
Abstract
Objectives:
Psychotropic drugs are prescribed to people with autism spectrum disorder (ASD) usually as a means to alleviate comorbidities associated with the disorder. However, despite the uncertainty regarding the efficacy of these treatments for ASD, their prevalence is continuously increasing. The goal of this study was to understand the characteristics associated with drug prescription and compliance among young children with ASD.
Materials and Methods:
We studied patterns of drug utilization in a population-based sample of 211 young children with ASD in Southern Israel. Data regarding drug prescription and compliance (percentage of purchased drugs out of total prescriptions) were acquired from the electronic records of these patients. Compliance rates (CRs) were calculated as percentage of purchased drugs of the total number of prescriptions.
Results:
A total of 122 prescriptions were made for 75 children in our sample. Drug prescription was significantly associated with the severity of ASD and the types of comorbidity (p < 0.05). Atypical antipsychotic drugs were the most prevalent drugs (49 children; 23.2%), followed by stimulants (28 children; 13.2%) and first-generation antipsychotic drugs (16 children; 7.6%). The average CR in our sample was 75% ± 3% with about half of the children demonstrating full compliance, and less than fifth of them not complying at all with their drug prescription. CR had a positively linear association with ASD severity at a marginal statistical significance of p = 0.06. No other variables were statistically associated with drug compliance in our study.
Conclusions:
Our results highlight the significant effect of ASD severity on both the prescription and CRs of drugs among young children with ASD. Further examination of drug utilization for longer periods and larger samples will help confirming our findings and test the effects of other variables on these pharmaceutical parameters.
Introduction
A
Despite the uncertainty regarding the efficacy of psychopharmacological treatments for ASD, their use is increasing (Aman et al. 2005; Frazier et al. 2011). Several studies have examined characteristics associated with medical drug utilization among people with ASD (Mire et al. 2014; Schubart et al. 2014; Madden et al. 2016), but these studies largely focused on the prescription of such drugs and provided limited data on the factors associated with the compliance with these prescriptions. Hence, we studied the sociodemographic and clinical characteristics of young children diagnosed with ASD in Southern Israel and evaluated the potential effects of these characteristics on the prescription of drugs and the compliance rates (CRs) among these children.
Materials and Methods
Population
The population of Southern Israel (the Negev) includes ∼700,000 citizens, of which ∼60% are Jewish and ∼40% are Bedouin Arabs—two ethnic groups that differ in both their genetic background and culture. About 75% of this population are members of Clalit Health Services and receive their medical services at the Soroka University Medical Center (SUMC), which is the only tertiary hospital in the region. A total of 318 children between the ages of 1 to 6 years were referred to the Preschool Psychiatric Unit (PPU) at SUMC between the years 2006 and 2013. All these children underwent a rigorous clinical assessment, which included a comprehensive intake interview regarding the clinical and sociodemographic background of the diagnosed child and an examination by a child psychiatrist who provided a diagnosis of autism, pervasive developmental disorder not otherwise specified (PDD-NOS), or Asperger according to Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) criteria (American Psychiatric Association 2000). Children with suspected intellectual disability (ID) underwent a cognitive evaluation by a trained developmental psychologist. Consequently, children with an IQ <70 were determined as having ID. For the purpose of this study, the diagnoses of these children were reevaluated by the same child psychiatrist according to the new Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-V) criteria (American Psychiatric Association 2013). A level of ASD severity was assigned to each child in our sample according to the following DSM-V guidelines: (1) “Mild”—requiring support; (2) “Moderate”—requiring substantial support; and (3) “Severe”—requiring very substantial support. This study was approved by the Research Ethics Committee responsible for human studies at SUMC.
Data collection
Clinical and sociodemographic data on the individuals in our sample were retrieved from the PPU health records by using the Clicks® software, which is a clinic-based system linked to a clinic-resident management application, which enables medical staff to access their respective application or designated dataset. Data on drug prescription and purchasing frequency were retrieved from the OFEK system (Nirel et al. 2011), which is an online information system that contains electronic medical records from all health service providers in Israel (hospitals, clinics, drugstores, medical laboratories, etc.). Drugs were classified into four categories: (1) atypical antipsychotic (AA) drugs (i.e., Risperidone and Olanzapine); (2) first-generation antipsychotic (FGA) drugs (i.e., Haloperidol, Clotiapine, Neuleptil Chlorpromazine, and Perphenazine); (3) stimulants (ST) (i.e., Adderall and atomoxetine); and (4) sleep/tranquilizer (TRQ) (i.e., Melatonin, Promethazine, Clonazepam, and Triclonam elixir).
Compliance rates
The CRs for each patient i and each drug j were calculated as the sum of compliance of all drugs per patient or the sum of compliance of all patients per drugs as follow:
where m is the total number of prescribed drugs per patient, n is the total number of patients per drug, and Cij is the compliance of a patient (i) with a prescribed drug (j) according to the following scales:
0—A recommendation was made by a psychiatrist, but the drug was not purchased.
1—The drug was purchased inconsistently for only part of the prescribed period.
2—The drug was purchased consistently for the full period of the prescription.
We assumed that patients who bought the drugs also used them according to the physician's recommendation. Finally, we classified the CR to one of three categories: 0%–49%—no compliance; 50%–74%—partial compliance; and 75%–100%—full compliance.
Statistical analyses
We compared selected parameters between groups of patients divided according to patterns of drug prescription and drug compliance by using an independent t-test or a one-way ANOVA for continuous variables and chi-square or Fisher's exact tests for nominal variables. We used an unconditional logistic regression to assess the effect of multiple variables on drug prescription. All p values were two sided and statistical significance was defined as p < 0.05. Statistical analyses were conducted with SPSS 17th edition (SPSS, Inc., Chicago, IL).
Results
Population characteristics
Of the 318 children who were referred to the PPU with suspected social communication difficulties between the years 2006 and 2013, 235 children (73.9%) received a positive diagnosis of ASD. Of these, two children who were neither Jewish nor Bedouin, and 22 children who were not under medical surveillance at the PPU, were excluded from the study. Consequently, 211 children with ASD were included in this study (Table 1).
Significance level of bold values is: p < 0.05.
Comparison between children with (yes) and without (no) drug prescription.
Association with the number of prescribed drugs.
Prevalence of drug prescription
The associations between basic demographic and clinical characteristics and the prescription of drugs among the children with ASD in our sample are depicted in Table 1. A total of 122 prescriptions were made for 75 children in our sample. The majority of these children (50 children; 66.7%) received a prescription for only one type of drug, while six children (8.0%) received a prescription for three or more drugs. Drug prescription was more prevalent among Bedouin than among Jewish children (46% vs. 31%; p = 0.036). However, no significant differences were observed in the number of prescribed drugs between these two ethnic groups. Drug prescription was not associated with age at diagnosis, age of first prescribed drug, or gender of the children in our sample.
Notably, drug prescription was significantly associated with ASD severity, such that children with “moderate and severe ASD” were 7 times and 15 times (respectively) more likely to have a prescription of drugs than children with “mild ASD” (odds ratio [OR] = 7.11, confidence interval [95% CI] = 1.99–25.44, and OR = 15.01, 95% CI = 42.00–53.64, respectively). ASD severity was also positively correlated with the number of drugs prescribed (Spearman's r = 0.34; p < 0.001).
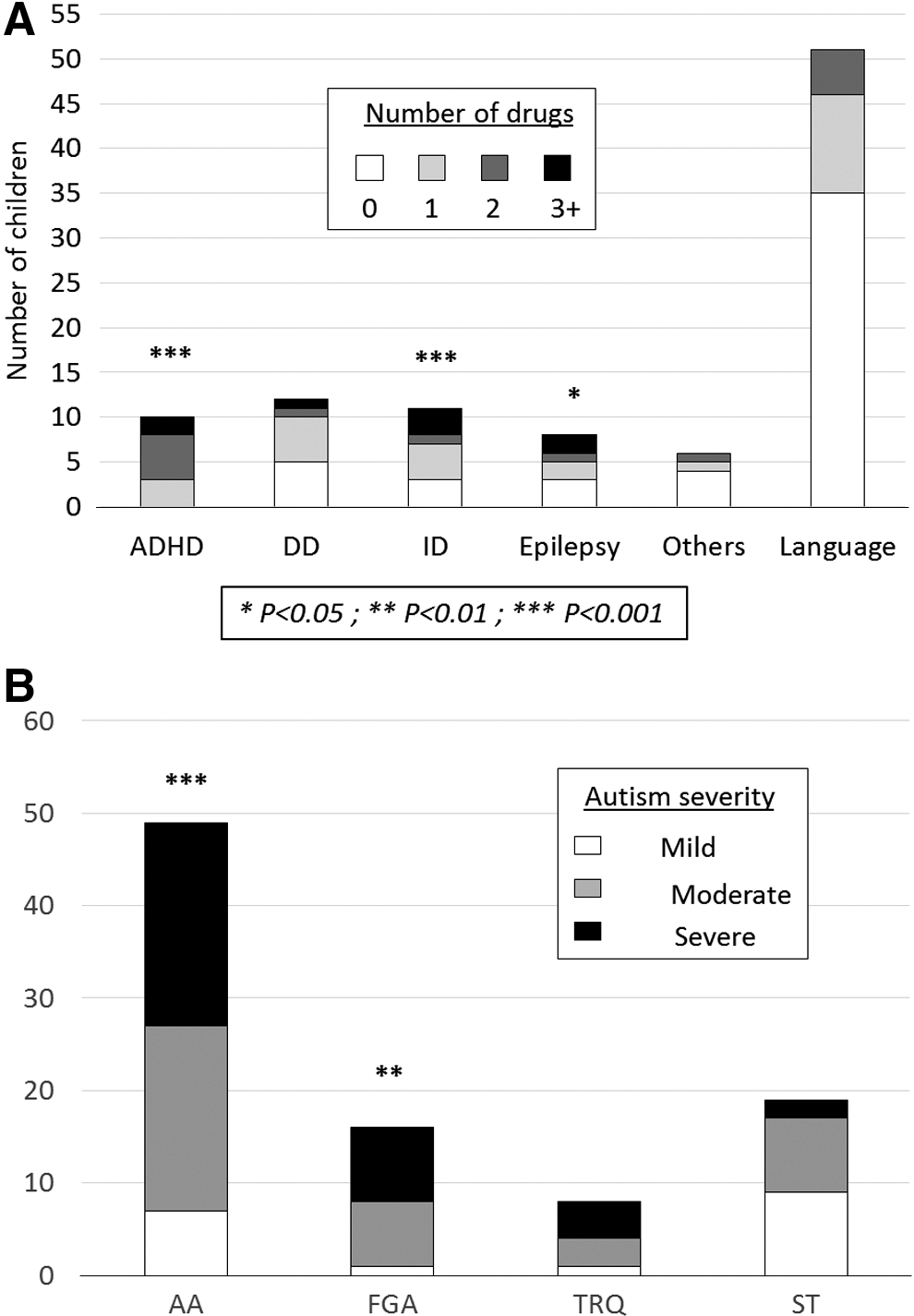
As expected, drug prescription was also associated with the types of ASD comorbidity (Fig. 1A). Specifically, children with ASD and attention-deficit/hyperactivity disorder (ADHD), ID, or epilepsy were prescribed more drugs than other children with ASD (Bonferroni corrected p < 0.05). Remarkable differences were also found in the prescription frequencies of different drugs (Fig. 1B). The most prevalent prescriptions in our sample were for AA drugs (49 children; 23.2%), followed by ST drugs (28 children; 13.3%), FGA drugs (16 children; 7.6%), and, finally, TRQ drugs (8 children; 3.8%). None of the children in our sample were prescribed with selective serotonin reuptake inhibitors (SSRIs) . Both AA and FGA drugs were significantly associated with more severe ASD (Bonferroni corrected p < 0.01; Fig. 1B).
Rate of drug prescription.
Finally, we run a multivariate logistic regression model with all the variables that were associated with drug prescription. Only ASD severity showed a statistically significant effect on drug prescription in that model (p < 0.01; Supplementary Table S1; Supplementary Data are available online at
Prescription compliance
Of the 75 children who received prescriptions in our sample, about half (34 children; 45.3%) fully complied with their prescribed drugs, whereas 14 children (18.7%) did not comply with their drug prescriptions (Table 2). Prescription compliance was not significantly associated with age at diagnosis, age of first prescribed drug, gender, or ethnic origin, although Bedouin children tend to show higher compliance with their prescriptions than Jewish children (Table 2). There was a marginally significant association between ASD severity and drug compliance (p = 0.06) where children with severe ASD demonstrated a higher compliance than children with moderate and mild ASD (Table 2). In addition, there were minor, but not statistically significant differences in CRs between children with different comorbidities (Fig. 2A). Finally, high CRs were observed for all drugs in our study; TRQ drugs showed the highest CR (85.7%), followed by FGA drugs (78.1%), ST drugs (76.0%), and, finally, AA drugs (74.4%) (Fig. 2B).

Rate of drug compliance.
Kruskal–Wallis test.
Chi-square test for linearity.
Discussion
ASD is a lifelong, pervasive neurodevelopmental disorder that currently has no cure. Prescriptions of psychotropic drugs for people with ASD are mainly directed to treat specific comorbidities in these people (Gerhard et al. 2009). In our study, we evaluated the rates of prescription and compliance of psychotropic drugs among a sample of children with ASD and assessed the effect of various characteristics of the children on these rates. The prevalence of drug prescription among children with ASD in our sample (35.5%) was slightly lower than the reported 40% or more in other studies (Mire et al. 2014; Lake et al. 2015; Jobski et al. 2017; Madden et al. 2016). This discrepancy can be explained by the relatively young age of children in our sample and the known effect of age on drug prescription in children with ASD (Madden et al. 2016). The highest rate of prescription in our sample was for AA drugs, followed by ST drugs. These types of drug are also the two most frequently prescribed drugs reported in most studies of children with ASD (Jobski et al. 2017; Park et al. 2016).
In our sample, drug prescription was significantly associated with ASD severity. This association is not surprising, as families of children with more severe ASD are more likely to use health services and seek treatments that will help the children cope with symptoms of the disorder. In addition, ASD severity is also affected by the number and severity of associated comorbidities in these children (Adams et al. 2013; Tureck et al. 2015). Some of these comorbidities have effective treatments that likely help reduce the clinical burden for these children [e.g., melatonin to manage sleep disturbance (Leu et al. 2011; Rossignol and Frye 2011)]. The effectiveness of different drugs on specific symptoms among children with ASD is also reflected in our observation that children with certain comorbidities tend to be prescribed more drugs. Similar findings were found in a study in North America, where more than 80% of subjects with comorbid bipolar disorder, ADHD, obsessive-compulsive disorder (OCD), or anxiety disorder received drugs on a regular basis (Coury et al. 2012).
We found a higher prevalence of drug prescriptions among Bedouin children than among Jewish children. However, these ethnic differences are probably attributed to the differences in ASD severity between these two populations. Indeed, when we included both ethnic origin and ASD severity in the same logistic regression model, the effect of child ethnicity completely disappeared. The differences in ASD severity between Jewish and Bedouin children in our sample likely stem from underdiagnoses of children with milder forms of ASD in the Bedouin population (Raz et al. 2015; Mahajnah et al. 2015).
A unique aspect of our study was the monitoring of the compliance with the prescribed drugs in our sample. We observed remarkable differences in CRs, which were related to ethnicity, ASD severity, and comorbidities of children in our sample. However, none of these differences were statistically significant, possibly due to the relatively small size of our sample. Thus, studies with larger samples are required to determine the effect of these characteristics on compliance with prescription of drugs among children with ASD.
It is worth noting that the compliance for the different drug types in our sample ranged between 74.4% (AA) and 85.7% (TRQ). These rates are significantly higher than the CRs (40%–52%) reported in another study of children with ASD (Logan et al. 2014) than the typical CRs for drugs among people with other psychiatric conditions (Osterberg and Blaschke 2005). We will continue monitoring the compliance to drug prescriptions in our growing sample for longer periods to examine whether such high CR is a true characteristic of our sample.
Our study has several limitations, including the relatively small sample size, which limits the statistical power to find small effects and complicates the generalizability of the results. In addition, we did not have consent to contact the patients and their families and, therefore, we could not investigate the reasons underlying the various levels of compliance with the drug recommendation. In addition, we did not have information regarding nonpharmacological interventions in these children, which may have influenced both prescription and compliance with these drugs. Finally, CRs were based on drug purchase data assuming that continuous purchase of the drug indicates full compliance with it. However, we acknowledge that these assumptions do not always hold and a more accurate assessment of CR could be achieved through other approaches (e.g., monitoring of biological makers).
Conclusions
Our results highlight the significant effect of ASD severity on both the prescription and CRs of drugs that are used to alleviate symptoms of different comorbidities among young children with ASD. Further examination of variables associated with patterns of drug utilization for longer periods and of larger populations will help confirming our findings and test the effect of other variables on these medical parameters.
Clinical Significance
This is the first study to examine clinical and sociodemographic factors associated with drug utilization among young children with ASD in an ethnically diverse population. Findings indicate that severity of symptoms is the most important factor to affect both drug prescription and their compliance regardless of age, sex, and ethnic origin of these children. In addition, we saw that children with ADHD, ID, and epilepsy are more likely to get drug prescriptions than children with no such symptoms. However, no such differences were seen in the CRs of these children, which were relative high for all children and all prescribed drugs. High CRs for medications, as observed in our study, usually improve the effectiveness of these drugs. Thus, this is encouraging for both clinicians who prescribed these drugs and the children who use them.
Footnotes
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.