
Abstract
Objectives:
Numerous studies have suggested cognitive deficits as consistently associated with adolescent depression. No study to date, however, has assessed neurocognitive predictors of selective serotonin reuptake inhibitor (SSRI) treatment response in adolescents with depression. This study examined neurocognitive tasks at baseline as predictors of clinical improvement with SSRI treatment (fluoxetine) at week 6 and 12 in an adolescent population.
Methods:
Adolescents with depression were recruited from a child and adolescent psychiatry outpatient clinic at a university medical center. Twenty-four adolescents (mean age 14.8 years) with Major Depressive Disorder completed tasks of the Cambridge Neuropsychological Test Automated Battery, including visual memory, executive functioning, sustained attention, and impulsivity. Depression severity, measured by the Children's Depression Rating Scale-Revised (CDRS-R), was assessed at week 6 and 12 and clinical improvement was defined as percentage (%) change in CDRS-R from baseline.
Results:
Clinical improvement is noted at both week 6 (mean % change in CDRS-R [M] = 46.8, standard deviation [SD] = 51.9) and week 12 (M = 87.9, SD = 57.2). Results reveal that less difficulty in sustained attention (p = 0.02), lower impulsivity (p = 0.00), and better planning (p = 0.04) at baseline were predictors of greater clinical improvement at week 6. Lower impulsivity at baseline remained significantly predictive of clinical improvement at week 12 (p = 0.01).
Conclusion:
Neurocognitive assessments could potentially help identify a subset of depressed adolescents who may not respond to conventional SSRI treatment and who may be better candidates for alternative or augmentation treatments.
Introduction
M
Clinical guidelines warrant the use of psychotherapy, antidepressant medications, or both as first-line treatment for child and adolescent depression. Psychotherapeutic approaches have demonstrated significant effects in this age group and a more recent meta-analysis has shown robust effects for cognitive-behavioral therapy and interpersonal therapy with this population (Zhou et al. 2015). Nevertheless, while mild-to-moderate depression may respond to psychotherapy alone, more severe or chronic episodes generally require treatment with antidepressants, either alone or combined with psychotherapy (Brent and Maalouf 2009). Furthermore, antidepressants may be the only possible treatment modality whenever psychotherapy is unavailable or inadequate for the patient's condition (Birmaher et al. 2007).
Selective serotonin reuptake inhibitors (SSRIs), particularly fluoxetine, constitute the most studied class of antidepressant medications, especially in the adolescent age group (Cheung et al. 2005; Dolle and Schulte-Körne 2013). Across all randomized controlled trials conducted on SSRIs, depressed patients have demonstrated good response rates (40% to 70%), although placebo response rates were also high (30% to 60%). The resultant number needed to treat (NNT) to achieve response to SSRI is 10 (Brent and Maalouf 2009; Marazziti et al. 2010). For Fluoxetine specifically, response rate was noted at 59%, while the NNT was 4.69 (Gibbons et al. 2012). Overall, roughly 40% of depressed youth fail to show adequate response to treatment (Snyder 2013). There is therefore a need for novel strategies aimed at improving response rate in the treatment of this population. Such strategies should allow for the early identification of those individuals most likely to benefit from antidepressants and the matching of treatment to patient characteristics.
Several studies in the adult population suggest that neurocognitive measures can be used as markers for SSRI response in depression (McIntyre et al. 2013; Snyder 2013; Rock et al. 2014). A range of cognitive deficits has been described in adult patients who subsequently demonstrated poor clinical response to SSRI treatment. Impaired attention predicted increased relapse rate 6 months later in Fluoxetine responders (Majer et al. 2004). In a 12-week Fluoxetine trial, nonresponders had poorer pretreatment performance on Stroop color Naming, but performed similar to responders on the Wisconsin Card Sorting Test. Gorlyn et al. (2008) showed that SSRI responders outperformed nonresponders across all cognitive domains obtained at baseline with the largest differences observed in executive, language, and working memory functions. Better performance on psychomotor speed and word fluency tests was also a significant predictor of SSRI treatment response (Bruder et al. 2014). A recent meta-analysis demonstrated that poor planning and organization are predictive of low antidepressant treatment response in late-life depression (Pimontel et al. 2016).
Deficits in various cognitive functions have also been described in depressed children and adolescents (Maalouf et al. 2011; Wagner et al. 2015). Depressed children and adolescents have demonstrated slow reaction times as well as problems with accuracy and inhibition on complex attention tasks (Cataldo et al. 2005; Brooks et al. 2010). Depressed youths have also been significantly slower than controls when performing attention-switching tasks, working memory, and cognitive and motor speed tasks (Baune et al. 2014). They tend to engage in rumination, which was found to predict impairments in selective attention and attention-switching tasks (Connolly et al. 2014). In addition, adolescents with MDD have impaired decision making and those with higher depressive symptoms exhibited lower reaction time, suggesting faster reactivity to affective stimuli (Han et al. 2012; Sommerfeldt et al. 2016). Children with MDD performed worse than healthy controls on inhibition capacity, verbal fluency, sustained attention, verbal memory, and planning according to a recent meta-analysis (Wagner et al. 2015). In addition, slow processing speed in adolescents (Gale et al. 2015) along with difficulties in inhibition and shifting (Kertz et al. 2016) were predictive of depression in adulthood. Similarly, adolescents who made both total errors and nonperseverative errors on the Wisconsin Card Sorting Task were more likely to exhibit higher levels of anxiety symptoms 2 years later (Han et al. 2016). Depressed adolescents undergoing SSRI treatment exhibited persistent impulsivity, visual memory, and no improvement in executive functioning compared to healthy controls (Shehab et al. 2016). Poor executive function and impulsivity were also shown to be state markers of depression not present in remitted adolescents (Maalouf et al. 2011).
Although several studies have described different neurocognitive deficits in adolescent depression and changes in cognitive functioning during SSRI treatment, no studies have investigated what neurocognitive profile at baseline is associated with clinical improvement. This study aimed at identifying what pretreatment neurocognitive profile would predict clinical improvement in depressed adolescents treated with SSRI. Our previous work has shown that SSRI-treated depressed adolescents exhibit deficits in visual memory and sustained attention, and no improvement in executive functioning when compared to healthy controls (Shehab et al. 2016). Based on these findings and the literature on executive functioning in adult depression, we have opted to examine these cognitive tasks in adolescent depression and anticipate that less difficulty in sustained attention, lower impulsivity, and better planning and visual memory at baseline will be predictors of clinical improvement at both intervals. Due to ethical reasons as well as limitations within the clinical setting, we were not able to incorporate a control group of depressed adolescents not in treatment or a control group of depressed adolescents receiving psychotherapy only and limited this study to depressed adolescents receiving SSRI. Nevertheless, our study is the first to investigate neurocognitive predictors of clinical improvement in pediatric depression.
Methods
Study design and setting
The study protocol was approved by the Institutional Review Board of the American University of Beirut Medical Center (AUBMC). Participants were recruited from the child and adolescent psychiatry outpatient clinic at the AUBMC. This is a 12-week follow-up study of depressed adolescents treated with Fluoxetine.
Participants
A total of 24 adolescents aged 12 to 18 years, who had received a diagnosis of MDD according to the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSM-IV-TR) (American Psychiatric Association, 2000) criteria, were eligible to enroll in this study. Participants were recruited if they had a current diagnosis of MDD according to the Development and Well-Being Assessment (DAWBA) and a Children's Depression Rating Scale-Revised (CDRS-R) score above 40.
The exclusion criteria included the following: (1) prorated full scale IQ (obtained using two subscales, matrices and special span, of the four-subscale Wechsler Nonverbal Scale of Ability [WNV]) below 70, (2) psychotic symptoms, (3) substance abuse or dependence, (4) history of bipolar disorder, (5) history of untreated attention-deficit/hyperactivity disorder (ADHD), (6) history of head trauma and/or other neurological disease, (7) either biological parent with bipolar disorder, (8) having been on an antidepressant other than Fluoxetine over the past 2 weeks, and (9) having been on Fluoxetine over the past 6 weeks.
At baseline (Table 1), participants included 8 males (33.3%) and 16 females (66.7%). The average age of participants was 14.8 (SD = 1.6) with an average IQ of 92.7 (SD = 14.0).
ADHD, attention-deficit/hyperactivity disorder; CDRS-R, Child Depression Rating Scale-Revised; MDD, major depressive disorder; OCD, obsessive compulsive disorder; PTSD, post-traumatic stress disorder; SD, standard deviation; SSRI, selective serotonin reuptake inhibitor.
Drug administration
Participants were started on Fluoxetine according to the following protocol: Fluoxetine 20 mg with the option of increasing to 30 or 40 mg if there is no significant improvement (Table 1). Subjects received psychoeducation during their assessment session, but no formal form of psychotherapy (cognitive behavioral therapy or other) was provided. Fluoxetine was chosen because it is one of two medications that are approved by the United States Food and Drug Administration (FDA) for the treatment of depression in adolescents.
Assessment and outcome measures
Upon entering the study, participants were assessed using the DAWBA and CDRS-R. Neurocognitive tasks (see section Computerized neurocognitive tasks) in addition to the WNV were also administered at baseline. Follow-up sessions were scheduled 6 and 12 weeks after the first visit; the CDRS-R was repeated during each of those sessions. At week 6 and 12, 21 and 15 participants were reassessed, respectively. Demographic variables included age, gender, age of onset for depression, duration of current depression, and number of total depressive episodes.
Wechsler Nonverbal Scale of Ability
The WNV is a test of general cognitive ability for individuals between the ages of 4–21 years and 11 months (Wechsler and Naglieri 2006). It has good validity and reliability and may be used with different populations for the purposes of clinical assessments (Wechsler and Naglieri 2006). The brief version of the WNV was used in this study as a screening for nonverbal IQ, consisting of the two subtests, Matrices and Spatial Span, which produce a single ability score. Participants who scored below 80 were excluded from the study.
The Development and Well-Being Assessment
The DAWBA is a structured interview used to formulate psychiatric diagnoses of children/adolescents based on DSM-IV-TR criteria (Goodman et al. 2000). The DAWBA includes questions that inquire about psychiatric symptoms as well as the impact of those symptoms on the child's/adolescent's and his/her family's life. Diagnoses generated by the DAWBA include MDD and other depressive disorders, bipolar disorders, anxiety disorders, ADHD and other behavioral disorders, psychotic disorders, developmental disorders, and others. The DAWBA has excellent discriminant validity (Fleitlich-Bilyk and Goodman 2004) and has been adapted into various languages, and used in numerous epidemiological and clinical studies worldwide (Goodman et al. 2005). In this study, participants completed the online self-report Arabic version of the DAWBA. The Arabic DAWBA has shown good concurrent validity with clinician diagnoses in young children (Alyahri and Goodman 2006), and has demonstrated good diagnostic validity, sensitivity, and specificity in a child and adolescent clinical sample (Zeinoun et al. in review). All psychiatric diagnoses generated by the interview were confirmed by the first author.
The Children's Depression Rating Scale, Revised
The CDRS-R is a standardized semistructured interview administered by a trained professional and used for assessment of depression (Poznanski and Mokros 1996). The CDRS-R assesses 17 symptom areas, each rated on a scale of 1 to 5 or 1 to 7, adding up to an overall score ranging from 17 to 113 (Poznanski et al. 1984). While the interview focuses on the child as the primary informant, parents' or other caregivers' reports can be additionally incorporated into the rating for each item. Furthermore, three of the items are rated based on the interviewer's observations alone (Mayes et al. 2010). Overall scores of 40 or more are considered indicative of a diagnosis of depression. The CDRS-R has demonstrated strong internal consistency (α = 0.85) and good discriminant validity between depressed and nondepressed children and adolescents (Poznanski et al. 1984; Mayes et al. 2010). In this study, we use the Arabic version of the CDRS-R, which was translated by our team. The Arabic CDRS-R was found to have high internal consistency, Cronbach's α = 0.94. The outcome variables include the percentage change (% change) in CDRS-R scores from baseline to week 6 and percentage change in CDRS-R from baseline to week 12.
Computerized neurocognitive tasks
Neurocognitive functioning was assessed using tasks from the Cambridge Neuropsychological Tests Automated Battery (CANTAB). These tasks are appropriate for use in children and adolescents and have demonstrated adequate sensitivity to psychiatric disorders (Sahakian and Owen 1992; De Luca et al. 2003).
Delayed matching to sample
This task measures immediate and delayed visual memory using a four-choice simultaneous and delayed recognition memory paradigm. The primary outcome variable is the percentage of total correct responses. The subjects are shown a complex visual pattern (the sample) and then, after a brief delay, the sample disappears and four patterns are shown; the subjects are asked to identify the sample that disappeared.
Stockings of Cambridge
This task is a measure of planning and problem solving, and is suggestive of executive functioning. The primary outcome measures are the mean number of moves in the problems requiring 3, 4, and 5 moves. Balls are shown on a computer screen that is divided into two displays. The subject must use the balls in the lower display to copy the pattern shown in the upper one. The balls may be moved one at a time by touching the required ball and then touching the position to which it should be moved.
Rapid visual processing
This is a test of sustained attention, inhibition, and impulsivity, and speed of information processing. A white box is displayed in the center of the computer screen, inside which digits, from 2 to 9, are displayed in a pseudo-random order, at the rate of 100 digits per minute. The subject must detect consecutive odd or even sequences of digits (for example, 2-4-6 and 3-5-7) and respond by pressing the touch pad. Omissions and commissions are transformed into target sensitivity (RVPA′) and response bias (RVPB″). RVPA′ is the signal detection measure of sensitivity to the target, which indicates how well the participant can detect the target ranging from 0.00 to 1.00, and is therefore a measure of sustained attention. RVPB″ is the signal detection measure of the strength of visual trace required to elicit a response, which indicates the tendency to respond regardless of the presence of the target. It ranges from −1.00 to 1.00 and tests for inhibition and impulsivity. A high RVPB″ score indicates less impulsivity, whereas high RVPA′ indicates less difficulty in sustained attention.
Statistical analyses
Analyses were conducted using the Statistical Package for Social Sciences (SPSS), version 22. The mean and SD of continuous variables and frequencies and percentages for the categorical variable are reported. Participants who dropped out of the study were excluded from the final analysis. Pearson correlations were conducted assessing the relationship between the demographic variables and neurocognitive predictors with the outcome variable, % change in CDRS-R at both week 6 and 12, and an independent t-test comparing males and females on % change in CDRS-R. In addition, point biserial correlations were produced for comorbid anxiety, demographics, and neurocognitive measures.
Simple linear regression analyses were carried out to assess for baseline predictors of % change in CDRS-R scores during each of the 6- and 12-week interval. Normality analyses were conducted and variables were found to be normal. Due to the small sample size, we did not attempt to a run a multivariate regression with all the predictors in the model. For each predictor variable, only the significant relationships with a p-value ≤0.05 were considered. In addition to assessing the relationship between every neurocognitive variable and clinical improvement separately, we also entered each neurocognitive variable with one other neurocognitive variable into the regression, and considered only the results that led to an increase in the standardized β. Results are reported as β coefficients and 95% confidence interval. A multivariate regression analysis, including the variables, delayed matching to sample (DMS), and RVPA′ was run. Variables were checked for multicollinearity.
Results
Clinical characteristics
The average CDRS-R at baseline was 51.0 with an SD of 7.6. The average of % change of CDRS-R is noted at week 6 (M = 46.8, SD = 51.95) and week 12 (M = 87.95, SD = 57.22) (Fig. 1). Comorbid disorders, as outlined in Table 1, include post-traumatic stress disorder (PTSD), oppositional defiant disorder (ODD), obsessive compulsive disorder (OCD), other anxiety disorders, and treated ADHD. Participants under treatment for ADHD were asked to take their stimulant medication on the day of testing. Participants' medication dosages varied as follows: 14 (58.3%) were prescribed 20 mg, 2 (8.3%) were prescribed 30 mg, and 5 (20.8%) were prescribed 40 mg.
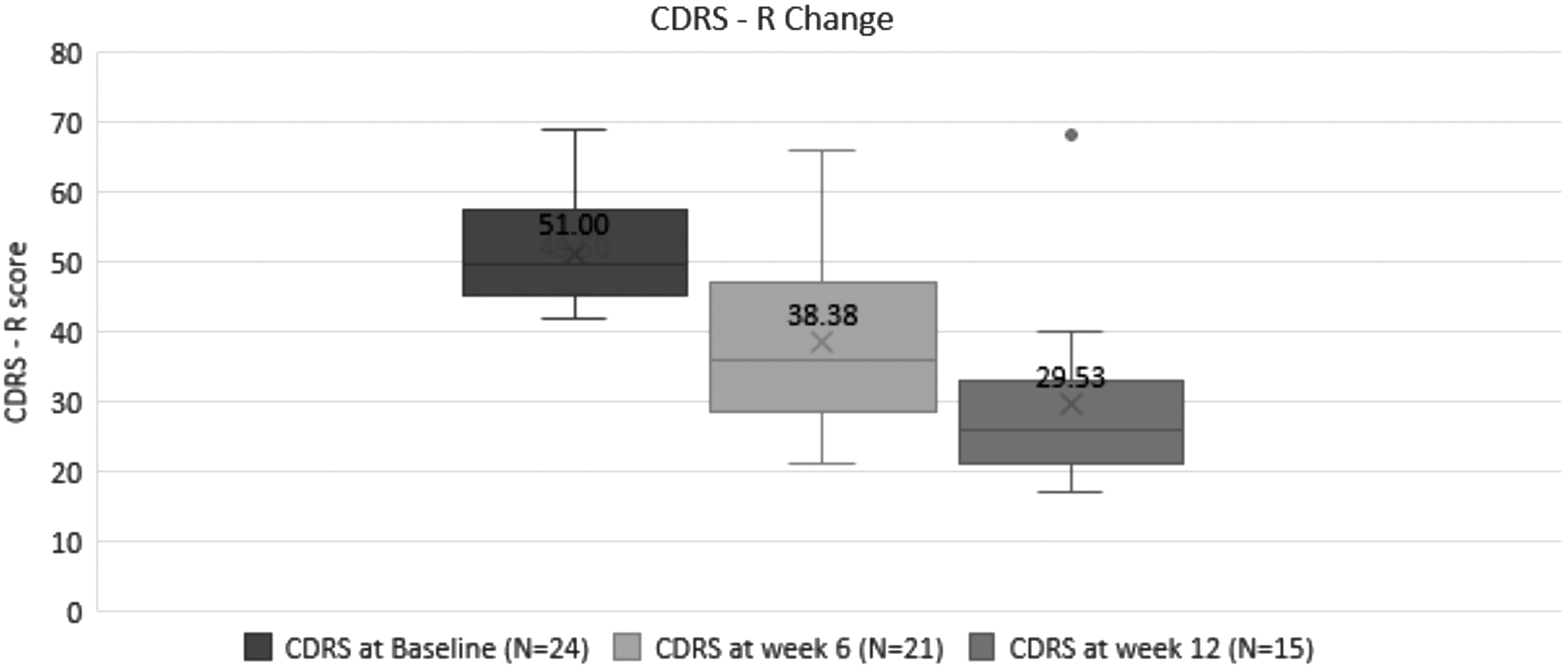
CDRS-R mean at baseline, and week 6 and 12. CDRS-R, Child Depression Rating Scale-Revised.
Correlation with demographics at week 6
A correlation matrix was produced to assess the relationship between IQ and age and the outcome variable % change in CDRS-R at week 6. No significant relationship emerged with % change in CDRS-R. In addition, an independent t-test comparing males and females on % change in CDRS-R revealed no significant difference between males (M = 72.8; SD = 62.9) and females (M = 30.8; SD = 38.2), p = 0.12. Of the sample, 12 (50%) also reported comorbid anxiety disorders. Similarly, no significant relationship emerged between age of onset of most recent MDD, duration of current depression and total number of depressive episodes, and % change in CDRS-R at week 6. No differences emerged on % change in CDRS-R at week 6 across the three groups of medication dosages F(2, 17) = 0.17, p > 0.05.
Correlation with demographics at week 12
Similarly, a correlation matrix was produced to assess the relationship between IQ and age and the outcome variable % change in CDRS-R at week 12, with 15 participants. No significant relationship emerged with the outcome % change in CDRS-R. In addition, there was no significant difference between males (M = 131.2, SD = 54.4) and females (M = 72.2, SD = 51.7) on % change in CDRS-R, p = 0.08. Similarly, no significant relationship emerged between the age of onset of most recent MDD and total number of depressive episodes and % change in CDRS-R at week 12. Duration of current MDD, however, was significantly negatively associated with % change in CDRS-R at week 12, r = −0.53, p = 0.02. No differences emerged on % change in CDRS-R at week 12 across the three groups of medication dosages F(2, 12) = 0.04, p > 0.05.
Correlation between clinical improvement at week 6 and baseline neurocognitive measures
Pearson's correlation was conducted to assess the relationship between the neurocognitive measures at baseline (RVPA, RVPB, DMS percent correct, Stockings of Cambridge [SOC] mean moves 3, SOC mean moves 4, SOC mean moves 5, and SOC minimum moves) and % change in CDRS-R at week 6 (Table 2). A significant relationship emerged between RVPA′ and % change in CDRS-R, r = 0.53, p = 0.00. A higher RVPA′ at baseline, indicating less difficulty in sustained attention at baseline, was associated with an increase in % change in CDRS-R (i.e., more clinical improvement). Similarly, a significant relationship emerged between RVPB″ and % change in CDRS-R, r = 0.64, p = 0.00. A higher RVPB″ at baseline, indicating less impulsivity at baseline, was associated with an increase in % change in CDRS-R. A significant relationship between SOC mean moves 3 and % change in CDRS-R also emerged, r = −0.45, p = 0.02, indicating that the greater the number of moves used to solve a 3-move problem (suggesting difficulty in executive functioning/planning), the less likely that there is an improvement in % change in CDRS-R. No significant relationship emerged with DMS, r = 0.15, p = 0.26, SOC 4, r = −0.04, p = 0.43, SOC 5, r = −0.32, p = 0.08, and SOC minimum moves, r = 0.33, p = 0.07.
CDRS-R, Child Depression Rating Scale-Revised; DMS, delayed matching to sample: visual memory; RVP, rapid visual processing; RVPA, sustained attention; RVPB, impulsivity; SOC, Stockings of Cambridge: problem solving and planning.
Correlation between clinical improvement at week 12 and baseline neurocognitive measures
A correlation matrix was produced to assess the relationship between the neurocognitive measures at baseline (RVPA, RVPB, DMS, SOC mean moves 3, SOC mean moves 4, SOC mean moves 5, and SOC minimum moves) and % change in CDRS-R at week 12 (Table 2). The relationship between RVPA′ and % change in CDRS-R bordered on statistical significance, r = 0.42, p = 0.06. As RVPA′ increased, % change in CDRS-R increased. A significant relationship emerged between RVPB″ and % change in CDRS-R, r = 0.63, p = 0.00, indicating that as RVPB″ increased, % change in CDRS-R increased. In addition, a significant relationship between SOC mean moves 3 and % change in CDRS-R is noted, r = −0.45, p = 0.05, which indicates that as the number of moves used to solve a 3-move problem increased, % change in CDRS-R decreased. No significant relationship emerged with DMS, r = −0.01 p = 0.49, SOC 4, r = −0.05, p = 0.43, SOC 5, r = −0.35, p = 0.10, and SOC minimum moves, r = 0.24, p = 0.19.
Predictors of clinical improvement at week 6
Simple linear regression analyses were carried out to assess the relationship between each neurocognitive measure and % change in CDRS-R at week 6 (Table 3).
CDRS-R, Child Depression Rating Scale-Revised; DMS, delayed matching to sample: visual memory; RVP, rapid visual processing; RVPA, sustained attention; RVPB, impulsivity; SOC, Stockings of Cambridge: problem solving and planning.
RVPB″ emerged as a significant predictor of % change with a standardized β = 0.64, p = 0.00, accounting for 41% of the variance in the outcome. RVPA′ was also a significant predictor, with a standardized beta of β = 0.53, p = 0.02, accounting for 27.5% of the variance in the outcome. Entering the variable RVPA′ with DMS percent correct as control, however, reveals RVPA′ as a significant predictor with an increase in the standardized β for RVPA′ to β = 0.65, p = 0.01, accounting for 30.1% of the variance.
In addition, SOC mean moves 3 was a significant predictor, with a standardized beta of β = −0.45, p = 0.04, accounting for 20.4% of the variance.
Predictors of clinical improvement at week 12
Simple linear regression analyses were conducted to assess the relationship between each neurocognitive measure and % change in CDRS-R at week 12 (Table 4). In this study, RVPB″ emerged as the only significant predictor of % change in CDRS with a standardized β = 0.63, p = 0.01, accounting for 39.4% of the variance in the outcome.
CDRS-R, Child Depression Rating Scale-Revised; DMS, delayed matching to sample; RVP, rapid visual processing; SOC, Stockings of Cambridge.
Correlation between comorbid anxiety and demographics
Point biserial correlations reveal no significant relationship between comorbid anxiety and IQ and age. A chi-square assessing the relationship between anxiety comorbidities and gender similarly revealed no significant relationship.
Correlation between comorbid anxiety and neurocognitive measures
Point biserial correlations revealed no significant relationship between comorbid anxiety and each of the neurocognitive measures: RVPA′, RVPB,″ DMS, and SOC mean moves 3, 4, and 5.
Correlation between comorbid anxiety and % change in CDRS-R at week 6 and 12
Point biserial correlations revealed no significant relationship between comorbid anxiety and % change in CDRS-R at week 6 and 12.
Discussion
This study examined neurocognitive predictors of clinical improvement with SSRI treatment of adolescents with MDD at week 6 and 12. Results revealed that better sustained attention, lower impulsivity, and better planning as measured by our behavioral tasks were predictive of greater clinical improvement at week 6. At week 12, lower impulsivity at baseline remained a significant predictor of clinical improvement. More severe impairments on these tasks were associated with poorer treatment outcomes.
Consistent with these findings, a number of studies have identified several cognitive deficits as predictors of treatment response in adult populations, including impaired attention and mental processing speed (Herrera-Guzmán et al. 2008) and poor planning (Bruder et al. 2014; Pimontel et al. 2016). Although several studies have reported various neurocognitive deficits in depressed adolescents (Baune et al. 2014; Wagner et al. 2015), to our knowledge, our findings are the first to describe the neurocognitive predictors of clinical improvement in this population.
Impulsivity emerged as a robust predictor of poor clinical improvement in our sample at week 6 and 12. Numerous studies have found that depressed adolescents are more impulsive than healthy controls on behavioral and decision-making tasks (Cataldo et al. 2005; Maalouf et al. 2011). Our findings suggest that youth with high impulsivity may be better candidates for interventions other than monotherapy with SSRI, such as combination therapy, augmentation therapy, or pharmacotherapy with a non-SSRI to help optimize their treatment response. In addition, behavioral impulsivity may indicate subthreshold ADHD symptoms, although, in our sample, untreated ADHD was an exclusion criterion. Adolescents with combined ADHD and MDD are less likely to respond to conventional treatment (Turgay and Ansari, 2006).
Worse sustained attention was also a predictor of poor clinical improvement in our sample. Impaired sustained attention has been extensively associated with bipolar symptoms (Clark et al. 2002) and proposed to be bipolar specific (Maalouf et al. 2010). Although participants with history of bipolar disorder were excluded from this study, it is possible that poor performance on sustained attention tasks is a proxy of subsyndromal manic symptoms. Several studies have reported subthreshold bipolar symptomatology as predictors and correlates of treatment resistance in adults with depression, even in samples where bipolar disorder is explicitly excluded (Correa et al. 2010; Dudek et al. 2010). Similarly, depressed adolescents with subsyndromal manic symptoms were less likely to respond to SSRI and combination of SSRI and Cognitive Behavioral Therapy treatments (Maalouf et al. 2012). Up to 80% of patients resistant to treatment for depression were found to have bipolar spectrum disorder in one study (Sharma et al. 2005). It is suggested that patients with depression and subthreshold bipolarity are best treated with mood stabilizer after antidepressant use (Licht et al. 2008). Neurocognitive assessments at baseline may serve to identify those who are less likely to respond to the conventional treatment and are good candidates for alternative treatment options.
Worse performance on the SOC task, indicating more difficulty in problem solving and planning, was also shown to predict poor clinical improvement. While performance on the component of the SOC task with moderate difficulty (3-move problems) predicted clinical improvement, performance on the more difficult components of the task did not, most likely due to a ceiling effect. These findings are consistent with studies associating executive dysfunction with poor treatment response in adult depression: poor performance on SOC in nonresponders to bupropion (Herrera-Guzmán et al. 2008) and executive dysfunction as a predictor of poor response to Citalopram in geriatric depression (Alexopoulos et al. 2005). Executive dysfunction in depressed mood states may translate into deficits in cognitive control processes essential for emotional regulation. Negative and self-focused cognitions central to depression further deplete executive functioning resources. It may be that individuals with worse executive functioning at baseline are better served with a combination treatment (pharmacotherapy and psychotherapy), and with psychotherapy focusing on cognitive training. For example, in one study, problem-solving therapy targeting executive dysfunction was shown to improve depressive symptoms in geriatric populations (Alexopoulos et al. 2005). This study, however, assessed executive functioning through a single task only. Future studies would need to use a more comprehensive range of tasks tapping into the multidimensional nature of this construct in adolescents (Shehab et al. 2016).
Visual memory, as measured by DMS, was not predictive of treatment response in this sample. While previous studies have found no group differences on visual memory between depressed adolescents and healthy controls (Brooks et al. 2010; Maalouf et al. 2011), one study found visual memory deficits to predict clinical response to bupropion in young adults (Herrera-Guzmán et al. 2008).
Our study has a number of limitations. The sample size and the rate of dropout by week 12 did not allow us to conduct analyses on treatment responders versus nonresponders. The lack of a placebo control group is also another limitation. With a placebo group, we could have explored predictors of clinical improvement on placebo and determined whether they differed from those on SSRI. Furthermore, future studies could benefit from including comparison groups of adolescents with depression receiving psychotherapy or no treatment. Based on the findings, directly assessing for subsyndromal mania as predictors of clinical improvement in this population is also of relevance. Inclusion of a wider array of neurocognitive tests and larger sample sizes are needed in future studies that would aim to replicate our findings.
Conclusion
To sum up, cognitive deficits known to represent a core component in MDD emerge now as important predictors of poor clinical improvement in depressed adolescents treated with SSRI. The use of cognitive measures to predict treatment outcomes may prove to be a cost-efficient and rapid approach to differentiate responders from nonresponders early on and allow psychiatrists to relay more realistic prognoses, tailor the course of treatment, match patients with the most optimal treatment, and ultimately enhance compliance (Bruder et al. 2014).
Clinical Significance
Cognitive deficits are important predictors of poor clinical improvement in depressed adolescents treated with SSRIs. The use of cognitive measures to predict treatment outcomes may prove to be a cost-efficient and rapid approach to differentiate responders from nonresponders early and allow clinicians to tailor the course of treatment accordingly.
Footnotes
Disclosures
Dr. Fadi Maalouf receives grants support from the Medical Practice Plan–Faculty of Medicine at the American University of Beirut and is on the speaker Bureau of Eli Lilly and Company. Dr. David Brent receives research support from NIMH, royalties from Guilford Press, royalties from the electronic self-rated version of the C-SSRS from ERT, Inc., royalties from performing duties as an UptoDate Psychiatry Section Editor, and consulting fees from Healthwise. R.B., H.T., and S.S. have no conflict of interests.