesized that at study endpoint, the ATX group would show poorer sleep quality when compared with the PBO group. Also, although our PT program included little content related to improving sleep, it did focus on increasing the child's compliance in daily routines and as such might have affected sleep quality. Therefore, we hypothesized that PT could have a positive effect on bedtime resistance and our secondary aim was to examine the effects of PT on sleep quality.
Methods
The background, methods, and primary outcomes of CHARTS have been previously described (Silverman et al. 2014; Handen et al. 2016). Informed consent (parent/guardian permission) and assent were carried out with procedures and documents approved by the institutional review boards of the three sites.
Participants
Study participants were 5.0–14.11 years of age, male and female, and had a minimum mental age (MA) of 24 months based upon the Stanford-Binet 5th Edition (Roid 2003), or the Mullen Scales of Early Learning (Mullen 1989). They met criteria for an ASD (i.e., autistic disorder, Asperger's Disorder, Pervasive Developmental Disorder not otherwise specified [PDD-NOS]) based on clinical evaluation using the Diagnostic and Statistical Manual—Fourth Edition-TR (DSM-IV-TR) (American Psychiatric Association 2000), and confirmed by the Autism Diagnostic Interview—Revised (ADI-R) (Rutter et al. 2003). They also exhibited clinically significant symptoms of overactivity and/or inattention at both home and school, defined as a mean item score of ≥1.50 on the parent and teacher Swanson, Nolan, and Pelham (SNAP) scales (Bussing et al. 2008) and a Clinical Global Impressions-Severity score of ≥4 for ADHD (Guy 1976).
Participants were free of psychotropic medications (with the exception of those on stable doses of melatonin) for 2 weeks before study randomization. A child could be enrolled if he or she was taking a stable dose of anticonvulsant medication for seizures over the previous 6 months and had no seizure activity (one participant was taking seizure medication). Children were excluded if they had serious mental health concerns (e.g., schizophrenia or bipolar disorder), a major medical condition, clinically significant abnormal laboratory values or ECG results, prior treatment with an adequate trial of ATX (minimum of 4 weeks, with at least 1 week at ≥1.0 mg/kg) within the last 2 years, or prior PT.
Study design
CHARTS was a 10-week, parallel-group, randomized, multisite RCT. One hundred twenty-eight children and adolescents were randomized to one of four treatments (32/group). The four treatment arms were ATX + PT, ATX alone, PT + PBO, or PBO alone. Randomization was stratified by site in equal numbers to one of the four treatment conditions and balanced by MA (≤6 years vs. >6 years). ATX assignment was double blind, whereas PT assignment was single blind (i.e., coordinators, behavior therapists, and parents were aware of PT assignment), but the blind was maintained for all other study clinicians. Participants were assessed weekly to check for medication response, evaluate side effects, and make necessary dosing adjustments. The Children's Sleep Habits Questionnaire (CSHQ; Owens et al. 2000) was administered at the Baseline Visit and at week 10 to caregivers of the last 54 study participants, to accumulate more information about the effects of ATX on sleep.
Treatment
Atomoxetine
ATX doses were administered twice daily to reduce the possibility of side effects. The initial dose was 0.3 mg/(kg·d) (rounded to the nearest 5 mg) and increased weekly by 0.3 mg/(kg·d) to optimal improvement or limiting side effects. The target dose was 1.2 mg/(kg·d), but if necessary this could be increased to 1.8 mg/(kg·d).
Parent training
PT was conducted using a manualized program (Bearss et al. 2015), consisting of nine weekly sessions, lasting 60–90 minutes, with a behavior therapist. PT targeted behavioral noncompliance; it was not specifically directed toward sleep disturbance, with the exception of an optional module on strategies to improve sleep. Two participant parents identified a sleep problem as a top priority at baseline and were administered the sleep module.
Outcome measure
Children's Sleep Habits Questionnaire
The CSHQ (Owens et al. 2000) is a standardized questionnaire designed for use in children 4–12 years of age. The questionnaire includes 48 items and is rated retrospectively over the previous week by caregivers, to screen for common sleep problems. The Total Sleep Disturbance Score comprises 33 of the 48 items. The CSHQ incorporates items related to eight key sleep domains: (1) bedtime resistance (2) sleep onset latency, (3) sleep duration, (4) anxiety around sleep, (5) night awakenings, (6) disordered breathing during sleep, (7) parasomnias, and (8) morning waking/daytime sleepiness.
In addition, raters of the CSHQ are asked to report the total hours their child slept in a day and the total number of minutes that their child was awake after sleep onset (WASO). A total score of 41 or greater on the CSHQ 33 items has been recommended as the cutoff for identifying sleep problems in children (Owens et al. 2000; Johnson et al. 2016). The CSHQ was used as the primary outcome measure for the current report. We analyzed the sleep disturbance score based on the total of the CSHQ 33 items, total hours of sleep per day, and total WASO.
Statistical analyses
Since sleep measures were collected starting midway through the trial, baseline characteristics of participants with and without CSHQ data were compared using t-tests, and chi-square tests. Analysis of covariance was used to compare participant sleep parameters at 10 weeks across groups, adjusting for baseline levels (i.e., CSHQ 33-item total score, total number of hours of sleep per day, and total number of minutes WASO). Cohen's (1962) d was used to convey effect sizes for ATX versus PBO conditions.
Results
Sample characteristics
Of the 128 participants in CHARTS, caregivers of 54 study participants completed the CSHQ at both baseline and endpoint. The children had a mean age of 8.3 (+2.0) and mean IQ of 81.8 (+21.4). Table 1 summarizes baseline characteristics by treatment group. As shown in the table, the children were predominately white (69%), in regular education classes (54%), and with household incomes below $60,000 (59%). Seven (13%) participants were taking melatonin to help them sleep. Compared with participants without CSHQ scores, participants with CSHQ scores were significantly more likely to be female, had significantly lower ADHD symptoms (SNAP IV), and were more compliant behaviorally (Home Situations Questionnaire) (Table 2).
One-way ANOVA test showed a significant difference between treatment groups at baseline for mothers' age (p = 0.03).
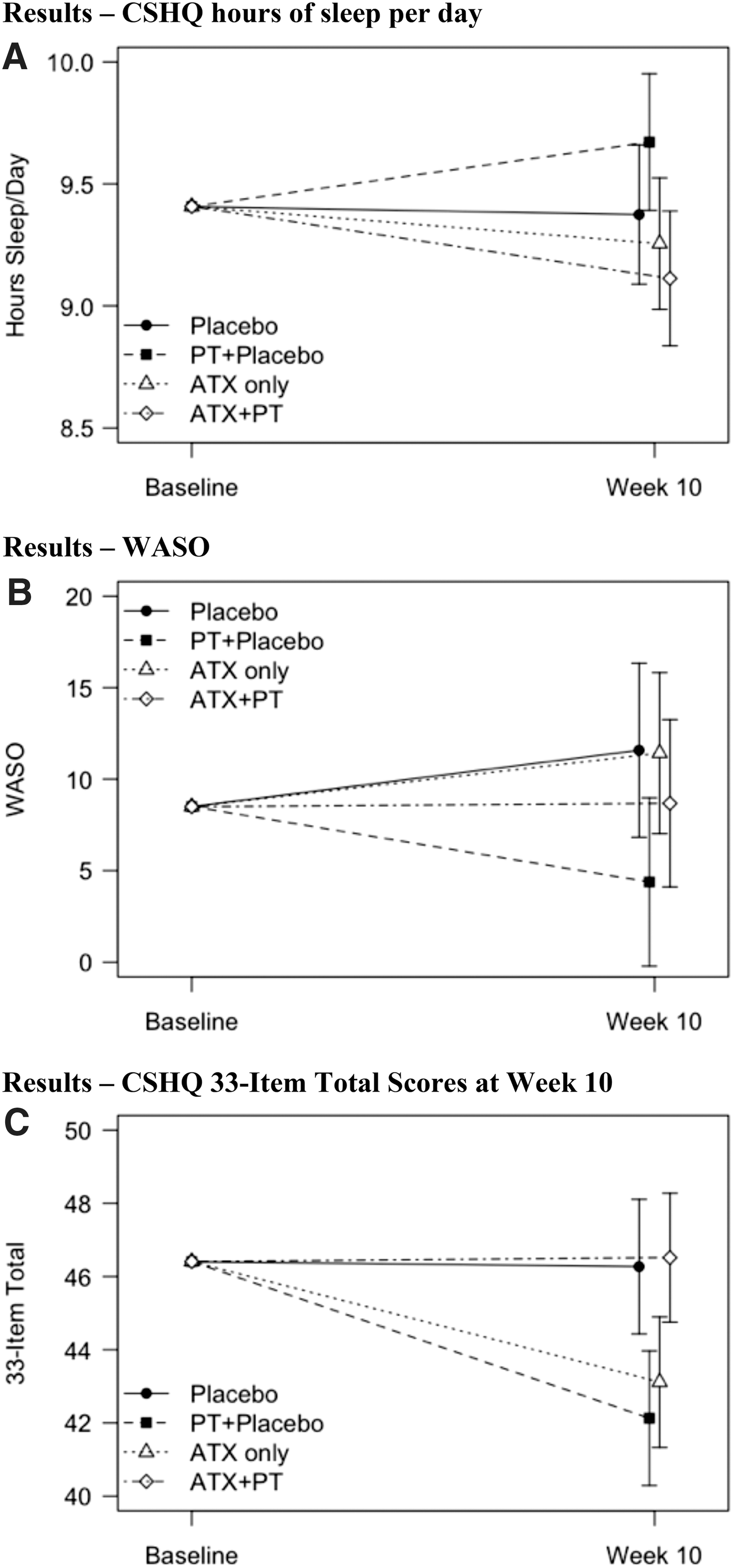
Week 10, CSHQ 33-Item Total Score (SD) for each treatment group were ATX + PT = 46.1 (10.1); ATX alone = 41.5 (6.9); PT alone = 43.2 (7.4); and PBO = 47.5 (8.7).
Sample characteristics reflect frequency counts and percent per treatment group.
ATX, atomoxetine; CSHQ, Children's Sleep Habits Questionnaire; HSQ, Home Situation Questionnaire; PBO, placebo; PT, parent training; SNAP, Swanson, Nolan, Pelham Scale.
Population mean and SD are 100 ± 15.
ADHD, attention-deficit/hyperactivity disorder; CSHQ, Children's Sleep Habits Questionnaire; HSQ, Home Situations Questionnaire; PDD-NOS, pervasive developmental disorder–not otherwise specified; SD, standard deviation; SNAP, Swanson, Nolan, Pelham Scale.
After controlling for baseline sleep quality, neither ATX, nor PT, nor their combination, was significantly associated with effects on either week 10 hours of sleep per day (p = 0.55, d = 0.3) or week 10 minutes awake after sleep (p = 0.66, d = 0.07) (Fig. 1A, B). The interaction of ATX by PT was significant in the model for week 10 CSHQ 33-item total scores (p = 0.04), but neither the main effect of ATX nor of PT were significant compared with PBO and no-PT, respectively (p > 0.7 for both). As shown in Figure 1C, CSHQ 33-Item total scores were lower at 10 weeks for participants in the PT-only group and the ATX-only group compared with participants in the PBO and the ATX + PT groups. Thus, if we collapse across PT conditions (PT included/PT not included) and across ATX conditions (ATX vs. PBO), then the net effect for PBO and ATX is the appearance of two essentially parallel lines, indicating no effect of drug condition.
Least squares mean ± standard error from ANCOVA models adjusting for baseline for
Discussion
Because ATX may be useful for children and youth with ADHD who are prone to sleep disturbance (Garnock-Jones and Keating 2009), we wanted to know if this would hold for children and adolescents with ASD and ADHD.
We found that all of the main effects for drug (ATX) and for PT were nonsignificant, suggesting little direct effect of either treatment. As noted earlier, one interaction (for CSHQ 33-item total) was significant. However, there is no a priori reason to hypothesize any interaction between drug and PT conditions, and if we correct for multiplicity by the Bonferroni method (0.05/3 = 0.017), the sole “significant” interaction effect is no longer significant. Considering that power could be an issue due to our small sample size and the possibility of type 2 error, we calculated effect sizes for each outcome variable: (a) total hours of sleep per day, (b) WASO, and (c) CSHQ total of the 33 items (d = 0.30, d = 0.15, d = 0.08), respectively.
In their meta-analysis, Kidwell et al. (2015), found a moderate and significant effect for stimulant medication on total sleep time in children and adolescents with ADHD (d = −0.59), who had been involved in seven RCTs (N = 223). The results indicated that stimulant medication was significantly associated with shorter sleep time. We found that the individuals randomized to ATX also had a shorter total sleep time compared with those who received PBO (i.e., ∼20 minutes shorter, d = 0.3), but the difference in total hours of sleep was not significant.
In terms of total sleep time, the stimulant effect was medium, whereas the ATX effect was small. This could have been due to the small sample size and a lack of power. But it could also be that ATX is an adequate alternative to stimulant medications for treating ASD and ADHD, especially in the presence of sleep disturbance. In the Harfterkamp et al. (2012) RCT, the investigators found no significant difference between the ATX group and control group on parent-reported insomnia. However, there was a significant increase in early morning awakenings, which reportedly decreased after 12 weeks of open-label treatment (Harfterkamp et al. 2012, 2013). In spite of this, both the CHART study and the Harfterkamp RCT found that ATX was generally well tolerated (Handen et al. 2016; Harfterkamp et al. 2012; Tumuluru et al. 2017) and acceptable to participant families (Hollway et al. 2016).
It has been shown that PT programs developed to target sleep disturbance may be efficacious (Johnson et al. 2014; Knight and Johnson 2014). However, the PT in this study was focused on improving behavioral noncompliance and contained only one optional module targeting sleep behavior. This module was requested by only two families, so it is not surprising that PT did not have a significant effect on sleep variables.
Limitations
Because the CSHQ was introduced late in the CHARTS trial, only 54 of 128 participants had baseline and endpoint CSHQ data. Data showed differences in ADHD and noncompliance severity ratings between children with and without CSHQ data. These differences likely arose because, part way through the study, in consultation with the Data Safety and Monitoring Board, we broadened enrollment to include children with ADHD Primarily Inattentive Type (rather than ADHD combined type). Other limitations include: (a) the use of the parent-rated CSHQ, a subjective index of sleep (e.g., actigraphs may have increased the validity or our results); (b) our small sample size (i.e., 54 of 128 participants [42%]), which likely undermined statistical power; and (c) supplementation with melatonin at stable doses for 13% of participants, probably influencing some CSHQ scores.
Future research
Psychopharmacological alternatives for treating ADHD symptoms in children with ASD are available. For example, a recent study of 62 children and adolescents ages 5–14 years with ASD and ADHD showed that extended-release guanfacine (XR) may also be effective for treating ADHD symptoms with minimal effects on sleep (Scahill et al. 2015). A possible future study would be to compare ATX, guanfacine (XR), and PBO, in a three-armed parallel group design to determine, which is more effective and with the fewest side effects (e.g., sleep problems, etc.).
Conclusion
The effect of ATX on hours of sleep was small and not significant, in comparison to a medium and significant effect of stimulant. We found no significant changes due to ATX or PT from baseline to endpoint on measures of sleep quality (i.e., sleep quality neither improved nor worsened). Clinicians who wish to treat ADHD symptoms effectively in children and adolescents with ASD may opt to use ATX rather than psychostimulants in patients who present with insomnia or who later develop insomnia with stimulant treatment.
Clinical Significance
The results of this study are helpful for informing clinical practice, since sleep disturbance is common in both ASD and ADHD and may exacerbate daytime behavior problems (Liu et al. 2006; Hollway and Aman 2011). When determining a treatment regimen for children with ASD and ADHD, it would be prudent for clinicians to assess sleep disturbance before treatment. The presence of sleep disturbance may be a clinical indicator for considering ATX as a potential alternative to stimulant medications.
Footnotes
Acknowledgments
The authors gratefully acknowledge the guidance and supervision of the DSMB, consisting of Edwin H. Cook, Jr., MD (University of Illinois at Chicago), Walter J. Meyer, MD (University of Texas-Galveston), Carson R. Reider, PhD (Ohio State University), and Wesley K. Thompson, PhD (University of California-San Diego).
Disclosures
Dr. Hollway has received research funding from Forest Research Institute, Sunovion Pharmaceuticals, Supernus Pharmaceuticals, Young Living, F. Hoffman-La Roche AG, Bracket Global LLC, Autism Speaks, and NIH. Dr. Aman has received research contracts, consulted with, served on advisory boards, or done investigator training for AMO Pharma Ltd., Bracket Global, CogState, Inc., Confluence Pharmaceuticals, CogState Clinical Trials Ltd., Coronado Biosciences, Forest Research, Hoffman-La Roche, Johnson & Johnson, Lumos Pharma, MedAvante, Inc., Ovid Therapeutics, ProPhase LLC, and Supernus Pharmaceuticals. Dr. Arnold has received research funding from Curemark, Forest, Lilly, Neuropharm, Novartis, Noven, Shire, Supernus, and YoungLiving (as well as NIH and Autism Speaks); has consulted with Gowlings, Neuropharm, Organon, Pfizer, Sigma Tau, Shire, Tris Pharma, and Waypoint; been on advisory boards for Arbor, Ironshore, Novartis, Noven, Otsuka, Pfizer, Roche, Seaside Therapeutics, Sigma Tau, and Shire; and received travel support from Noven. Dr. Williams has been an investigator for studies funded by Shire Pharmaceuticals, Forest Research Institute, Young Living, Supernus Pharmaceuticals, Autism Speaks, and NIH. Dr. Handen has received research funding from Hoffman-La Roche, Curemark, Eli Lily Pharmaceuticals, Autism Speaks, NIH, and NICHD. The Drs. Marrisa Mendoza-Burcham, Rebecca Andridge, Luc Lecavalier, Laura Silverman, and Tristram Smith, have nothing to disclose.