
Abstract
Objective:
This population-based epidemiologic study aimed to analyze the prevalence and trends of atypical antipsychotic (AAP) use and identify factors associated with AAP prescribing among children and adolescents in Korea.
Methods:
Using the Health Insurance Review and Assessment Service—Pediatric Patients Sample data between 2010 and 2014, we assessed the prevalence of and secular trends in AAP use; utilization of individual AAP drug based on the type of healthcare services, healthcare institutions, and health security programs; and factors associated with AAP use.
Results:
The average annual prevalence of AAP use was 417 per 100,000 children and adolescents, which increased by 40% from 2010 to 2014. The major AAP drug of choice has shifted from risperidone (72.70% and 49.29% in 2010 and 2014, respectively) to aripiprazole (11.31% and 34.64% in 2010 and 2014, respectively). Quetiapine was mainly prescribed for inpatients. Therefore, hospitals have 2–3 times higher proportion of quetiapine use than clinics. A prominent difference exists in the prescribing rates and AAP drug of choice based on income level. Patients enrolled in the Medical Aid (MA) program had a higher AAP prescription rate than those enrolled in the National Health Insurance (NHI) program (adjusted odds ratio: 7.78). Moreover, MA recipients were more frequently prescribed with cheaper alternatives, such as risperidone, compared with NHI recipients.
Conclusion:
AAP has been increasingly used among the pediatric population in Korea. Future studies are needed to identify the causes of this increase and establish evidence on appropriate AAP use. In addition, relevant policies should be developed to ensure that low-income mentally ill children could take advantage of the best available therapy.
Introduction
A
In Western countries, a number of epidemiologic studies on AAP use have been performed, which provided valuable information on the extent and trend of utilization over time, variation in utilization among different populations and regions, and patient and prescriber characteristics associated with its utilization, among others. Such information is useful in identifying potential problems associated with AAP use within a population, which sometimes require special attention and lead to policy intervention. For example, the prevalence of AAP drug use among “commercially insured youths” in the United States was reported to be 267.1 per 100,000 participants aged 19 years and younger in 2001 (Curtis et al. 2005). In contrast, the prevalence of AAP medication use among pediatric patients enrolled in the Midwestern “State Medicaid” program in the United States was observed to be 1310 per 100,000 children in the same year (Patel et al. 2005), which was about four times higher than that among pediatric patients enrolled in “the commercial insurance” based on the findings of the study of Curtis et al. (2005). In addition, Patel et al. (2005) reported that the utilization rate of AAP drugs in the Midwestern Medicaid program increased by 10-fold from 1996 (140 per 100,000 children) to 2001 (1310 per 100,000 children). In Germany, the annual prevalence rate of AAP drugs increased by twofold from 2005 (0.10%) to 2012 (0.24%) (Bachmann et al. 2014). Many recently published studies in Western countries have reported an association between AAP use and the risk of developing metabolic abnormalities such as significant weigh gain, dysfunction of appetite control, and type 2 diabetes mellitus (Rummel-Kluge et al. 2010; Pringsheim et al. 2011; Rubin et al. 2015).
Compared with the Western countries, a paucity of pediatric epidemiologic studies on AAP use exists in Asian countries, including Korea, which causes us difficulty in identifying potential issues and preparing strategies to resolve these issues. Thus, we conducted a population-based epidemiologic study on pediatric AAP use in Korea to (i) assess the national prevalence and trends of AAP use; (ii) identify the characteristics of AAP users; (iii) evaluate the utilization of individual AAP drug based on the types of healthcare services, healthcare institutions, and health security programs; and (iv) determine the factors associated with AAP prescribing. We expect that the results of this study will contribute to real-world evidences on AAP use among the Asian pediatric population.
Methods
Data source
The Health Insurance Review and Assessment Service (HIRA)–Pediatric Patients Sample (PPS) claims data between 2010 and 2014 (serial nos.: HIRA-PPS-2010-0068; 2011-0077; 2013-0069; 2012-0065; and 2014-0053) were used to estimate the prevalence of AAP use among the pediatric patients with MI in Korea and changes in the prevalence rates in the recent years. Korea has a universal health security system, which covers the entire population. The HIRA-PPS is an annual 10% age- and sex-stratified random sample (about 1,000,000 individuals with claims records) of the entire pediatric beneficiaries in Korea, which comprise those enrolled in the National Health Insurance (NHI, about 97%) and Medical Aid (MA, about 3%) programs (Song 2009). The HIRA-PPS data provide claims records that include demographic information, such as age and sex; diagnostic, procedural, and prescription records for healthcare services provided; and information on healthcare institutions (Kim et al. 2014). The research protocol was approved by the Institutional Review Board of Yonsei University (IRB no.: 1040917-201606-SB-181-01E). The need for informed consent from the study population was waived by the board.
Study population
The study population was defined as patients aged between 2 and 19 years old who had at least one claims record with a diagnostic code of MI (10th International Classification Disease Code “F”) from the HIRA-PPS data from 2010 to 2014. The F codes include ADHD (F90.0); tic disorder (F95); pervasive developmental disorder (F84), including ASD; depression (F32); schizophrenia (F20, F29); bipolar affective disorder (F31); and other MIs, such as mild mental retardation (F70), obsessive-compulsive disorder (F42), and so on (Diagnostic and Statistical Manual of Mental Disorders, 5th ed. [DSM-5], American Psychiatric Association 2013). More detailed diagnosis codes are presented in Appendix A1. Infants younger than 2 years were excluded from the study population due to the uncertainty of their diagnoses. We divided the study population into three age groups: preschoolers (2–6 years), elementary school students (7–12 years), and adolescents (13–19 years).
AAPs were classified as N05A, which refer to antipsychotics, based on the Anatomical Therapeutic Chemical classification system of the World Health Organization. According to the previous literatures (Newcomer 2005; Crystal et al. 2009; Kumar et al. 2013; Wang et al. 2013; Park et al. 2014; Saloner et al. 2014; Sohn et al. 2015) and clinical experts' advices, 10 drugs among the antipsychotics listed under the N05A class were considered as AAPs: amisulpride, aripiprazole, blonanserin, clozapine, olanzapine, paliperidone, quetiapine, risperidone, ziprasidone, and zotepine. We defined the patients treated with AAPs as those with a MI who received at least one prescription for any of the 10 AAPs.
Data analysis
We performed both patient-unit and claim-unit analyses depending on the purpose of the analysis using a population-based cross-sectional study design. For each study year from 2010 to 2014, we estimated the annual prevalence of patients with MI and those treated with AAPs for MIs. The percent change in the prevalence was calculated from 2010 to 2014 to examine whether the number of patients with MI and AAP use among children and adolescents have been increasing or decreasing in the Korean society.
(1) Patient-unit MI prevalence (%) = (Number of pediatric patients with MI/total number of pediatric population) × 100
(2) Patient-unit AAP use prevalence (%) = (Number of pediatric patients with AAP medication/total number of pediatric population) × 100
(3) Patient-unit AAP use prevalence among MI pediatric patients (%) = (Number of MI pediatric patients with AAP medication/number of pediatric patients with MI) × 100
(4) Claim-unit AAP use prevalence among MI pediatric claims (%) = (Number of claims with AAP medication in MI pediatric claims/number of MI pediatric claims) × 100
Moreover, the proportion of prescriptions issued that included AAPs among patients with MI was estimated. We examined the characteristics of patients prescribed with AAP medications using a demographic analysis. Furthermore, an annual descriptive analysis was performed based on the types of healthcare services, healthcare institutions, and health security program that patients were enrolled in to compare trends in the use of individual AAP drug over a 5-year period from 2010 to 2014. The types of healthcare services were classified into inpatient and outpatient services. The patients were classified as inpatients if they had experienced hospital admission at least once and outpatients if they had only outpatient visits during the study year. In addition, the types of healthcare institutions were categorized in accordance with the Korean Medical Service Act as follows: clinics (<30 beds and primarily for outpatients), hospitals (≥30 beds), general hospitals (≥100 beds and either ≥7 medical specialists for ≤300 beds or ≥9 medical specialists for >300 beds), tertiary care hospitals (≥20 medical specialists and designated by the Korea Ministry of Health and Welfare), and other healthcare institutions, such as public health centers and veterans hospitals (Ministry of Health and Welfare 2016). For individual patients who had used healthcare services more than once during the study year, the types of healthcare institutions were determined based on the healthcare institutions that provided services to the patients as indicated in the index claims record during that year. The types of health security programs were exclusively divided into NHI and MA program. Patients enrolled in the MA program were defined as those with at least one experience in the MA program. In contrast, patients enrolled in the NHI program were defined as those continuously enrolled in the NHI program during the study year.
A logistic regression analysis was conducted to identify the characteristics of the patients and healthcare providers that are associated with AAP prescribing. The dependent variables of patients who received at least one AAP prescription during a year were denoted as 1 and 0 if otherwise in the logistic regression model. All statistical analyses were performed using the Statistical Analysis Software (SAS) program (version 9.4; SAS Institute, Inc., Cary, NC). The significance level was set at 1%.
Results
Prevalence of MIs and AAP medication use among children and adolescents
Over the 5-year study period, the average annual prevalence of MIs among pediatric patients was 3784 per 100,000 children and adolescents. Meanwhile, the average annual prevalence of AAP use for at least once to treat MIs among pediatric patients was 417 per 100,000 children and adolescents (Table 1). Interestingly, although the prevalence of MI among pediatric patients slightly decreased by 2.59%, the prevalence of AAP use among this population considerably increased by ∼40% from 2010 to 2014 (9592 kids; 35,621 in 2010 vs. 44,873 in 2014). The estimated average annual prevalence of MI for over 5 years increased with age: 2.53%, 3.33%, and 4.70% among preschoolers (2–6 years), elementary school students (7–12 years), and adolescents (13–19 years), respectively. The same trend that is associated with age was observed for the prevalence of AAP medication use among patients: 0.08%, 0.48%, and 0.55% among preschoolers, elementary school students, and adolescents, respectively.
Patient with MI means “Patient-unit MI prevalence (%) = (Number of pediatric patients with MI/total number of pediatric population) × 100.”
Patient with AAP medication means “Patient-unit AAP use prevalence (%) = (Number of pediatric patients with AAP medication/total number of pediatric population) × 100.”
No. of pediatric population aged between 2 and 19 years old was estimated from the Korea Statistics Office report.
AAP medication use in the treatment of MIs was limited.
AAP, atypical antipsychotic; MI, mental illness (e.g., ADHD [F90.0]; tic disorder [F95]; pervasive developmental disorders [F84], including autistic spectrum disorder; depression [F32]; schizophrenia [F20]; bipolar affective disorder [F31]; and other MIs); SD, standard deviation; ADHD, attention-deficit/hyperactivity disorder.
Figure 1 shows the AAP use among pediatric patients with MI, whereas Table 1 displays the AAP use among the entire Korean pediatric population. The annual prevalence of AAP use among pediatric patients with MI steadily increased from 9.16% in 2010 to 13.07% in 2014, which is a 1.43-fold increase (Fig. 1). In addition, the proportion of prescriptions that include AAP to treat pediatric MI increased by 1.36 times from 14.81% in 2010 to 20.08% in 2014.
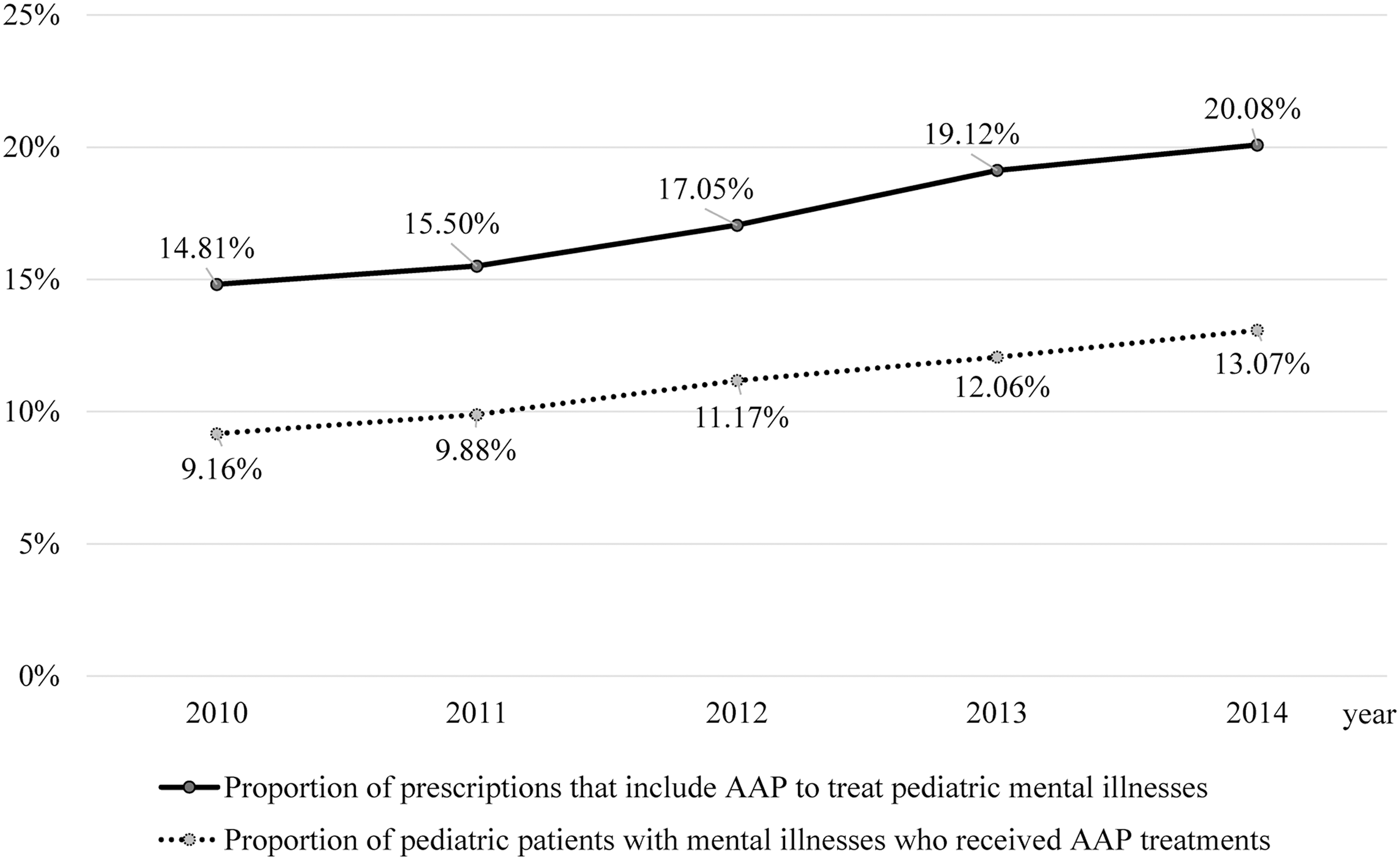
Annual trend in the prevalence of AAP treatments among Korean children between 2010 and 2014. Note: The denominator refers to the number of patients with mental illnesses (or prescriptions), whereas the numerator pertains to the number of patients prescribed with AAP drugs (or prescriptions). AAP, atypical antipsychotic.
Characteristics of patients and prescribers associated with AAP use
Table 2 shows the characteristics of pediatric patients with MI who were prescribed with AAPs. Two-thirds of the patients with AAP prescriptions were boys, of whom 60.21% were adolescents. More than 10% of the patients with AAP prescriptions were enrolled in the MA program. This rate is more than triple the enrollment rate in the MA program among the general pediatric patients (Song 2009). Patients with ADHD (24.86%) and tic disorder (24.75%) accounted for the largest proportion of AAP users, followed by those with depression (8.58%) and ASD (7.77%). More than 50% and 85% of the patients were prescribed with AAPs by clinics (55.33%) and psychiatrists, respectively.
Patients enrolled in the MA program were defined as those enrolled in the program at least once, whereas patients enrolled in the NHI program were defined as those who were not included in the Medical Aid program at least once during the study period.
Roughly 2/3 of patients had more than one diagnosis across the study period.
Inpatients were defined as those who were admitted at least once during the study period, whereas outpatients were defined as those who received only outpatient care during the study period.
We used the first prescription for visiting healthcare institution to define the type of healthcare institution, physician specialty, and location of healthcare institution of the patients.
AAP, atypical antipsychotic; ADHD, attention-deficit/hyperactivity disorder; ICD-10, 10th revision of the International Statistical Classification of Diseases; NHI, National Health Insurance; MA, Medical Aid.
Utilization of individual AAP drug
Figures 2 –4 demonstrate the distribution of individual AAP drug prescribed across the different types of healthcare services and institutions and health security programs. First, the utilization rate of individual AAP drug varied depending on whether pediatric patients with MI were treated in an outpatient or inpatient setting. For example, risperidone appears to be the dominant AAP drug of choice for outpatient care, which accounted for 72.70% of the total AAP prescriptions in the outpatient setting in 2010 (Fig. 2). In contrast, risperidone and quetiapine are the most frequently prescribed AAPs for inpatient care, each of which account for about 39% and 30% of the total AAP prescriptions in 2010, respectively. For both outpatient and inpatient care, the utilization of risperidone has been decreasing from 2010 to 2014, with a more dramatic use reduction for outpatient care (from 72.70% in 2010 to 49.29% in 2014) than for inpatient care (from 38.53% in 2010 to 33.64% in 2014). The reduced proportion of risperidone prescriptions led to the increase in aripiprazole prescription for both outpatient (from 11.31% in 2010 to 34.64% in 2014) and inpatient (from 9.45% in 2010 to 16.79% in 2014) care, implying a switching trend between the two drugs in Korea. Quetiapine was the second most commonly prescribed AAP among inpatient children and adolescent with MI in both 2010 and 2014, although a decreasing trend in its utilization was observed over this period.
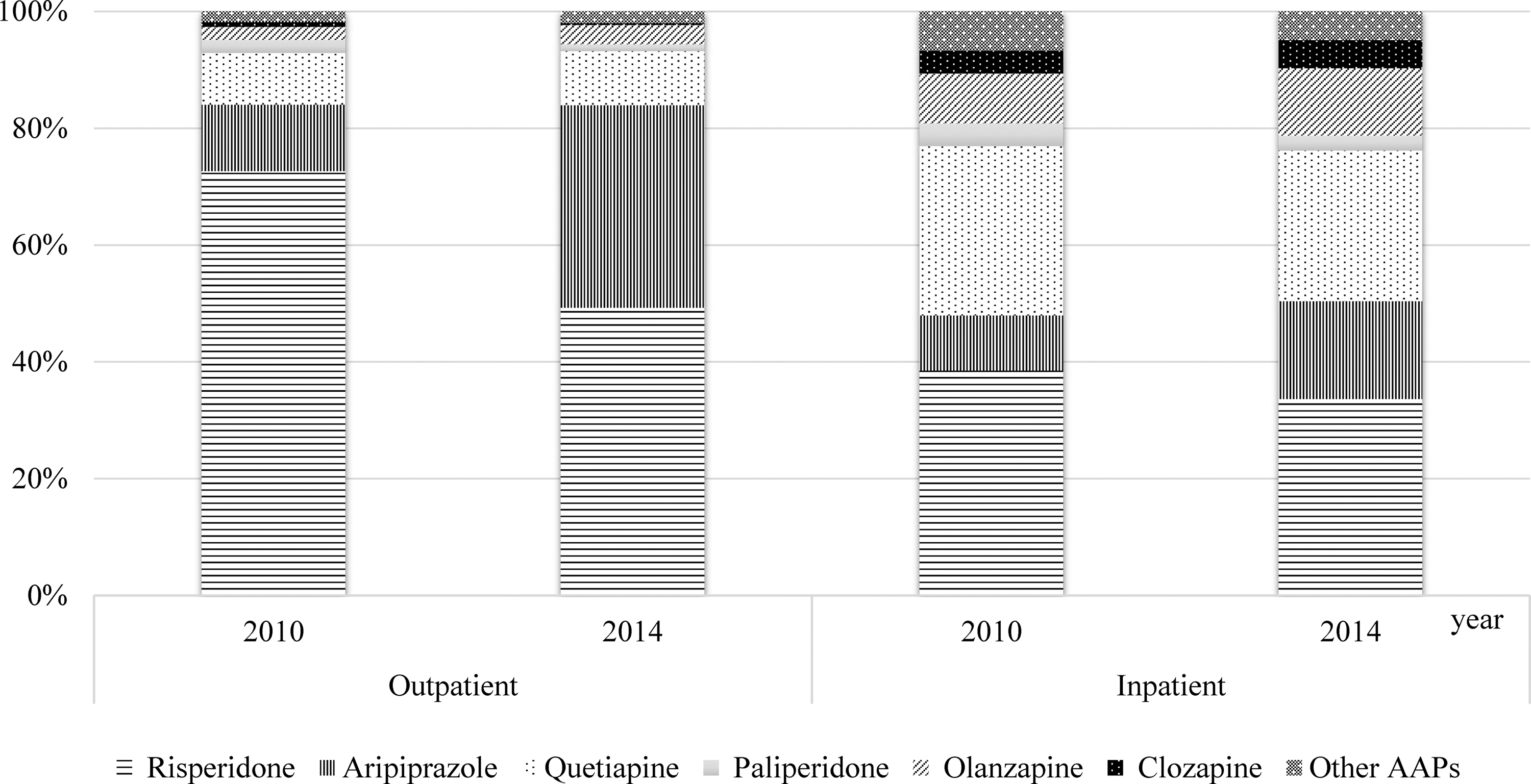
Distribution of individual AAP prescribed to treat pediatric mental illness based on the type of healthcare services in Korea. Note: If a prescription contained more than one AAP, each prescription was counted. AAP, atypical antipsychotic.
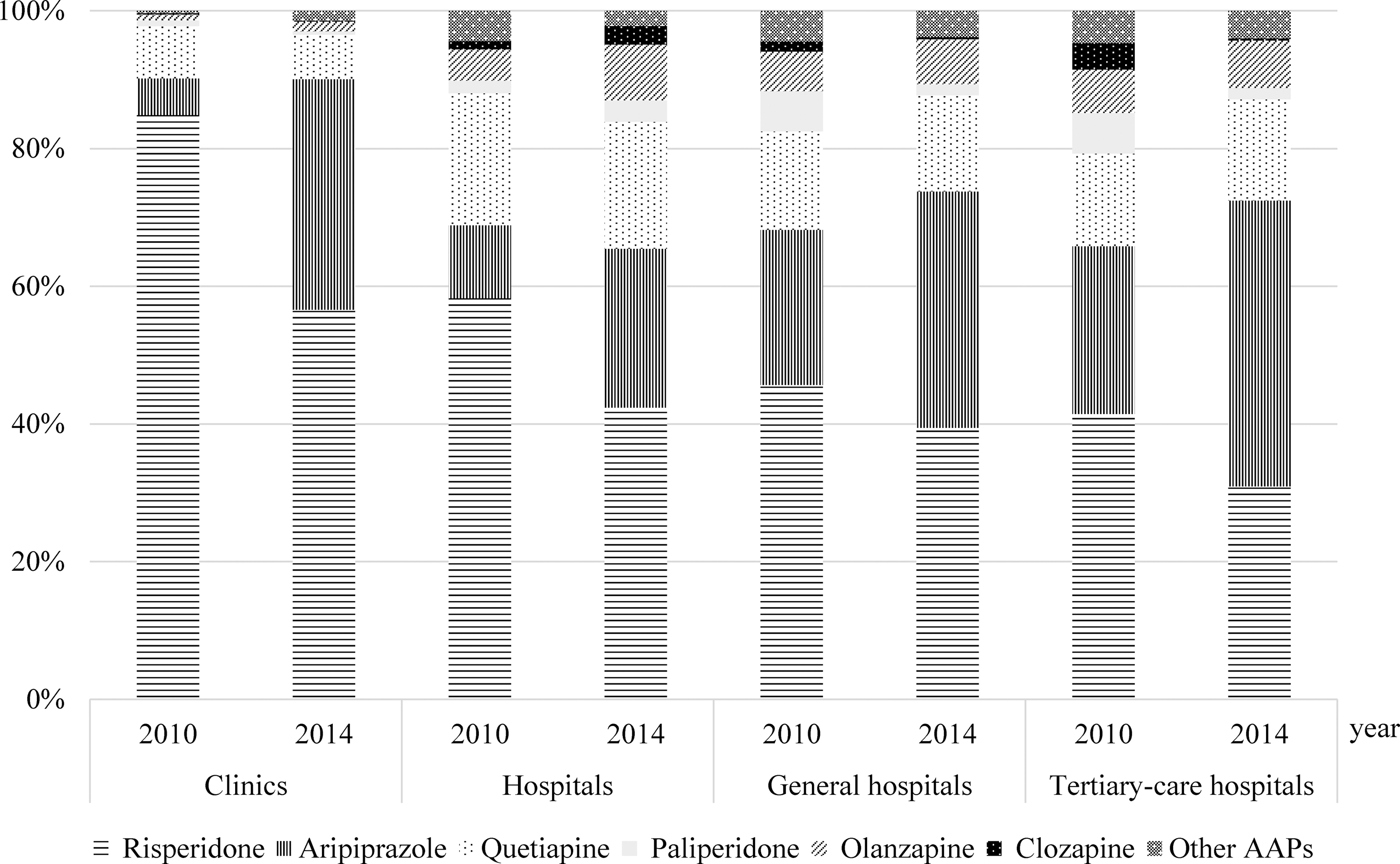
Distribution of individual AAP prescribed to treat pediatric mental illnesses based on the type of healthcare institutions in Korea. Note: If a prescription contained more than one AAP, each prescription was counted. AAP, atypical antipsychotic.
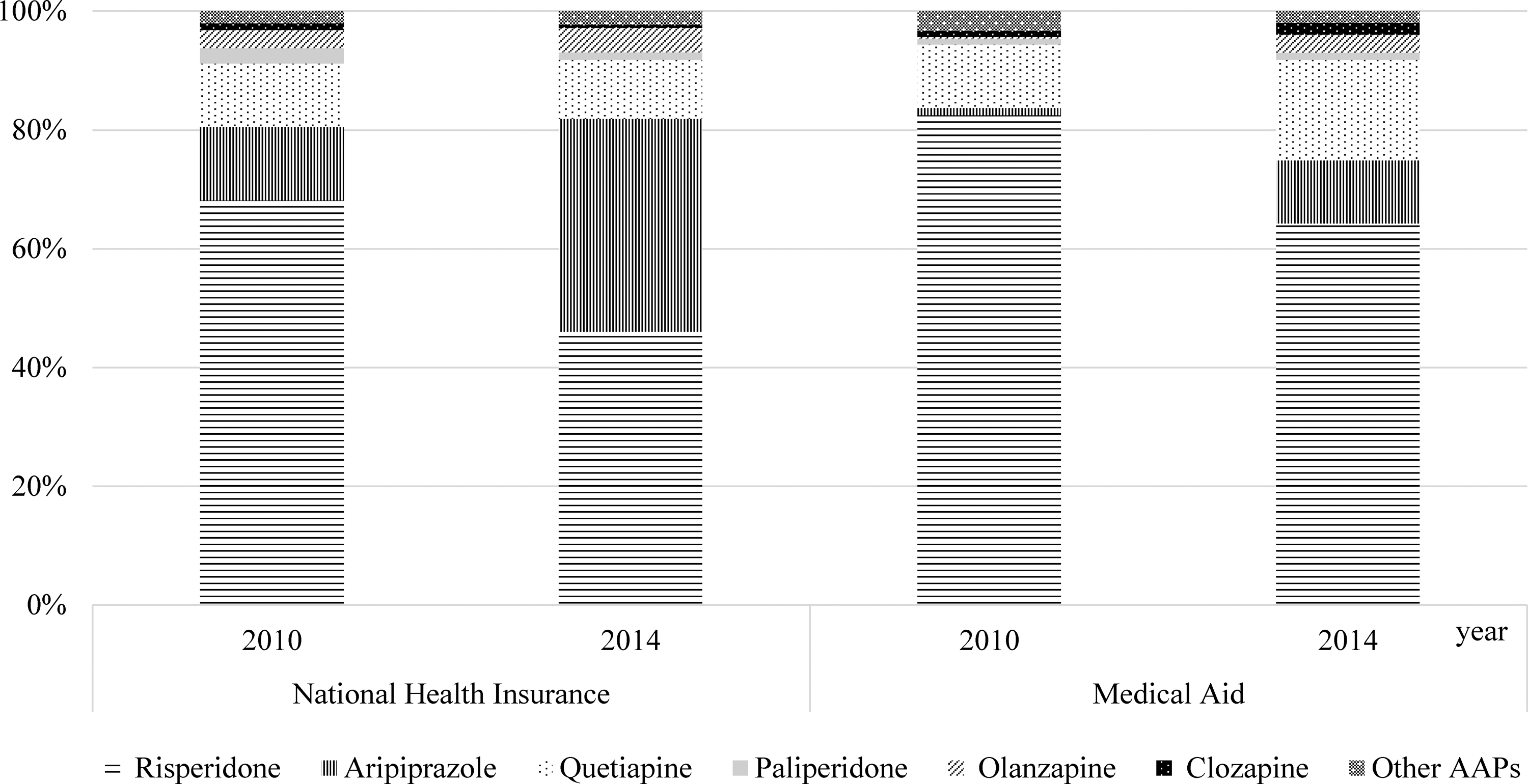
Distribution of individual AAP prescribed to treat pediatric mental illnesses based on the type of health security program in Korea. Note: If a prescription contained more than one AAP, each prescription was counted. AAP, atypical antipsychotic.
As shown in Figure 3, AAP prescriptions differ based on the type of healthcare institutions. In all types of healthcare institutions, risperidone was the most commonly prescribed AAP drug in 2010. However, the variation in the proportion of risperidone prescriptions was very high: the largest and smallest variations were observed in clinics (84.87%) and tertiary care hospitals (41.45%), respectively. Over the 5-year period, the proportion of risperidone prescriptions decreased, whereas that of aripiprazole prescriptions increased. Moreover, considerable reduction was observed in risperidone prescriptions among all types of healthcare institutions. In particular, the proportion of aripiprazole prescriptions in 2014 was more than six times than that in 2010 among clinics. The magnitude of the decrease in risperidone prescription was most prominent among clinics. Quetiapine was also a frequently prescribed AAP drug among all types of healthcare institutions. Based on the data on AAP prescriptions in 2014, the proportion of quetiapine prescriptions was 6.45% among clinics. However, the proportion of quetiapine prescriptions was 2–3 times higher (13.94%–18.42%) among hospitals, where admissions were possible, than among clinics. The proportion of quetiapine prescriptions remained almost the same between 2010 and 2014 regardless of the type of healthcare institutions.
The individual AAP drug utilization also differs depending on the type of health security program that the patients were enrolled in Figure 4. Those who are enrolled in the NHI program were prescribed with risperidone, aripiprazole, and quetiapine in order in 2010. This order remained the same in 2014. However, the proportion of risperidone prescription considerably decreased (from 68.15% in 2010 to 46.04% in 2014), whereas that of aripiprazole prescription remarkably increased (from 12.36% in 2010 to 35.82% in 2014), resulting in the change in risperidone/aripiprazole (R/A) ratio from 5.51 (68.15%/12.36%) in 2010 to 1.29 (46.04%/35.82%) in 2014 among the NHI patients. In both 2010 and 2014, risperidone (from 82.46% in 2010 to 64.28% in 2014) was the dominant AAP drug of choice for patients enrolled in the MA program, followed by quetiapine (from 10.67% in 2010 to 16.89% in 2014) and aripiprazole (from 1.23% in 2010 to 10.64% in 2014). The R/A ratio among the MA enrollees also decreased from 67.04 (82.46%/1.23%) in 2010 to 6.04 (64.28%/10.64%) in 2014, which was a considerably larger change than that among the NHI enrollees. However, the ratio remains significantly higher among the MA enrollees than among the NHI enrollees.
Factors associated with AAP prescribing
The logistic regression analysis result showed that female patients were less frequently prescribed with AAPs than male patients (odds ratio [OR], 0.72; 95% confidence interval [CI], 0.70–0.75), and a similar trend was observed among older children (OR: 4.41 and 6.40 for participants aged 7–12 and 13–19 years old, respectively) compared with their younger counterparts (Table 3). The proportion of AAP prescribing linearly increased over time during the 5-year study period. The varying tendency of AAP prescribing was observed among the different types of MI. For instance, patients with ASD (OR, 3.88; 95% CI, 3.61–4.18) and tic disorder (OR, 5.14; 95% CI, 4.84–5.47) were more likely to be treated with AAPs than those with ADHD. In contrast, patients with depression had a lower probability of receiving AAP treatments than those with ADHD (OR, 0.79; 95% CI, 0.75–0.84). Moreover, children from a low-income class, which are defined as those who are MA beneficiaries, had 7.78 times higher probability of receiving AAPs for their MI (OR, 7.78; 95% CI, 7.26–8.34) than those from a high-income class.
Value is statistically significant (p < 0.01).
Patients enrolled in the MA program were defined as those enrolled in the program at least once, whereas patients enrolled in the NHI program were defined as those who were not included in the MA program at least once during the study period.
We used the first prescription for visiting healthcare institution to define the type of healthcare institution, physician specialty, and location of healthcare institution of patients.
ADHD, attention-deficit/hyperactivity disorder; ASD, autism spectrum disorder; CI, confidence interval; MA, Medical Aid; NHI, National Health Insurance; OR, odds ratio; ref, reference.
The characteristics of healthcare providers were also associated with AAP prescribing for pediatric MI. The OR for the probability of prescribing AAPs increases as the level of healthcare institutions increases. The OR for hospitals, general hospitals, and tertiary hospitals are 1.95 (95% CI: 1.85–2.06), 1.73 (1.65–1.82), and 2.11 (2.02–2.21), respectively, compared with those of clinics. The healthcare institutions from the metropolitan area were more likely to prescribe AAPs than those from the city or rural area.
Discussion
To the best of our knowledge, this study is the first to examine the population use of AAP medications among children and adolescents in Asia. Although the use of AAP medication among pediatric patients was expected to increase in line with the findings of previous Western studies, no study results have shown the actual use of these drugs in Asia. The findings from this study are based on the NHI claims data in Korea, which encompass the entire population of the country. Therefore, these findings are meaningful in that they are highly representative and can serve as data for estimating AAP use in Asia.
This study presented the prevalence of AAP medication use and its recent trend among Korean children and adolescents. Between 2010 and 2014, the average annual prevalence of AAP prescription in Korea was 417 per 100,000 children and adolescents. As shown in Table 4, this prevalence was lower than that among Medicaid enrollees in the early 2000s, as observed by U.S. studies (Patel et al. 2005), but higher than that among private insured enrollees in 2001 and 2012, as determined by U.S. and German studies, respectively (Curtis et al. 2005; Bachmann et al. 2014).
Although a number of studies on the prevalence of antipsychotic drugs in other countries are available, only studies that directly present the prevalence and those where the prevalence rate can be easily derived are summarized in this table.
This value was derived by multiplying the prevalence of any psychotropic drug prescription (2.30%) by the rate of atypical antipsychotic prescription (0.17 × 0.96).
MCO, managed care organization.
The percentage of patients who were prescribed with AAP increased between 2010 and 2014 among all age groups. In the 2–6-year-old age group, the average annual AAP prescription rate between 2010 and 2014 was 81 per 100,000 pediatric population, which was lower than that reported among 2–4-year-old Medicaid enrollees (650 per 100,000 pediatric population) between 2001 and 2010 in the state of Kentucky in the United States (Lohr et al. 2015). The average annual AAP prescription rate between 2010 and 2014 for 7–12-year-old and 13–19-year-old age groups in Korea was 478 and 542 per 100,000 pediatric population, respectively. These figures are slightly higher than the AAP prescription rates for similar age groups enrolled in managed care organization in the United States (410 and 340 per 100,000 people aged 10–14 and 15–19 years old, respectively). However, these prescription rates were slightly lower than those among the Medicaid recipients in three U.S. states (1050–3400 and 1220–1480 per 100,000 people aged 10–14 and 15–19 years old, respectively) (Patel et al. 2005). In particular, the annual AAP prescription rate among adolescents was considerably lower than that among Medicaid recipients in a mid-Atlantic state (5200 per 100,000 people aged 13–17 years old) (Burcu et al. 2014). Two in every three patients who were prescribed with AAP were boys, and most patients were diagnosed with ADHD, tic disorder, depression, and ASD, similar to those of the U.S. study in 2015 (Lohr et al. 2015; Olfson et al. 2015).
The national health security program of Korea operates on a two-tier system: NHI and MA programs. The NHI program is a wage-based contributory insurance program that covers about 97% of the population, whereas the MA program is a government-subsidized program for the indigent population that accounts for about 3% of the population (Song 2009). Our study results showed that ∼11% of patients prescribed with AAP were MA beneficiaries, which is more than thrice the percentage of MA beneficiaries among the general population. The MA beneficiaries had 7.78 times higher probability of being treated with AAP drugs for MI than NHI beneficiaries (OR, 7.78; 95% CI, 7.26–8.34). These findings imply that pediatric patients from a low-income class had a higher probability of being treated with AAP than those from a high-income class. A similar finding was observed in a U.S. study, where the Medicaid beneficiaries had higher AAP prescription rate than private insurance subscribers (Patel et al. 2005). Such a phenomenon may be attributed to two factors. First, among the various therapeutic modalities that are considered when treating MI among children and adolescents, pharmacotherapy is relatively less costly than nonpharmacologic therapies, such as counseling or behavioral intervention (Ahn 2009). In Korea, drug therapy is subsidized by the NHI and MA programs, but most counseling and behavioral therapy are not covered by these programs. Considering the high financial burden, physicians may administer relatively less costly drug therapy to MA recipients with low-income levels than to NHI recipients. Second, MA beneficiaries may have more severe MIs than NHI beneficiaries. As such, they may receive combined treatments that includes drug therapy. However, this study cannot provide evidence for such speculation given the lack of information on disease severity from insurance claims data.
The investigation on trends in individual AAP drug utilization showed that risperidone was the dominant AAP drug of choice, but its prescribing rate remarkably decreased over the 5-year study period. In contrast, the prescribing rate of aripiprazole substantially increased during the same period. The predominant use of risperidone in the 2000s has been reported in studies conducted in foreign countries as well (Patel et al. 2002; Aparasu and Bhatara 2007). The prescription rate of aripiprazole was also reported to increase following its market entry in the mid-2000s (Health Insurance Review and Assessment Service 2016). Changes in the use of risperidone and aripiprazole in Korea can be explained by the timing of insurance coverage, market adoption behavior, and insurance price. Aripiprazole was listed on the NHI and the MA drug coverage in Korea in 2004, and subsequently, more active use of aripiprazole was observed in the late 2000s (Health Insurance Review and Assessment Service 2016).
In general, the market adoption of new medical technologies, including pharmaceuticals, expanded from tertiary care hospitals to clinics. Likewise, the use of aripiprazole would also expand to the clinical level after the full identification of its efficacy and adverse effects by tertiary care hospitals. Moreover, aripiprazole has a broader range of indications, including schizophrenia, bipolar disorder, depression as a supportive agent, pediatric autistic disorder, and pediatric Tourette's syndrome, than risperidone, which is also one of the reasons for the increased prescription rate of the former (Ministry of Food and Drug Safety 2016). The price of aripiprazole is believed to be the reason for its relatively lower prescription rate among MA recipients than among NHI patients, despite the aforementioned points. The MA recipients in Korea are subject to a per diem rate, and thus, they have a fixed amount of maximum aid per day. Considering that 2 mg of risperidone, which is recognized as the bioequivalent amount, costs about 1/3 times as much as 10 mg of aripiprazole, physicians face limitations in prescribing such high-priced drug to MA recipients. To address these issues, the Korean government announced its Comprehensive Plan on Mental Health Promotion based on the framework of raising the per diem of MA recipients and patients with severe mental disorders. The plan was announced in 2016 and will be implemented in 2017 (Korea Government Task Force 2016).
The risk of developing metabolic disease using AAP has been reported, and AAP is known to have a heterogeneous side effect compared to first-generation antipsychotics (Fraguas et al. 2011). Therefore, epidemiological studies and evaluation of the appropriateness of AAP use should be vigorously conducted in Asia to track the occurrence of side effects such as metabolic diseases caused by increased use of AAP.
This study have several limitations, most of which pertain to the nature of the administrative claims data. First, the study participants, namely, AAP users with MI, were identified based on the diagnosis and drug codes reported in the insurance claims by healthcare providers. Therefore, the probability of misclassification of the study participants and over- or underestimation of the prevalence of AAP use depends on the accuracy of the report. However, the HIRA-PPS claims data are considered to have high validity because the positive predictive value of the actual diagnosis was estimated to be 83.4% (Park et al. 2003). Second, the AAP users in this study were defined as those who received AAP drug prescription at least once during the study year. However, considering that the claims data do not provide information on drug compliance, we are not sure whether someone prescribed with a drug actually took the drug. Third, many psychotropic drugs are known to be prescribed in an off-label manner among children and adolescents in Korea (Lee 2011). However, given that the information on the off-label and nonreimbursable use of drugs cannot be obtained from claims data, our estimation of AAP use based on claims data may underestimate the actual AAP use among this population. Despite such limitations, we believe that this study is significant because it is the first to estimate the AAP prescription rate among pediatric patients at the population level, analyze the changes in prescription trend over the recent years, and identify the associated factors with AAP prescribing.
Conclusions
This study showed that the prevalence of AAP prescription progressively increased among Korean children and adolescents, similar to that observed in other developed countries. The major AAP drug of choice among prescribers has shifted from risperidone to aripiprazole over the 5-year study period. This shift is commonly observed in all types of healthcare services (i.e., inpatient and outpatient services) and institutions (i.e., clinics and hospitals). Quetiapine was mainly prescribed for inpatient care; therefore, hospitals had a higher proportion of its use than clinics. A prominent difference exists in the prescribing rates and AAP drug of choice among those available in Korea based on the income level. For example, MA beneficiaries receive AAP medication therapy about eight times more than NHI beneficiaries. In addition, MA recipients were more frequently prescribed with cheaper alternatives, such as risperidone, compared to NHI recipients. Relevant policies should be developed to ensure that mentally ill children from a low-income class can take advantage of the best available therapy choices, including both pharmacologic and nonpharmacologic treatments.
Clinical Significance
This study has produced real-world evidence on the use of AAPs among the pediatric population based on nationally representative insurance claims data as follows: (i) use of AAPs increased in Korea; (ii) mentally ill children from a low-income class (i.e., MA beneficiaries) were more likely to be prescribed with AAPs than those from a high-income class; and (iii) variations exist in the AAP drug of choice based on the type of healthcare services (inpatient vs. outpatient), healthcare institutions (clinics vs. hospitals), and health security programs (MA vs. NHI beneficiaries).
Footnotes
Acknowledgments
The authors thank Dr. Jin-Won Kwon and Dr. Min-Jung Chang for their comments with initial interpretation of results for this study.
Disclosures
The authors do not have any competing financial support or conflict of interests to declare. This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors and was not supported by any statistical consultants.
| ICD-10-codes | Description |
|---|---|
| F01–F09 | Mental disorders due to known physiological conditions |
| F10–F19 | Mental and behavioral disorders due to psychoactive substance use |
| F20–F29 | Schizophrenia, schizotypal, delusional, and other nonmood psychotic disorders |
| F30–F39 | Mood (affective) disorders |
| F40–F48 | Anxiety, dissociative, stress-related, somatoform, and other nonpsychotic mental disorders |
| F50–F59 | Behavioral syndromes associated with physiological disturbances and physical factors |
| F60–F69 | Disorders of adult personality and behavior |
| F70–F79 | Intellectual disabilities |
| F80–F89 | Pervasive and specific developmental disorders |
| F90–F98 | Behavioral and emotional disorders with onset usually occurring in childhood and adolescence |
| F99 | Unspecified mental disorder |
ICD-10, 10th revision of the International Statistical Classification of Diseases.