
Abstract
Objective:
Patterns of benzodiazepine (BZD) use and long-term use among young adults are not well known. Our aim was to study trends in BZD use and long-term use among 18–25-year-old young adults by gender and active substance in a nationwide retrospective longitudinal register-based setting.
Methods:
All Finns aged 18–25 years with reimbursed purchases of BZDs in 2006–2014 recorded to the Finnish Prescription Register were included. Annual prevalence rates of BZD use and long-term use among young adults were reported overall, according to gender, drug group (anxiolytic or hypnotic), and active substance. Long-term use of BZDs was defined as purchasing ≥180 Defined Daily Doses (DDDs) in at least two drug purchases during a calendar year.
Results:
Overall prevalence of BZD use among young adults decreased from 24.0 to 18.8 users per 1000 inhabitants in 2006–2014. Prevalence of long-term use decreased from 5.5 to 3.3 users per 1000 inhabitants. Overall BZD use was higher among females, whereas long-term use was more common among males. Use of anxiolytics was more common than use of hypnotics. Oxazepam, alprazolam, zopiclone, and zolpidem were the most used BZDs, whereas alprazolam and clonazepam were the substances with most long-term use. The use and long-term use of BZDs have decreased annually since 2008 among Finnish young adults. Further research is needed to investigate the reasons behind the decline.
Introduction
Y
Previous studies on BZD use among young adults have concerned specific populations, such as patients with substance use disorders, or focus on abuse of BZDs (McCabe 2005; Kornor et al. 2010; Riska et al. 2014). In studies assessing BZD use in general populations, young adults have been included as one of the age-groups (Lagnaoui et al. 2004; Cunningham et al. 2010; Hollingworth and Siskind 2010; Nordfjaern 2012; Olfson et al. 2015). In the United States, the prevalence of BZD use was 2.6% and 0.4% for long-term use among young adults (aged 18–35) (Olfson et al. 2015). In a Norwegian study cohort, 4% of young adults aged 18–25 years had received a prescription for BZDs, 1% used BZDs at least 180 DDD per year, and 0.5% were defined as chronic users (Nordfjaern 2012). Among Taiwanese incident, BZD users (aged 16–19), 5% were long-term users (Yeh et al. 2011).
There is limited population-based knowledge on the use of BZDs among young people due to the fact that most research has been conducted either among adults in general or among older adults (Kurko et al. 2016). The objective of this study was to assess nationwide trends in the prevalence of BZD use and long-term use among young adults 18–25 years of age over a 9-year period of 2006–2014 overall, according to gender and active substance.
Materials and Methods
Data sources
This nationwide, retrospective register-based study is based on data from the Prescription Register of the Social Insurance Institution of Finland. The National Health Insurance covers all Finnish residents. The Prescription Register contains individual level information on all reimbursed drug purchases dispensed to Finnish residents in outpatient care. In the database, all drugs are classified according to the World Health Organization's, (WHO 2017) Anatomical Therapeutic Chemical (ATC) classification system. The data compiled for the present study contain information on each patient's personal identifier, based on personal identification number in encrypted form, age at the end of the year, gender, ATC code of the dispensed drug, dispensing date, number of dispensed packages, and number of defined daily doses (DDDs) dispensed. According to Finnish legislation, ethical approval was not required to conduct this register-based study with anonymized patient data. Permission to use data was given by the register holder, the Social Insurance Institution of Finland.
The BZDs included in this study are presented in Supplementary Table S1 (Supplementary Data are available online at
The study population consisted of all 18–25-year-old young adults with at least one reimbursed purchase of BZD between January 1, 2006 and December 31, 2014. This age range of young adults was selected as the study population because the majority (94.3%, n = 68 167) of the 0–25-year-old BZD users (n = 72 266 in 2014) were from this age group (Fig. 1). In addition, the measurement for drug consumption used, DDD by WHO (2016) concerns only adults. Person's age was calculated at the end of each calendar year. Numbers of BZD users, dispensed prescriptions, and persons aged 0–25 years covered by the National Health Insurance in 2014 are presented in Figure 1.
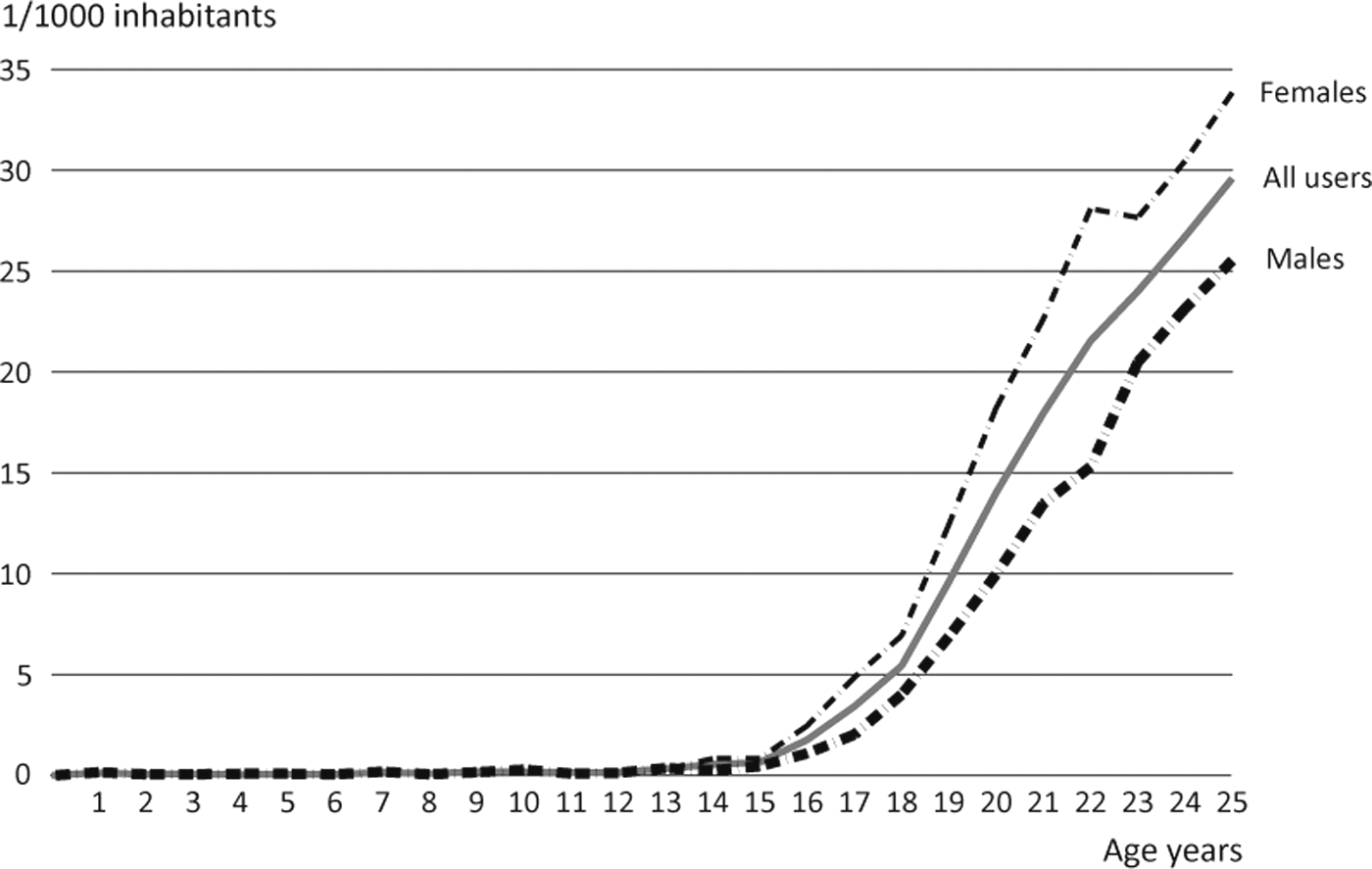
Prevalence (per 1000 inhabitants among persons 0–25 years of age) of BZD use by age and gender in 2014. BZD, benzodiazepine.
Study variable construction
BZDs in ATC-classes N03AE01, N05BA, and N06CA01 were classified as anxiolytics, and drugs in ATC-classes N05CD and N05CF as hypnotics.
Antiepileptic clonazepam was included in this study when used for other than epileptic indications, that is, when purchased without special reimbursement for epilepsy. In the Finnish system, patients' entitlement for special reimbursement is based on doctor's certificate fulfilling certain diagnosis criteria. These purchases with special reimbursements are distinguished in a register with special coding. In the nonepileptic indications, the dosing is lower compared with dosing for epilepsy (8 mg). The dosage of 1 mg was used as the DDD for clonazepam use based on the literature and clinical experience (White 2009; Drug and Alcohol Services 2012; Ashton 2013).
Reimbursed drug purchase of BZDs was used as a proxy for BZD use (Haukka et al. 2007). Long-term use of BZDs was defined as at least 180 DDD purchases of BZDs and two or more drug purchases during a calendar year corresponding to 6 months' use. This definition of 6 months' use was based on the WHO's recommendation as the definition for long-term use and a systematic review concerning long-term BZD use (World Health Organization 1996; Kurko et al. 2016). Drug consumption of BZDs per patient per year was calculated by using DDDs recommended by WHO (2016). DDDs of each patient's drug purchases were combined according to the patient's personal identifier.
One-year prevalence of BZD use and long-term BZD use were assessed overall, according to gender, drug group (anxiolytic or hypnotic, based on the ATC-classification), and active substance during 2006–2014. Prevalence rates (number of users per 1000 inhabitants) were calculated according to the number of the same age Finnish population.
Statistical analysis
While this study concerns entire population, data were analyzed with descriptive statistical methods. Binomial distribution was used to compare changes in prevalence rates between 2006 and 2014. For these prevalence rates, the 95% confidence intervals were calculated. The overall annual trends of each studied drug were assessed by comparing these confidence intervals. If the confidence intervals were not overlapping, the trend during the assessed period was considered to be statistically significantly changed. Descriptive data analyses were performed using statistical software IBM SPSS Statistics version 22.0, and binomial distribution was tested by R version 3.1.3.2015.
Results
Overall prevalence of BZD use among young adults decreased significantly, by 21.5% from 24.0 to 18.8 users/1000 inhabitants over a 9-year period (Fig. 2). The annual prevalence of BZD use increased between 2006 and 2008, the highest prevalence (28.6 users/1000 inhabitants) being observed in 2008. The BZD use was more common in females than males during the study period. In 2014, prevalence of BZD use among females was 22.8/1000 inhabitants and among males 15.1/1000 inhabitants.
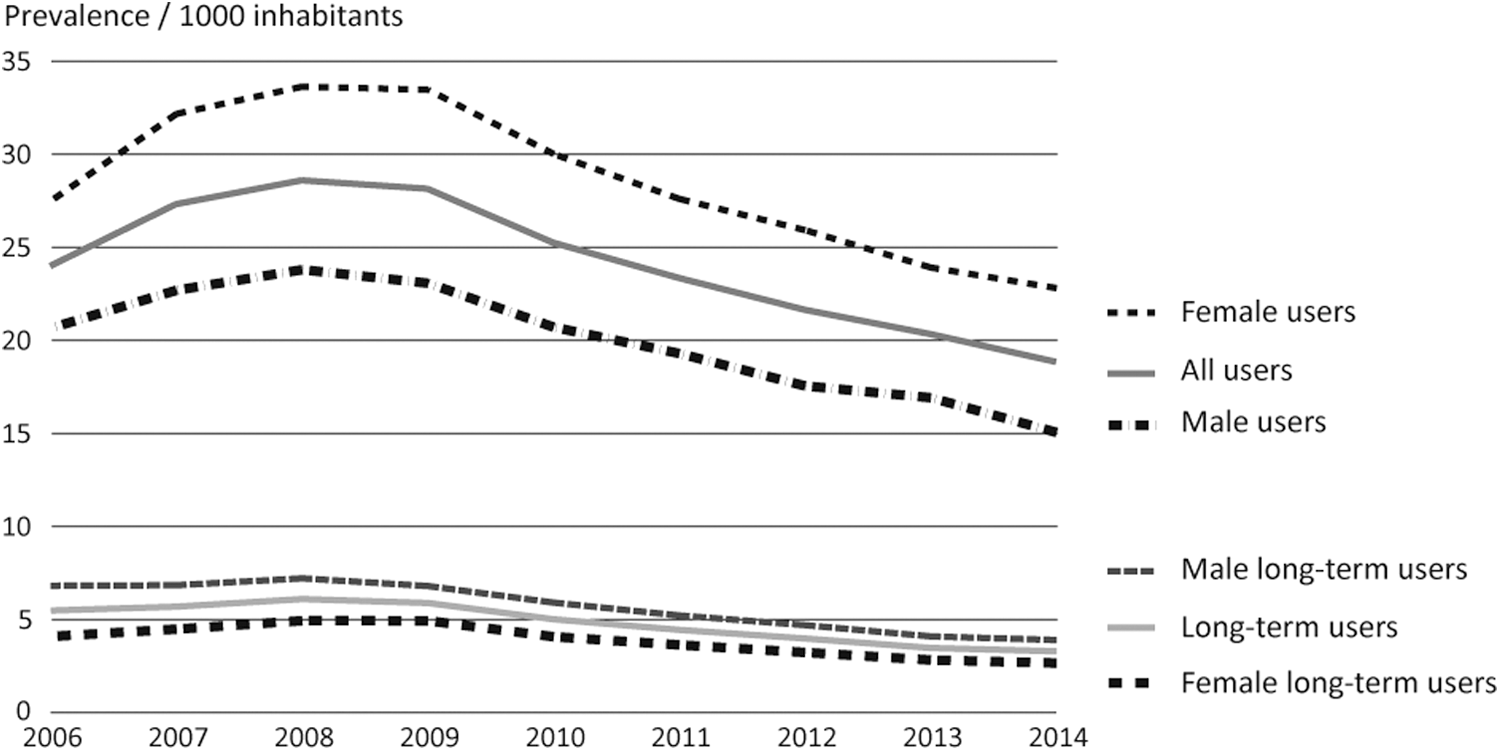
Prevalence of use and long-term use of BZDs among young adults by gender.
Overall prevalence of long-term BZD use among 18–25-year-old Finns decreased significantly, by 39.8% from 5.5 to 3.3 users/1000 inhabitants during 2006–2014. In 2014, the last studied year, 17.5% of all 18–25-year-old BZD users were defined as long-term users. The prevalence of long-term use was higher among males than females during the entire study period.
Use of anxiolytic BZDs was more common than use of hypnotics among Finnish young adults (Fig. 3). The overall prevalence of anxiolytic use decreased 20.6%, from 15.2 to 12.1 users/1000 inhabitants during the study period. The use of hypnotics decreased from 12.5 to 8.5/1000 inhabitants, 31.8% between 2006 and 2014. Long-term use of anxiolytics was more common than long-term use of hypnotics among young adults during the study period. In 2014, the prevalence of long-term use of anxiolytics was 2.6/1000 inhabitants and hypnotics 0.7/1000 inhabitants. Both long-term use of anxiolytics and long-term use of hypnotics decreased during 2006–2014.
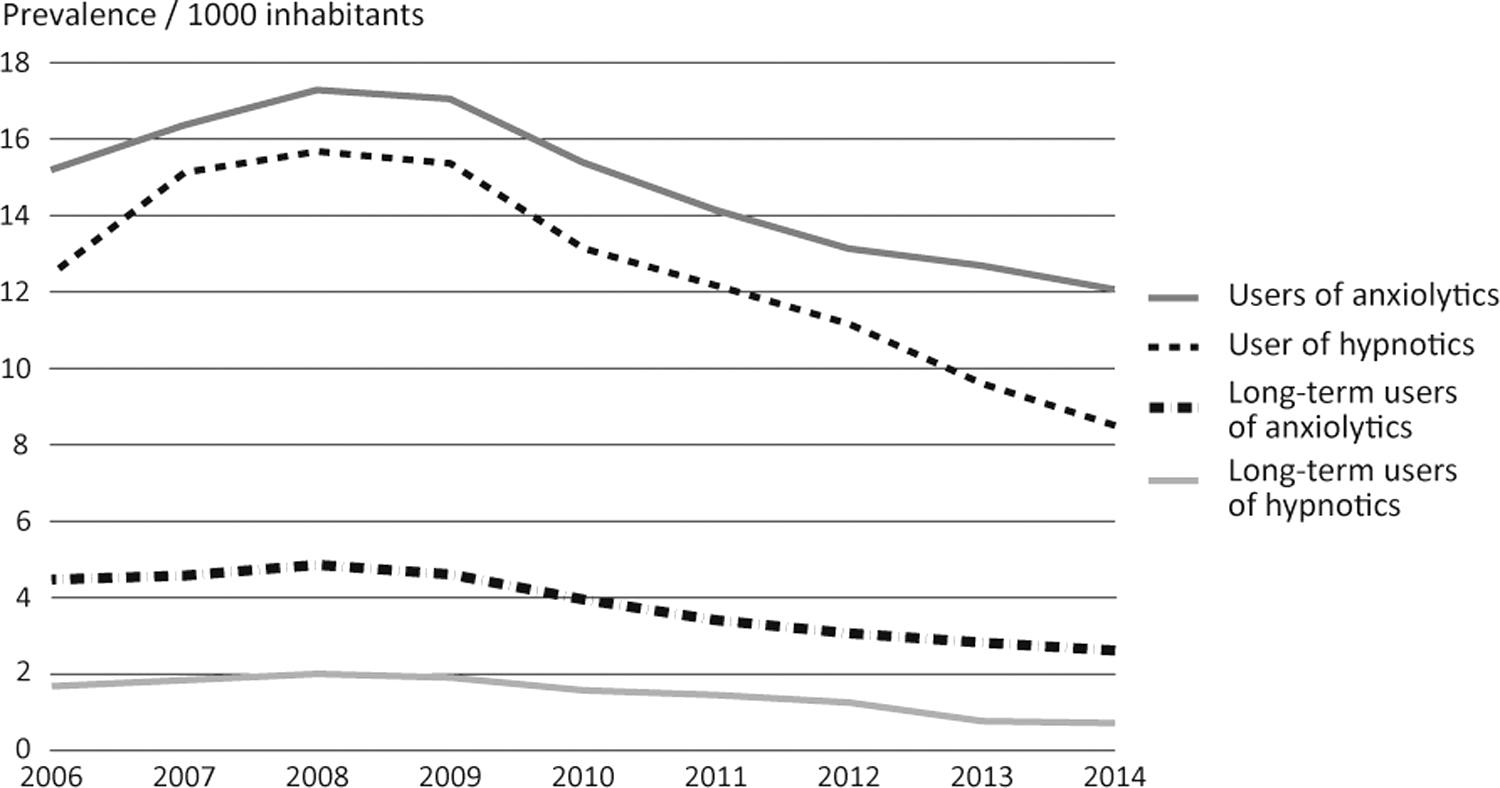
Prevalence of use and long-term use of anxiolytics and hypnotics among young adults.
Oxazepam and alprazolam were the most commonly used anxiolytics (Fig. 4). The most commonly used hypnotics were z-drugs zopiclone and zolpidem. Over the 9-year study period, there was a decline in the use of almost every studied substance. Alprazolam use decreased the most (53.5%) between 2006 and 2014. Only the prevalence of oxazepam use increased by 17.4%, from 5.3 in 2006 to 6.2/1000 inhabitants in 2014. Use of diazepam and clonazepam was lower than that of oxazepam and alprazolam. During the study period, prevalence of diazepam use ranged between 2.0 and 3.4/1000 inhabitants, while clonazepam use ranged between 1.6 and 2.3/1000 inhabitants, respectively.
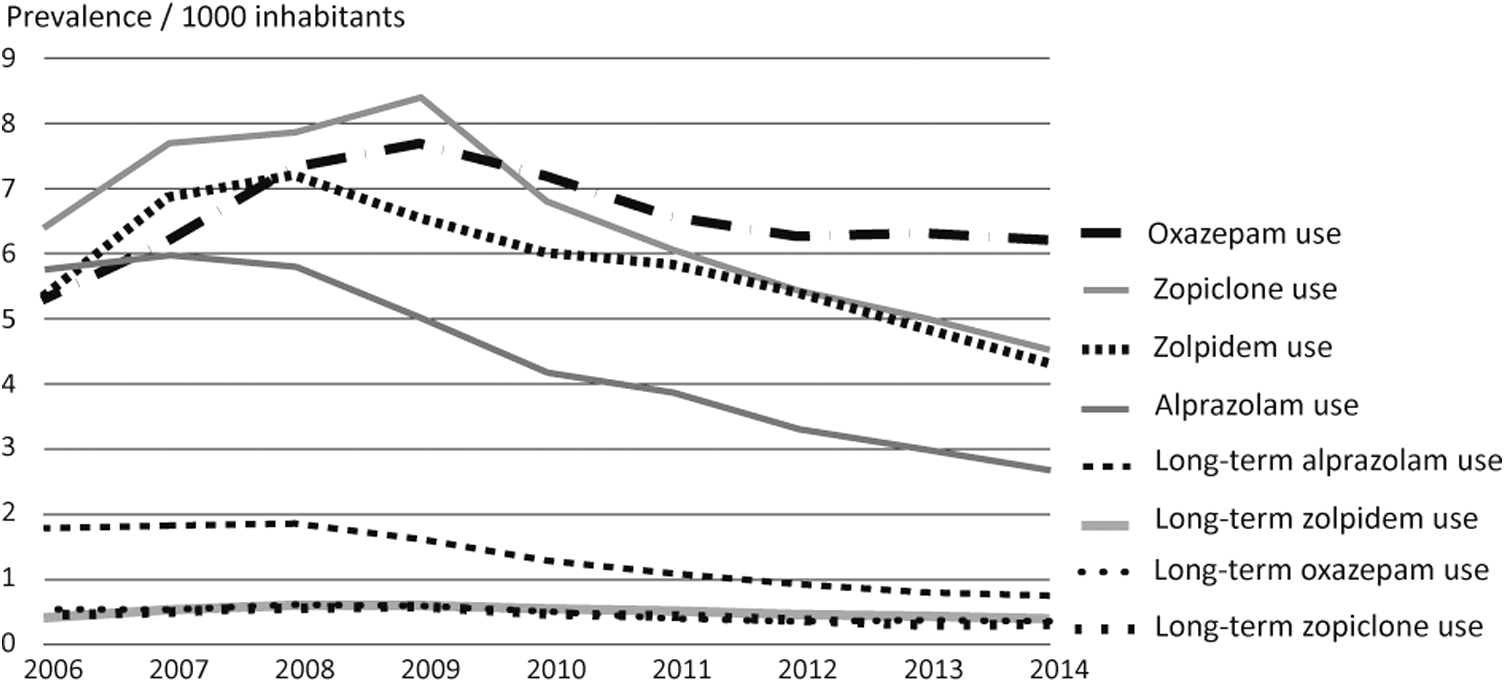
Prevalence of use and long-term use of four most commonly used BZDs among young adults.
Long-term use of BZDs was relatively low among young adults during the study period. The highest prevalence of long-term use was observed in alprazolam users during 2006–2009 and in clonazepam users during 2010–2014 (Fig. 4).
The substance-level prevalence of long-term use decreased in users of all BZD substances between 2006 and 2014. The decline of long-term use was most significant in diazepam (58.7%) and alprazolam (57.9%) users. Compared with other BZDs, long-term use was more prevalent among subjects using diazepam and clonazepam. The relative proportions of long-term use among diazepam and clonazepam users were higher compared to other BZDs. More than half (59.9%–64.6%) of clonazepam users were long-term users during 2006–2014. Corresponding proportions were 24.9%–37.5% among diazepam users and 26.8%–32.3% among alprazolam users during the study period.
Discussion
To our knowledge, the present study is the first nationwide register-based study focusing on use and long-term use of BZDs among young adults. Therefore, the present study offers clinically significant new information on BZD use and long-term use of this less-studied user group. We found a decreasing trend of both BZD use and long-term use among Finnish young adults during the investigated 9-year study period. The overall prevalence of BZD use decreased by one fifth and long-term BZD use decreased by over one third between 2006 and 2014. Overall BZD use was more common among females, whereas long-term use was more common among males. The four most commonly used BZDs among young adults were oxazepam, alprazolam, zopiclone, and zolpidem. Oxazepam was the only substance with increased use between 2006 and 2014. Alprazolam and clonazepam were the substances mostly used for long-term.
This study was based on data from the Finnish Prescription Register covering all reimbursed BZD purchases in Finland among entire population during the investigated period. Key strengths of this study are the nationwide data and a long, 9-year study period. Completeness and accuracy of records in The Finnish Prescription Register is high.
Drug purchase was used as a proxy for BZD use, because there is concordance between prescription database information and self-reported BZD use (Haukka et al. 2007). However, this study may underestimate the total BZD use among young adults in Finland. The Finnish Prescription Register does not record nonreimbursed drug purchases, inpatients' drug use, or illegal drug use (Furu et al. 2010). Moreover, some diazepam and oxazepam purchases in small package sizes are not recorded in the Prescription Register, as they are not usually reimbursable. The coverage of the register was 76%–90% annually compared to wholesale data of BZD provided by the Finnish Medicines Agency (2017). Information on patient's diagnosis or severity of psychiatric condition is not included in the Prescription Register.
Previous studies on BZD use and long-term use have varied considerably in terms of definition for long-term use, time-period, and age group studied, making it difficult to compare the prevalence rates between studies. There may also be differences in treatment practices between countries. However, prevalence of BZD use (1.9%) among Finnish young adults in 2014 was similar to that reported in France (1.8%) (Lagnaoui et al. 2004), but lower than reported in the United States (2.6%) (Olfson et al. 2015), Norway (4.0%) (Nordfjaern 2012), and Taiwan (6.7%) (Yeh et al. 2011). Long-term use of BZDs (0.3%) by Finnish young adults was slightly less common than that reported among U.S. young adults (0.4%) in 2008 (Olfson et al. 2015), and among a sample of French young adults (0.6%) in 2001 (Lagnaoui et al. 2004). Furthermore, the prevalence of long-term use in Finland was lower than that observed in a Norwegian study cohort (1%) during 2004–2008 (Nordfjaern 2012) and among Taiwanese incident BZD users (5%) in 2001–2005 (Yeh et al. 2011).
It was not possible to include assessment of indications of BZD prescriptions in the present study. However, results showed that BZDs classified as anxiolytics were more commonly used than hypnotics, which may suggest that BZDs are more often used in anxiety than sleep disorders among young adults. At a substance-level, decreasing trend was observed among almost all BZDs except oxazepam, which was the only substance with increased use. In the last studied year (2014), oxazepam was the most commonly used BZD among Finnish young adults. Increased use of oxazepam may be due to its lower abuse liability (Griffiths et al. 1984). The present study found that long-term use of oxazepam was relatively uncommon. However, a recent study showed that oxazepam users were more prone to dose escalation compared with diazepam users (Tvete et al. 2016). Despite the decreasing trend of long-term use overall and at a substance-level, long-term use was common among users of high- or medium-potency BZDs, including clonazepam, diazepam, and alprazolam. In this study, a majority of all clonazepam users used the substance for long-term. Similarly, a recent study found that clonazepam use is often associated with dose escalation (Alessi-Severini et al. 2016). On the contrary, in the study of Cloos et al. (2015), clonazepam was associated with a lower risk for high-dose use compared with hypnotics and anxiolytics alprazolam and prazepam, which were associated with the highest risk for high-dose use.
The observed gender difference in overall BZD use is consistent with other studies, showing that use of BZDs is more common among females than males (Lagnaoui et al. 2004; Petitjean et al. 2007; Cunningham et al. 2010; Olfson et al. 2015). The higher prevalence of anxiety and sleep disorders in females during young adulthood partly explains this finding (Wittchen et al. 1998; Suvisaari et al. 2009). Yet, in our study, long-term use of BZDs was more prevalent in males than females. This could be partly explained by the previous finding reporting nonmedical, e.g., self-reported possible abuse or misuse, use of anxiolytics and hypnotics in adolescence to be significantly more common in males than females in Finland compared with many other European countries (Kokkevi et al. 2008). However, our study did not assess the possible abuse of BZDs.
Decreasing trend in BZD use found in this study suggests that prescribing patterns of BZDs have changed during recent years. Similar decreasing trend of BZD utilization has also been observed in the entire Finnish population (Saastamoinen et al. 2016). National guidelines on rational BZD prescribing recommend to restricting the length of BZD treatment to some weeks (National Supervisory Authority for Health and Welfare 2015, Working Group set up by the Finnish Medical Society Duodecim and the Finnish Sleep Research Society 2017). However, we found that nearly one out of five young adult BZD users could be defined as a long-term user. Decreasing trend of long-term BZD use among young adults raises questions about the factors associated with decreased use. It is probable that a part of BZD use has been replaced by other pharmaceutical use or psychosocial treatments. During recent years, mental health services among adolescents and young adults have increased, which reflects the enhanced recognition of the treatment need, but may also suggest that stigma associated with mental health service use has decreased (Pylkkänen and Laukkanen 2011). Availability of mental health services may have improved, and low-threshold online therapies are available too (Stenberg et al. 2016).
Based on the findings of this study, we suggest that patterns of long-term BZD use among young people need further research. Long-term treatment with BZDs can be considered medically justified for some patients. Therefore, it would be of importance to identify specific patient groups, which would benefit from long-term BZD treatment. However, equally important would be to recognize those patients who may experience harm of BZD use.
Conclusion
Both overall use and long-term use of BZDs have decreased annually since 2008 among Finnish young adults. Decreasing use may be the consequence of increased awareness of problems related to long-term BZD use and recommendations introduced to optimize the use of BZDs. Further research is needed to identify factors associated with the decline in BZD use among young adults.
Clinical Significance
In this first nationwide study on BZD use and long-term use focusing on young adults, we found a declining trend in use and long-term BZD use. Despite this decline, still nearly a fifth of young adult BZD users could be defined as long-term users and part of this long-term use may be inappropriate. Our findings urge physicians to pay more attention to BZD prescribing and monitoring for young men who are especially prone to long-term use. Special concern regarding prescribing of high-potency BZDs alprazolam and clonazepam is needed, as these substances were most commonly used for long-term.
Footnotes
Acknowledgment
We thank Assistant Anne-Mari Kilpeläinen, Information and Communications Unit, Social Insurance Institution, for her help in finalizing figures.
Disclosures
Terhi Aalto-Setälä, Marja Airaksinen, Leena Saastamoinen, Annamari Tuulio-Henriksson, Sanna Tähkäpää have no conflicts of interests.
Terhi Kurko has owned a few stocks of pharmaceutical company Orion Pharma in 2014–2015 and has received an expert fee from Pfizer in 2015.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.