
Abstract
Objective:
The aim of this study was to assess the efficacy and safety of stimulant and nonstimulant medications in children and adolescents using as an outcome measure the Attention-Deficit/Hyperactivity Disorder Rating Scale-IV (ADHD-RS-IV), and to examine the effect of medications in different ADHD subtypes (i.e., inattention and hyperactivity/impulsivity).
Methods:
MEDLINE, Scopus, EMBASE, EBSCO (E-journal, CINAHL and SportDiscus), PUBMED, and The Cochrane Central Register of Controlled Trials databases were searched. Randomized controlled trials (RCTs) with parallel group or placebo-controlled studies comparing the effect of medications (stimulants or nonstimulants) in children and adolescents with ADHD were included. The main outcomes were the ADHD-RS-IV total score and subtypes (inattention and hyperactivity/impulsivity). Treatment-emergent adverse events (TEAEs) and secondary outcomes such as systolic and diastolic blood pressure, and pulse rate were considered.
Results:
The search strategy identified 15 RCTs, including a total of 4648 children and/or adolescents diagnosed with ADHD aged 6 to 17 years old. Overall, both stimulant and nonstimulant medications reduce the ADHD-RS-IV score with a standardized mean difference (SMD) of −0.70 (confidence interval [95% CI], −0.85 to −0.55); in subgroup analyses, the SMD was −0.83 (95% CI, −1.11 to −0.54) for stimulant medications and −0.58 (95% CI, −0.69 to −0.46) for nonstimulant medications. Similar results were observed in inattention and hyperactivity/impulsivity subtypes. The placebo group also showed a medium effect SMD of −0.68 (95% CI, −0.82 to −0.54). The most frequent TEAEs for stimulant and nonstimulant medications, respectively, were decreased appetite (28.6% and 14.2%) and somnolence (4.4% and 34.1%).
Conclusions:
These results suggest that both stimulant and nonstimulant medications mitigate ADHD symptoms in children and adolescents, although subgroup analyses suggest a greater effectiveness of stimulant medications.
Introduction
A
Worldwide estimates of ADHD prevalence range from 8% to 10% in children and adolescents, and from 2.5% to 4% in adults (Faraone et al. 2003; Fayyad et al. 2007; McCarthy et al. 2012). The etiology of ADHD is presumably complex and multidimensional, combining genetic and environmental factors (Faraone et al. 2000; Biederman and Faraone 2005). Approximately one-third of childhood ADHD persists into adulthood (Kessler et al. 2006; Barbaresi et al. 2013).
According to the European guidelines, the treatment of children and adolescents with ADHD may include nonpharmacological options, including behavioral therapy, and pharmacological options, including stimulant and nonstimulant medications (Stuhec et al. 2015). Stimulant medications (derived from methylphenidate or amphetamines, along with behavioral interventions) are generally recommended as the first-line therapy for school-aged children and adolescents with severe ADHD (Catala-Lopez et al. 2015). These psychostimulant medications act through dopaminergic and noradrenergic pathways. The most commonly used stimulant medications are methylphenidate (MPH), dexmethylphenidate, dexamfetamine/dextroamfetamine, mixed amphetamine salts (MAS), lisdexamfetamine (LDX), and modafinil (Chan et al. 2016). An alternative to the use of stimulant medications involves the use of nonstimulant medications such as atomoxetine (ATX), a selective norepinephrine reuptake inhibitor, and two alpha-2 agonists such as guanfacine extended-release (GXR) and clonidine (CLO). Clonidine, used alone or in combination with MPH, has been shown to be effective in reducing the symptoms of ADHD in children (Biederman et al. 2008).
The results of a previous meta-analysis (Faraone 2009) showed that, in youths with ADHD, the efficacy of stimulants was significantly greater compared with nonstimulants (overall effect size of 0.78). Although this was a methodologically rigorous study, 15 medications were evaluated using 20 different ADHD measures. In fact, the authors acknowledged the variability of outcome measures as a limitation, which could affect the apparent efficacy of treatments. Apart from updating the previous research by including studies published from 2008 up to 2016, our meta-analysis is focused specifically on studies that have used the same outcome measure of ADHD symptoms (the ADHD Rating Scale-IV [ADHD-RS-IV]). In addition, this article reviews the effects of medications in different ADHD subtypes (inattention and hyperactivity/impulsivity), and describes treatment-emergent adverse effects and secondary outcomes related to drugs such as pulse rate, systolic blood pressure (SBP), and diastolic blood pressure (DBP).
Currently, the ADHD-RS-IV is one of the most widely used scale. It was developed for an accurate assessment of children and adolescents who are suspected of having ADHD (Dupaul et al. 1998). The ADHD-RS-IV contains versions for parents and teachers, and their internal consistency, reliability, and agreement between parent and teacher ratings have repeatedly been shown (Dupaul et al. 1998; Collett et al. 2003).
Therefore, the objective of this study was to assess the efficacy and safety of stimulant and nonstimulant medications in children and adolescents using the ADHD-RS-IV as the outcome measure and separately examine the effect of medications in different ADHD subtypes (i.e., inattention and hyperactivity/impulsivity).
Materials and Methods
The Preferred Reporting Items for Systematic Review and Meta-analyses (PRISMA) guidelines were followed to improve the reporting of this meta-analysis. This review has been registered in the International Prospective Register of Systematic Reviews (PROSPERO) (registration number: CRD42016052178).
Literature search
The databases MEDLINE, Scopus, EMBASE, EBSCO (E-journal, CINAHL and SportDiscus), PUBMED, and The Cochrane Library were searched from their inception to August 31, 2017. The search was conducted between August 20 and 31, 2017. We also looked at the reference lists of selected full text articles. The search terms used were attention-deficit/hyperactivity disorder, ADHD, ADHD Rating Scale-IV, ADHD-RS-IV, pharmacology, pharmacotherapy, stimulant, drug, medication, randomized (and randomised) controlled trial (RCT), trial, child, and adolescent. We developed a sensitive search strategy for each individual database (Supplementary Data S1; Supplementary Data are available online at
Study selection and inclusion criteria
The a priori inclusion criteria for this study were as follows: (1) patients: children and/or adolescents aged 6–18 years diagnosed with ADHD; (2) type of study: RCT and double-blind trials with parallel group or placebo controlled; (3) type of intervention: pharmacological interventions for ADHD treatment, such as stimulant medications (MPH, dexmethylphenidate, dexamfetamine/dextroamfetamine, MAS, LDX, and modafinil) or nonstimulant medications (ATX, GXR, and CLO); (4) duration of the intervention: at least 3 weeks; (5) main outcome: ADHD-RS-IV total score and subtypes (inattention and hyperactivity/impulsivity); (6) diagnostic criteria: ADHD-RS-IV; and (7) language: all languages were accepted. The exclusion criteria were as follows: (1) interventions in which the treatment group is being administered another complementary substance or another activity; (2) studies in which the ADHD-RS-IV was not used to diagnose ADHD. Two authors (A.J.C.U. and A.G.H.) independently screened the titles and abstracts of the retrieved studies by the search strategy. In the second step, those studies potentially eligible were re-evaluated in full text. In cases of disagreement, a third author (M.S.L.) proceeded to read the entire article and resolved the discrepancies.
Data collection
Data were extracted independently by two authors (A.J.C.U. and A.G.H.) using a predesigned extraction form that included the following data: title, year of publication, design of study (parallel vs. cross-over), blinding strategy, name and dose of medication, characteristics of trial participants (number, sex, and age), dropouts and adverse effects, method used to evaluate the results (questionnaires and scales to assess symptoms), and results of the main and secondary outcome (treatment-emergent adverse events [TEAEs], pulse rate [bpm], SBP, and DBP).
Risk of bias
The quality of studies was evaluated using two tools in accordance with The Cochrane Collaboration (Higgins et al. 2011) recommendation and the Grading of Recommendations Assessment, Development and Evaluation (GRADE) (Atkins et al. 2004; Guyatt et al. 2008). The Review Manager program (Update Software, Oxford) for assessing the risk of bias in RCTs (Higgins et al. 2011; Savovic et al. 2014) consists of seven criteria as indicators of the quality of trials according to the responses “low risk,” “high risk,” or “unclear” to the following domains: (1) random sequence generation; (2) allocation concealment; (3) blinding of participants and personnel; (4) blinding of outcome assessment; (5) incomplete outcome data; (6) selective outcome reporting; and (7) other potential threats to validity. The GRADE approach evaluates the quality of evidence for outcomes reported in systematic reviews and meta-analyses. In addition, it is a systematic and explicit approach that allow judgments to be made about the strength of evidence and it is an effective method for linking evidence quality and clinical recommendations. The GRADE approach was used by two independent reviewers (A.J.C.U. and A.G.H.) to evaluate the overall quality of evidence and the strength of the recommendation, as advocated by the Cochrane Back Review Group (Higgins and Green 2011). The overall quality of evidence was initially regarded as “high,” but was downgraded by one level for each of the five factors encountered: risk of bias (>25% of participants from studies with low quality), inconsistency of results (substantial I 2 statistic), absence of direct evidence, imprecision (based on the confidence interval [CI] estimator and the number of events, or the number of subjects included), and publication bias. Finally, authors resolved disagreements by consensus, and a third author (M.S.L.) was consulted to resolve disagreements when necessary.
Meta-analysis calculation
Random-effects models were used to calculate the standardized mean differences (SMD) with 95% CIs using Comprehensive Meta-Analysis software, V.2.2.064 (BioStat, Englewood, New Jersey). To display the results of the meta-analysis, the Review Manager (Update Software, Oxford) was used. Cohen's categories were used to evaluate the magnitude of the effect size, calculated according to the SMD statistic and considering scores of d ≥|0.8| as a large effect, scores from ≥|0.5| to <|0.8| as medium, scores from ≥|0.2| to <|0.5| as small, and scores ≥|0.1| to |0.2| as trivial (Cohen 1988).
The presence of heterogeneity between studies was tested using Cochran's Q. The magnitude of heterogeneity was determined using the I 2 statistic. A sensitivity analysis was conducted by deleting each study from the model one by one, to analyze its influence on the overall results. Egger regression tests were performed to detect small-study effects (Egger et al. 1997) and possible publication bias.
For the placebo group, the SMD value of the ADHD-RS-IV total score was calculated as the mean preintervention to postintervention in each study (i.e., in all cases, the preintervention and the postintervention data were used in the meta-analysis), divided by the pooled standard deviation, and correcting for small sample bias.
Finally, subgroup moderator analyses were conducted to determine whether medication effects differed according to the medication used (LDX and GXR).
Results
Study selection
The flowchart is shown in Figure 1. The literature search retrieved 1544 references after removing duplicate studies. The screening of titles and abstracts identified 42 potentially eligible articles; 27 of them were excluded after full text review (population, intervention, outcome, duplicates, and study type). Finally, 15 RCTs were included in the meta-analysis (Spencer et al. 2006; Biederman et al. 2007, 2008; Findling et al. 2008, 2010; Sallee et al. 2009; Takahashi et al. 2009; Connor et al. 2010; Findling et al. 2011; Jain et al. 2011; Coghill et al. 2013; Newcorn et al. 2013; Childress et al. 2014; Hervas et al. 2014; Wilens et al. 2015).

Flowchart for the selection of studies.
Participants
The meta-analysis included a total of 4648 children and adolescents diagnosed with ADHD. Subjects were diagnosed with ADHD by a psychiatrist or psychologist through clinical interview or by using the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association 2002). Trial participants were aged 6 to 17 years (mean 11.09; SD 2.07). There were more boys than girls (67.98%), and the majority were Caucasian (56.71%). Table 1 summarizes the characteristics of the participants.
ATX, atomoxetine; CLON-XR, clonidine hydrochloride extended-release; GXR, guanfacine XR; MAS, mixed amphetamine salts extended-release; MTS, methylphenidate transdermal system; LDX, lisdexamfetamine dimesylate; OROS-MPH, methylphenidate extended-release.
Study characteristics and medications
The characteristics of the 15 studies included in this meta-analysis (Spencer et al. 2006; Biederman et al. 2007, 2008; Findling et al. 2008, 2010; Sallee et al. 2009; Takahashi et al. 2009; Connor et al. 2010; Findling et al. 2011; Jain et al. 2011; Coghill et al. 2013; Newcorn et al. 2013; Childress et al. 2014; Hervas et al. 2014; Wilens et al. 2015) are detailed in Table 2.
Bold values represent the highest dose administered in those studies where several doses were administered.
ADHD-RS-IV, Attention-Deficit/Hyperactivity Disorder Rating Scale-IV; ATX, atomoxetine; CLON-XR, clonidine hydrochloride extended-release; DM, difference in means; GXR, guanfacine XR; MAS, mixed amphetamine salts extended-release; MTS, methylphenidate transdermal system; LDX, lisdexamfetamine dimesylate; ND, no data; OROS-MPH, methylphenidate extended-release; SE, standard error.
Stimulant medications
Stimulant medications were analyzed in seven RCTs (Spencer et al. 2006; Biederman et al. 2007; Findling et al. 2008, 2010; Findling et al. 2011; Coghill et al. 2013; Childress et al. 2014): two trials used a methylphenidate transdermal system (MTS) (Findling et al. 2008, 2010), another mixed amphetamine salts extended-release (MAS XR) (Spencer et al. 2006), two used methylphenidate extended-release (OROS-MPH) (Findling et al. 2008; Coghill et al. 2013), and four analyzed LDX (Biederman et al. 2007; Findling et al. 2011; Coghill et al. 2013; Childress et al. 2014) (Table 2). The mean duration of the interventions was 5.28 weeks, and the average adherence was 68.04%. The most frequently used dose optimization for MTS was 30 mg/day (55.2%), for MAS XR was 40 mg/day (27.0%), for OROS-MPH was 54 mg/day (53.2%), and for LDX was 70 mg/day (33.3%). Five studies evaluated the reduction from baseline to final assessment in ADHD-RS-IV total score and subtypes (inattention and hyperactivity/impulsivity) (Spencer et al. 2006; Findling et al. 2010, 2011; Coghill et al. 2013; Childress et al. 2014), although two did not provide sufficient information for their inclusion in the meta-analysis (Biederman et al. 2007; Findling et al. 2008).
Nonstimulant medications
Eight RCTs double-blind with parallel group analyzed nonstimulant medications (Biederman et al. 2008; Sallee et al. 2009; Takahashi et al. 2009; Connor et al. 2010; Jain et al. 2011; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015) (Table 2). Six trials analyzed the effect of GXR (Biederman et al. 2008; Sallee et al. 2009; Connor et al. 2010; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015), two used ATX (Takahashi et al. 2009; Hervas et al. 2014), and one assessed clonidine hydrochloride extended-release (CLON-XR) (Jain et al. 2011). The mean duration of the interventions was 9.50 weeks. The most dose optimization used was 4 mg/day (25.0%) for GXR, 1.8 mg/day (24.9%) for ATX, and 0.4 mg/day (33.0%) for CLON-XR. All studies evaluated the reduction from baseline to the endpoint in the ADHD-RS-IV total score and subtypes (inattention and hyperactivity/impulsivity).
Methodological quality of studies
Overall, the methodological quality of the studies was high. Most studies scored as “low risk” or “unclear” in the risk of bias summary (Supplementary Fig. S1). The only study that scored “high risk” in two indicators was considered to be of low quality (incomplete outcome data and selective outcome reporting items) (Childress et al. 2014), and the four studies that scored “high risk” in one indicator of bias were considered to be of average quality (Spencer et al. 2006; Connor et al. 2010; Findling et al. 2010; Newcorn et al. 2013). The “incomplete outcome data” item was most frequently evaluated as “high risk” since some studies did not adequately show all outcomes. Supplementary Figure S2 outlines the risk of bias assessment in these domains for the included studies.
Outcomes measures
All studies analyzed the absolute ADHD-RS-IV total symptom scores (Dupaul et al. 1998) and subtypes (inattention and hyperactivity/impulsivity), the ADHD-RS-IV was selected for its internal consistency and concurrent validity with attention problems assessed using the Achenbach scale (Achenbach 1991; McGoey et al. 2007). Also, several studies reported TEAEs (Spencer et al. 2006; Biederman et al. 2007, 2008; Findling et al. 2008, 2010; Sallee et al. 2009; Takahashi et al. 2009; Connor et al. 2010; Findling et al. 2011; Jain et al. 2011; Coghill et al. 2013; Newcorn et al. 2013; Childress et al. 2014; Hervas et al. 2014; Wilens et al. 2015) and secondary outcomes related to medications such as pulse rate (Sallee et al. 2009; Connor et al. 2010; Findling et al. 2010, 2011; Coghill et al. 2013; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015), SBP (Biederman et al. 2008; Findling et al. 2008, 2010; Sallee et al. 2009; Connor et al. 2010; Findling et al. 2011; Coghill et al. 2013; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015), and DBP (Biederman et al. 2008; Findling et al. 2008, 2010; Sallee et al. 2009; Takahashi et al. 2009; Connor et al. 2010; Findling et al. 2011; Coghill et al. 2013; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015).
Treatment-emergent adverse events
The most frequent (mean percentages) adverse effects associated with the use of stimulant and nonstimulant medications, respectively, were the following: decreased appetite (28.6%; 14.2%), nausea (7.9%, 10.3%) headache (14.5%, 20.8%), insomnia (12.3%, 8.6%), nasopharyngitis (6.0%, 7.1%), dizziness (5.1%, 10.0%), abdominal pain (7.8%, 11.5%), irritability (9.3%, 6.9%), somnolence (4.4%, 34.1%), and fatigue (4.3%, 16.0%). Supplementary Table S1 details the information on TEAEs observed in each study.
Ten studies reported on pulse rate, SBP, and DBP (Spencer et al. 2006; Biederman et al. 2008; Sallee et al. 2009; Connor et al. 2010; Findling et al. 2010, 2011; Coghill et al. 2013; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015). For pulse rate, there was a mean increase of 3.50 bpm in the stimulant group (Spencer et al. 2006; Findling et al. 2010, 2011; Coghill et al. 2013), and a reduction with nonstimulant medication use of −3.06 bpm (Sallee et al. 2009; Connor et al. 2010; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015). The mean SBP increased with stimulant medications by 1.46 mmHg (Findling et al. 2008, 2010; Findling et al. 2011; Coghill et al. 2013) and decreased with nonstimulant medications by −3.92 mmHg (Biederman et al. 2008; Sallee et al. 2009; Connor et al. 2010; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015). Similarly, the DBP showed a mean increase of 1.98 mmHg (Findling et al. 2008, 2010; Findling et al. 2011; Coghill et al. 2013) in participants using stimulant medications, and a mean reduction of −1.52 mmHg (Biederman et al. 2008; Sallee et al. 2009; Connor et al. 2010; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015) in those using nonstimulant medications; this reduction was caused by alpha-2 agonists (Biederman et al. 2008; Sallee et al. 2009; Connor et al. 2010; Newcorn et al. 2013; Hervas et al. 2014; Wilens et al. 2015), and partly reduced by the deviation of the atomoxetine that was positive (mean increase 3.93 mmHg in the two trials) (Takahashi et al. 2009; Hervas et al. 2014). However, none of these differences were statistically significant.
Meta-analysis results
Figure 2 shows the pooled estimates (SMD, 95% CI) of the effectiveness for all studies, and for each medication subgroup, that is, stimulants and nonstimulants, on reducing ADHD symptoms. The results showed a medium effect on the ADHD-RS-IV total score (SMD = −0.70, 95% CI: −0.85 to −0.55). Stimulant medications showed a larger effect (SMD = −0.83; 95% CI: −1.11 to −0.54) compared to nonstimulant medications, which showed a medium effect (SMD = −0.58; 95% CI: −0.69 to −0.46). Significant heterogeneity and important variability were found in the overall analysis (χ 2 = 97.38; df = 17; p < 0.001; I 2 = 83%) and in the stimulants subgroup (χ 2 = 72.73; df = 8; p < 0.001; I 2 = 89%), this was not significant in the nonstimulants subgroup (χ 2 = 13.80; df = 8; p = 0.090; I 2 = 42%).
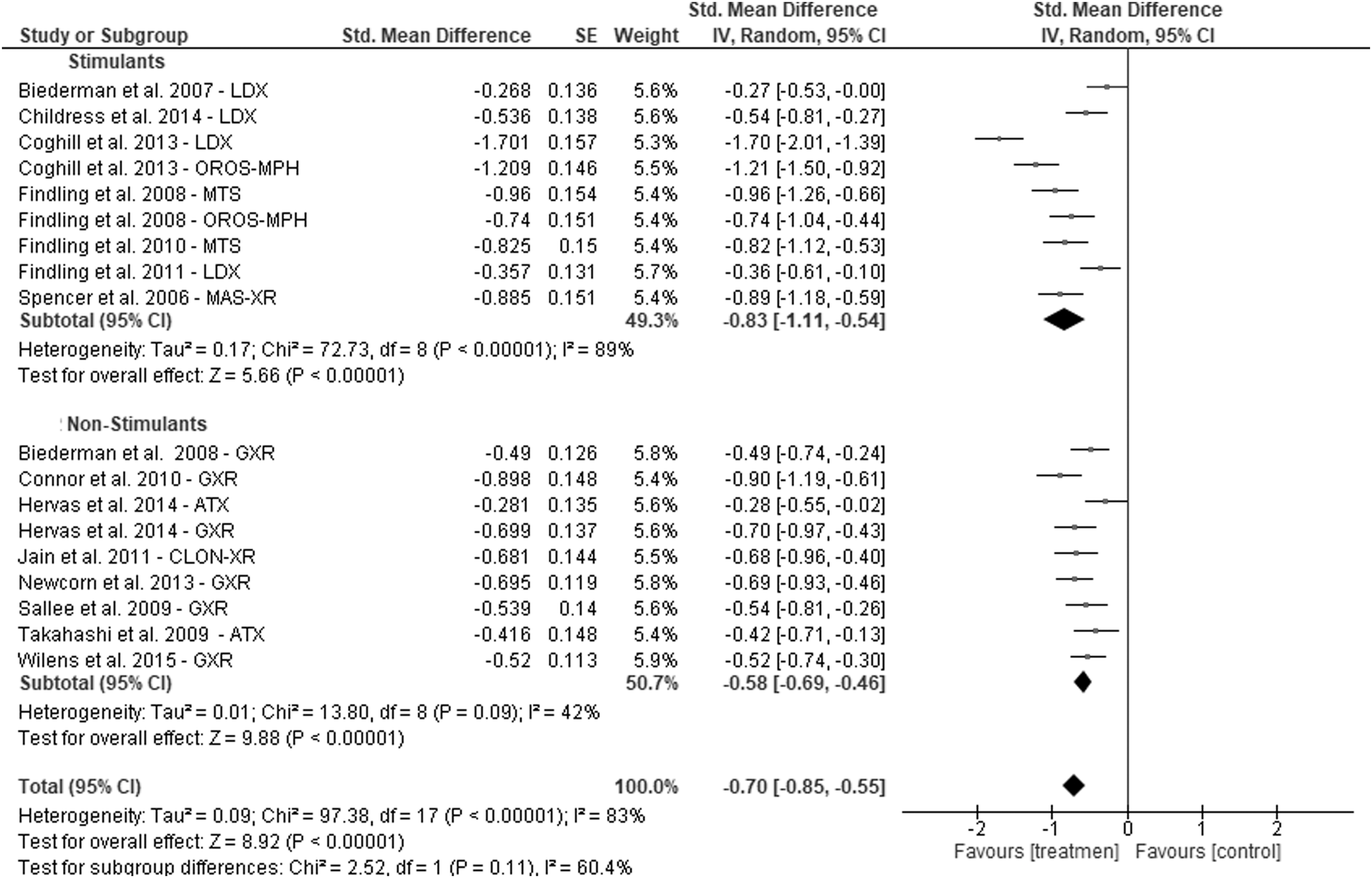
Forest plot total score.
Figures 3 and 4 show the pooled estimates of the effectiveness of stimulant and nonstimulant medications according to ADHD subtype (inattention and hyperactivity/impulsivity subtypes). The results showed a medium effect in the inattention subtype (SMD = −0.57: 95% CI: −0.76 to −0.38; I 2 = 87%) and similar results in the hyperactivity–impulsivity subtype (SMD = −0.58; 95% CI: −0.75 to −0.40; I 2 = 85%). In the inattention subtype, stimulant medications had a greater effect (SMD = −0.74, 95% CI, −1.20 to −0.28; I 2 = 94%) than nonstimulant medications (SMD = −0.46, 95% CI, −0.58 to −0.34; I 2 = 47%); similarly, in the hyperactivity–impulsivity subtype, the effect of stimulants was greater (SMD = −0.68, 95% CI, −1.09 to −0.27; I 2 = 92%) compared with nonstimulants (SMD = −0.52, 95% CI, −0.67 to −0.37; I 2 = 66%). Statistically significant within-group heterogeneity was found in the parameters and the overall analysis, except for the inattention subtype with nonstimulant medications.

Forest plot inattention.
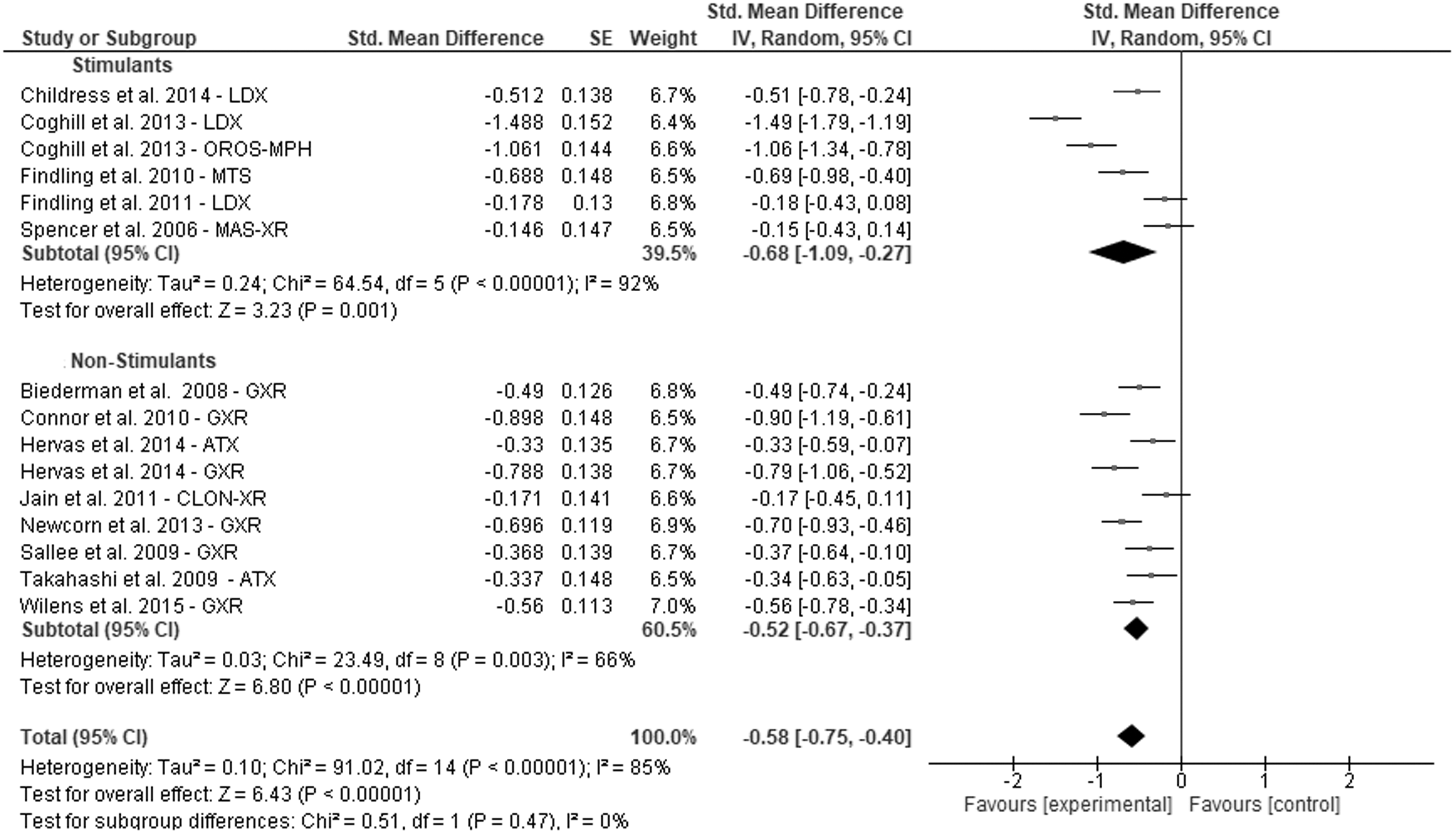
Forest plot hyperactivity/impulsivity.
According to the subgroup analyses (Fig. 5), four studies that included LDX medications (stimulants) showed a medium effect on the ADHD total score (SMD = −0.71, 95% CI, −1.32 to −0.11; I 2 = 95%); six studies that evaluated the effect of GXR (nonstimulants) also showed a medium effect (SMD = −0.63, 95% CI, −0.75 to −0.51; I 2 = 22%). In the inattention subtype, LDX (SMD = −0.78, 95% CI, −1.60 to 0.03; I 2 = 96%) and GXR (SMD = −0.54, 95% CI, −0.66 to −0.42; I 2 = 24%) had a medium effect. Finally, in the hyperactivity–impulsivity subtype, GXR also had a medium effect (SMD = −0.63, 95% CI, −0.77 to −0.48; I 2 = 50%), but this was not found for LDX (SMD = −0.72, 95% CI, −1.47 to 0.02; I 2 = 96%).
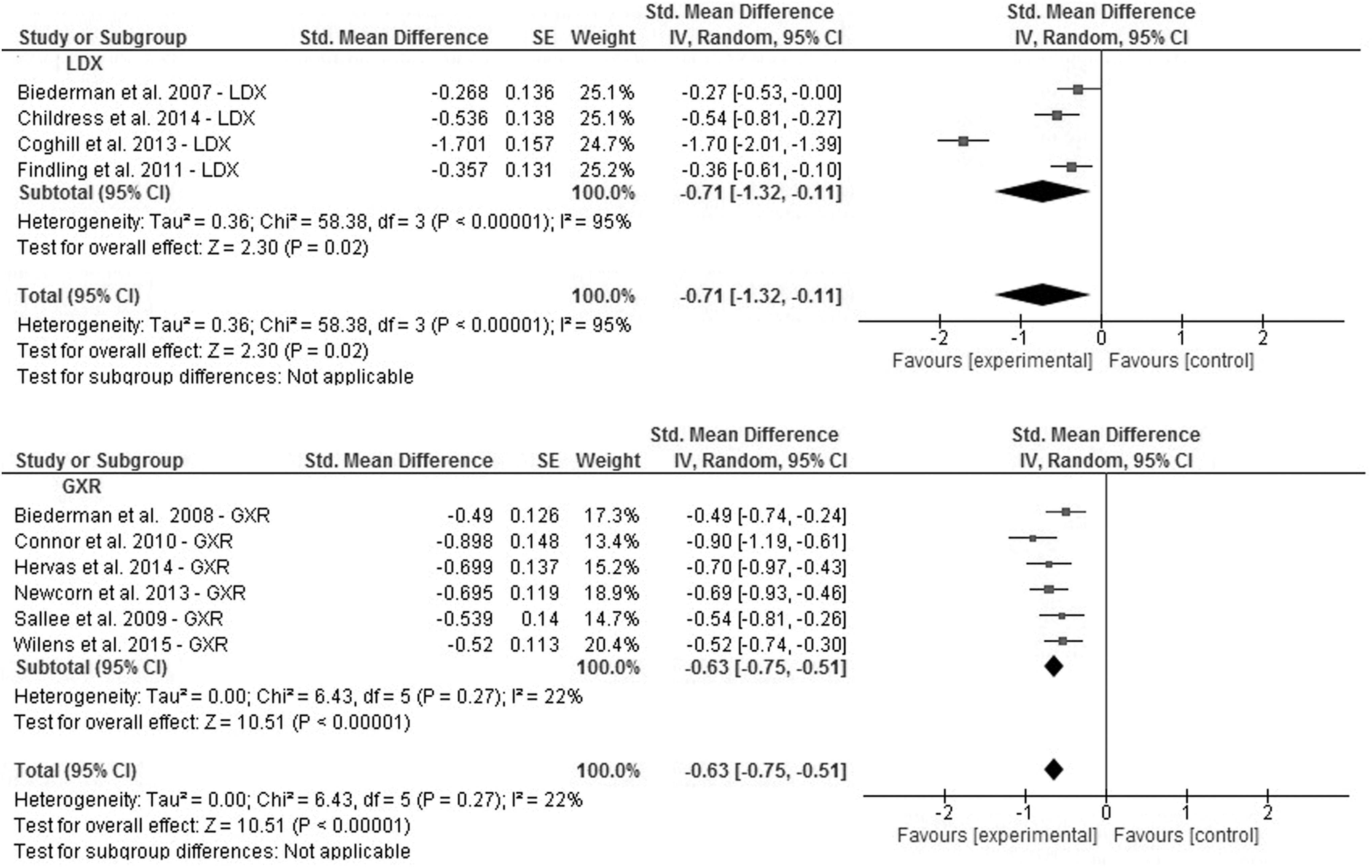
Forest plot total score LDX and GXR. GXR, guanfacine extended-release; LDX, lisdexamfetamine dimesylate.
Subgroup analyses were conducted to determine whether effects differed according to the age group (6–12, 13–17 or 6–17 years) and type of medication used (stimulant and nonstimulant medications). The age group with the greatest effect was 6 to 17 years (SMD = −1.43, 95% CI, −1.64 to −1.23; I 2 = 81%) for stimulant medications, and 6 to 12 years (SMD = −0.78, 95% CI, −0.96 to −0.59; I 2 = 13%) for nonstimulant medications. This analysis showed that the heterogeneity continued being high, except for children in the 6–12 year group in nonstimulant medications, MTS (SMD = −0.89, 95% CI, −1.10 to −0.68; I 2 = 0%) and ATX (SMD = −0.34, 95% CI, −0.54 to −0.15; I 2 = 0%) (Table 3).
ATX, atomoxetine; CLON-XR, clonidine hydrochloride extended-release; GXR, guanfacine XR; MAS, mixed amphetamine salts extended-release; MTS, methylphenidate transdermal system; LDX, lisdexamfetamine dimesylate; OROS-MPH, methylphenidate extended-release; SE, standard error; SMD, standard mean difference.
Finally, the placebo group also showed a medium effect on the ADHD-RS-IV total score (SMD = −0.68, 95% CI, −0.82 to −0.54; I 2 = 73%) (Supplementary Fig. S3).
GRADE assessment of the main analyses
On the basis of the GRADE system (Supplementary Tables S2 and S3), pooled data for the ADHD-RS-IV total score and for the inattention and hyperactivity/impulsivity subtypes were classified as moderately high evidence for both stimulant and nonstimulant medications. The strength of the evidence was lowered by the high degree of heterogeneity in the pooled results (I2 > 75%).
Publication bias and sensitivity analysis
There was a significant publication bias for all of the outcome variables and the number of studies required, as evidenced by the visualization of funnel plot asymmetry and an Egger regression intercept of −13.89, 95% CI, −25.29 to −2.48, p = 0.02 (Supplementary Fig. S4). Furthermore, in the sensitivity analysis, with each study deleted from the model once, the results remained statistically significant across all deletions.
Discussion
To the best of our knowledge, this is the first meta-analysis focused specifically on RCTs examining the evidence regarding the effects of stimulant and nonstimulant medications in children and adolescents with ADHD using the same outcome measure of ADHD symptoms (ADHD-RS-IV). Furthermore, this study reviewed the effects of medications in different ADHD subtypes (inattention and hyperactivity/impulsivity), and described TEAEs and secondary outcomes related to these medications, such as pulse rate and blood pressure. Our results suggest that, in children and adolescents, both stimulant and nonstimulant treatments are effective at reducing ADHD symptoms, although in all analyses, stimulant medications had a greater effect than nonstimulant ones. Moreover, no difference was found between the two types of medications in the frequency of adverse effects.
Stimulant medications
Regarding medication choice, most children with ADHD have comorbid psychiatric and learning disorders, and for the majority of them, stimulants are recommended as first-line treatment (Pliszka et al. 2006; Kolar et al. 2008; NICE 2008; Chan et al. 2016). Regarding this, a recent meta-analysis by Stuhec et al. (2015) reported that LDX is the most effective treatment (SMD = −1.28, 95% CI, −1.84 to −0.71) in terms of ADHD total score. A previous meta-analysis by Faraone (2009) highlighted the effect variability of ADHD medications and suggested that the efficacy of immediate-release (SMD = 0.99, 95% CI, 0.88–1.1) and long-acting stimulants (SMD = 0.95, 95% CI, 0.85–1.1) was greater compared with nonstimulants (SMD = 0.57, 95% CI, 0.53–0.62). In light of these results, several authors have suggested that LDX should be the first-line treatment of ADHD in children and adolescents (Findling et al. 2011; Coghill et al. 2014). Our estimates (SMD −0.71) are lower than those of these authors, but similar to other studies and meta-analyses in the adult population, in which the pooled SMD ranged from 0.57 and 0.86 (Wigal et al. 2009; Findling et al. 2011; Stuhec et al. 2016). Differences in inclusion criteria could be behind the differences between our results and those of Stuhec et al. (2015) and Faraone (2009), since our meta-analysis only included studies using the ADHD-RS-IV scale as the outcome measure, while in the two other meta-analyses, a wide variety of scales and questionnaires was used to assess ADHD symptoms.
Our data show that all stimulants had a medium effect on the ADHD-RS-IV total score, although OROS-MPH had the greatest effect in the inattention and hyperactivity/impulsivity subgroups; conversely, MAS XR had the lowest effect, and no differences were found among all stimulant medications. Although OROS-MPH showed good results, a poor response to MPH has been observed in children younger than 6 years (Loney et al. 1978), with a greater incidence of aggressive symptoms.
Nonstimulant medications
The efficacy and safety of nonstimulant medications in the treatment of ADHD have also been established, and they are recommended when there are comorbidities (Wilens and Biederman 1992). In this group, ATX constitutes a reasonable alternative for those cases in which stimulants are inadvisable, ineffective, or intolerable (Sibley et al. 2014). As in the case of stimulant medications, our effect estimates were more modest than those of Stuhec et al. (2015) and Schwartz and Correll (2014), also likely because of our strict inclusion criteria regarding the instrument used for measuring ADHD symptoms. Thus, while our SMD pooled estimate for ATX for the ADHD total score was −0.34, the estimates in the above-referenced meta-analyses were −0.68 and −0.64, respectively.
Placebo effect
Similar to other studies (Waschbusch et al. 2009; Sandler et al. 2010), the placebo group reported a medium effect on the ADHD-RS-IV total score, confirming that the placebo alone or combined with other medications can improve ADHD symptoms (Supplementary Fig. S3). It has been suggested that placebo effect implies neurochemical and neurophysiological changes (Mayberg et al. 2002), in such a way that participation in clinical research may itself be therapeutic (Horwitz and Horwitz 1993). However, it must be taken into account that the placebo effect may be influenced by a variety of factors, including the natural history of the disease, concomitant treatments, obliging reports, outcome reporting bias, informed consent, and/or severe methodological defects in the studies (Kienle and Kiene 1996; Hrobjartsson et al. 2011). Particularly important in the assessment of treatment response in children and adolescents with ADHD is to consider that placebos might positively influence parents' and teachers' expectancies about the effect of administering medication, and as consequence, their ratings could be positively biased. More research providing better understanding regarding the influence of medication expectancies on response treatment is needed.
Adverse effects
As has been previously reported (Banaschewski et al. 2004; Charach et al. 2004; Graham et al. 2011), the most frequent adverse effects for stimulant medications are decreased appetite, headache, insomnia, and irritability, while for nonstimulant medications these are somnolence, headache, and fatigue. Thus, the spectrum of symptoms differs between stimulant and nonstimulant medications, although there were no differences observed in our study.
Limitations and directions for future research
First, our results should be interpreted cautiously because of the limited number of studies for each group of medications. Second, our inclusion criteria specified that only studies evaluating ADHD using the ADHD-RS-IV instrument were included; this favors precision, and likely the validity of our estimates because this reduced heterogeneity by using only the most universally accepted instrument; however, this reduced comparability with other studies using different instruments or symptoms; therefore, both limitations should be taken into account for future research. Third, in most studies, it was not reported if subjects were taking another type of medication. Fourth, several designs did not adjust the dose based on the patient's weight or age. Fifth, studies did not inform what version of the ADHD-RS-IV scale was used (parents vs. school), or if it was through an interview by the researcher; therefore, we do not know the reliability of the data collection procedures. Sixth, most of the studies were funded by the pharmaceutical industry and this was not taken into account in the risk of bias as “other potential threats to validity.” Finally, like many other meta-analyses on this issue, the effects of stimulant and nonstimulant medications were heterogeneous regarding the wide variety of available medications and dose optimization.
Conclusions
This is the first meta-analysis estimating the effect of stimulant and nonstimulant medications on ADHD symptoms that includes only RCTs using the ADHD-RS-IV as the instrument for evaluating symptoms. Our results suggest that both stimulant and nonstimulant treatments are useful for attenuating ADHD symptoms in children and adolescents. In both the ADHD total scores and subtypes, the efficacy of stimulant medications was greater compared with nonstimulants. Although there were no differences, the frequency of various adverse effects was slightly different between stimulant and nonstimulant medications.
Clinical Significance
The results of this meta-analysis provide information to clinicians about several therapeutic options for children and adolescents with ADHD, showing better beneficial effects with stimulant medications. Future ADHD research should be designed to examine the effects of dosage, frequency, intensity, and treatment duration upon the observed clinical outcomes, including long-term efficacy.
Footnotes
Acknowledgment
A.G.H. is funded by Proyectos Basales (Proyecto 051641ZR_DAS) y Vicerrectoría de Investigación, Desarrollo e Innovación (Universidad de Santiago de Chile, USACH).
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.