
Abstract
Objective:
To assess the risk of incident cardiovascular events that led to hospitalizations or emergency department visits following atypical antipsychotic (AAP) treatment initiation in youth according to dose, duration of use, and concomitant use of leading psychotropic medication classes.
Methods:
We used computerized Medicaid claims to conduct a retrospective cohort study of youth (5–20 years) who initiated AAP treatment. AAP use was operationalized in a time-dependent manner according to current vs. former use, average daily dose (in risperidone dose equivalents), and duration of use. In a secondary analysis, concomitant use of (1) stimulants and (2) serotonin-reuptake inhibitors (SSRI/SNRIs) with AAPs was also assessed. To account for confounding, disease risk score methodology was used in discrete time failure models.
Results:
There were 74,700 youth who initiated AAP treatment (average follow-up = 24.8 months). During follow-up, the risk of cardiovascular events was significantly greater during current than former AAP use (RR = 1.55, 95% CI = 1.09–2.21). Furthermore, for current users of AAPs, the risk of cardiovascular events intensified with average daily dose (RR = 2.04, 95% CI = 1.11–3.77 for >3.75 mg/day vs. ≤1.25 mg/day). The risk of cardiovascular events did not significantly differ according to duration of AAP use. In AAP-treated youth, concomitant SSRI/SNRI use was associated with an increased risk of cardiovascular events (RR = 1.61, 95% CI = 1.01–2.57). By contrast, stimulant use concomitant with AAPs was not significantly associated with an increased risk of cardiovascular events.
Conclusions:
In publicly insured U.S. youth, current AAP use was associated with an increased risk of incident cardiovascular events, which intensified with increasing dose and with concomitant SSRI/SNRI use. Prudent interpretation of these findings suggests that further research is needed to identify youth subpopulations with the greatest risk of developing AAP treatment-emergent cardiovascular events.
Introduction
W
Off-label treatment—for indications that are not approved by the U.S. Food and Drug Administration—accounts for much of this increase. Specifically, attention-deficit/hyperactivity and other behavioral disorders such as conduct disorder now constitute the largest proportion of youth treated with AAPs (Crystal et al. 2009; Penfold et al. 2010; Matone et al. 2012; Burcu et al. 2014). While antipsychotic use has increased dramatically in both privately and publicly insured youth (Crystal et al. 2009; Olfson et al. 2012a), the increase is more prominent in Medicaid insured (i.e., publicly insured) youth, with a five- to sixfold greater prevalence of use (Crystal et al. 2009). The increase in AAP use has occurred in the face of mounting reports of cardiometabolic adverse events (Correll et al. 2009).
The results from meta-analyses of randomized clinical trials and population-based studies show that AAP-treatment emergent abnormalities in youth include hyperlipidemia, hyperglycemia, type 2 diabetes, disturbances in prolactin levels, and weight gain—for which children are at greater risk (Safer 2004; Calarge et al. 2009a, 2009b; Correll et al. 2009; Andrade et al. 2011; Cohen et al. 2012; Bobo et al. 2013; Safer et al. 2013; Rubin et al. 2015; Sohn et al. 2015; Burcu et al. 2017a). In addition to these risks, an increased risk of serious cardiovascular events was also reported in population-based studies—mostly in adults (Douglas and Smeeth 2008; Ray et al. 2009; Lin et al. 2014; Wu et al. 2015). In these population-based adult studies, AAPs have been linked to stroke, acute myocardial infarction, ventricular and other arrhythmias, and sudden cardiac death (Douglas and Smeeth 2008; Ray et al. 2009; Lin et al. 2014; Wu et al. 2015). Several AAP medications are associated with potassium ion channel inhibition and prolongation of QTc interval—a surrogate measure for the risk of torsades de pointes (Haddad and Anderson 2002; Kongsamut et al. 2002; Harrigan et al. 2004; Roden 2004). However, much less is known about adverse cardiovascular risks in youth populations following AAP use.
We conducted a large retrospective cohort study of Medicaid-insured youth from four geographically diverse states who initiated treatment with AAPs, and we assessed the risk of incident cardiovascular events identified from hospitalizations and emergency department visits. We examined the risk of cardiovascular events according to average daily AAP dose and duration of AAP use. Furthermore, the majority of AAP prescriptions in US youth involve a coprescription of other psychotropic medication classes, mainly stimulants or selective serotonin reuptake inhibitor/serotonin–norepinephrine reuptake inhibitors (SSRI/SNRIs) (Fontanella et al. 2014; Kreider et al. 2014; Burcu et al. 2016). Thus, in a secondary analysis, we also assessed the risk of cardiovascular events according to the concomitant use of stimulants or SSRI/SNRIs with AAPs.
Methods
Data source
This retrospective cohort study utilized computerized data from the 2004–2009 Medicaid administrative claim files (Medicaid Analytic eXtract [MAX] data) from four large geographically diverse states, namely California, Florida, Illinois, and New Jersey (Medicaid, “MAX general information”; Ray and Griffin 1989). Administrative Medicaid claims data are often used in population-based studies of adverse drug events and consist of the person-level enrollment files, claim-level files for inpatient hospital, outpatient and physician services, and prescription drug dispensings (i.e., filled prescriptions). The enrollment files provide data on sociodemographic characteristics and monthly enrollment status for each Medicaid enrollee. An encrypted identification number was assigned to each Medicaid enrollee to link enrollment files to inpatient, outpatient, and prescription drug claims. The inpatient and outpatient claims files provide data on services rendered during inpatient and outpatient medical encounters, including service beginning and end dates as well as the ICD-9-CM (International Classification of Diseases and Related Health Problems, Ninth Revision, Clinical Modification) diagnosis codes and procedure codes (e.g., CPT [Current Procedural Terminology] and ICD-9-CM procedure codes). In the prescription drug claim files, the dispensing date, days of supply, strength, and national drug code (NDC) information were available for each dispensed medication to youth. The study was reviewed and approved by the University of Maryland Institutional Review Board.
Study population
The study cohort comprised 74,700 youth between ages 5 and 20 who recently initiated treatment with an oral form of AAP medication (aripiprazole, clozapine, olanzapine, paliperidone, quetiapine, risperidone, or ziprasidone). The AAP treatment initiation date served as the index date for cohort entry. A “new-user” design approach was applied to assemble youth who initiated treatment with AAPs by requiring no antipsychotic (conventional or atypical) medication use during 365 days before the index date (McMahon and MacDonald 2000; Ray 2003). Additional cohort selection criteria were applied to define the final study cohort (Fig. 1).
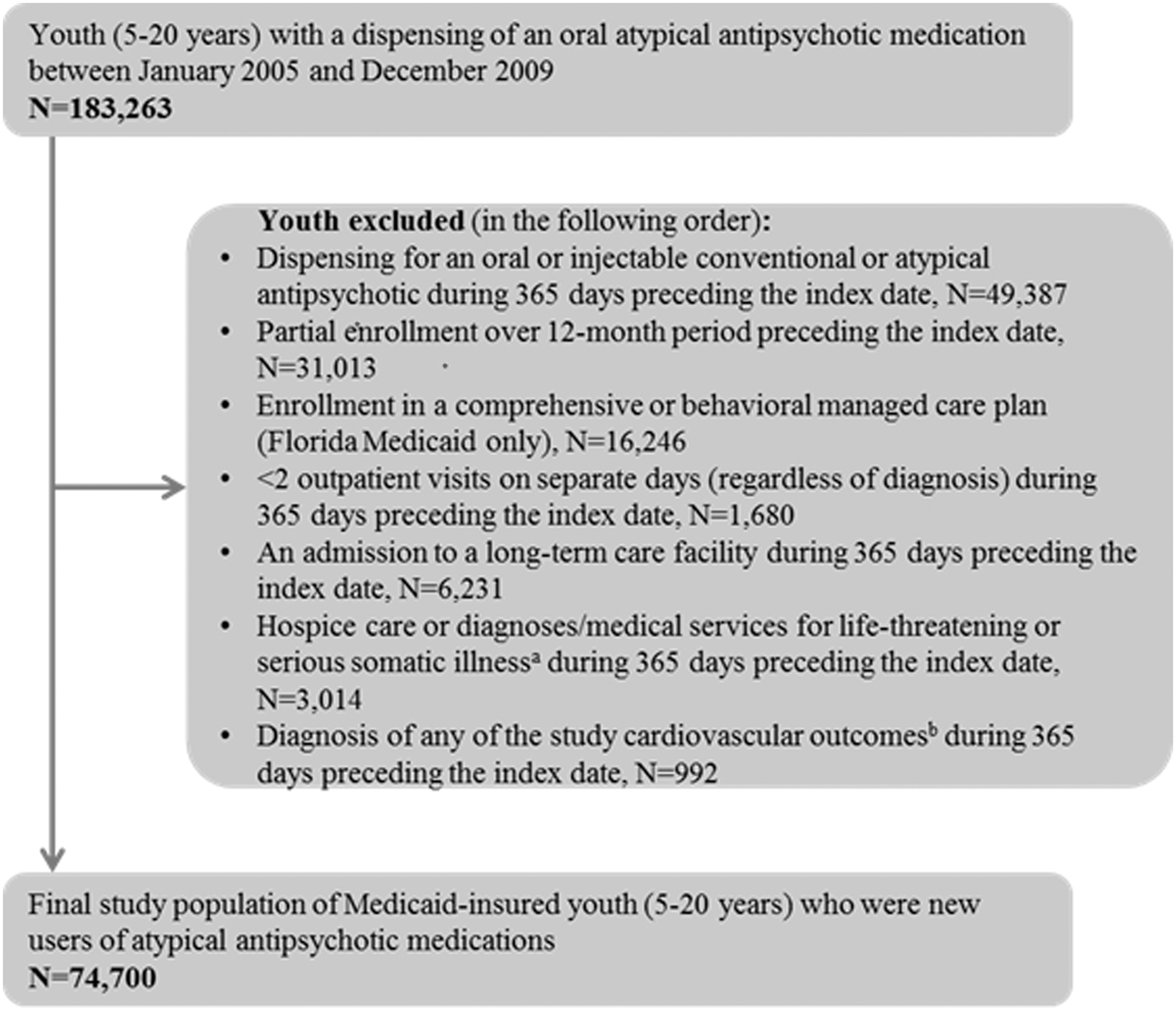
Flowchart for the study cohort of Medicaid-insured youth (5–20-year-olds) who were new users of atypical antipsychotic medications, 2005–2009. aLife-threatening or serious somatic conditions included sickle cell disease, cystic fibrosis, cerebral palsy, cancer, human immunodeficiency virus (HIV) infection, organ transplant, dialysis/end stage renal disease, respiratory failure, aplastic anemia, congenital immune deficiencies, Down syndrome, other lethal chromosomal anomalies, fatal metabolic diseases. bAcute myocardial infarction, stroke, ventricular arrhythmia, cardiac arrest, respiratory arrest, aortic or thoracic aneurysm, transient cerebral ischemia, ischemic heart disease, heart failure, cardiomyopathy, angina, and hypertensive disease.
Continuous enrollment for 12 months before the index date was required to ensure the availability of adequate data to assess prescription drug use and medical diagnoses. We excluded youth who were enrolled in Florida Medicaid Managed Care Programs because of concerns over the quality and completeness of claim records from the Florida Medicaid Managed Care Data (Byrd and Dodd 2012, 2013). To ensure active interaction with the healthcare system, youth who had less than 2 outpatient visits (on separate days) in the year before the index date were excluded. In addition, youth were excluded if they had an admission to a long-term care facility or hospice care or if they were diagnosed with a life-threatening or serious somatic illness during 365 days preceding the index date (Supplementary Appendix S1; Supplementary Data are available online at
Cardiovascular events
The primary study outcome was the incidence of adverse cardiovascular events following treatment initiation with AAP medications. We adopted an approach from previously published population-based studies in youth to define cardiovascular events (Winterstein et al. 2007; Olfson et al. 2012b). Cardiovascular events were expressed as a composite outcome; they were defined by an inpatient stay or an emergency department visit with a primary or secondary diagnosis of acute myocardial infarction (ICD-9-CM 410.x), stroke (ICD-9-CM 430.x, 431.x, 433.x, 434.x, and 436), ventricular arrhythmia (ICD-9-CM 427.1, 427.4, 427.41, 427.42), cardiac arrest (ICD-9-CM 427.5), respiratory arrest (ICD-9-CM 799.1), aortic or thoracic aneurysm (ICD-9-CM 441.0, 441.1), transient cerebral ischemia (ICD-9-CM 435.x), ischemic heart disease (ICD-9-CM 411.8), heart failure (ICD-9-CM 428.x), cardiomyopathy (ICD-9-CM 425.x), or angina (ICD-9-CM 413.x). The composite outcome also included severe/serious hypertension that led to hospitalizations or emergency department visits defined as an inpatient or emergency department claim with a primary diagnosis of hypertensive disease (ICD-9-CM 401.x-405.x).
As described by Olfson et al. (2012b), these cardiovascular events have established validity in adults (Goldstein 1998; Tirschwell and Longstreth 2002; Heckbert et al. 2004; Kiyota et al. 2004; Hennessy et al. 2010; Leonard et al. 2011; Tamariz et al. 2012). In addition, acute myocardial infarction and stroke have been previously validated specifically in US youth, with positive predictive value of >0.90 (Cooper et al. 2011). Moreover, in our study, we focused on diagnostic codes derived from hospitalizations and emergency department visits and did not use diagnoses from outpatient physician encounters. Diagnoses from outpatient office visits are more likely to be subject to misclassification bias due to services rendered for monitoring or diagnostic work-up (Strom 2013). Furthermore, to enhance the validity of cardiovascular events from hospitalizations and emergency department visits, we also conducted a post hoc analysis wherein only the primary diagnoses were used to define all the aforementioned inpatient or ED-related cardiovascular events.
The study cohort was followed until incident cardiovascular events, the 21st birthday, end of study (i.e., December 31, 2009), or end of continuous enrollment in Medicaid, whichever came first.
AAP use
As the study was nested in a cohort of youth who initiated treatment with AAPs, there were no AAP nonusers in the study. In each month of follow-up, AAP use was categorized as either current or former use in a time-dependent manner. The comparison of current to former users rather than to nonusers attempted to mitigate potential unmeasured confounding, as current AAP users are more comparable to former AAP users than nonusers with respect to clinical characteristics associated with AAP use (Ray et al. 2004).
The monthly use status was considered current if there were days of supply available [allowing a 30-day lag for carry-over effects (Cleophas 1993)] in the month of follow-up. Otherwise, AAP use was considered former. We also conducted a sensitivity analysis by not allowing the 30-day lag to account for carryover effects.
During follow-up, we also calculated average daily AAP dose as well as cumulative duration of AAP use (in days). Both average daily AAP dose and cumulative duration of AAP use were measured in a time-dependent manner per person in each month of follow-up. The average daily dose was estimated as total AAP dosage dispensed (in risperidone equivalents) divided by duration of AAP use. The dose equivalence conversion factors for AAPs were adopted from previously published studies (Lehman and Steinwachs 1998; Woods 2003; Meltzer et al. 2008; Bobo et al. 2013; Burcu et al. 2017a) (Supplementary Appendix S2). The cumulative duration of AAP use was estimated as the sum of total days of supply available beginning from the index date.
Analysis
All statistical analyses were conducted using SAS version 9.3 (SAS Institute, Inc., Cary, NC). We used discrete time failure models to estimate the incidence of cardiovascular events. The unit of analysis was person-months. Compared to the traditional Cox proportional hazard regression models, these discrete time models provide computational efficiency as well as practical advantages, especially when there are several time-varying exposure groups (Prentice and Gloeckler 1978; D'Agostino et al. 1990; Allison 2010).
To adjust for confounding, we utilized the disease risk score methodology using the Miettinen full-cohort approach (Miettinen 1976; Arbogast and Ray 2009, 2011; Glynn et al. 2012; Burcu et al. 2017b). Similar to the propensity score, the disease risk score is a summary confounder score that attempts to help build parsimonious models (and to improve the performance of the models) especially when there is a large number of study covariates. The disease risk score in this study was estimated as the probability of incident cardiovascular events conditional on study covariates. The study covariates included psychiatric, cardiovascular, and other clinical characteristics, sociodemographic, and administrative characteristics, as well as healthcare utilization characteristics (Supplementary Appendix S3). Rather than adjusting for all the study covariates, the final regression models were adjusted only for the estimated disease risk score, which was expressed as percentile rank groups (Supplementary Appendix S4), and time from the index date.
First, we assessed the risk of incident cardiovascular events in current vs. former AAP users. Subsequently, in current AAP users only, we assessed the risk of cardiovascular events according to (1) average daily AAP dose and (2) duration of AAP use. In a sensitivity analyses, we excluded youth who had a diagnosis of any cardiovascular condition or who had a dispensing of any cardiovascular medications in the year before the index date.
Also, since stimulants and SSRI/SNRIs were the leading psychotropic medication classes used concomitantly with AAPs, we conducted a secondary analysis to assess the risk of cardiovascular events according to stimulant or SSRI/SNRI use concomitant with AAPs. The use of stimulants and the use of SSRI/SNRIs were categorized as current/former/nonuse in each month of follow-up. In these secondary analyses, because stimulant or SSRI/SNRI use became main exposure variables (rather than study covariates/confounding variables), the disease risk scores were recalculated for the study cohort accordingly. In examining the risk of cardiovascular events according to use of stimulants or SSRI/SNRIs concomitant with AAPs, additional sensitivity analyses were conducted by excluding youth who had usage of stimulants or SSRI/SNRIs in the year before AAP treatment initiation to attenuate prevalent user bias (Ray 2003).
Results
Characteristics of youth who initiated treatment with AAPs
The study population included 74,700 youth (5–20 year olds) who initiated treatment with AAPs between 2005 and 2009 (Table 1). A majority of the study cohort was between ages 5 and 14 (67.7%), male (63.3%), non-white (55.3%), eligible for Medicaid coverage due to low family income, that is, TANF/CHIP (55.8%), and enrolled in fee-for-service programs (57.6%). There was at least one clinician-reported psychiatric diagnosis in 92.1% of the study cohort. Attention-deficit hyperactivity disorder (42.3%), depressive disorders (34.7%), and disruptive behavioral disorders (29.4%) were the leading clinician-reported psychiatric diagnostic groups. More than half of the study cohort (56.7%) had a psychiatric medication use before initiating treatment with AAPs, most commonly, stimulants (34.4%) and antidepressants (24.9%). SSRI/SNRIs were by far the most commonly used antidepressant subclass.
Other (race/ethnicity) includes youth of Asian, Native Hawaiian, or other Pacific Islander race/ethnicity, and youth with more than one race or unknown race/ethnicity.
SSI, Supplemental Security Income (youth with disabilities); TANF/CHIP, Temporary Assistance for Needy Families/Children's Health Insurance Program (youth eligible for Medicaid based on low family income); PDD/ID, pervasive developmental disorder/Intellectual disability; ADHD, attention-deficit/hyperactivity disorder; SSRI/SNRI, selective serotonin reuptake inhibitor/serotonin–norepinephrine reuptake inhibitor; TCA, tricyclic and other related cyclic antidepressant.
AAP use and the risk of incident cardiovascular events
Following the initiation of treatment with AAPs, the average follow-up was 24.8 months (median = 22.0 months, interquartile range [IQR] = 10.0–38.0 months) and the average duration of AAP use was 293.5 days (median = 151.0 days, IQR = 60.0–401.0 days) (data not shown). There were 142 incidents of cardiovascular events that resulted in hospitalization or emergency department visit (Table 2). The absolute risk for incidents of cardiovascular events was greater during current than former AAP use (0.84 vs. 0.67 per 10,000 person-months of follow-up). Compared with former use, current use of AAPs was associated with a 55% increased risk of cardiovascular events (relative risk [RR] = 1.55, 95% Confidence Interval [CI] = 1.09–2.21). Furthermore, in current users of AAPs, the risk of cardiovascular events intensified with increasing average daily dose, with a RR of 2.04 (95% CI = 1.11–3.77) for >3.75 mg/day compared with ≤1.25 mg/day (in risperidone dose equivalents). However, in current AAP users, the risk of cardiovascular events did not significantly differ according to the duration of AAP use.
The estimates for the absolute risk per 10,000 person-months represent unadjusted absolute risk estimates.
Adjusted for disease risk score (expressed as percentile ranks) and time from cohort entry (i.e., follow-up month).
Average daily dose was calculated in risperidone dose equivalents.
In a post hoc analysis, when only the primary (not secondary) diagnoses from inpatient or emergency department claims were used to define the study outcome, there were 114 incident cases of cardiovascular events. In that post hoc analysis, the risk of incident cardiovascular events also intensified with increasing average daily dose (RR = 2.17, 95% CI = 1.11–4.25 for >3.75 mg/day compared to ≤1.25 mg/day), but did not significantly differ according to the duration of AAP use. The findings were also similar in the following sensitivity analyses: (1) when the 30-day lag was not used to allow for AAP carryover effects or (2) when youth were excluded if they had a diagnosis of any cardiovascular condition or had a dispensing of any cardiovascular medication in the year previous to the index date (Supplementary Appendix S5).
Concomitant use of leading psychotropic medication classes and the risk of incident cardiovascular events
In AAP-treated youth, concomitant use of SSRI/SNRIs (RR = 1.61, 95% CI = 1.01–2.57) was associated with an increased risk of incident cardiovascular events (Table 3). The increased risk of cardiovascular events associated with SSRI/SNRI use concomitant with AAPs also remained elevated when youth with SSRI/SNRI use before the index date were excluded (RR = 1.83, 95% CI = 1.06–3.15) (Supplementary Appendix S5). By contrast, stimulant use concomitant with AAPs (RR = 0.76, 95% CI = 0.44–1.29) was not significantly associated with an increased risk (Table 3). There was also no increased risk of cardiovascular events associated with concomitant use of stimulants with AAPs (RR = 0.79, 95% CI = 0.33–1.88) when youth with stimulant use before the index date were excluded (Supplementary Appendix S5).
The estimates for the absolute risk per 10,000 person-months represent unadjusted absolute risk estimates.
Adjusted for disease risk score (expressed as percentile ranks) and time from cohort entry (i.e., follow-up month).
SSRI/SNRIs, selective serotonin reuptake inhibitor/serotonin–norepinephrine reuptake inhibitors.
Discussion
In a large retrospective cohort study of Medicaid-insured youth who initiated treatment with AAP medications, we found that the risk of incident cardiovascular events was significantly greater during current than former AAP use. Furthermore, among current AAP users, the risk of cardiovascular events intensified significantly with the average daily dose but not with the duration of AAP use. Finally, in AAP-treated youth, concomitant use of SSRI/SNRIs was associated with an increased risk of cardiovascular events. By contrast, stimulant use concomitant with AAPs was not significantly associated with an increased risk of cardiovascular events.
To our knowledge, this is the first population-based study in youth that assesses the risk of adverse cardiovascular events that led to hospitalizations or emergency department visits following treatment initiation with AAPs. In our study, cardiovascular events were assessed from hospitalizations and emergency department visits to reflect on the seriousness of the events and to avoid outpatient visit claims that may be related to monitoring or diagnostic work-up. Nevertheless, our findings are consistent with a previous study that compared 4140 youth treated with antipsychotics (conventional or AAPs) to a random sample of 4500 youth not treated with psychotropic medications with respect to the receipt of a cardiovascular diagnosis (McIntyre and Jerrell 2008). In that study, antipsychotic use was associated with an increased risk of youth being diagnosed with cardiovascular disorders (McIntyre and Jerrell 2008). While pediatric data from population-based studies are scarce, there are noteworthy data from short-term clinical studies in youth showing substantial increases in cardiometabolic parameters following AAP use. For instance, in a small cohort of 338 children and adolescents who were new users of AAPs, substantial elevations were observed in weight, non-high-density lipoprotein (HDL) cholesterol, and triglycerides over a median of 11 weeks of follow-up (Correll et al. 2009).
Dose and duration response findings
There are no published population-based reports in youth that assessed the risk of cardiovascular events according to dose and duration of AAP use. However, our finding that the cardiovascular risk increases with increasing AAP dose mirrors findings from adult studies. For example, in a large cohort of Medicaid-insured adults, current users of AAPs, compared with nonusers, had a significantly increased risk of cardiac death, which increased significantly with increasing dose (Ray et al. 2009). In another study of adults that used a case-crossover design, AAP use was associated with 2.74-fold increased risk of myocardial infarction (compared with nonuse), which also increased with increasing dose (Lin et al. 2014).
With respect to the duration-response findings in our study, the risk of cardiovascular events did not increase with increasing duration of AAP use—also consistent with several studies in adults. For example, the increased risk of myocardial infarction in AAP-treated adults was significantly greater during early periods of treatment (Lin et al. 2014). In a self-controlled case series study, the use of AAPs was associated with a 2.32-fold increased risk of stroke, which was also more apparent during early course of treatment (Douglas and Smeeth 2008). In another study, the risk of ventricular arrhythmia or cardiac death was greater in adults receiving short-term antipsychotic treatment compared with those receiving long-term treatment (Wu et al. 2015). The absence of an increased risk of cardiovascular events with the increasing duration of AAP use can be explained in two ways. In one, an early experience of adverse cardiovascular symptoms following AAP initiation may result in treatment discontinuation, thereby potentially eliminating susceptibles in long-term treatment. Second, physiological adaptation to the drug-induced cardiovascular effects may develop over the course of AAP treatment.
Concomitant use of SSRI/SNRIs or stimulants
Concomitant use of antidepressants or stimulants with AAPs increased substantially in the past decade among Medicaid-insured youth (Kreider et al. 2014). In current AAP users, we observed a significantly increased risk of cardiovascular events with concomitant use of SSRI/SNRIs but not with concomitant use of stimulants. Several AAP medications are metabolized by the cytochrome P-450 (CYP) enzyme system, and several SSRI/SNRI medications are potent inhibitors of CYP enzymes (Sproule et al. 1997; Spina et al. 2008; Kennedy et al. 2013). Concomitant use of SSRI/SNRIs with AAPs may therefore increase serum concentrations of AAPs, which may in turn increase AAP-treatment emergent cardiovascular events (Kennedy et al. 2013). In addition, between 2011 and 2013, FDA issued safety warnings for three serotonin reuptake inhibitors (i.e., fluoxetine, citalopram, and escitalopram) based on several case reports of abnormal heart rhythms, QTc prolongation, and ventricular arrhythmia associated with the use of these antidepressant agents (United States Food and Drug Administration 2011, 2012, 2013).
The risk of cardiovascular events associated with pediatric use of stimulants remains controversial, with some population-based studies showing an increased risk, while the majority demonstrating no increased risk (Zito and Burcu 2017). The underlying mechanisms, by which stimulant medications may induce serious cardiovascular events, are not fully understood.
Strengths and limitations
Our study has several strengths. For one, we used a “new-user” design to mitigate bias due to unmeasured confounding and compared current to former AAP users rather than to nonusers (Ray 2003; Ray et al. 2004; Schneeweiss et al. 2007; Schneeweiss and Suissa 2013). Compared with nonusers, former users share more common characteristics (measured or unmeasured) with current users (Ray et al. 2004; Schneeweiss et al. 2007). We also conducted several sensitivity analyses to assess the robustness of the main study findings. Our study also has limitations. First, while the new-user design and the use of disease risk score methodology attempted to mitigate confounding, unmeasured confounding remains a threat in all designs of observational data. Second, drug use was defined from dispensings and may not necessarily reflect the actual usage (ingestion of the drug). However, medication use defined from administrative claims has high agreement with self-report (Johnson and Vollmer 1991; West et al. 1995). Third, in the current study, we created a composite outcome measure for cardiovascular events and were unable to assess death (cardiovascular-related death) and examine individual cardiovascular events (e.g., stoke, myocardial infarction) due to infrequent occurrence of events in youth. The most common event was severe hypertension event that led to hospitalizations or emergency department visits. Nevertheless, the cardiovascular events used in the composite outcome were ascertained from hospitalizations or emergency department visits to identify acute serious events. For example, while some cardiovascular events may need long-term AAP exposure, others may precipitate suddenly after brief period of exposure due to varying pathophysiologic mechanisms (e.g., metabolic changes, QTc prolongation, etc.). Unfortunately, events such as OTc prolongation are not readily available in retrospective observational studies using claims data and even in electronic medical records. Prospective research designs are best suited to address the underlying mechanisms of AAP-treatment emergent cardiac events in youth. Our study findings attempt to set the foundation for further research to examine the underlying physiological mechanism of AAP-treatment emergent risk of individual cardiovascular events. In addition, the focus of the current study was to assess the risk of cardiovascular events associated with AAP drug class, not with each individual AAP medication. However, the study findings provide a motivation for future research to assess the comparative cardiovascular safety of individual AAP medications (when used alone and in combination with individual antidepressant medications), with an appropriate study design that will attempt to attenuate channeling bias. In addition, the relative risk estimates for cardiovascular events should be interpreted with caution given the low incidence of these events in current AAP use following AAP initiation (0.84 cases/10,000 months of follow-up). Furthermore, the study findings should also be interpreted based on a broader context of both benefits and risks of AAP treatment in children and adolescents according to psychiatric disorder. For example, the benefit-risk assessment of AAP medications in youth is likely to produce a different conclusion in the treatment of schizophrenia than in the treatment of ADHD. Compared with behavioral disorders, psychiatric disorders such as schizophrenia or bipolar disorder in youth have different underlying psychopathology, may require more extensive AAP treatment pattern (duration, dose) and are potentially cardiovascular risk factors in youth, regardless of AAP use. Nonetheless, our analyses accounted for detailed clinician-reported psychiatric diagnoses as well as other covariates that attempted to measure psychiatric severity (e.g., psychiatric-related hospitalizations or emergency department visits, etc.). These analyses aimed to alleviate confounding by indication and underlying “psychopathology”.
Finally, the study findings may not be generalizable to privately insured U.S. youth. However, the prevalence of AAP use is markedly greater in Medicaid insured than privately insured youth (Crystal et al. 2009; Burcu et al. 2016).
Conclusions
In Medicaid-insured youth, current AAP use was associated with an increased risk of incident cardiovascular events that led to hospitalizations or emergency department visits. Furthermore, this risk intensified with the increasing AAP dose and with SSRI/SNRI use concomitant with AAPs.
Clinical Significance
The findings suggest that AAP medications should be used judiciously in clinically appropriate doses (i.e., the lowest dose that is necessary [and clinically appropriate] to achieve the desired clinical benefit). Further research is warranted to support current oversight policies to improve benefit-risk monitoring (Schmid et al. 2015) and to identify youth subpopulations having the greatest risk of developing AAP treatment-emergent cardiovascular events.
Footnotes
Disclosures
The authors have no conflicts of interest or financial relationships relevant to this article to disclose.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.