
Abstract
Objective:
To analyze liver function tests (LFT), weight, metabolic syndrome (MetS) and at risk of meeting MetS criteria (AR-MetS) in children and adolescents on antipsychotics (AP) during a year-long follow-up.
Methods:
Two hundred sixteen patients, AP naïve or quasi-naïve (<30 days on AP), were included. Total bilirubin, the enzymes aspartate aminotransferase (AST), alanine aminotransferase (ALT), alkaline phosphatase (ALP), weight and other parameters of MetS were measured at baseline, and at 3, 6 and 12 months, while patients remained on the same AP.
Results:
At baseline, patients (mean age: 14.1 ± 3.1 years; 60.2% male) were on risperidone (N = 143), olanzapine (N = 37), or quetiapine (N = 36), although the sample decreased over time to 67 patients at 12 months (risperidone N = 46, olanzapine N = 10, and quetiapine N = 11). Around 3% of patients had ALT/AST levels that were at least twice the upper limit of normal (ULN) at 3 and 6 months; whereas roughly 19% of patients had ALP levels that were at least twice the ULN in at least one assessment after baseline, but had no clinical symptoms. From baseline to 6 months, significant increases were observed in ALT levels in the whole sample (p = 0.005), whereas ALP increased only in patients on risperidone. Patients showed significant weight gain, and more individuals met criteria for MetS and AR-MetS over time (from baseline: 2.8% and 8.3%, to 1 year: 10.5% and 23.9%, respectively). There was a trend-level group effect in global ALT across time (p = 0.076). Patients with MetS showed higher ALT concentrations (28.9 [18.4–39.4] U/L) than AR-MetS (20.4 [8.5–32.2] U/L), and no-AR-MetS (19.2 [8.4–29.9] U/L).
Conclusions:
Less than 3% of children and adolescents on AP during 1-year follow-up showed an increase in ALT or AST levels in one or more of the assessments, and none of these increases was of clinical significance. Patients with MetS and AR-MetS increased during this period, and the possible role of ALT levels to monitor these patients deserves further study.
Introduction
T
LFT could become abnormal with SGA use due to three main mechanisms (Marwick et al. 2012): (1) impairment of bile secretion, which leads to cholestasis, and could be partially immunomediated by a hypersensitivity reaction; (2) direct toxic effects on hepatocytes that lead to liver cytolysis through a gradual accumulation of minor toxic metabolites; and (3) weight gain and MetS leading to nonalcoholic fatty liver disease (NAFLD). Risperidone has been linked to cholestatic hepatitis; quetiapine, olanzapine, and ziprasidone to hepatocellular damage; and clozapine to hepatic necrosis and cholestatic hepatitis (Slim et al. 2016). Apart from the potential hepatotoxicity, olanzapine and clozapine are linked to a greater risk of inducing weight gain, as are quetiapine and risperidone to a lesser degree (Martínez-Ortega et al. 2013; Slim et al. 2016), and this could lead to a higher risk of producing NAFLD.
A systematic review in adults on treatment with any type of antipsychotics (AP) reported a median of 32% of patients showing abnormalities in LFT, with 4% of cases being clinically significant. Clozapine was the AP most associated with these abnormalities (Marwick et al. 2012).
In children and adolescents on risperidone, a retrospective study over 5.6 months (Szigethy et al. 1999) as well as prospective studies of up to 1 year with the same sample (Erdogan et al. 2008, 2010; Karaman et al. 2016) showed that risperidone may commonly cause insignificant changes to LFT. In another retrospective study, with data from children and adolescents on olanzapine for a mean of 8 ± 6 months, 59% of patients showed an abnormally elevated value on at least one of the LFTs measured: alanine aminotransferase (ALT), aspartate aminotransferase (AST), or lactate dehydrogenase, whereas those who also took divalproex were associated with greater increases in LFT than those on olanzapine alone (Gonzalez-Heydrich et al. 2003).
Regarding the possible link between abnormal LFT and MetS, a study in the general population performed in children and adolescents (Park et al. 2013) observed that high ALT values within the normal range were associated with MetS in obese as well as normal-weight adolescents. In fact, NAFLD can be considered the hepatic manifestation of MetS (Alterio et al. 2014), and elevated ALT levels, a marker of NAFLD (Fraser et al. 2007).
To the best of our knowledge, there have been no published prospective 1-year follow-up studies examining LFT in AP-naive or quasi-naive children and adolescents on different SGA, and the possible relationship between LFT and MetS in this population.
Thus, the main purpose of our study was to analyze how LFT changed over 1 year follow-up in children and adolescents who were antipsychotic naive or quasi-naive and began using an SGA; and whether there were any differences in LFT between patients using different prescribed SGA. We also focused on the possible relationship between LFT and MetS or being at risk of MetS (AR-MetS) in the same sample.
We hypothesized that during the first months after beginning the SGA treatment there would be a mean transient increase in some LFT, but no significant changes over the first year of treatment. Moreover, we also expected that the number of patients with MetS and AR-MetS would increase during the follow-up and that these patients would have increased LFT.
Methods
Subjects
Four child and adolescent Psychiatry Departments at University Hospitals in Spain recruited the sample. Both inpatients and outpatients attending these facilities during a 2-year period (May 2005–April 2007), who met the inclusion criteria, were invited to participate in the study (for a full description of the study design see Merchan-Naranjo et al. 2012). The inclusion criteria were the following: age between 4 and 17 years at the time of first evaluation, with any psychiatric diagnoses according to Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision (DSM-IV-TR, American Psychiatric Association 2000) criteria, except for eating disorders; and being AP naive (prescribed an AP drug for the first time at baseline) or quasi-naive (having begun any first AP treatment up to 30 days before baseline). Patients who did not come to at least two assessments after baseline during the follow-up were not included in the study. There were no exclusion criteria.
From the whole sample, only patients who continued their SGA treatment during the entire follow-up period with the same single drug were included in this analysis. If a patient switched to a different antipsychotic or another one was added, only the visits before that change were included. Additionally, since most patients were on risperidone, olanzapine or quetiapine, three patients who were on different AP were removed from the analysis (Fig. 1). Thus, the final sample included 216 subjects.
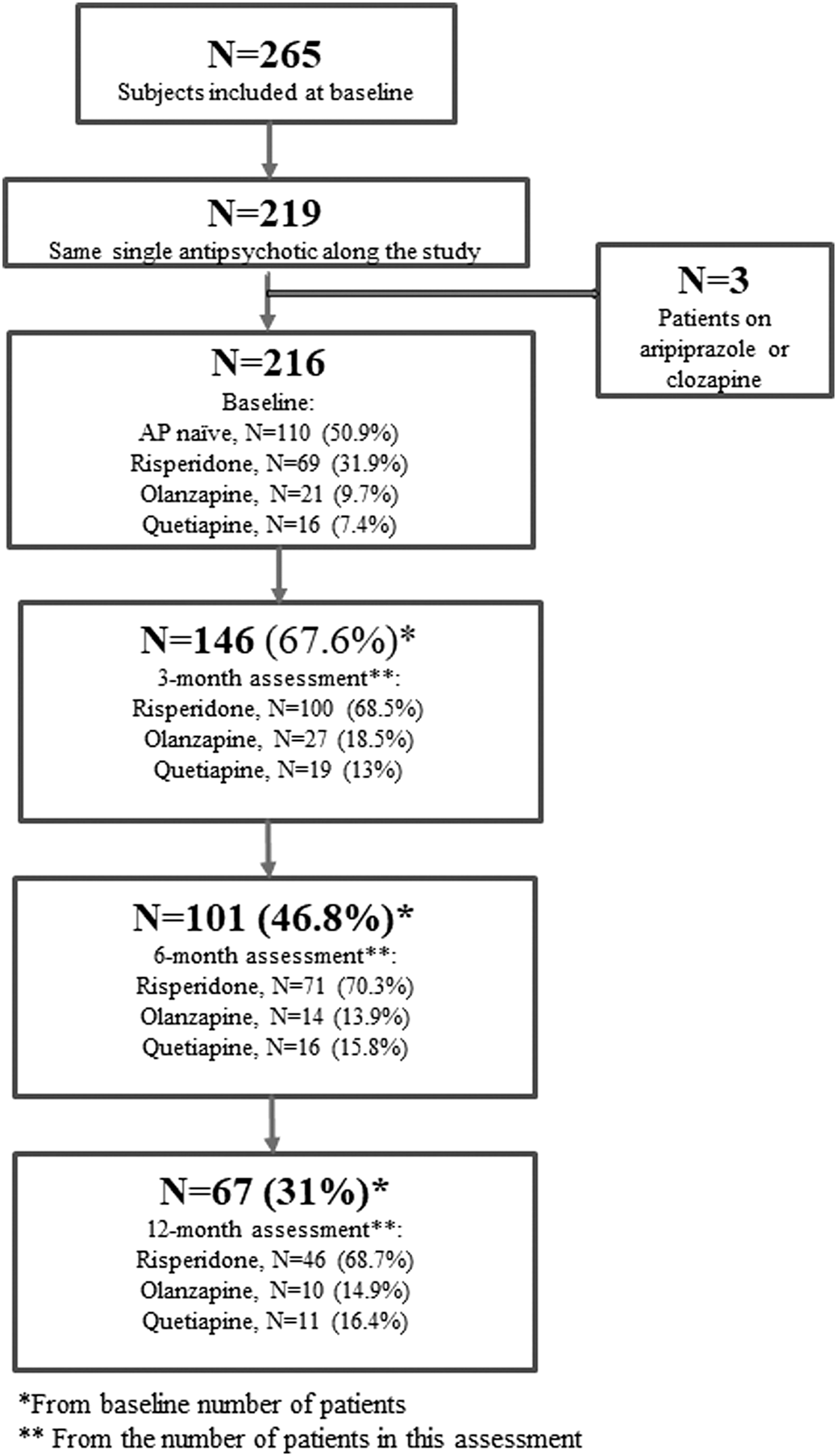
Flowchart of the patients included in the different assessments.
The study was approved by the Ethics Committee of all participating centers. Parents/legal guardians of patients and patients older than 12 years of age gave written informed consent and patients younger than 12 years agreed to participate.
Procedure
There were four assessments during the follow-up: at baseline, and at 3, 6, and 12 months, whereas patients were on the same SGA. In each evaluation, a fasting blood analysis was performed; weight, height, and blood pressure were measured and SGA as well as other pharmacological treatment were registered (drugs, dosage). SGA doses were converted to chlorpromazine equivalents (Andreasen et al. 2010). Family history of obesity was registered by asking parents/legal tutors of patients about each patient's family up to third-degree relatives.
Assessment
Liver function tests
All of the LFT parameters (AST, ALT, alkaline phosphatase [ALP], and total bilirubin [TB]) were measured with molecular absorption with the following analyzers: at Hospital Clínic de Barcelona, with an Advia 2400 chemistry analyzer from Siemens (Siemens Healthcare, Tarrytown, NY); in Hospital Gregorio Marañón, with a Boehringer Mannheim/Hitachi 714 analyzer (Boehringer Mannheim Diagnostics); in Hospital Sant Joan de Déu with an Architect ci82000 analyzer (Abbott Diagnostics, NJ), and in Hospital Niño Jesús with a Cobas c711-Roche (Switzerland). The reference ranges in all hospitals for AST and ALT were <40 IU/L, for ALP 46–116 IU/L, and for TB 0.4–1.2 mg/dL.
Other biochemical parameters
The other parameters were measured using the Boehringer Mannheim/Hitachi 714 automated chemistry analyzer (Boehringer Mannheim Diagnostics) as follows: glucose (Glucose/hexokinase [HK]; Roche Diagnostics, Germany); total cholesterol (Cholesterol/high performance [HP]; Boehringer Mannheim Diagnostics); high-density lipoproteins (HDL)-cholesterol (HDLC3; Roche Diagnostics, Germany); and triglycerides (Tg; Roche Diagnostics, Germany). Low-density lipoproteins (LDL)-cholesterol was calculated using the Friedewald formula (Friedewald et al. 1972).
Height, weight, and blood pressure
Height and weight were measured with a SECA 220 sliding-weight scale in all of the centers during this period. Body weight was measured in kilograms (kg) to the nearest 0.2 kg, wearing light clothes, and no shoes. Body mass index (BMI) calculated as weight in kg/height in m2 (kg/m2) and standardized BMI adjusted for age and sex (zBMI) were also calculated using standard Spanish tables (Sobradillo et al. 2004).
MetS and AR-MetS criteria
MetS was defined according to the National Cholesterol Education Program Adult Treatment Panel III criteria modified by Cook for children and adolescents (Cook et al. 2003), as three of the following: obesity with BMI ≥95th percentile, blood pressure ≥90th percentile, Tg ≥110 mg/dL, HDL cholesterol ≤40 mg/dL, or glucose ≥100 mg/dL. AR-MetS was defined (Fraguas et al. 2008) as BMI ≥95th percentile or BMI ≥85th percentile plus at least one of the following: blood pressure >90th percentile, total cholesterol ≥200 mg/dL, LDL cholesterol >130 mg/dL, HDL cholesterol <40 mg/dL, Tg ≥150 mg/dL, or glucose ≥100 mg/dL.
These criteria were mutually exclusive, and patients were included in only one category based on the severity of their condition.
Diagnoses
At baseline, psychiatric diagnoses according to DSM-IV-TR criteria were made by child and adolescent psychiatrists in each center. Diagnoses were grouped into categories (for a full description of diagnostic categories and AP treatment associated, see Baeza et al. 2014).
Data analyses
For descriptive purposes, continuous variables were expressed as means, standard deviations, and ranges, and categorical variables were expressed as frequencies and/or percentages. The chi-square test (χ 2) was used to compare percentages of discrete variables.
The linear mixed-effects model for longitudinal data (R) was used to analyze whether there were changes in the whole sample (or among patient groups using different SGA) in LFT during the follow-up, and these models were adjusted for age and sex.
To assess the sociodemographic differences between patients that met criteria for MetS, those with AR-MetS, and those with neither (No-AR-MetS), we used analysis of variance (ANOVA) tests if the variable was continuous or χ 2 if it was categorical. Student's t test was used to compare assessments one by one when ANOVA was significant. We also used linear mixed-effects model for longitudinal data to assess the relationship between each LFT at baseline and the outcome (MetS, AR-MetS or No-AR-MetS) during the follow-up.
All tests were two-tailed. Statistical analyses were carried out with the SPSS 18.0 (Statistical Package for the Social Sciences, Chicago) and R statistics version 3.2.1 (
Results
Sociodemographic characteristics, diagnoses, and treatment at baseline
Sociodemographic data, diagnoses, and treatment at baseline are shown in Table 1.
Psychotropic medication could include: anxiolytics/hypnotics, antipsychotics, antidepressants, mood stabilizers, anticholinergics, or stimulants.
Patients on antipsychotics or antipsychotic naive at baseline and any other psychotropic medication at baseline.
Patients on antipsychotics or antipsychotic naive at baseline and any other psychotropic medication at baseline, except for anxiolitics/hypnotics.
SD, standard deviation.
Sample size decreased over the follow-up (Fig. 1) due to patients switching to a new AP (n = 20, 9.3%), adding a new AP (n = 3, 1.4%), or having missing blood analysis results due to technical problems in the laboratory (n = 6, 2.8%). Additionally, 49 (22.7%) patients left the study for medical reasons (mainly, clinical improvement, which led to stopping AP treatment), 14 (6.5%) for treatment noncompliance, and lastly, 55 (25.5%) for failure to continue the follow-up. There were no differences in age, gender, baseline diagnoses, and hospitalization between patients who were excluded or left the study and those who completed it (data not shown).
Evolution of LFT and weight during the follow-up
Table 2 describes the patients who had increased LFT measured in upper limit of normal (ULN) units and Table 3 specifies ALT/AST levels for each patient with an increase in any of the assessments. Mean levels of LFT in the whole sample are described in Table 4.
One case with >3 × ULN.
Six cases with >3 × ULN.
Three cases with >3 × ULN, four cases with >3 × ULN, and one case with >8 × ULN.
Two cases with >3 × ULN, one case with >5 × ULN, and one case with >7 × ULN.
Four cases with >3 × ULN and one case with >5 × ULN.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; TB, total bilurubin; ULN, upper limit of normal.
AP was stopped 9 months after starting due to clinical improvement. Patient did not come to the 12-month assessment because she was not on AP. But another analysis from 2 months later (while taking valproic acid) showed ALT/AST levels of 14/16 U/L.
Abnormal ALT/AST levels are written in bold.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ULN, upper limit of normal; AP, antipsychotics.
Quasi-naive patients on risperidone N = 69, olanzapine N = 21 and quetiapine N = 16.
Patients on risperidone N = 100, olanzapine N = 27, and quetiapine N = 19.
Patients on risperidone N = 71, olanzapine N = 14, and quetiapine N = 16.
Patients on risperidone N = 46, olanzapine N = 10, and quetiapine N = 11.
ALT, alanine aminotransferase; AST, aspartate aminotransferase; ALP, alkaline phosphatase; TB, total bilirubin; AP, antipsychotic; CPZ, chlorpromazine; BMI, body mass index; zBMI, standardized body mass index adjusted for age and gender; SD, standard deviation.
From baseline to 1-year follow-up, ALT, AST, ALP, and TB levels did not display any significant differences. Comparing 3- and 6-month follow-up levels with baseline, only ALT levels showed a significant increase of 8.6 (2.5–14.7) U/L at 6 months (p = 0.005). In the whole sample, weight also increased significantly during the follow-up, with patients gaining a mean of 0.9 (0.8–0.9) kg/month (p < 0.001), whereas BMI and zBMI also increased (p < 0.001).
When we divided the sample by sex, no differences were observed in LFT levels in any of the assessments between male and female patients (data not shown). When examining concomitant psychotropic medication (antidepressants, mood stabilizers, anxiolytic/hypnotics, stimulants, anticholinergic drugs), we observed higher levels of ALT at 6 months in comparison to baseline for patients taking any additional medication (31.5 [17.3–40.7] U/L vs. 19 [1.6–36.4] U/L, p = 0.002). Patients on concomitant psychotropic medication also showed significant increases in both weight (60.3 ± 17.7 kg vs. 54.7 ± 18.2 kg, F = 12.725, p < 0.001), and BMI (22.4 ± 4.2 vs. 21.2 ± 4.1, F = 11.552, p = 0.001), but not zBMI (−0.5 ± 1.4 vs. 0.2 ± 1.4, F = 3.229, p = 0.073).
LFT and weight with the different AP prescribed
LFT and weight differences for each prescribed SGA are shown in Table 4. The three SGA did not show any significant differences in terms of ALT, AST, or TB levels. ALP levels showed a significant increase at 3 months in subjects taking risperidone (mean: 20.4 U/L, p = 0.011); however, these differences were not found in later assessments. The weight increase was significant for each SGA: risperidone being associated with a mean increase of 0.67 (0.56–0.79) kg/month (p < 0.001), olanzapine 0.98 (0.65–1.30) kg/month (p < 0.001), and quetiapine 0.74 (0.45–1.03) kg/month (p < 0.001).
Characteristics of patients with MetS, AR-MetS, or No-AR-MetS at baseline and during the follow-up
Over 1 year of follow-up, the percentage of patients with MetS and ARMetS increased almost four-fold and three-fold, respectively (Table 2). There were no differences in sociodemographic data, prescribed SGA (Table 5) or LFT levels between groups. Patients with MetS at baseline had more first-degree family members who were overweight or obese than the other groups (66.7% compared with 22.2 and 19.4% of AR-MetS and No-AR-MetS, respectively; F = 7.882, p = 0.019), but this difference did not remain significant in later assesments.
Met-S patients: at baseline N = 6 (2.8%), at 3 months N = 6 (4.6%), at 6 months N = 5 (5.6%), and at 12 months N = 6 (10.5%).
AR-Met-S patients: at baseline N = 18 (8.3%), at 3 months N = 28 (21.3%), at 6 months N = 22 (23.2%), and at 12 months N = 16 (23.9%).
No-AR-Met-S patients: at baseline N = 192 (88.9%), at 3 months N = 112 (74.1%), at 6 months N = 74 (71.2%), and at 12 months N = 45 (65.6).
MetS > AR-MetS, p = 0.789 and No-AR-MetS > AR-MetS, p = 0.004.
MetS > AR-MetS, p = 0.069 and MetS > No-AR-MetS, p = 0.018.
Statistically significant results are written in bold.
ALT, alanine transferase; MetS, metabolic syndrome; AR-MetS, at risk for metabolic syndrome; SD, standard deviation.
There was a trend-level group effect in global ALT across time (p = 0.076). Patients with MetS showed higher ALT concentrations (28.9 [18.4–39.4] U/L] than AR-MetS (20.4 [8.5–32.2] U/L], and No-AR-MetS (19.2 [8.4–29.9] U/l).
Discussion
This study found that LFT during 1 year of follow-up in children and adolescents who began using an SGA showed nonsignificant changes, with few patients having ALT or AST levels that were higher than 2× or 3× ULN. ALT levels did significantly increase from baseline to 6 months, although this was transient. Patients showed significant weight increase, with a progressively greater number of patients meeting criteria for MetS and AR-MetS during the follow-up. Although mean ALT levels increased (within the normal range) in patients with MetS compared with those with AR-MetS and No-AR-MetS, differences did not reach statistically significant levels.
LFT have been scarcely reported in children and adolescents on SGA. Safety studies finding no significant LFT changes have been published, but these are not well detailed (Zuddas et al. 2000; Shea et al. 2004). Moreover, there is heterogeneity in reporting abnormal LFT levels (percentage out of normal range, peak or mean levels) (Szigethy et al. 1999; Gonzalez-Heydrich et al. 2003; Erdogan et al. 2008, 2010; Karaman et al. 2016; Matera et al. 2017) and we considered ULN to be the most standardized measure. This measure showed slight increases in ALT or AST levels, whereas we also found that almost 19% of patients had ALP levels 2 × ULN or higher during the follow-up period. Considering that the enzyme ALP also increases with bone growth, due to osteoblast leakage (Loh and Metz 2015), in children and adolescents its increase beyond the normal range does not necessarily reflect the condition of the liver, and this could explain the percentage of patients in our study with higher ALP levels during the follow-up.
Moreover, the enzyme AST, apart from being found in hepatic cells, may also be present in skeletal muscles, the heart, pancreas, brain, etc., and its increase is not a clear sign of liver damage. The enzyme ALT, on the other hand, is most directly linked to liver damage, because it is almost only found in hepatic cells (Gianini et al. 2005). In our study, all patients that had increased ALT levels also showed an increase in AST levels, and this could be linked to hepatocellular damage.
There was a significant increment in ALT levels from baseline to 6 months (within the normal range), which decreased at 12-month assessment. Moreover, there was a significant difference in ALT levels at 6-month assessment between patients on concomitant psychotropic treatment and those not taking any; however, this disappeared at 12 months. A transient increase of some LFT after starting risperidone has been reported prospectively in children and adolescents (Karaman et al. 2016) as well as in adults with different AP (Marwick et al. 2012). The adaptation hypothesis (the development and induction of a state of immunotolerance against the drug or its metabolite) could explain why patients develop only mild abnormalities, which eventually resolve after continued usage of the drug (Dara et al. 2016).
Other studies have found an increase in all LFT levels during follow-up. In prospective studies of children and adolescents on risperidone followed-up for 6 months (Erdogan et al. 2010) and 1 year (Karaman et al. 2016), all LFT levels significantly increased from baseline to endpoint, but stayed within the normal range, with 38.2% and 21% of patients, respectively, showing higher LFT levels that were out of the normal range, and only one case (1%) of ALT 3 × ULN and AST 2 × ULN at 1-year assessment. Recently, in children and adolescents on risperidone, a nonsignificant increase in mean levels of ALT and AST has been reported over a mean follow-up of 7.6 months (Matera et al. 2017). All of the studies stress the importance of routinely monitoring LFT.
When we divided our sample based on the three different SGA prescribed, only patients on risperidone showed significantly increased levels of ALP from baseline to 6-month assessment. The other parameters studied did not significantly differ between the SGA. Thus, we did not find any significant differences in LFT levels despite the structural differences between the three SGA and their different mechanisms acting on the liver (cholestasis, liver cytolysis, or NAFLD). For instance, both olanzapine and quetiapine are diazepines, and have a structural overlap with chlorpromazine, a drug which tends to be associated with a greater risk of hepatic injury (Slim et al. 2016). We have not found any other long-term reports in children and adolescents, which compared the effects of different SGA on LFT.
Weight significantly increased in the whole sample during the follow-up, and also when we divided the sample according to the different SGA. Weight gain with SGA in children and adolescents has been widely reported (Arango et al. 2014; Ronsley et al. 2015; Baeza et al. 2017; and for review, Martínez-Ortega et al. 2013; Almandil et al. 2013).
Moreover, we found that patients on treatment concomitant to SGA significantly gained more weight during the follow-up than those only on SGA. AP polypharmacy (Maayan and Correll 2011) as well as other concomitant treatment (Correll 2007; Goldstein et al. 2008) have been associated with a higher risk of obesity in children and adolescents, although there are some controversial data (Martin et al. 2000; de Hoogd et al. 2012). Since our study did not include patients with more than one AP, it is possible that the concurrent usage of other treatments such as mood stabilizers could have caused the greater weight increase in patients with concomitant treatment. Antidepressants (selective serotonin reuptake inhibitors and serotonin and norepinephrine reuptake inhibitors) were not linked to weight gain in children and adolescents in a review conducted by Reekie et al. (2015), but other authors have not confirmed this (Mansoor et al. 2013). Benzodiazepines have been found to be weight neutral (Hasnain and Vieweg 2013).
We also observed in our sample an increased number of patients who met criteria for MetS (from 2.8% to 10.5%) during the 12 months of follow-up. Studies of MetS in children and adolescents are mainly in the general population (for review, see Graf and Ferrari 2016). There have been few prospective studies related specifically to MetS in children and adolescents on SGA, among them Arango et al. (2014), Calarge et al. (2009), Correll et al. (2009), Jensen et al. (2017), and Matera et al. (2017).
Arango et al. (2014) reported in children and adolescents on risperidone, olanzapine, or quetiapine, an increased number of patients with MetS from baseline (2.5% of the sample) to 6-month assessment (7.9%). In 99 patients on risperidone for an average of 2.9 years.
Calarge et al. (2009) found that children with excessive weight were 12 times more likely to have at least one laboratory metabolic abnormality and 7 times more likely to have at least one criterion of MetS compared with lean subjects. However, only one subject met criteria for MetS.
Correll et al. (2009) in adolescents on risperidone, olanzapine, quetiapine, or aripiprazole with a mean of 10.8 weeks of follow-up reported significant weight gain with each SGA, but different metabolic profiles (olanzapine and quetiapine associated with higher cholesterol and triglyceride levels, and risperidone with high triglyceride levels, whereas no metabolic changes were observed with aripiprazole). About 6.5% patients on quetiapine met criteria for MetS, as did 2.5% of patients on olanzapine or aripiprazole, whereas none of the patients on risperidone reached this threshold; although, there were no significant differences between the groups. In adolescents with a first episode of psychosis (FEP), it was reported that FEP subjects had significantly greater waist circumference and lipid abnormalities than matched controls, regardless of AP exposure. Moreover, in FEP adolescents the elevated metabolic risk has been found to predate exposure to AP (Jensen et al. 2017).
Using ultrasounds, Matera et al. (2017) have described a tendency for the constitution of liver parenchyma to change in children and adolescents on risperidone for a mean of 7.6 months, whereas mean values of waist circumference, BMI, zBMI, total cholesterol, and prolactin increased.
Patients with MetS at baseline (while they were AP naive or <30 days on AP) had a greater number of first-degree family members who were overweight/obese than the other groups. This characteristic among family members has been widely reported in children and adolescents without AP treatment (for review, Nielsen et al. 2015) and obesity has been found to be heritable (Locke et al. 2015). However, we did not find this association in our sample when patients were already on SGA (after the baseline assessment).
Regarding AR-MetS in our study, there was also an almost three-fold increase up to 12-month follow-up. Interestingly, our AR-MetS patients were younger than MetS and No-AR-MetS in all of the assessments, although only at 6 months was this statistically significant. This signals the importance of monitoring metabolic parameters at any age, even in younger patients on SGA, since it can help alter the trajectory toward cardiovascular disease and type 2 diabetes through early recognition and intervention to reduce cardiometabolic risk (Eapen et al. 2013).
Our study found that mean ALT levels were higher (within the normal range) in patients who met MetS criteria compared with those with AR-MetS and No-AR-MetS, but the difference was not statistically significant. No other prospective studies have been found regarding the possible link between LFT and MetS in children and adolescents on different AP. However, in the general population, Park et al. (2013) reported that subjects in the upper tertile of ALT levels (within the normal range) had a higher risk of all the components of MetS. The authors concluded that ALT levels, in addition to BMI, might be a marker for early detection of MetS. In adults, a statistically significant correlation between weight gain and liver enzyme elevation was found (Rettenbacher et al. 2006). In this study, patients on SGA that had gained at least 7% of their baseline body weight during the 13-week follow-up showed significantly greater increases in transaminases compared with those with <7% weight gain. However, we could find no studies in the literature examining the link between MetS and LFT in adults on AP.
Limitations and strengths
There are several limitations to our study: (1) High attrition, which reduced the sample size during the follow-up, limited the statistical power to identify differences between SGA; (2) The naturalistic methodology, which yielded results that cannot be compared with randomized or controlled studies, included patients with comorbid pathologies independent from their psychiatric disorder, although, at the same time, this sort of methodology could provide more generalizable results that are similar to clinical practice; (3) Patients'diagnoses were registered from clinical records and not systematically assessed with a structured interview; (4) The only way to measure adherence to treatment was the testimony of parents/legal tutors, and we could not measure AP levels in all patients; (5) Family history of obesity was assessed by asking parents/legal tutors about each patient's relatives, and this may have created a bias and underreporting of cases.
Moreover, we did not compare the different assays to measure the biochemical parameters between the different centers, although all centers work under the same external quality control schemes and fulfill all quality criteria established by the Spanish Society of Clinical Chemistry and Laboratory Medicine; Liver function was evaluated with blood tests, and imaging tests (i.e., ultrasounds) were not performed; We did not use a wall-mounted stadiometer to measure height, although this method is considered the gold standard for such measurements; and due to the number of variables registered in the study and the number of multiple comparisons performed, it is possible that there is a type 1 error in some of the comparisons, although this is an observational and exploratory study.
Additionally, it should be taken into account that this study was conducted from 2005 to 2007 in Spain. At that time, the SGA approved by the Agencia Española del Medicamento y Productos Sanitarios (Spanish Agency of Medicines and Medical Devices) to be used in Spain were: risperidone, olanzapine, quetiapine, clozapine, and ziprasidone, although most of these were being used off-label in children and adolescents (Baeza et al. 2014). Aripiprazole was not avalaible in Spain until 2005, and its use in children and adolescents did not begin until even later, whereas in the United States of America it had been on the market since 2002.
Some of the strengths of the study include its prospective design, with 12 months of follow-up; the sample's homogeneity, with AP-naive or quasi-naive children and adolescents, and the repeated measurements of laboratory parameters during the follow-up.
Conclusions
We did not find significant changes in LFT during 1 year of follow-up in children and adolescents who started an SGA. Although there were a few cases of patients with ALT or AST levels that were higher than two or three times ULN at 3 and 6 month assessments, none of these was clinically significant and all returned to normal in later assessments. From baseline to 6 months, ALT levels significantly increased in the whole sample, whereas ALP significantly increased only in risperidone patients. Patients all showed significant weight gain, with a progressively greater number of patients meeting criteria for MetS and AR-MetS during the follow-up. Mean ALT levels increased in patients with MetS and AR-MetS, although they remained within the normal range and did not reach significant levels.
These results suggest that SGA use does not seriously affect liver function in children and adolescents. Nevertheless, considering the increased use of SGA in this population, the potential consequences of MetS and AR-MetS on LFT should be further studied.
Clinical Significance
This study helps confirm the 1-year safety of some SGA in LFT in children and adolescents. Despite significant discrete increases in ALT in the whole sample, and in ALP among risperidone patients in some evaluations, no clinical symptoms were reported. However, since increases in LFT tend to be asymptomatic, it is important to monitor them. Moreover, this study helps broaden awareness of the possible link between MetS and AR-MetS and higher ALT levels within the normal range. Thus, although these findings need to be confirmed, they suggest that increased ALT levels in a child or adolescent on SGA could be clinically significant as a sign of MetS or AR-MetS. The recommended frequency of LFT assessments is still not well established, although at baseline and at 3 months, and later annually has been suggested (Correll 2008). In at-risk patients with significant weight gain, measuring ALT regularly could be helpful.
Footnotes
Acknowledgments
The authors would like to thank the Center for Biomedical Research in the Mental Health Network (CIBERSAM), Madrid (Spain), Mr. R. Borras for his statistical advice, and Mr. A.D. Pierce for his English editorial assistance.
Disclosures
I.B. has received honoraria and travel support from Otsuka-Lundbeck and Janssen, research support from Fundación Alicia Koplowitz, and grants from the Spanish Ministry of Health, Instituto de Salud Carlos III. R.C.-E. has a grant from the Spanish Ministry of Health, Instituto de Salud Carlos III, and has received travel support from Shire. J.A.A. has been a consultant to or has received honoraria or grants from Eli Lilly, Shire, Janssen Cilag, Spanish Ministry of Health, Instituto de Salud Carlos III, Agència d'Informació, Avaluació i Qualitat en Salut (AIAQS), and Fundación Alicia Koplowitz. D.M.-S. has received grants from Instituto de Salud Carlos III and support from Otsuka for attending some conferences. C.A. is a consultant for Astra-Zeneca, Bristol Myers Squibb, Janssen-Cilag, Pfizer, and Servier; has received grants/support from the Spanish Ministry of Health, Instituto de Salud Carlos III, the European Comission, Fundación Alicia Koplowitz, Astra-Zeneca, and Bristol Myers Squibb. J.C.-F. has been a consultant for Eli Lilly and has received grants from the Spanish Ministry of Health, Instituto de Salud Carlos III, the European Comission, and Fundació La Marató de TV3. E.d.l.S., J.M.-N., D.I., M.C.M.-C., P.A., and P.R.-L. declare no conflicts of interest.