l -Carnosine as Adjunctive Therapy in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder: A Randomized,Double-Blind,Placebo-Controlled Clinical Trial
Available accessResearch articleFirst published online June, 2018
l -Carnosine as Adjunctive Therapy in Children and Adolescents with Attention-Deficit/Hyperactivity Disorder: A Randomized,Double-Blind,Placebo-Controlled Clinical Trial
This study aimed to investigate the efficacy and tolerability of l-carnosine as an add-on to methylphenidate in management of children with attention-deficit/hyperactivity disorder (ADHD).
Methods:
This was an 8-week, randomized, double-blind placebo-controlled study. Fifty-six drug-free children and adolescents aged 6–17 years old with a diagnosis of ADHD entered the study. The patients were randomly assigned to l-carnosine (800 mg/d in two divided doses) or placebo plus methylphenidate (0.5–1.5 mg/kg/d) for 8 weeks. Children were assessed using the Teacher and Parent ADHD Rating Scale-IV (ADHD-RS-IV) at baseline and at weeks 4 and 8 postbaseline.
Results:
Fifty patients completed the study, and all had two postbaseline measurements. Using the general linear model repeated measures, significant effect was observed for time × treatment interaction on total and inattention subscales of the Parent ADHD-RS (Greenhouse-Geisser corrected: F = 3.783, df = 1.444, p = 0.041 and F = 4.032, df = 1.600, p = 0.030). Improvements in the Teacher ADHD-RS were not significantly different between the two groups in total (Greenhouse-Geisser corrected: F = 0.200, df = 1.218, p = 0.705), as well as inattention and hyperactivity subscale scores (p = 0.956 and 0.281, respectively). The frequency of side effects was not significantly different between the two treatment arms.
Conclusions:
l-carnosine, as a supplementary medication, might be beneficial in treatment of children with ADHD. However, further investigations and different doses of l-carnosine are required to replicate these findings in children with ADHD.
Introduction
Attention-deficit/hyperactivity disorder (ADHD) represents a neurodevelopmental condition affecting 3%–7% of children and is characterized by age-inappropriate inattentiveness and increased hyperactivity and impulsivity (Taylor et al. 2004; Fayyad et al. 2007; Willcutt 2012). ADHD is presumably associated to imbalance of catecholamine metabolism in the cerebral cortex and dysregulation of dopaminergic and noradrenergic neural circuits (Millichap 2008; Bauer et al. 2016). Treatment of ADHD focuses on administration of stimulants, including methylphenidate (Banaschewski et al. 2004). These stimulants produce complete remission in about only 30% of cases, and about 10%–30% of patients with ADHD may not respond to stimulants or may not be able to endure potential adverse events, including reduced appetite, sleep disturbances, mood lability, and exacerbation of comorbid tic disorders (Banaschewski et al. 2004; Steele et al. 2006). Since all cases cannot be attributed to one mechanism (Pliszka 2005), further neurotransmitter systems are becoming of interest for development of effective treatments for refractory ADHD patients (Durrant and Heresco-Levy 2014). Glutamate is the primary excitatory neurotransmitter found in the brain (Pittenger et al. 2011), essential in frontostriatal transmission and often co-transmitted with dopamine (Chuhma et al. 2009). Cortical glutamatergic activity is demonstrated to be decreased in some ADHD cases (Durrant and Heresco-Levy 2014). Moreover, dopaminergic and glutamatergic system neurotransmission studies and genetic evaluations have suggested involvement of the NMDA receptor dysregulation in ADHD pathophysiology (Kotecha et al. 2002; Turic et al. 2004). Altogether agents with effects on the dopamine and glutamate pathways, NMDA receptor, and GABA modulators are of interest as probable medications for ADHD treatment.
There is growing evidence for the use of Complementary or Alternative Medicines (CAMs; e.g., l-carnosine) in different neuropsychiatric disorders (Sarris et al. 2011; Ghajar et al. 2016). Evidence indicated that more than half of the children diagnosed with ADHD are treated with one or more CAMs by their parents (Chan et al. 2003). Therefore, evidence is required to support claims for efficacy of this treatment in this vulnerable group (Sarris et al. 2011). For those patients who cannot tolerate or have limited response to stimulants, or families who simply prefer nonstimulant therapy, finding new nonstimulus medicines and supplements that affect the disorder is essential (Greenhill et al. 2002; Banaschewski et al. 2004; Curtis and Patel 2008; Sarris et al. 2011).
One example of the supplements used is l-carnosine, a dipeptide of the β-alanine and l-histidine known as an antiaging, antioxidant, and neuroprotective compound, found in high concentrations in the brain tissue (Wang et al. 2000; Prokopieva et al. 2016). Carnosine, co-localized at glutamatergic synapses (Sassoè-Pognetto et al. 1993), is indicated to decrease glutamate levels, inhibit glutamate release, and is postulated as an NMDAR and GABA modulating agent (Shen et al. 2007, 2010; Brondino et al. 2016; Ouyang et al. 2016). Carnosine accumulates in the subfrontal cortex and may enhance the frontal lobe function (Trombley et al. 1998; Chez et al. 2002), the area of scientist's interest in ADHD patients. Particular characteristics of l-carnosine consist of being highly bioavailable, penetrable through the blood–brain barrier with few side effects, and no danger of overdose make it a drug of interest between CAMs (Prokopieva et al. 2016).
In this 8-week, double-blind placebo-controlled trial, we aimed to assess the efficacy of l-carnosine adjuvant to methylphenidate in treatment of children with ADHD. To the best of our knowledge, this study is the first double-blind and placebo-controlled clinical trial assessing the adjunctive role of l-carnosine in patients with ADHD.
Materials and Methods
Trial design and setting
This study was an 8-week, randomized, parallel group, double-blind placebo-controlled trial undertaken by outpatients at the Roozbeh Psychiatric Hospital affiliated with Tehran University of Medical Sciences (TUMS) during March 2016 to July 2017. The protocol was approved by the Institutional Review Board (IRB) of TUMS (Grant No. IR.TUMS.REC.1394.1290) and was in accordance with the Declaration of Helsinki and its successive revisions. After a complete description of the procedures and the purpose of the study, written informed consent was obtained from each patient's parent or their legal guardian. The trial was registered in the Iranian registry of clinical trials (www.irct.ir; trial identifier with the IRCT database: IRCT201601031556N84).
Participants
Subjects who initiated the study were newly diagnosed (drug naive) outpatient boys and girls aged 6–17 years who met the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria for ADHD supported by Kiddie Schedule for Affective Disorders (KSADS) (Ghanizadeh et al. 2006) and a medical history. Children were excluded if they had been previously diagnosed with a psychiatric comorbidity except for oppositional defiant disorder (ODD). Other exclusion criteria were history or current diagnosis of pervasive developmental disorders, mental retardation (defined as intelligence quotation below 70); any evidence of suicide risk, receiving l-carnosine in the last 3 weeks; history of allergy to l-carnosine or methylphenidate (Ritaline); presence of any medical problem; presence of uncontrolled seizures; systolic blood pressure more than 120 mm Hg; resting pulse rate <60/min or >115/min; receiving any supplement or medication for ADHD or other psychotropic medications; and current abuse or dependence on drugs within 6 months. It was declared to each patient and their guardian that they were free to withdraw from the trial without any negative effect on their treatment.
Randomization, allocation concealment, and blinding
Patients were randomly assigned to treatment groups in a 1:1 ratio using a computer-generated code. The assignments were kept in sealed, opaque, and stapled envelopes with an aluminum foil inside each envelope to make the content of the envelope unrecognizable in intense light until data analysis. l-carnosine and placebo were encapsulated and were identical. The person dispensing the drug, the patient, the physician who referred the patient, the rater, and the statistical analyzer were all blinded to allocation.
Intervention
Eligible subjects were randomly assigned to receive methylphenidate hydrochloride (MPH; Ritaline; 0.5–1.5 mg/kg) plus either l-carnosine (ACER) 800 mg/d or Placebo for an 8-week trial. Methylphenidate was titrated up during the trial according to the following schedule: 10 mg/d (two divided doses) for the first week followed by 20 mg/d (two divided doses) from the second week till the rest of the trial. Patients who weighed more than 30 kg received 30 mg/d (three divided doses) from the third week of the study. Medication adherence was measured by comparison of weekly tablet counts with participant reports of medication intake to estimate the proportion of dispensed medication that was actually ingested.
Outcome
The principal measure of outcome was the Teacher and Parent ADHD Rating Scale-IV (ADHD-RS-IV) (Dupaul et al. 1998; Pappas 2006) that has been used extensively in Iran in school-age children and provides valid measures of behavioral abnormality and attention (Akhondzadeh et al. 2004; Salardini et al. 2016). The primary outcome measure was change in scores of the parent version of ADHD-RS-IV from baseline to week 8 in each group. Secondary outcome measures were change in scores of the teacher version of ADHD-RS-IV and response rate in each group.
Safety
Side effects were systematically recorded throughout the study and were assessed using a checklist composed of 25 side effects, including psychological, neurologic, autonomic, and other side effects (Noorbala et al. 1999; Akhondzadeh et al. 2000; Modabbernia et al. 2012). There were no early dropouts due to early adverse events in this trial. Parents and children were asked to immediately inform the research team in case of any unexpected symptom or complaint during the study period.
Sample size
A minimal sample size of 50 (25 patients in each group) was calculated based on the assumption of a clinically significant difference of 4 on the Teacher and Parent ADHD-RS, a standard deviation of 5 on the Teacher and Parent ADHD-RS (according to the pilot study), a power of 90%, and a two-sided significance level of 0.05. Assuming a 10% attrition rate, a total sample size of 56 was estimated.
Statistical analyses
Statistical Package of Social Science Software (SPSS version 22; IBM Company) was used to carry out the statistical analysis. General linear model (GLM) repeated measure was used to compare Teacher and Parent ADHD-RS scores between treatment groups during the study course. A two-way repeated measures analysis of variance (time–treatment interaction) was used. The two groups were considered as a between-subject factor, and the three measurements during treatment were counted as within-subject factor. This was done for the Teacher and Parent ADHD-RS scores. A traditional “observed cases” (OC, the patients who completed the trial) analysis at 8 weeks was the primary efficacy analysis. In addition, intention to treat analysis with the last observation carried forward procedure was also performed. To estimate the effect size for the two outcome measures, we calculated the partial eta squared (η2) in the repeated measures GLM analysis.
Results
Baseline characteristics of the patients
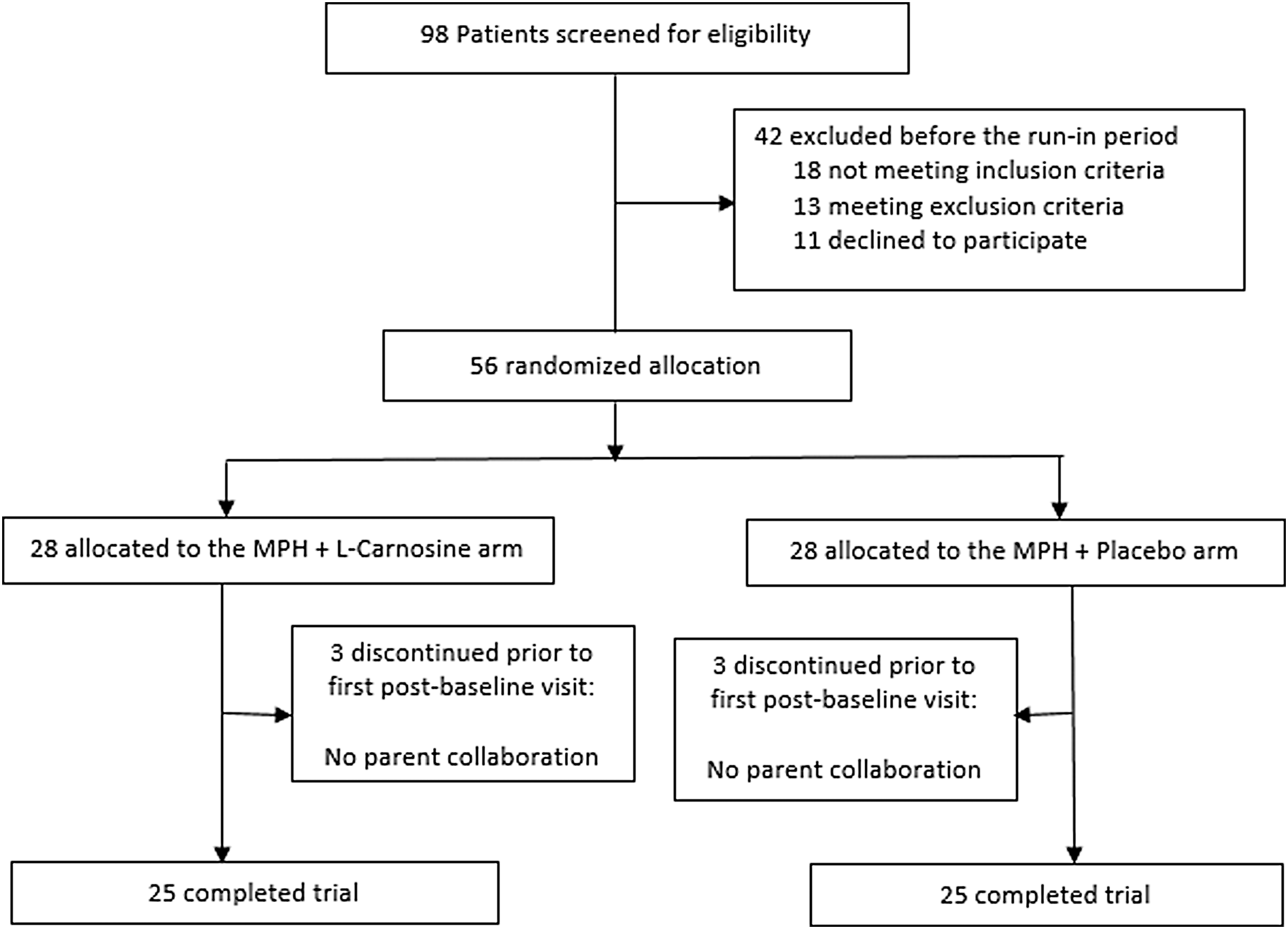
From a total of 98 children screened for the trial, 56 were randomly assigned to receive either l-carnosine (n = 28) or placebo (n = 28) in 2 trial arms. Fifty patients completed the study, and all had two postbaseline measurements. Three patients in the l-carnosine (withdrawn consent) and three patients in the placebo group (withdrawn consent) dropped out, all before week 4 (Fig. 1). However, all 6–17-year-old individuals were considered in the inclusion criteria; in the final population we had 6–13-year-old participants. As demonstrated in Table 1, baseline characteristics of the patients were not significantly different between the two trial arms (Table 1). There was no significant difference in terms of baseline total and subscales of Parent and Teacher ADHD-RS scores between the two treatment arms.
Flow diagram representing case selection for the trial program.
Baseline Characteristics of Patients According to Treatment Groups
Indicates the p-value reported by Fisher exact test.
ADHD, attention-deficit/hyperactivity disorder; MPH, methylphenidate hydrochloride; SD, standard deviation.
The Parent ADHD-RS
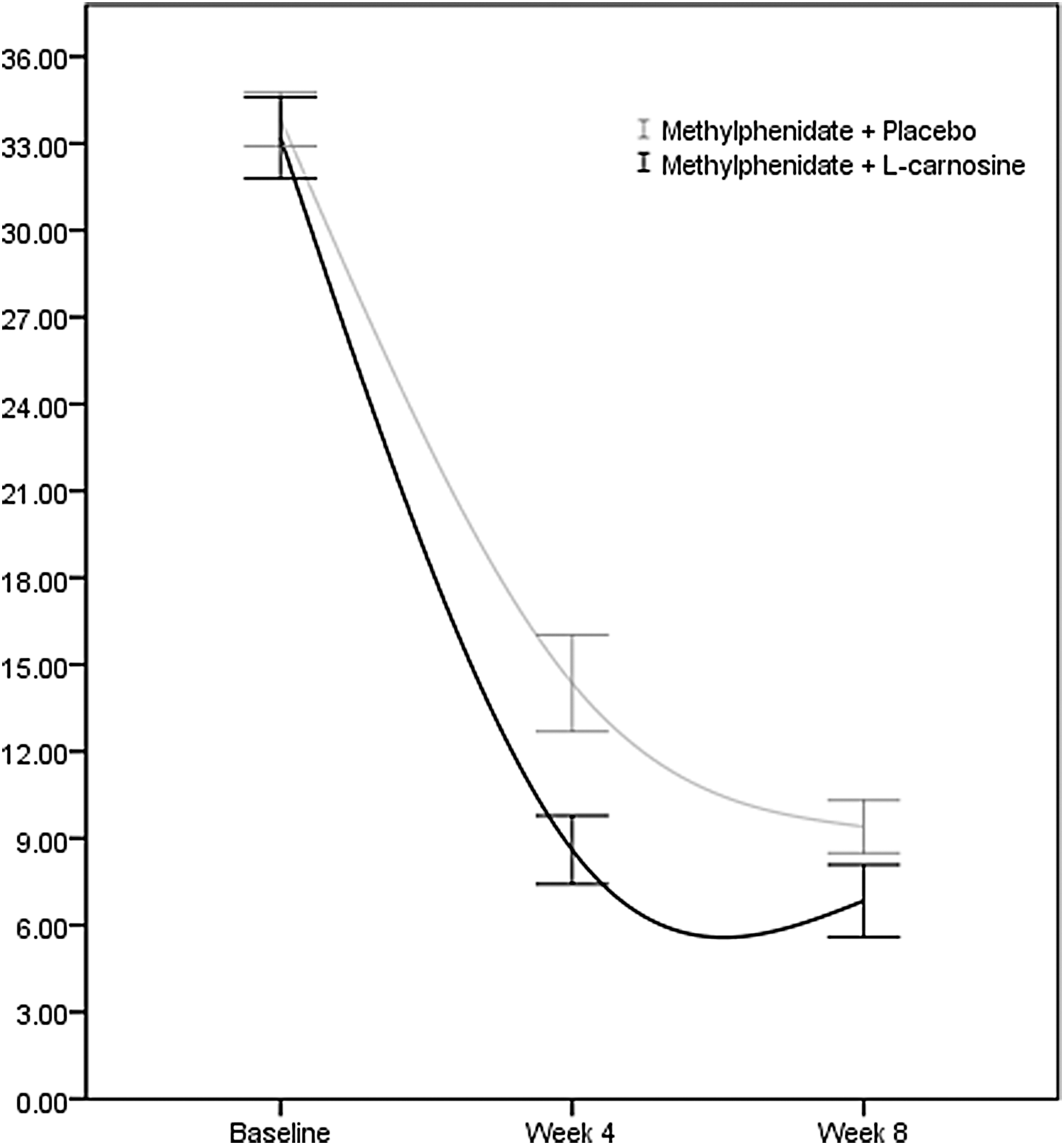
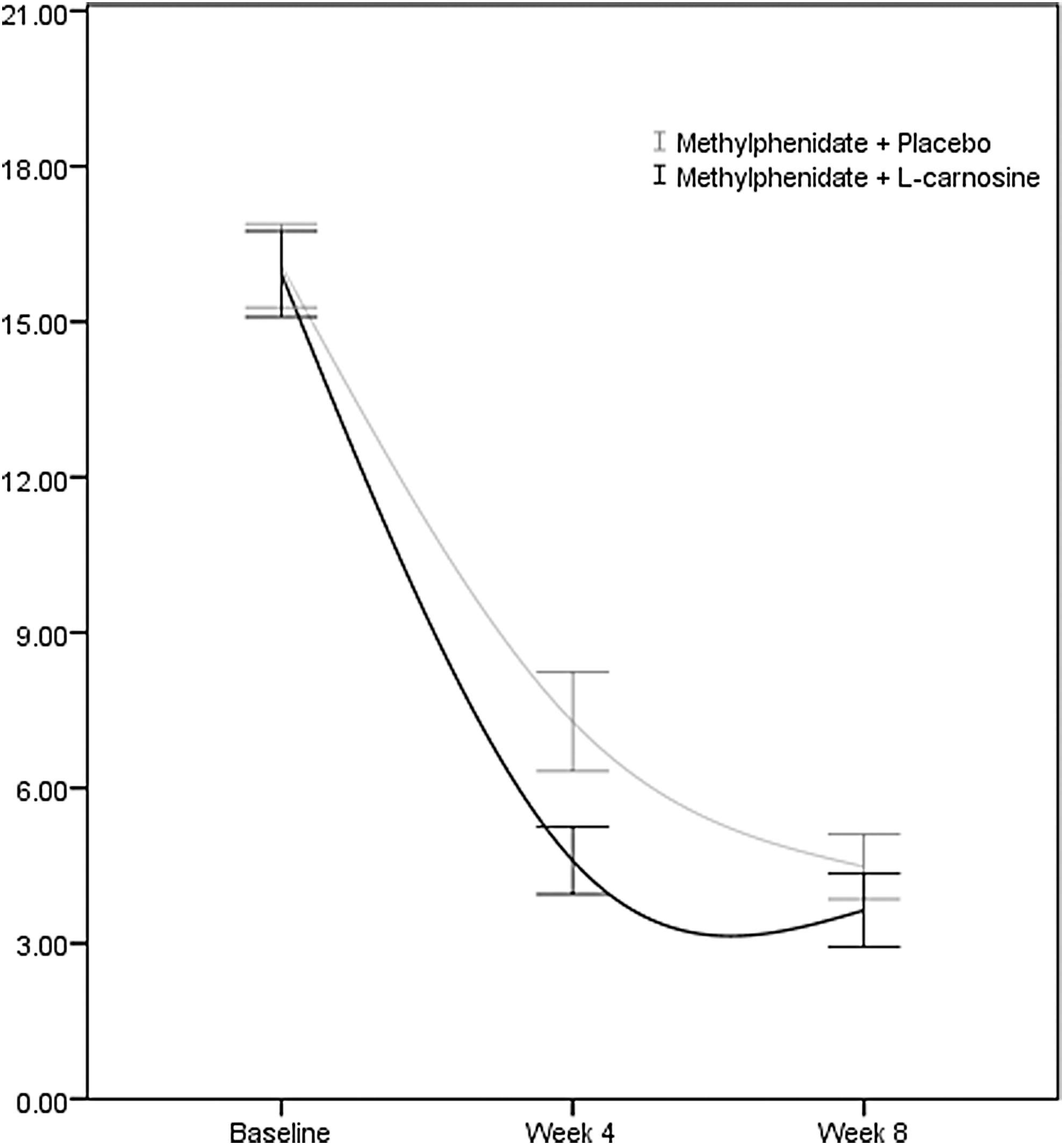
The GLM analysis of repeated measures revealed significant effects for time (Greenhouse-Geisser corrected: F = 430.638, df = 1.444, p < 0.001) and treatment (between-subject factor; Greenhouse-Geisser corrected: F = 4.556, df = 1, p = 0.038) interactions on the total Parent ADHD-RS scores. The effect of time × treatment interaction was also significant (Greenhouse-Geisser corrected: F = 3.783, df = 1.444, p = 0.041) over the trial period of 8 weeks, showing that the behavior of two treatment groups was different across time on the total Parent ADHD-RS scores (Fig. 2). Partial η2 of 0.073 was calculated for total Parent ADHD-RS score. Similarly, the two-factor repeated measure analysis of variance (ANOVA) demonstrated significant effects of time (Greenhouse-Geisser corrected: F = 391.135, df = 1.600, p < 0.001) and time × treatment interaction (Greenhouse-Geisser corrected: F = 4.032, df = 1.600, p = 0.030) for the inattention scale over the study period (Fig. 3). Partial η2 of 0.077 was calculated for inattention subscale scores. The results of the two-factor repeated measure ANOVA showed a significant effect of time on the changes in hyperactivity scale scores (Greenhouse-Geisser corrected: F = 297.707, df = 1.332, p < 0.001). However, the effect of time × treatment interaction term was not significant, showing that the behavior of both treatment groups was similar on the hyperactivity subscale across time (Greenhouse-Geisser corrected: F = 2.453, df = 1.332, p = 0.113).
Repeated measure for comparison of the effects of two treatment groups on Total Parent ADHD Rating Scale score. Values represent mean ± SEM. ADHD, attention-deficit/hyperactivity disorder; SEM, standard error of the mean.
Repeated measure for comparison of the effects of two treatment groups on Parent ADHD Inattention Rating Subscale scores. Values represent mean ± SEM.
The Teacher ADHD-RS
The GLM analysis of repeated measures revealed significant effects for time (Greenhouse-Geisser corrected: F = 14.994, df = 1.218, p < 0.001), but not for treatment (between-subject factor; Greenhouse-Geisser corrected: F = 0.240, df = 1, p = 0.626), or the time × treatment interaction term (Greenhouse-Geisser corrected: F = 0.200, df = 1.218, p = 0.705) over the trial period of 8 weeks for the total Teacher ADHD-RS score (Fig. 4). Similarly, repeated measure ANOVA demonstrated no significant effect for the time × treatment interaction term for inattention (Greenhouse-Geisser corrected: F = 0.012, df = 1.323, p = 0.956) and hyperactivity (Greenhouse-Geisser corrected: F = 1.231, df = 1.186, p = 0.281) scale scores.
Repeated measure for comparison of the effects of two treatment groups on Total Teacher ADHD Rating Scale scores. Values represent mean ± SEM.
Adverse events
Seven side effects were recorded during the course of the study (Table 2). No serious adverse event was observed in any of the patients. The most common side effects were abdominal pain (28%), headache (20%), and insomnia (16%) in the l-carnosine group and abdominal pain (24%) and headache (24%) in the placebo group. Frequency of side effects did not differ significantly between the two groups (Table 2).
The results of the present study support the short-term beneficial effects of l-carnosine as an adjuvant treatment in patients with ADHD. The results demonstrated improvements in the total score and the inattention subscale of the Parent ADHD-RS compared to placebo. However, the p-values reported in the GLM analysis were not robust (0.04 and 0.03). The effect size was calculated as partial η2 of 0.073 and 0.077 for total and inattention subscale scores, respectively. Improvements in the Teacher ADHD-RS were not significantly different between the two groups, most likely because of the overcrowded classrooms in developing countries like Iran, which resulted in teachers not being able to dedicate enough time to consider and follow each student's behavior. However, it is also plausible that no effect was identified from teachers because of little add-on benefits of l-carnosine. To the best of our knowledge, this is the first placebo-controlled survey of l-carnosine supplementation in patients with ADHD.
One of the possible mechanisms of the observed beneficial effects of l-carnosine on ADHD symptoms could be through its role as an NMDA receptor regulator. NMDA receptor modulators show satisfactory improvements in neuropsychological disorders such as depression and autism (Ghaleiha et al. 2013; Jafarinia et al. 2016; Hajizadeh-Zaker et al. 2017). Among hypotheses for ADHD, dysfunction of NMDA-type glutamate receptors has recently been suggested by accumulating genetic and animal studies (Lehohla et al. 2004; Elia et al. 2012; Pei-Chen Chang et al. 2014). The provided initial evidence suggests elevation of glutamate levels in the prefrontal cortex and anterior cingulate cortex (ACC) of patients with ADHD (Carrey et al. 2003; Kavirajan 2009), which may increase NMDA glutamate receptor activity with a positive correlation between this glutamatergic dysregulation and impulsivity and hyperactivity symptoms (Bauer et al. 2016). Carnosine inhibits glutamate release and protects against NMDA-induced neurotoxicity (Shen et al. 2007).
Memantine, an NMDA receptor antagonist, provides improvement in symptoms of both children and adults with ADHD (Findling et al. 2007; Surman et al. 2013; Biederman et al. 2017). Interestingly, Atomoxetine, an approved ADHD treatment that is supposed to bind to the presynaptic noradrenaline transporter (NET), is found to block NMDA receptors (Ludolph et al. 2010). In a 6-week clinical trial, Sarcosine, a glycine transporter-1 inhibitor (modulating the glutamatergic neurotransmission system through activating NMDA-type glutamate receptors) induced significant improvements in ODD symptoms of children with ADHD (Tzang et al. 2016).
Another possible explanation for the observed beneficial effects of l-carnosine could be its GABA-modulatory activity (Trombley et al. 1998). GABA and glutamate have critical roles in inhibitory and excitatory neurotransmission, respectively (Brennan and Arnsten 2008); and alterations in the interactions among glutamate, GABA, and dopamine neuronal circuits are likely to be involved in the pathophysiology of ADHD (Durrant and Heresco-Levy 2014). It is reported that GABA concentration was reduced in primary motor cortex of ADHD children (Edden et al. 2012) with correlations with impulsive and aggressive behavior (Silveri et al. 2013). Carnosine is a GABA modulating agent (Brondino et al. 2016), which increases the extracellular GABA level (Ouyang et al. 2016) possibly by modifying homocarnosine levels or by a direct chelating effect on zinc at GABA receptor sites (Ozonoff et al. 1991). Interestingly, there is no common idea regarding increase or decrease of Glx (combination of glutamate, glutamine, and GABA) in different areas of brain in patients with ADHD (Naaijen et al. 2015). Some studies showed decrease (Perlov et al. 2007; Dramsdahl et al. 2011). Some studies found increased Glx in striatal areas (Carrey et al. 2007; Hammerness et al. 2012), which seemed to decline after treatment with MPH (Carrey et al. 2002, 2003).
Another possible explanation for the observed beneficial effects of l-carnosine could be its antioxidant activity (Boldyrev et al. 2013). Inflammation is becoming a therapeutic target for neuropsychological disorders, including depression and ADHD (Lopresti 2015; Alamdarsaravi et al. 2017). ADHD is indicated to be associated with increased oxidative stress in a recent meta-analysis, although findings are inconsistent (Joseph et al. 2015; Lopresti 2015). Pinus marinus (French maritime pine bark) and zinc both have strong antioxidant activities and have support for treatment of ADHD in randomized, double-blind placebo-controlled studies (Akhondzadeh et al. 2004; Trebatická et al. 2006). l-Carnitine's antioxidant activity is mediated through different mechanisms, including reactive oxygen species and peroxyl radical scavenging and metal ion chelation (Boldyrev et al. 2013).
The present study was in line with previous reports regarding the role of anti-inflammatory agents and GABA-modulatory and NMDA receptor antagonists in treatment of ADHD, but the response was not satisfactory enough may be because a low dose of l-carnosine was used in this trial. In one of our recent unpublished trials, we treated chronic schizophrenia patients with a dose of 2 g/d of l-carnosine, and this yielded satisfying results and a good tolerability profile. Around medium effect sizes and not seeing significant effects in teacher scales indicated that decisive conclusion about the l-carnosine efficacy in individuals with ADHD needs further investigations.
Even though the present study has several strengths such as the double-blind placebo-controlled design and the rigorous adjustment for baseline clinical variables, various limitations should be addressed to prevent overgeneralization of the findings. First, the population size was relatively small. Second, the follow-up period was relatively short to make the accurate long-term effects of l-carnosine clear. The patient nutritional condition was not evaluated at admission although alteration of plasma amino acid levels might not correlate with nutritional status (Jackson and Garrod 1978). Finally, absence of functional and cognitive assessments (e.g., Clinical Global Impressions) and cognitive measurement of attention are other limitations of the present study. However, a consistent relationship between ADHD-RS-IV scores and Clinical Global Impression (CGI) levels was reported (Goodman et al. 2010). We conducted this trial on all newly diagnosed ADHD patients; however, including only the treatment-resistant patients might have led to more convincing outcomes through purifying the trial arms from children who are responders to common stimulant medications.
Conclusion
The results of this study must be considered preliminary. Eight weeks of treatment with l-carnosine (800 mg/d) as an add-on to methylphenidate appeared to be safe and well tolerated. Meaningful beneficial effects on the Parent ADHD-RS scores of patients with ADHD were indicated although no significant effect was detected on the Teacher ADHD-RS. Efficacy and tolerability of l-carnosine in higher doses and longer treatment periods, as well as in female-predominant populations, are still unclear and may be appropriate targets for further investigation.
Clinical Significance
To the best of our knowledge, there is lack of evidence on the efficacy of l-carnosine add-on to methylphenidate in patients with ADHD. Results from this trial indicate that l-carnosine can be considered as an effective adjuvant therapy in ADHD.
Footnotes
Disclosures
The authors declare no conflicts of interest.
Acknowledgments
This study was the postgraduate thesis of F.A.-N. toward the Iranian Board of Psychiatry under supervision of S.A. This study was supported by a grant from TUMS to S.A. (Grant No. 29573). The funding organization had no role in the design and conduct of the study; in the collection, analysis, and interpretation of the data; or in the preparation, review, or approval of the article and the decision to submit the article for publication.
References
1.
American Psychiatric Association.. Diagnostic and Statistical Manual of Mental Disorders, 5th ed., (DSM-5). Washington, D.C: American Psychiatric Association; 2013.
2.
AkhondzadehS, Ahmadi-AbhariSA, AssadiSM, ShabestariOL, KashaniAR, FarzanehganZM: Double-blind randomized controlled trial of baclofen vs. clonidine in the treatment of opiates withdrawal. J Clin Pharm Ther, 25:347–353, 2000.
3.
AkhondzadehS, MohammadiM-R, KhademiM: Zinc sulfate as an adjunct to methylphenidate for the treatment of attention deficit hyperactivity disorder in children: A double blind and randomized trial [ISRCTN64132371]. BMC Psychiatry, 4:9, 2004.
4.
AlamdarsaraviM, GhajarA, NoorbalaA-A, ArbabiM, EmamiA, ShaheiF, MirzaniaM, JafariniaM, AfaridehM, AkhondzadehS: Efficacy and safety of celecoxib monotherapy for mild to moderate depression in patients with colorectal cancer: A randomized double-blind, placebo controlled trial. Psychiatry Res, 255:59–65, 2017.
5.
BanaschewskiT, RoessnerV, DittmannRW, SantoshPJ, RothenbergerA: Non-stimulant medications in the treatment of ADHD. Eur Child Adolesc Psychiatry, 13:i102–i116, 2004.
6.
BauerJ, WernerA, KohlW, KugelH, ShushakovaA, PedersenA, OhrmannP: Hyperactivity and impulsivity in adult attention-deficit/hyperactivity disorder is related to glutamatergic dysfunction in the anterior cingulate cortex. World J Biol Psychiatry, 10:1–9, 2016.
7.
BiedermanJ, FriedR, TarkoL, SurmanC, SpencerT, PopeA, GrossmanR, McDermottK, WoodworthKY, FaraoneSV: Memantine in the treatment of executive function deficits in adults with ADHD: A pilot-randomized double-blind controlled clinical trial. J Atten Disord, 21:343–352, 2017.
8.
BoldyrevAA, AldiniG, DeraveW: Physiology and pathophysiology of carnosine. Physiol. Rev, 93:1803–1845, 2013.
9.
BrennanAR, ArnstenAF: Neuronal mechanisms underlying attention deficit hyperactivity disorder. Ann N Y Acad Sci, 1129:236–245, 2008.
10.
BrondinoN, Fusar-PoliL, PanisiC, DamianiS, BaraleF, PolitiP: Pharmacological modulation of gaba function in autism spectrum disorders: A systematic review of human studies. J Autism Dev Disord, 46:825–839, 2016.
11.
CarreyN, MacMasterFP, FogelJ, SparkesS, WaschbuschD, SullivanS, SchmidtM: Metabolite changes resulting from treatment in children with ADHD: A 1H-MRS study. Clin Neuropharmacol, 26:218–221, 2003.
12.
CarreyN, MacMasterFP, SparkesSJ, KhanSC, KusumakarV: Glutamatergic changes with treatment in attention deficit hyperactivity disorder: A preliminary case series. J Child Adolesc Psychopharmacol, 12:331–336, 2002.
13.
CarreyNJ, MacMasterFP, GaudetL, SchmidtMH: Striatal creatine and glutamate/glutamine in attention-deficit/hyperactivity disorder. J Child Adolesc Psychopharmacol, 17:11–17, 2007.
14.
ChanE, RappaportLA, KemperKJ: Complementary and alternative therapies in childhood attention and hyperactivity problems. J Dev Behav Pediatr, 24:4–8, 2003.
15.
ChezMG, BuchananCP, AimonovitchMC, BeckerM, SchaeferK, BlackC, KomenJ: Double-blind, placebo-controlled study of l-carnosine supplementation in children with autistic spectrum disorders. J. Child Neurol, 17:833–837, 2002.
16.
ChuhmaN, ChoiWY, MingoteS, RayportS: Dopamine neuron glutamate cotransmission: Frequency-dependent modulation in the mesoventromedial projection. Neuroscience, 164:1068–1083, 2009.
17.
CurtisLT, PatelK: Nutritional and environmental approaches to preventing and treating autism and attention deficit hyperactivity disorder (ADHD): A review. J Altern Complement Med, 14:79–85, 2008.
18.
DramsdahlM, ErslandL, PlessenKJ, HaavikJ, HugdahlK, SpechtK: Adults with attention-deficit/hyperactivity disorder—A brain magnetic resonance spectroscopy study. Front Psychiatry, 2:65, 2011.
19.
DupaulG, PowerT, AnastopoulosA, ReidR: ADHD Rating Scale-IV. New York, NY, Guilford, 1998.
20.
DurrantAR, Heresco-LevyU: The role of N-methyl-d-aspartate receptor-mediated neurotransmission in attention deficit (hyperactivity) disorder (ADHD/ADD). Curr Psychopharmacol, 3:184–194, 2014.
21.
EddenRA, CrocettiD, ZhuH, GilbertDL, MostofskySH: Reduced GABA concentration in attention-deficit/hyperactivity disorder. Arch Gen Psychiatry, 69:750–753, 2012.
22.
EliaJ, GlessnerJT, WangK, TakahashiN, ShtirCJ, HadleyD, et al.: Genome-wide copy number variation study associates metabotropic glutamate receptor gene networks with attention deficit hyperactivity disorder. Nat Genet, 44:78–84, 2012.
23.
FayyadJ, De GraafR, KesslerR, AlonsoJ, AngermeyerM, DemyttenaereK, De GirolamoG, HaroJM, KaramEG, LaraC, LépineJP, OrmelJ, Posada-VillaJ, ZaslavskyAM, JinR: Cross-national prevalence and correlates of adult attention-deficit hyperactivity disorder. Br J Psychiatry, 190:402–409, 2007.
24.
FindlingRL, McNamaraNK, StansbreyRJ, MaxhimerR, PericlouA, MannA, et al.: A pilot evaluation of the safety, tolerability, pharmacokinetics, and effectiveness of memantine in pediatric patients with attention-deficit/hyperactivity disorder combined type. J Child Adolesc Psychopharmacol, 17:19–33, 2007.
25.
GhajarA, NeishabouriS, VelayatiN, JahangardL, MatinniaN, HaghighiM, GhaleihaA, AfaridehM, SalimiS, MeysamieA, AkhondzadehS: Crocus sativus L: versus citalopram in the treatment of major depressive disorder with anxious distress: A double-blind, controlled clinical trial. Pharmacopsychiatry, 50:152–160, 2016.
26.
GhaleihaA, AsadabadiM, MohammadiM-R, ShaheiM, TabriziM, HajiaghaeeR, HassanzadehE, AkhondzadehS: Memantine as adjunctive treatment to risperidone in children with autistic disorder: A randomized, double-blind, placebo-controlled trial. Int J Neuropsychopharmacol, 16:783–789, 2013.
27.
GhanizadehA, MohammadiMR, YazdanshenasA: Psychometric properties of the Farsi translation of the kiddie schedule for affective disorders and schizophrenia-present and lifetime version. BMC Psychiatry, 6:10, 2006.
28.
GoodmanD, FaraoneSV, AdlerLA, DirksB, HamdaniM, WeislerR: Interpreting ADHD rating scale scores: Linking ADHD rating scale scores and CGI levels in two randomized controlled trials of lisdexamfetamine dimesylate in ADHD. Prim Psychiatry, 17:44, 2010.
29.
GreenhillLL, FindlingRL, SwansonJM: A double-blind, placebo-controlled study of modified-release methylphenidate in children with attention-deficit/hyperactivity disorder. Pediatrics, 109:e39, 2002.
30.
Hajizadeh-ZakerR, GhajarA, MesgarpourB, AfaridehM, MohammadiMR, AkhondzadehS: l-Carnosine as an adjunctive therapy to risperidone in children with autistic disorder: A randomized, double-blind, placebo-controlled trial. J Child Adolesc Psychopharmacol, 28:74–81, 2018.
31.
HammernessP, BiedermanJ, PettyC, HeninA, MooreCM: Brain biochemical effects of methylphenidate treatment using proton magnetic spectroscopy in youth with attention‐deficit hyperactivity disorder: A controlled pilot study. CNS Neurosci Ther, 18:34–40, 2012.
32.
JacksonMJ, GarrodPJ. Plasma zinc, copper, and amino acid levels in the blood of autistic children. J Autism Child Schizophr, 8:203–208, 1978.
33.
JafariniaM, AfaridehM, TafakhoriA, ArbabiM, GhajarA, NoorbalaAA, SaraviMA, AgahE, AkhondzadehS: Efficacy and safety of oral ketamine versus diclofenac to alleviate mild to moderate depression in chronic pain patients: A double-blind, randomized, controlled trial. J Affect Disord, 204:1–8, 2016.
34.
JosephN, Zhang-JamesY, PerlA, FaraoneSV: Oxidative stress and ADHD: A meta-analysis. J Atten Disord, 19:915–924, 2015.
35.
KavirajanH: Memantine: A comprehensive review of safety and efficacy. Expert Opin Drug Saf, 8:89–109, 2009.
36.
KotechaSA, OakJN, JacksonMF, PerezY, OrserBA, Van TolHH, MacDonaldJF: A D2 class dopamine receptor transactivates a receptor tyrosine kinase to inhibit NMDA receptor transmission. Neuron, 35:1111–1122, 2002.
37.
LehohlaM, KellawayL, RussellVA: NMDA receptor function in the prefrontal cortex of a rat model for attention-deficit hyperactivity disorder. Metab Brain Dis, 19:35–42, 2004.
38.
LoprestiAL: Oxidative and nitrosative stress in ADHD: Possible causes and the potential of antioxidant-targeted therapies. Atten Defic Hyperact Disord, 7:237–247, 2015.
39.
LudolphAG, UdvardiPT, SchazU, HenesC, AdolphO, WeigtHU, FegertJM, BoeckersTM, FöhrKJ: Atomoxetine acts as an NMDA receptor blocker in clinically relevant concentrations. Br J Pharmacol, 160:283–291, 2010.
40.
MillichapJG: Etiologic classification of attention-deficit/hyperactivity disorder. Pediatrics, 121:e358–e365, 2008.
41.
ModabberniaA, SohrabiH, NasehiAA, RaisiF, SaroukhaniS, JamshidiA, TabriziM, AshrafiM, AkhondzadehS: Effect of saffron on fluoxetine-induced sexual impairment in men: Randomized double-blind placebo-controlled trial. Psychopharmacology (Berl), 223:381–388, 2012.
42.
NaaijenJ, LythgoeDJ, AmiriH, BuitelaarJK, GlennonJC: Fronto-striatal glutamatergic compounds in compulsive and impulsive syndromes: A review of magnetic resonance spectroscopy studies. Neurosci Biobehav Rev, 52:74–88, 2015.
43.
NoorbalaAA, AkhondzadehS, Davari-AshtianiR, Amini-NooshabadiH: Piracetam in the treatment of schizophrenia: Implications for the glutamate hypothesis of schizophrenia. J Clin Pharm Ther, 24:369–374, 1999.
44.
OuyangL, TianY, BaoY, XuH, ChengJ, Wang ShenY, ChenZ, LyuJ: Carnosine decreased neuronal cell death through targeting glutamate system and astrocyte mitochondrial bioenergetics in cultured neuron/astrocyte exposed to OGD/recovery. Brain Res Bull, 124:76–84, 2016.
45.
OzonoffS, PenningtonBF, RogersSJ: Executive function deficits in high‐functioning autistic individuals: Relationship to theory of mind. J Child Psychol Psychiatry, 32:1081–1105, 1991.
PittengerC, BlochMH, WilliamsK: Glutamate abnormalities in obsessive compulsive disorder: Neurobiology, pathophysiology, and treatment. Pharmacol Ther, 132:314–332, 2011.
50.
PliszkaSR: The neuropsychopharmacology of attention-deficit/hyperactivity disorder. Biol Psychiatry, 57:1385–1390, 2005.
51.
ProkopievaV, YaryginaE, BokhanN, IvanovaS: Use of carnosine for oxidative stress reduction in different pathologies. Oxid Med Cell Longev, 2016:2939087, 2016.
52.
SalardiniE, ZeinoddiniA, KohiA, MohammadiM-R, MohammadinejadP, KhiabanyM, ShahriariM, AkhondzadehS: Agomelatine as a treatment for attention-deficit/hyperactivity disorder in children and adolescents: A double-blind, randomized clinical trial. J Child Adolesc Psychopharmacol, 26:513–519, 2016.
53.
SarrisJ, KeanJ, SchweitzerI, LakeJ: Complementary medicines (herbal and nutritional products) in the treatment of attention deficit hyperactivity disorder (ADHD): A systematic review of the evidence. Complement Ther Med, 19:216–227, 2011.
54.
Sassoè-PognettoM, CantinoD, PanzanelliP, di CantognoLV, GiustettoM, MargolisFL, De BiasiS, FasoloA: Presynaptic colocalization of carnosine and glutamate in olfactory neurones. Neuroreport, 5:7–10, 1993.
55.
ShenY, HeP, FanY-Y, ZhangJ-X, YanH-J, HuW-W, OhtsuH, ChenZ: Carnosine protects against permanent cerebral ischemia in histidine decarboxylase knockout mice by reducing glutamate excitotoxicity. Free Radic Biol Med, 48:727–735, 2010.
56.
ShenY, HuW-W, FanY-Y, DaiH-B, FuQ-L, WeiE-Q, LuoJH, ChenZ: Carnosine protects against NMDA-induced neurotoxicity in differentiated rat PC12 cells through carnosine-histidine-histamine pathway and H 1/H 3 receptors. Biochem Pharmacol, 73:709–717, 2007.
57.
SilveriMM, SneiderJT, CrowleyDJ, CovellMJ, AcharyaD, RossoIM, JensenJE: Frontal lobe γ-aminobutyric acid levels during adolescence: Associations with impulsivity and response inhibition. Biol Psychiatry, 74:296–304, 2013.
58.
SteeleM, JensenPS, QuinnDM: Remission versus response as the goal of therapy in ADHD: A new standard for the field?. Clin Ther, 28:1892–1908, 2006.
59.
SurmanCB, HammernessPG, PettyC, SpencerT, DoyleR, NapoleanS, ChuN, YorksD, BiedermanJ: A pilot open label prospective study of memantine monotherapy in adults with ADHD. World J Biol Psychiatry, 14:291–298, 2013.
TrebatickáJ, KopasováS, HradečnáZ, ČinovskýK, ŠkodáčekI, ŠubaJ, MuchováJ, ZitnanováI, WaczulíkováI, RohdewaldP, DurackováZ: Treatment of ADHD with French maritime pine bark extract, Pycnogenol®. Eur Child Adolesc Psychiatry, 15:329–335, 2006.
62.
TrombleyPQ, HorningMS, BlakemoreLJ: Carnosine modulates zinc and copper effects on amino acid receptors and synaptic transmission. Neuroreport, 9:3503–3507, 1998.
63.
TuricD, LangleyK, MillsS, StephensM, LawsonD, GovanC, WilliamsN, Van Den BreeM, CraddockN, KentL, OwenM, O'DonovanM, ThaparA: Follow-up of genetic linkage findings on chromosome 16p13: Evidence of association of N-methyl-d aspartate glutamate receptor 2A gene polymorphism with ADHD. Mol Psychiatry, 9:169–173, 2004.