
Abstract
Objectives:
The use of antipsychotic drugs by youth is associated with serious side effects, especially when prescribed in higher dosages and for a longer period. Despite this, little is known about recent trends in the dosages and duration of use of antipsychotic drugs in children and adolescents. The aim of this study was to describe trends in prevalence, incidence, dosages, duration of use, and preceding psychotropic medication in Dutch youth who had been prescribed antipsychotic drugs from 2005 to 2015.
Methods:
We analyzed 84,828 antipsychotic prescriptions of youths aged 0–19 years between 2005 and 2015, derived from a large Dutch community pharmacy-based prescription database (IADB.nl).
Results:
Since a peak of 9.8 users per 1000 youths in 2009, prevalence rates stabilized. Dosages in milligram per kilogram declined for the most frequently prescribed antipsychotic drugs during the study period. The median duration of use was 6.0 (95% CI 5.4–6.6) months. Boys used antipsychotic drugs significantly longer than girls, with a median of 6.9 (95% CI 6.1–7.7) versus 4.6 (95% CI 3.9–5.3) months (p < 0.01). Of the youths prescribed antipsychotics, 12.4% used them for at least 48 months. The majority of youths had used other psychotropic agents in the year before the start of an antipsychotic drug (62.4% in 2005 and 64.7% in 2015).
Conclusions:
Despite a stabilization of usage rates and decline in dosages and duration of use, one in eight youths still used antipsychotic drugs for 4 years or longer. A substantial share of youths may, therefore, be at high risk for serious side effects.
Introduction
T
However, in recent years, concerns have been raised regarding the use of antipsychotic drugs in children. For instance, off-label prescriptions are very common, which involves particular risks as evidence for efficacy is often lacking (Sohn et al. 2016). More importantly, few studies have adequately monitored long-term antipsychotic safety profiles in children. Indeed, second-generation antipsychotics appear to have major side effects, including weight gain, metabolic abnormalities, and extrapyramidal symptoms (Cohen et al. 2012). Moreover, it has been suggested that some side effects are more common in children than in adults (Vitiello et al. 2009). These might have a major impact later in life, as metabolic changes and tardive dyskinesia can be irreversible even upon drug discontinuation. Children receiving antipsychotic medication indeed show an increased risk of developing type 2 diabetes and metabolic syndrome, which significantly affects future quality of life and life expectancy (Calarge et al. 2009; Bobo et al. 2013).
Given these concerns, pharmacoepidemiological research is crucial to monitor the extent of antipsychotic drug use in youth. Unfortunately, however, few studies have reported on the duration of use or the dosages of antipsychotics in children and adolescents (Kalverdijk et al. 2008; Burcu et al. 2014; Nakane et al. 2014; Verdoux et al. 2015), whereas especially high dosages and long duration of use might enhance the risk for serious side effects (Laita et al. 2007; Bobo et al. 2013). Furthermore, although comedication has been widely described, to our knowledge, no study has addressed the use of psychotropic medication preceding the start of an antipsychotic drug in children. Thus, it would be valuable to evaluate whether the prescription of stimulants precedes antipsychotic treatment. Although aggressive, maladaptive behavior is an important indication for antipsychotic drug use in youths (Schroder et al. 2017), stimulants have emerged as an alternative to antipsychotics to treat aggression associated with attention-deficit/hyperactivity disorder (ADHD) (Connor et al. 2002). Finally, as recent research showed that prevalence rates of antipsychotic use differ remarkably between countries (Kalverdijk et al. 2017), it is of interest to know how trends on incidence and duration of therapy explain these differences. Since 2005, no such information concerning antipsychotic drug use in youth in the Netherlands is known (Kalverdijk et al. 2008).
Therefore, the aim of this study is to examine antipsychotic drug prescription trends for children and adolescents in the Netherlands from 2005 to 2015, including the prevalence, incidence, dosages, and duration of therapy. We provide, to our knowledge, the first descriptions of trends in dosages of antipsychotic drugs in youths in a Western population.
Methods
Data source
This study was performed with pharmacy dispensing data from the population-based prescription database IADB.nl (Visser et al. 2013). The IADB database comprises prescription drug dispensing data from community pharmacies in the northern and eastern part of the Netherlands from 1994 onward, covering a population of approximately 600,000 people. This population largely corresponds to the composition of the general Dutch population (Visser et al. 2013). It includes all prescriptions, irrespective of type of health insurance (also including people without insurance), prescriber, and reimbursement status. Prescriptions during hospital stays are not included.
The total population estimates were based on general population statistics from the Dutch Central Bureau for Statistics. First, cities completely covered by IADB pharmacies were analyzed, to determine the proportion of the population visiting the pharmacy at least once a year. This proportion was used to estimate the coverage of IADB pharmacies in all other areas.
The study database IADB.nl uses deidentified medical records that could not lead to individual patients. According to the Code of Conduct for Health Research by the Foundation Federation of Dutch Medical Scientific Societies, being approved by Dutch data protection authority in 2004 (Foundation Federation of Dutch Medical Scientific Societies 2004), no ethics committee approval is needed for research using anonymous medical records. This study was conducted in accordance with the Declaration of Helsinki.
Study sample and variables
Patients aged 0 through 19 years who used at least one antipsychotic drug between January 1, 2005, and December 31, 2015, were selected. Antipsychotic drugs were defined as class N05A according to the World Health Organization's Anatomical Therapeutic Chemical/Defined Daily Dose Classification System, except from N05AN (lithium). Clozapine, olanzapine, quetiapine, sulipiride, risperidone, aripiprazole, paliperidone, serindole, and lurasidone were considered second-generation antipsychotics. The remaining drugs of class N05A were considered first-generation antipsychotics.
All other psychotropic drugs were defined as anxiolytics (class N05B), hypnotics and sedatives (class N05C), antidepressants (class N06A), psychostimulants (class N06B), lithium, clonidine, carbamazepine, and valproic acid.
Data analyses
First, prevalence and incidence rates of antipsychotic drug use per year per 1000 youths in the population were calculated. A new (incidental) user was defined as a youth being present in the database for at least 90 days and receiving an antipsychotic drug prescription for the first time. Prescription data from 2004 were used to identify starters in 2005. We stratified prevalence and incidence by gender, age group (0–6 years, 7–12 years, 13–19 years), and type of drug. Incidence rates were also stratified by type of prescriber (GP or specialist). Confidence intervals (CIs) were calculated using the Score method with continuity correction (Tobi et al. 2005). Proportions were compared using the chi square test.
Then we performed a dose analysis. Weight of the children was estimated using the Denekamp scale to provide milligram per kilogram dosages (Kinderformularium 1997). The Denekamp scale provides the median weight for boys and girls at different ages, based on anthropometric references of Dutch youth. Prescriptions of the four most prescribed antipsychotics were used for the dose analysis. Only prescriptions issued for at least 7 days were selected to exclude rescue medication. Pipamperone was excluded from the dose analysis as this is often prescribed as a 40 mg/mL liquid formulation and daily dose was not consequently noted in the database as milliliters (mL) or milligrams (mg). The age on the first of January of the year of prescription was used. Means are presented as value ± the standard deviation (SD).
We calculated duration of antipsychotic drug use by median and mean survival times using Kaplan–Meier analyses. The start of an episode of antipsychotic drug use was defined as already described. An episode ceased if at least the number of days for which medication was prescribed plus 90 days had passed and the youth could still be followed in the database. All other cases were considered censored. Duration of use was stratified by gender, age groups (at time of start of the antipsychotic drug), start year, and type of drug. Subgroups were compared using the Logrank test. Starters from the year 2015 were excluded from the survival analysis, as the cohort could only be followed until the end of 2015, and in this year high rates of censoring would take place. Duration of antipsychotic use was presented in months, with 30 days being considered 1 month.
An analysis on preceding psychotropic medication was also performed. Psychotropic prescriptions issued 1 year before the first antipsychotic drug prescription were considered as preceding psychotropic medication. Concurrent psychotropic treatment was defined as a psychotropic prescription being issued within the start and stop date of an antipsychotic drug prescription. Prescriptions were stratified by year and gender.
Differences were considered significant at p < 0.05. Statistical analyses were performed with SPSS for windows, version 21 and Microsoft Excel 2010.
Results
The total population aged 0–19 years ranged from 131,980 persons in 2005 to 126,666 persons in 2015. The total number of antipsychotic prescriptions of youths aged 0–19 years between 2005 and 2015 was 84,828.
Prevalence
The overall prevalence of antipsychotic drug use ranged from 7.2 (95% CI 6.8–7.7) in 2005 to 9.0 (95% CI 8.5–9.5) per 1000 youths in 2015. The prevalence rates stratified for age, gender, and year are presented in Table 1. The prevalence was highest in 2009 with 9.8 (95% CI 9.3–10.3) users per 1000 youths (Fig. 1). Boys were more likely to use antipsychotic drugs in all years and in all age groups. The most frequently prescribed antipsychotic drugs were risperidone (61.9% of all antipsychotic drug users), pipamperone (18.2%), aripiprazole (9.5%), quetiapine (9.3%), and olanzapine (3.7%). Trends of the three mostly prescribed antipsychotics are shown in Figure 1. The prevalence of first-generation antipsychotics ranged from 2.2 (95% CI 2.0–2.5) in 2005 to 2.3 (95% CI 2.1–2.6) in 2010 and 1.6 (95% CI 1.4–1.8) in 2015 per 1000 youths. The prevalence of second-generation antipsychotics increased from 5.4 (95% CI 5.0–5.8) in 2005 to 7.8 (95% CI 7.3–8.3) in 2015 per 1000 youths.
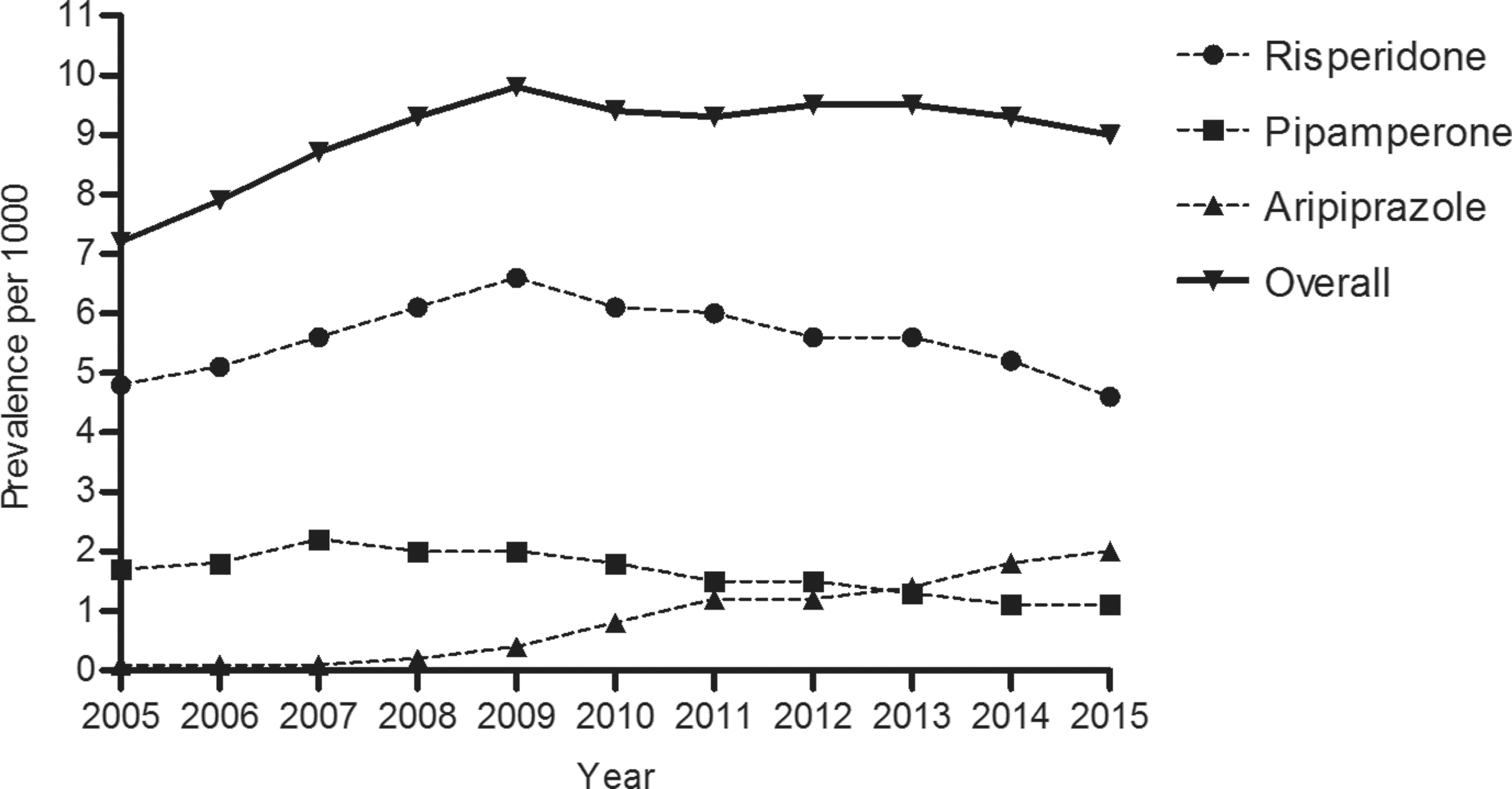
Prevalence of antipsychotic prescriptions in youth aged 0–19 years. Prevalence per 1000 youths. Prevalence of the unique agents adds up to more than the total prevalence, as one patient can contribute to more than one line.
n = 66,430 boys, n = 65,550 girls.
n = 70,255 boys, n = 67,996 girls.
n = 64,777 boys, n = 61,889 girls.
p < 0.05, significantly different compared with baseline (2005).
Incidence
The overall incidence rate was 2.0 (95% CI 1.8–2.3) per 1000 minors both in 2005 and in 2015. Incidence peaked in 2007 with 2.6 (95% CI 2.3–2.9) new users per 1000 aged 0–19 years. The incidence rates, stratified for age, gender, and year, are presented in Table 2. Risperidone was the preferred antipsychotic drug to start with for all age categories in all years. Antipsychotic drugs were mainly started by specialists (2005: 75.5%, 2015: 67.8%).
n = 66,430 boys, n = 65,550 girls.
n = 70,255 boys, n = 67,996 girls.
n = 64,777 boys, n = 61,889 girls.
p < 0.05, significantly different compared with baseline (2005).
Dosages
For 13,006 prescriptions, analysis of the dosing (in milligram per kilogram) could be performed. For the four mostly used antipsychotics, the mean dosage decreased from 2005 to 2015, with the largest decrease for aripiprazole and quetiapine. The mean dosage (±standard deviation) for aripiprazole was 0.29 mg/kg (±0.16) in 2005 and 0.11 mg/kg (±0.09) in 2015. The mean dosage for quetiapine decreased from 3.53 mg/kg (±3.00) in 2005 to 0.93 mg/kg (±1.09) in 2015. For risperidone, the mean dosage was 0.03 mg/kg (±0.03) in 2005 and 0.02 mg/kg (±0.03) in 2015; for olanzapine, the mean dosage was 0.12 mg/kg (±0.09) in 2005 and 0.09 mg/kg (±0.06) in 2015.
Duration of use
The overall median and mean duration of use of antipsychotic drugs were 6.0 months (95% CI 5.4–6.6) and 19.1 months (95% CI 17.8–20.4) respectively, with considerable differences between subgroups (Table 3).
Analysis was performed for the years 2005–2014.
Analysis for the years 2011–2013, as in these years aripiprazole was prescribed to a considerable share of the total population.
The duration of use was longest for children aged 7–12 years with a median of 9.8 months (95% CI 8.1–11.4) and a mean of 25.5 months (95% CI 23.2–27.8) (Fig. 2). Boys had a significantly longer duration of therapy than girls, which was consistent over the years (p < 0.01). Overall, risperidone was prescribed for the longest period.
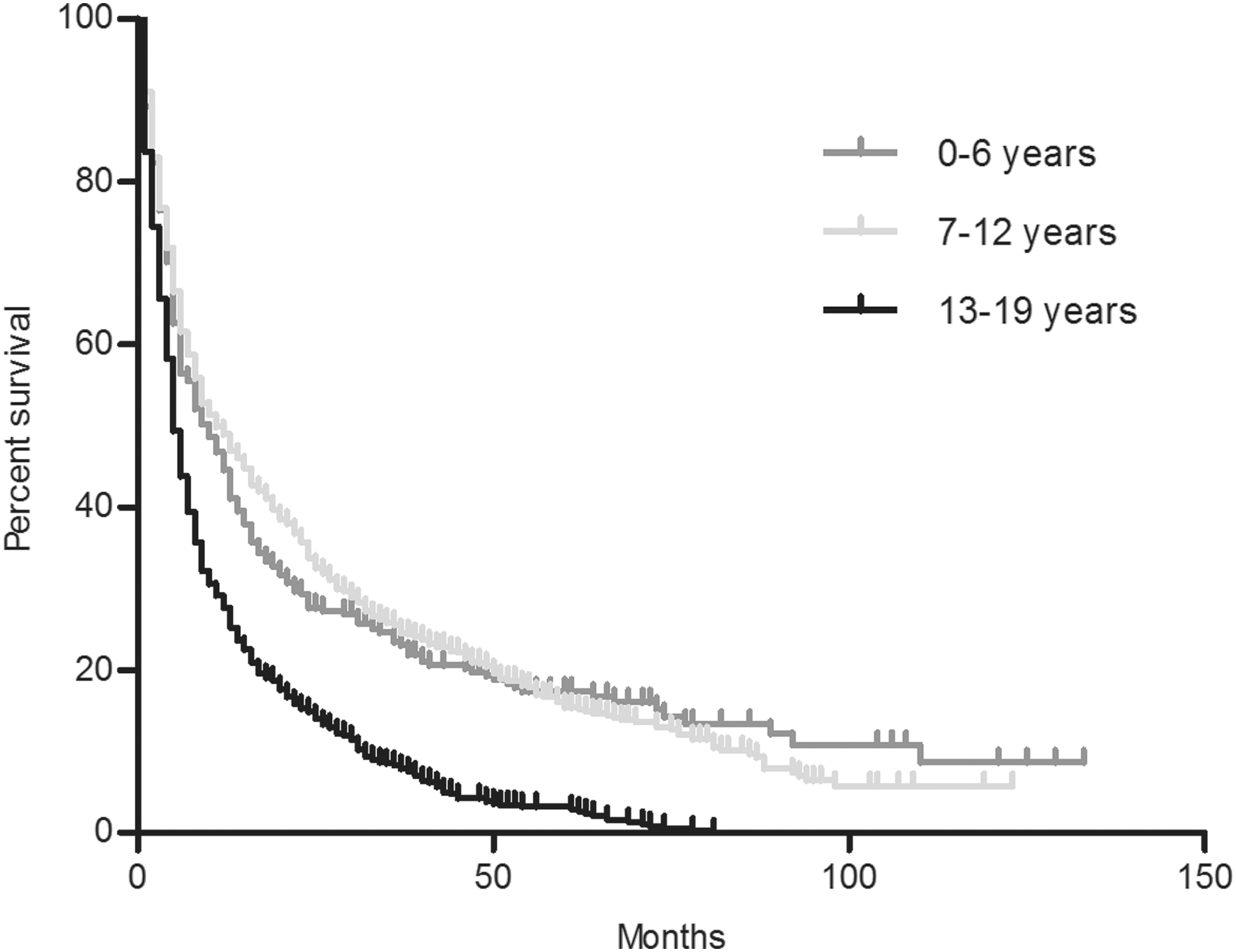
Duration of antipsychotic drug use in youth aged 0–19 years. Kaplan–Meier survival curve; tick marks indicate censored data. Analysis was performed for the years 2005–2014.
A large difference between the median and mean durations of therapy can be seen. This means that a small share of patients used antipsychotic drugs for a relatively long period. Overall, 12.4% of the youths used antipsychotic drugs for at least 48 months. As is shown in Figure 2, 19.4% of the children aged 7–12 years used an antipsychotic drug for 48 months or longer.
Other psychotropic medication
The majority of the population used other psychotropic medication in the year before the first start of an antipsychotic drug. This is consistent through the years; in 2005, 62.4% and in 2015, 64.7% of children starting with antipsychotic treatment and used other psychotropic medication in the preceding year. Centrally acting sympaticomimetics, benzodiazepines, and selective serotonin reuptake inhibitors were prescribed most often in every year, both as preceding and concomitant medication. In 2005, 32.5% of youths were prescribed a stimulant in the year preceding the first prescription of an antipsychotic drug, in 2015 this was 36.4%. Approximately half of the patients used psychotropic comedication during antipsychotic treatment from 2005 to 2015 (51.3%), peaking in 2009 with 55.6%. Boys used more comedication than girls (49.4% vs. 47.1%), which was not statistically significant (p = 0.10).
Discussion
From 2005 to 2015 in the Netherlands, prevalence rates stabilized since a peak of 9.8 users per 1000 youths in 2009. The duration of use decreased to a median of 6.8 months and a mean of 10.9 months in 2014. Also, dosages per kilogram for the mostly prescribed antipsychotic drugs in youth declined. Furthermore, first time antipsychotic prescriptions were preceded by the use of other psychotropic medication in the majority of cases.
The major increase in antipsychotic drug use in youth who had been described in the Netherlands from 1997 to 2005 (Kalverdijk et al. 2008) continued until 2009. The recent stabilization in usage is similar in other countries such as the United States and Denmark (Goddard et al. 2016; Edelsohn et al. 2017; Halfdanarson et al. 2017). We found a decline of usage rates in the youngest age group aged 6 years or younger, which mirrors findings from other studies (Lohr et al. 2015; Schroder et al. 2017). However, the prevalence of usage in adolescents increased. The overall plateauing of antipsychotic drug use in children might be attributed to more awareness of serious side effects in youth among health professionals after growing evidence from the literature (Correll 2008; Cohen et al. 2012).
Nevertheless, the usage rates of antipsychotic drugs in Dutch youth remain fairly high compared with other European countries (Kalverdijk et al. 2017). For example, a German study carried out between 2004 and 2011 found a prevalence between 2.0 and 2.6 per 1000 minors and a French study conducted between 2006 and 2013 reported usage rates between 4.6 and 4.9 per 1000 youths (Verdoux et al. 2015; Schroder et al. 2017). Several factors might contribute to these differences. First, prevalence of psychiatric disorders may vary between countries, which can be partly due to differences in diagnosing patterns (Post et al. 2017). The most important registered psychiatric disorders that may warrant antipsychotic drug use by children and adolescents in the Netherlands include behavioral problems associated with autism spectrum disorder, bipolar disorder, and schizophrenia. However, for example, for pervasive developmental disorders such as autism, differences in prevalence by geographical region are not supported by current literature (Elsabbagh et al. 2012). Second, access to healthcare, child and adolescent psychiatrists, and prescription medicine might influence usage rates of antipsychotic drugs as well. In a densely populated country such as the Netherlands, the access to healthcare is more easily guaranteed than in a country with great regional differences such as France (Verdoux and Tignol 2003). Furthermore, the number of psychiatrists per persons in the Netherlands is one of the highest in Europe (World Health Organization 2015), which is reflected by the high rate of first prescriptions being issued by specialists in this study. Also, access to prescription medicine for children in the Netherlands is guaranteed, as health insurance is compulsory and antipsychotics are fully reimbursed. Third, prescription behavior of child and adolescent psychiatrists might be influenced by cultural factors or differences in training. For example, French psychiatrists are known to have a more psychoanalytical basis and might thus be more reluctant to prescribe psychotropic drugs (Verdoux 2007).
Despite the relatively high prevalence, the duration of use decreased from a median of 1.9 years during 1997–2005 (Kalverdijk et al. 2008) to a median of 6.0 months during 2005–2015, although a sizable share of children and adolescents used antipsychotic drugs for a long time. For example, 19.4% of children treated with an antipsychotic drug aged 7–12 years used antipsychotics for 4 years or longer. These children might benefit substantially from such treatment. However, simultaneously, a longer duration of use might incur a greater risk to develop side effects, such as dyskinetic movements, metabolic changes, and the development of diabetes (Laita et al. 2007; Bobo et al. 2013). Remarkably, few studies describe duration of antipsychotic drug use in youth. Verdoux et al. (2015) reported a median duration of only 1 month in a French community-based study, which suggests that these concerns mainly rescue medication for managing acute behavioral problems. Burcu et al. (2014) described a median duration of use of 180 days in a population of Medicaid-insured youth, similar to our findings.
Consistent with earlier findings (Kalverdijk et al. 2008; Burcu et al. 2014), boys showed a significantly longer duration of use than girls. As mentioned, other studies have shown that antipsychotics in children are mainly prescribed to treat aggressive, impulsive, and hyperkinetic behavior associated with ADHD, autism, and mental retardation (Bachmann et al. 2014; Olfson et al. 2015; Schroder et al. 2017). We might speculate that this explains the longer duration of use in boys, as physical aggressive behavior is more prevalent among boys than among girls (Archer 2004), and might exist for a longer time. However, as boys differ in a lot of ways from girls, also other factors might contribute to the difference in duration of use.
For both stimulants and antipsychotic drugs, there is evidence for efficacy in aggressive and impulsive behavior associated with ADHD (Connor et al. 2002). These agents are often found to be used concomitantly (Alessi-Severini et al. 2012; Olfson et al. 2015; Burcu et al. 2016), which is also confirmed in this study. Interestingly in our study, we found that most first-time antipsychotic prescriptions in youth were not preceded by a stimulant prescription, although the latter agents are known to have a more favorable side effect profile. However, overall, most antipsychotic prescriptions were preceded by any type of other psychotropic medication. This is different from an earlier study conducted in adolescents with new onset psychotic symptoms, wherein most antipsychotics were not preceded by another psychotropic such as antidepressants or benzodiazepines (Woods et al. 2016). This finding might be explained by the sudden onset of psychotic symptoms and limited pharmacological treatment options other than antipsychotic drugs. This also might suggest that in our cohort, antipsychotics were mainly used to treat aggressive behavior rather than psychosis.
In our study, we found a trend toward lower dosages of antipsychotic drugs per kilogram from 2005 to 2015. A decrease in dosing in children has also been observed in a Japanese study (Nakane et al. 2014). This trend might be the result of the growing number of trials investigating antipsychotic drug use in children, generating new information on specific dosing schemes. For example, in aripiprazole, after its introduction on the market, adult dosing schemes were advised as no specific information for children was available. For both aripiprazole and risperidone, formal dose recommendations were only available from 2009 in the Netherlands. Besides these guideline changes, also other factors might have influenced the dose changes over time. These include gender and age of the patients in the cohort, being moderators of weight and, therefore, influencing dosing. In this study, we corrected for these factors using estimates of weight normalized for age and gender. Also, patients' ethnicities and socioeconomic statuses might impact dosing over time. Although these latter variables were not known in our cohort, we expect these factors to be fairly constant during the study period, as the area covered by the pharmacies that delivered the prescription data did not significantly change.
Implications for future research include further investigation of international trends in duration of therapy and dosages of antipsychotic treatment in youths. In this way, country-specific exposure of antipsychotic medication to children and adolescents can be better quantified. Furthermore, by identifying specific populations at risk, tailored interventions to prevent serious side effects can be made.
This study has several limitations. First, prescription rates do not represent actual usage rates, as medication might be taken in other dosages or not be taken at all. Second, the IADB database only includes pharmacies in the northern and eastern parts of the Netherlands, which might not be representative for the whole country as these regions consist of more rural areas than the western part of the country. Some literature suggests antipsychotic drug prescribing might increase with density of population for young children (Verdoux et al. 2015), which might have led to an underestimation of usage rates. Nevertheless, other studies do not show such an association (Alessi-Severini et al. 2012). However, the IADB database has previously proven to be representative for the whole Dutch population (Visser et al. 2013). Third, by our definition of a new incidental user, also patients on ongoing treatment with a discontinuation of at least 3 months are defined as a new user. Also, as no inpatient prescriptions are included in the database, children who were hospitalized for a longer period of time might have been defined as a new incidental user upon discharge as well. This might have resulted in an overestimation of incidence rates and an underestimation of duration of use. However, hospitalization in child and adolescence psychiatry is rather rare. Moreover, a more strict definition of new users might have led to more children falsely being not identified as new users, for example, when they moved into an area being covered by the database in the past months. Fourth, no information on diagnoses was available. Lastly, the analysis of dosages per kilogram was based on median weight reference values of Dutch youth. As antipsychotics are known to induce weight gain, the weight of the children in our cohort might be above average. Therefore, our analysis of dosages per kilogram might be an overestimation.
Strengths of this study are the use of a large data set that was not limited to type of health insurance or health provider, in a country that is representative of the Western developed world. We provide a unique analysis of trends in dosages, duration of therapy, and used preceding psychotropic medication, which is of great importance to address the health risks of use of antipsychotics in youths.
Conclusions
In the Netherlands, overall antipsychotic drug prescription rates among children and adolescents stabilized and dosages per kilogram declined from 2005 to 2015. Although overall duration of use decreased, one in eight youths used antipsychotic drugs for at least 4 years.
Clinical Significance
Youths with severe behavioral problems might substantially benefit from long-term antipsychotic treatment and high dosages. However, longer duration of use and higher dosages may also increase the risk for side effects of antipsychotics. Our study shows that a substantial share of Dutch youths who use antipsychotics use them for a considerable long time. Therefore, we recommend adequate screening for side effects in chronic users. Furthermore, healthcare providers should assess whether an attempt to discontinue antipsychotic drugs in chronic users is indicated.
Disclosures
The authors declare that they have no potential conflicts of interest.