
Abstract
Objective:
To compare the effectiveness between parent–child interaction therapy (PCIT) and methylphenidate in preschool children with attention-deficit/hyperactivity disorder (ADHD) symptoms and disruptive behaviors who had remaining significant behavior problems after previous behavioral parent training.
Methods:
We included 35 preschool children, ranging in age between 3.4 and 6.0 years. Participants were randomized to PCIT (n = 18) or methylphenidate (n = 17). Outcome measures were maternal ratings of the intensity and number of behavior problems and severity of ADHD symptoms. Changes from pretreatment to directly posttreatment were compared between groups using two-way mixed analysis of variance. We also made comparisons of both treatments to a nonrandomized care as usual (CAU) group (n = 17) regarding intensity and number of behavior problems. All children who started one of the treatments were included in the analyses.
Results:
Mothers reported a significantly more decreased intensity of behavior problems after methylphenidate (pre–post effect size d = 1.50) compared with PCIT (d = 0.64). ADHD symptoms reduced significantly over time only after methylphenidate treatment (d = 0.48) and not after PCIT. Changes over time of children in the CAU treatment were nonsignificant.
Conclusions:
Although methylphenidate was more effective than PCIT, both interventions may be effective in the treatment of preschool children with disruptive behaviors. Our findings are preliminary as our sample size was small and the use of methylphenidate in preschool children lacks profound safety data as reflected by its off-label status. More empirical support is needed from studies with larger sample sizes.
Introduction
B
Two treatment options may be suitable for preschool children with continuing disruptive behaviors after BPT: parent–child interaction therapy (PCIT) and methylphenidate. PCIT is an empirically supported first-line treatment for young children with disruptive behavior problems that emphasizes improving the quality of the parent–child relationship and changing parent–child interaction patterns (Nixon 2002; Thomas and Zimmer-Gembeck 2007; Eyberg et al. 2008). Based on eight single group studies, a meta-analyses showed that large effect sizes (d = 1.31) have been achieved on mothers reports of child behavioral problems through treatment with PCIT (Thomas and Zimmer-Gembeck 2007). Compared with standard BPT, PCIT is a more intensive and individualized treatment. While in standard BPT mainly the parents are involved, in PCIT both the parents and the child participate together.
The key component of PCIT is coaching of the parents during their interactions with their child, thus providing the parent the opportunity to practice adequate parenting strategies and to get feedback on their performance immediately (Thomas and Zimmer-Gembeck 2007). This performance based on in vivo coaching, as well as treatment completion directed by mastery criteria are different from regular BPT.
Besides, being effective in decreasing oppositional behaviors, PCIT may also reduce symptoms of ADHD and related impairments. ADHD symptoms have not been the primary focus in the PCIT outcome studies, but given the high comorbidity between ADHD and disruptive behavior disorders one might assume that PCIT is effective on the full range of disruptive behavior problems, including impulsivity, hyperactivity, and inattentiveness (Wagner and McNeil 2008). Moreover, the Eyberg Child Behavior Inventory (ECBI), used in PCIT to assess progress during treatment and as an outcome measure, contains a lot of ADHD-related items.
A second often applied treatment option for children still exhibiting significant behavior problems after BPT is treatment with methylphenidate, a well-established treatment for ADHD symptoms in children with ADHD, oppositional behavior, and conduct problems above 6 years (Hinshaw and Arnold 2015; Pringsheim et al. 2015). However, in preschool children, the use of methylphenidate is off-label and indeed studies evaluating the efficacy and safety of methylphenidate in preschool children are scarce.
Only one randomized controlled study has investigated methylphenidate in preschool children with ADHD, with or without a comorbid oppositional defiant disorder (Greenhill et al. 2006; Ghuman et al. 2007). While that study showed that methylphenidate was effective, the effect size was smaller compared with the effects of methylphenidate in school-aged children. Furthermore, adverse events were much more frequent, including emotional lability, appetite loss, trouble with sleeping, stomach aches, social withdrawal, and lethargy. Yet, the use of methylphenidate has increased in young children (Zito et al. 2000; Efron et al. 2003).
In the present randomized controlled trial, we compared the effectiveness of PCIT and methylphenidate on mother-reported behavior problems and ADHD symptoms in preschool children with disruptive behaviors who had not improved sufficiently after previous BPT. We also compared changes over time between both treatments and a care as usual (CAU) group. Our hypothesis was that preschool children would respond more favorably to PCIT than to methylphenidate, given that the previously reported effect size of treatment with methylphenidate in the Preschool ADHD Treatment Study (Greenhill et al. 2006) (d = 0.89–1.00) were lower than those achieved through treatment with PCIT (d = 1.31) (Thomas and Zimmer-Gembeck 2007).
Methods
Study design
Before randomization (T1), mothers completed the pretreatment outcome measures. Next, families were randomly assigned to either PCIT or methylphenidate, in a 1:1 ratio. An external assistant using a computerized random number generator performed the randomization. No stratification took place. Both for treatment completers and dropouts, posttreatment outcome measurements were collected from the mother directly after treatment (T2).
Furthermore, in a comparison group, we assessed changes over time in disruptive behaviors of children who had also responded insufficiently to BPT, but received CAU. In the CAU comparison group, we collected assessments directly after BPT (T1) and 3–6 months later (T2).
Participants
Patients were recruited from the disruptive behavior department of our outpatient clinic for child and adolescent mental health. We included children of either sex, between 2.5 and 6 years of age, who had a score on the Intensity Scale of the ECBI (Eyberg and Pincus 1999) ≥131 and/or at least three DSM-IV-TR oppositional defiant symptoms based on clinical interview, with a full-scale intelligence quotient equivalent of >70, as measured by the Snijders–Oomen Nonverbal Intelligence Test (SON-R) (Laros et al. 1991) or the Wechsler Preschool and Primary Scale of Intelligence (WPPSI-III-NL) (Hendrikson and Hurks 2009), who at the time of referral had at least six ADHD symptoms in total, or at least four symptoms in one ADHD symptom domain (i.e., inattention or hyperactivity/impulsivity) as assessed with the Parent Interview for Child Symptoms (PICS-4) (Schachar et al. 2000) and the Teacher Telephone Interview (TTI) (Tannock et al. 2002) by trained clinicians.
Children were excluded if they had had previous treatment with PCIT, ongoing psychosocial treatment, ongoing treatment with psychotropic medication, or a major medical condition that would interfere with involvement in a long-term study or could be affected negatively by methylphenidate, including the presence of hyperthyroidism, cardiac arrhythmias, angina pectoris, or glaucoma. The study was approved by the Medical Ethics Committee of the University Medical Center Groningen.
Parents of 71% (n = 25) of all study participants had followed a manualized 12 sessions BPT program (van der Veen-Mulders et al., 2017) before entering the study. Most parents of this group (n = 15, 60%) completed the BPT, whereas ten families (40%) stopped the treatment before the last session (range 2–8 sessions). Parents of 29% (n = 10) of all study participants had participated in behavioral treatment at home, mostly with weekly visits during 6–12 months.
We originally aimed to include 60 participants. With sample sizes of 30 and 30 in 2 active treatment conditions, we estimated to achieve sufficient power to detect between-group differences on the primary outcome (Intensity Scale of the Eyberg Child Behavior Inventory [ECBI-I]). Unfortunately, however, we managed to include only 35 participants between April 2011 and September 2015, mostly due to parental disagreement with treatment allocation through randomization (see Fig. 1 for a flow chart). We had to discontinue the inclusion with fewer participants than planned because the funding for the study stopped. Baseline characteristics of the two randomly determined treatment groups and of the nonrandomized CAU group are presented in Table 1.
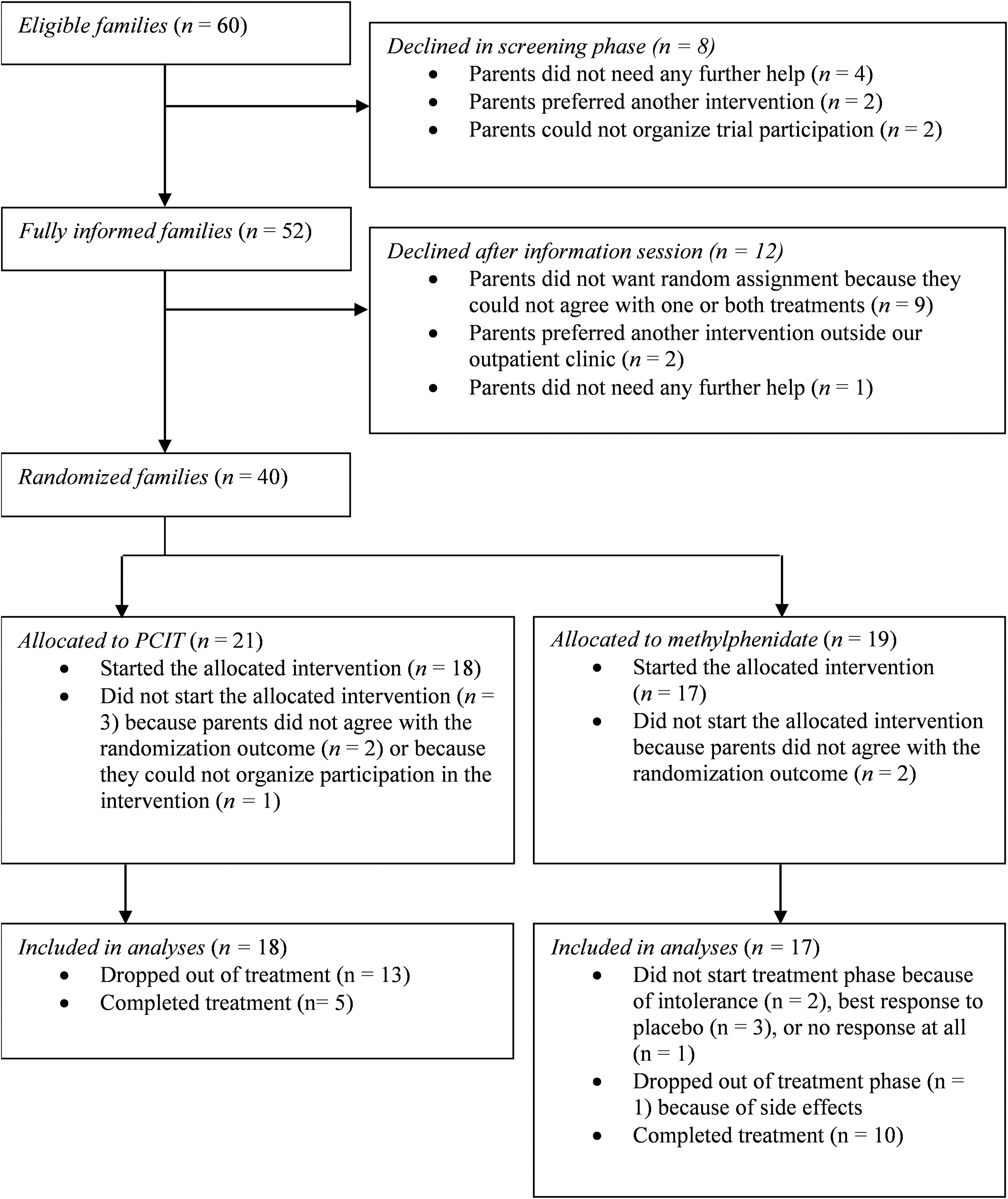
Flowchart.
There were no statistically significant between-group differences (as assessed by Fisher's exact test or t test) apart from the ECBI-P ratings of the care as usual group which were significantly lower than those of the Parent–Child Interaction Therapy group; F(2, 49) = 6.54, p = 0.003.
As assessed with the Snijders–Oomen Nonverbal Intelligence Test (SON-R) or the Wechsler Preschool and Primary Scale of Intelligence (WPPSI-III-NL). For three children discrepancy between performance—and verbal IQ was too high to calculate a total IQ.
As assessed with the Parent Interview for Child Symptoms (PICS-4) and the Teacher Telephone Interview (TTI).
Based on a clinical interview.
ADHD, attention-deficit/hyperactivity disorder; ADHD Index, ADHD Index: subscale of The Conners Parent Rating Scale-Revised: Short Form; ECBI-I, Intensity Scale of the Eyberg Child Behavior Inventory; ECBI-P, Problem Scale of the Eyberg Child Behavior Inventory; IQ, intelligence quotient; ODD, oppositional defiant disorder; SD, standard deviation.
We also asked (before randomization) which was the parents' preferred treatment. Fifteen families (43%) were allocated to the treatment they preferred (n = 5 to PCIT and n = 10 to methylphenidate) and 10 (29%) families (n = 4 to PCIT and n = 6 to methylphenidate) were not. Seven families (20%) had no preference beforehand and from three families (8%) we have no information about their preference.
Treatments
Parent–child interaction therapy
PCIT is a treatment that targets the quality of the parent–child relationship and parent–child interaction patterns. In PCIT, parents are taught specific skills to establish a nurturing and secure relationship with their child while increasing their child's prosocial behavior and decreasing disruptive behaviors. The treatment focuses on two basic interactions trained in two phases: in child-directed interaction, parents learn to apply play therapy skills to their child, aiming to strengthen the parent–child relationship; whereas in parent-directed interaction, parents learn to use behavioral management techniques, to enhance compliance of their child.
In line with the treatment manual, the length of PCIT treatment was variable and consisted of 1- to 2-hour weekly sessions. The number of sessions depended on parental progress and was not time limited. Following the PCIT manual, pre-established mastery criteria were coded in each session and the treatment was tailored depending on the parents' progress toward these criteria. Parents should master the child-directed interaction skills before they could go further toward the parent-directed interaction phase. Families met the completion criteria if they mastered both the child-directed and parent-directed interaction skills and if they reported the intensity of behavior problems as well as the amount of behavior problems below clinical levels on the ECBI (<132 and <15, respectively).
The PCIT treatments were conducted by four cognitive behavioral therapists who had been trained by licensed trainers. The training protocol included an intensive didactic component, where trainees learned the theory base, received an overview of the session-by-session PCIT protocol, and observed demonstration sessions conducted by accomplished trainers. Furthermore, during the training, many opportunities to practice the PCIT skills in vivo were provided. The training also included 1 year of biweekly group telephone consultation calls with a certified trainer.
To enhance treatment integrity, four sessions of two PCIT treatments of every therapist were videotaped and checked by one of the licensed trainers. Furthermore, the therapists scored high adherence to the PCIT protocol, visually checked, on a treatment integrity checklist after each session. Therapists discussed the treatments on a 2-weekly basis in their peer review group, in which adherence to the treatment procedures was subject of discussion as well.
Methylphenidate
Treatment with methylphenidate was manualized and consisted of a maximum of three phases: a 1-week open safety lead-in phase, a 4-week double-blind crossover titration phase, and a 6-week active treatment phase. We conducted the 1-week open safety lead-in phase and the 4-week double-blind crossover titration phase similar to the preschool ADHD treatment study (Greenhill et al. 2006; Kollins et al. 2006). Purpose of the open safety lead-in phase was to investigate which dose children tolerated without unacceptable adverse events. In the double-blind crossover titration phase, we tested which of the tolerated doses was the most effective one. Finally, after establishing the optimal dose, children started a 6-week treatment.
In the open safety lead-in phase, children began with 2.5 mg methylphenidate once a day, which was gradually increased to 7.5 mg three times a day. Because of the low effect size (0.22) and only trend significant differences with placebo (p < 0.06) on the 1.25-mg three times a day dose in the Preschool ADHD Treatment Study (PATS), we omitted this dosage in our study. Adverse events were monitored by telephone. Children with moderate to severe adverse events at doses lower than 5 mg were not eligible to enter the next phase. If that was the case, we collected T2 outcome data directly after the first phase.
Children who tolerated at least the 5-mg dosing in the first week subsequently entered the 4-week double-blind crossover titration phase in which the optimal dose was determined. During 4 consecutive weeks, children received one of three doses of active methylphenidate (2.5, 5, 7.5 mg) or placebo three times daily in identical capsules, in a random order. Children who tolerated all doses, except 7.5 mg, entered the crossover titration with the planned week on 7.5 mg dose replaced with an additional 5-mg week. Double-blind randomization was performed by the pharmacy department of the University Medical Center Groningen. At the end of each week, behavior ratings were obtained from parents using the ECBI and from teachers using the Teacher Report Form (TRF) (Achenbach and Rescorla 2000). Furthermore, parent- reported adverse events were collected with the Multimodal Treatment of ADHD (MTA) Side Effect Rating Scale (Greenhill et al. 2006). After the 4-week double-blind crossover titration phase, before breaking the blind, parent and teacher ratings were individually graphed for each week, and adverse events were also sorted per week. Using procedures developed in the MTA study (Greenhill et al. 1996) and later refined by Swanson et al. (2001), two independent clinicians reviewed the graphs and adverse events tables. In case the best response was to placebo, the child was given no further medication. Also, children with no clinical benefit at any point during the study were not given further medication. If that was the case, we collected T2 outcome data directly after the 4-week double-blind crossover titration phase. All other children started the 6-week active treatment phase with the individually determined optimal methylphenidate dose given to the child for the next 6 weeks, followed by collection of the T2 outcome data. Doses could be titrated up or down following consensus involving two experienced clinicians in these 6 weeks.
Outcome measures
The primary outcome in this study was the mothers' scores on the ECBI-I (Eyberg and Pincus 1999) in which they evaluated the intensity with which the child exhibited problem behaviors. The ECBI (Eyberg and Pincus 1999) is a 36-item inventory designed to measure current disruptive behavior problems in children aged 2–16. On every item parents rated the intensity of behavior problems from 1 for never to 7 for always. ECBI-I scores ≥131 are considered to represent clinical levels of behavior problems.
Furthermore, as secondary outcome measures we evaluated the Problem Scale of the Eyberg Child Behavior Inventory (ECBI-P) (Eyberg and Pincus 1999), on which mothers reported if they considered, for each of the 36 behaviors, whether these were a problem for them or not. Moreover, we used maternal ratings of ADHD symptoms on the ADHD Index: subscale of The Conners Parent Rating Scale-Revised: Short Form (CPRS-R:S) (Conners 1997). This subscale consists of 27 items covering inattentive and hyperactive/impulsive behaviors. Mothers rated each item ranging from 0 for not at all true to 3 for very much true.
ECBI-I and ECBI-P data were collected in the two treatment groups and in the CAU group. Data on the ADHD Index were only gathered in the two treatment groups, but not in the CAU group.
Statistical analyses
To test the hypothesis that preschool children would respond more favorably to PCIT than to methylphenidate, differences in changes on the outcome measures from T1 to T2 between the PCIT group and the methylphenidate group were compared with two-way mixed analysis of variance (ANOVA). We analyzed all families who started treatment, including those who dropped out prematurely. On the primary outcome measure (ECBI-I), we had no missing values and neither on the ECBI-P. Four missing ADHD Index scores at T2 were imputed, based on the last observation carried forward: two in the methylphenidate group and two in the PCIT group. In one of these four cases, the participant dropped out of PCIT treatment, in another the participant did not start the active methylphenidate treatment phase, whereas in the other two cases the participants completed their treatments. Effect sizes were calculated with Cohen's d, defined as the difference between two means (T1 and T2) divided by the pooled standard deviation (SD). A possible association between preference of allocation to the treatment of preference and treatment dropout was computed with Fischer's exact test. Finally, changes over time (T1–T2) on mothers' ratings of ECBI-I and ECBI-P in both treatment CAU group were analyzed with paired t-tests to compare these changes with the changes in both treatment groups. The statistical significance level for all analyses was tested two tailed and set at p < 0.05 (two tailed). This was not adjusted for multiple comparisons because, as given the modest sample size, we aimed to minimize type II error.
Results
Flow-through methylphenidate treatment, safety, and tolerability
The mean treatment period for methylphenidate was 12.6 weeks (SD = 6.83, range 0–25). Fifteen children (88%) tolerated all methylphenidate doses in the open safety lead-in phase without unwarranted adverse events. Two children (17%) did not tolerate the lowest dose of 2.5 mg, one because of increased irritability and emotionality and one because of increased lethargy and high blood pressure. Thus, 15 children started the 4-week double-blind crossover titration phase, 12 children (70%) with all doses, and three (18%) only with 2.5 and 5 mg doses because of increased adverse events using the 7.5 mg dose in the open safety lead-in phase.
In three participants (18%), the best response was to placebo and one child (6%) had no benefit at any dose. Therefore, 11 children (66%) started the 6-week active treatment phase with the most optimal dose. One child (6%) dropped out after 1 day of treatment because of increased levels of tics and hyperactivity. Ten (60%) children completed the active treatment phase, using 2.5 mg three times daily (n = 1), 5 mg three times daily (n = 7), or 7.5 mg three times daily (n = 2). For two children, the doses were increased during the 6-week treatment period; for four children, the doses were lowered; and in four children, the doses remained stable. Doses were never higher than 7.5 mg three times daily.
Flow-through PCIT
The mean treatment period was 22.3 weeks for PCIT (SD = 16.2, range 2–57). PCIT contained on average 13.4 sessions (SD = 9.46, range 3–37). Of the nine single mothers, three participated (partly) with the biological father of the child. The nine 2-parent families participated with both parents.
Thirteen families stopped the treatment (72%) before they met the completion criteria and five families (18%) finished PCIT. Ten of the treatment dropout families stopped during or at the end of the child-directed interaction phase (77%) and three families during the parent-directed phase (23%). Reasons for treatment dropout included parental preference for treatment with medication (n = 5, 38%), parents feeling that PCIT did not meet parental expectations (n = 3, 23%), parents feeling that PCIT had yielded enough progress with no need for treatment anymore despite ECBI ratings still being in the clinical range (n = 3, 23%). Finally, two families (16%) stopped because they could not manage to come to treatment on a regular basis because of a stressful family situation.
Allocation to the treatment of preference versus treatment dropout
Significantly more families allocated to their treatment of preference completed the treatment compared with those allocated to their nonpreferred treatment (12/15 [i.e., 80%] vs. 3/10 [i.e., 30%], respectively), p = 0.034.
Comparison of effectiveness of PCIT versus methylphenidate
A statistically significant interaction between the effects of time and treatment (methylphenidate or PCIT), F(1) = 5.99, p = 0.020, indicated that methylphenidate was more effective than PCIT in decreasing mothers' ECBI-I ratings. At T2, the mean ECBI-I of the PCIT group was 154 (SD = 26.5, range = 115–203) versus 123 (SD = 34.7, range = 57–180) for the methylphenidate group. Our two-way mixed ANOVA revealed a statistically significant effect of time on reducing the ECBI-I ratings, both after PCIT treatment, F(1,17) = 5.61, p = 0.030, d = 0.64, and after treatment with methylphenidate, F(1,16) = 22.9, p < 0.001, d = 1.50.
Furthermore, no significant interaction effect of time and treatment group, F(1,33) = 1.99, p = 0.167 was found on mothers' ECBI-P ratings, but we did find a statistically significant effect of time on mothers' ECBI-P ratings for both the PCIT group F(1,17) = 6.21, p = 0.023, d = 0.74, and the methylphenidate group, F(1,16) = 12.4, p = 0.003, d = 0.70. At T2, the mean ECBI-P of the PCIT group was 17.6 (SD = 9.78, range = 0–31) versus 14.3 (SD = 8.55, range = 1–29) for the methylphenidate group.
Finally, no statistically significant interaction effect of time and treatment group was found for the ADHD Index, F(1,33) = 2.73, p = 0.108. At T2, the mean ADHD Index of the PCIT group was 23.3 (SD = 5.87, range = 14–34) versus 18.8 (SD = 8.50, range = 0–34) for the methylphenidate group. On mother's ADHD Index ratings, there was only a statistically significant effect of time in the group treated with methylphenidate, F(1,16) = 5.60, p = 0.031, d = 0.48, but not in the PCIT treatment group, F(1,17) = 1.07, p = 0.317.
Changes in child behavior in the CAU group
The mean CAU period was 16.8 weeks (SD = 6.51, range = 12–30). Paired t tests revealed that mean ECBI-I scores did not differ significantly between T1 and T2, t(16) = 1.99, p = 0.064,, nor did mothers' ratings on the ECBI-P, t(16) = 0.062, p = 0.951.
Discussion
We compared the effectiveness between PCIT and methylphenidate in preschool children with disruptive behavior problems who had not responded sufficiently to BPT. Children in both treatment groups improved significantly over time, both in intensity and in the number of behavior problems, whereas changes in children who received 3–6 months of CAU treatment were nonsignificant. Regarding the intensity of behavior problems, the effects of methylphenidate were superior. ADHD symptoms reduced significantly over time only after methylphenidate treatment and not after PCIT. These findings are in contrast with our hypothesis that PCIT would be more effective than methylphenidate, perhaps due to the fact that previous studies investigated effectiveness of PCIT as a first-stage treatment (Thomas and Zimmer-Gembeck 2007). Interestingly, in the methylphenidate treatment group, the effect size for the intensity of behavior problems was much larger than the effect size for ADHD symptoms.
Not all children responded favorably to methylphenidate. The clinicians advised parents of three children to stop treatment because of adverse side effects. In four children, there were no effects of treatment with methylphenidate in the double-blind crossover titration phase. All in all, our findings regarding adverse events and magnitude of effects of methylphenidate are in line with the preschool ADHD treatment study, which showed that methylphenidate reduced ADHD symptoms in preschool children, although with a smaller effect size than what has been found in school-aged children and with more adverse effects (Greenhill et al. 2006).
Dropout before completing parent training is often substantial. In a recent review (Chacko et al. 2016) a dropout rate of at least 51% was reported. In our study, as many as 13 out of 17 families allocated to PCIT stopped treatment before the completion criteria were met. One factor that may have been related to this high rate of treatment dropout could be that before randomization, only 2 of these 13 families that prematurely terminated PCIT had pronounced preference for PCIT. Furthermore, treatment with methylphenidate can result in immediate decrease of disruptive behavior, whereas effectiveness of treatment with PCIT takes time, effort, and patience.
Demoralization due to prolonged behavioral treatment may have been at play in the high rate of PCIT treatment dropout. It could be that PCIT is most appropriate for families with enough energy, support, and opportunities to carry on. Perhaps, in the families with obstacles to participate, these difficulties should be the first target of treatment before starting a demanding behavioral intervention such as PCIT. The fact that the investigated families all had a potential adverse experience with former BPT because of remaining significant behavior problems after treatment may have created a possible disadvantage for the PCIT treatment, in the comparison between PCIT and methylphenidate treatment results. However, even though the PCIT participants had a nonsufficient experience with former BPT, and dropout rates were high, still moderate changes in disruptive behaviors were established.
The results of our study should be interpreted in light of its strengths and limitations. This was the first randomized controlled study directly comparing a behavioral and pharmacological treatment in preschool children with disruptive behaviors as a second-stage treatment. Such clinically relevant head-to-head comparisons are very rarely done. Moreover, we had a comparison group of otherwise comparable children who were not involved in any of the two treatments of our trial. Despite these strengths, a major limitation of our study has been that we failed to include the required number of families which limited its statistical power and generalizability of findings.
As a consequence of the small sample size, this study should be seen as a pilot study rather than as a hypothesis testing study. More than 72% of the eligible families declined because one or both treatments were not acceptable for them. Significant challenges were also to stimulate clinicians to refer suitable families and to motivate parents to participate.
Clinicians' attitudes concerning manualized treatment (Shafran et al. 2009) may have played a role, for example, the belief that their specific patients would not fit into a protocol because they are much more complicated than patients in clinical trials (Taylor and Chang 2008). The families who did consent to participate may not be representative of the typical patient population (Hoekstra 2017). Perhaps, a multicenter study patient preference trial (Corbett et al. 2016) would have provided better opportunities to recruit enough families to participate. Another potential limitation has been the exclusive use of self-reports as opposed to blinded treatment outcomes.
Conclusions
Despite these limitations, the tentative conclusion is that optimally dosed methylphenidate may be a more effective intervention than PCIT in reducing the intensity of behavior problems of preschool children who had responded insufficiently to previous BPT. However, our findings are preliminary as our sample size was small, and the use of methylphenidate in preschool children lacks profound safety data as reflected by its off-label status. More empirical support is definitely needed from studies with larger sample sizes.
Clinical Significance
Based on our preliminary study, although optimally dosed methylphenidate was more effective than PCIT, both interventions may be effective in the treatment of preschool children with disruptive behaviors and may be attempted when the response to behavioral parent training has been insufficient.
Disclosures
P.J.H. has received funding from Shire for a research project and has been member of a Shire advisory board meeting. B.J.V.D.H. and L.V.D.V.-M. received royalties as one of the editors of “Sociaal Onhandig” (published by Van Gorcum), a Dutch book for parents of children with autism spectrum problems and ADHD that is being used in parent training. B.J.V.D.H. is and has been involved in the development and evaluation of several parent training programs, and is and has been a member of Dutch ADHD guideline groups, all without financial interests.
Footnotes
Acknowledgment
Trial Registration: The Dutch Cochrane Center, NTR3201.