
Abstract
Objectives:
Osteoporosis is a major risk factor for fracture and treatment is mainly preventive. Patients with severe psychiatric condition and treated with antipsychotics are at risk for vitamin D deficiency and iatrogenic hyperprolactinemia, two serious risk factors of osteoporosis. We aim to determine whether all antipsychotics are similar regarding the risk of osteoporosis in young patients.
Methods:
From January 2009 to March 2015, we determined the vitamin D blood level (VDBL) among 484 inpatients and from January 2012 to March 2015, we determined the prolactin blood level (PBL) among 205 inpatients. We systematically recorded well-documented risk factors (e.g., age, gender, ethnic origin, body mass index, or season) and suspected risk factors (e.g., disease type or antipsychotic treatment).
Results:
Up to 89% of the inpatients had a VDBL under the recommended threshold. Up to 60% of the inpatients had hyperprolactinemia. The multivariate model found a significant effect on VDBL for seasonality (higher VDBL in summer), ethnicity (lower VDBL in Black individuals), and treatment exposure. The multivariate model found a significant effect on PBL for gender and treatment exposure. In both models, aripiprazole had a safer profile compared with other antipsychotics.
Conclusion:
Because adolescence is a period of bone construction and a critical window of opportunity for maximizing bone mass, we recommend vitamin D supplementation in young patients with severe mental condition. It could be interesting to reconsider to regularly monitor PBL among youth patients treated with antipsychotic, with the exception of aripiprazole.
Introduction
A
Although the World Health Organization has not already listed antipsychotic medications among risk factors for osteoporosis (Crews and Howes 2012), it is legitimate to wonder whether young patients exposed to SGAs would be at a greater risk. Osteoporosis is a major risk factor for fracture and elderly morbidity. Most treatment possibilities are preventive. Few works exist on the link between osteoporosis and antipsychotic medications (Kishimoto et al. 2012; Wu et al. 2013; Wang et al. 2014). Antipsychotic medications block dopamine receptors, reducing the prolactin's inhibition level leading to iatrogenic hyperprolactinemia through the hypothalamic–pituitary–gonadal axis (Haddad and Wieck 2004). Hyperprolactinemia is associated with lower bone mineral density (BMD). Two mechanisms seem to be involved in this association. The first is reduction of gonadal hormones, estradiol, and testosterone. Lower sex hormone levels are associated with lower BMD and reduction of osteoclast activity. The second mechanism appears to be by direct effects on bone metabolism (Goffin et al. 2002; Seeman and Estrogen 2004; Kaufman 2006).
The relationship between higher osteoporosis rate among patients compared with controls and use of antipsychotics medication is complex to investigate (Kishimoto et al. 2012). It appears that factors other than hyperprolactinemia contribute to the reduction of BMD: low physical activity, smoking addiction, low calcium intake, low vitamin D blood level (VDBL), dark skin, family history, gender, prior fracture, and the use of specific medications (corticosteroids, anticoagulants, thyroid hormones, and methotrexate). In addition to VDBL >30 ng/mL, which is crucial to protect against osteoporosis (Dawson-Hughes et al. 2005), other hormonal factors may also interfere (hypogonadism, hyperthyroidism, hyperparathyroidism, and hypercorticism (Burge 2000; Kishimoto et al. 2012).
Regarding vitamin D deficiency, young psychiatric patients seem to be a particularly vulnerable population (Crews et al. 2013). Indeed results from several studies have suggested that vitamin D has positive effects on bone growth during adolescence (Välimäki et al. 2004; Högström et al. 2006). Therefore exposing young psychiatric patients to SGA iatrogenic hyperprolactinemia may induce a cumulative risk of osteoporosis. It appears that the balance Vitamin D/prolactin should be investigated as a biological risk marker of osteoporosis in this particular population.
The aim of the current cross-sectional study was (1) to enlarge the recruitment of a previous study on VDBL in child and adolescent patients with severe psychiatric conditions (Bonnot et al. 2011); (2) to investigate medication risk factor for hyperprolactinemia and hypovitaminosis D among youth inpatients with severe mental illness; (3) to take into account other risk factors of osteoporosis, such as diagnosis, gender, body mass index (BMI), ethnicity, and seasonality (sun exposure).
Methods
Participants
Inclusion criteria were patients admitted in the Child and Adolescent Psychiatric Department of La Pitié- Salpêtrière University Hospital from January 1, 2009 to March 2015 for VDBL assessment and from January 2012 to March 2015 for prolactin blood level (PBL). Exclusion criteria were eating disorders, as defined in the International Classification of Disease, 10th Revision (
We previously published a study with a subset of the participants regarding VDBL assessment (Bonnot et al. 2011). In this first study, we determined the VDBL of all consecutive inpatients in 2009 (N = 136) to evaluate whether adolescent psychiatric inpatient VDBL is lower than the 30 ng/mL optimal threshold and to document low-VDBL risk factors. PBL was not assessed in the previous study. We decided to enlarge the sample, and regarding VDBL assessment, 348 patients were added to the sample in the work presented here. PBL assessment was recorded for 205 patients in the work presented here. Diagram flow (Fig. 1) summarizes the VDBL and PBL procedures in the 502 patients.

Diagram flow summarizes the VDBL and PBL procedures in the 502 patients. PBL, prolactin blood level; VDBL, vitamin D blood level.
Our university Ethics Committee approved the study that first focused on VDBL. We added assessment of PBL during the last 3 years of the study.
Variables
We prospectively recorded patients' sociodemographic data, skin color (Caucasian, North African, or black) (Cavalli-Sforza et al. 1994), treatments, BMI, blood results, and date of sample collection. Type of disease was assessed according to International Classification of Disease, 10th Revision. We divided participants' disorders into four categories: (1) psychotic disorders, including schizophrenia, schizoaffective disorders, unspecified psychosis not due to a substance or known physiological condition, and “organic psychotic disorders” (ICD10 codes: F20–F29); (2) developmental conditions, including pervasive developmental disorders, intellectual disabilities, and other developmental neuropsychiatric conditions (F70–F89); (3) behavioral impairments, including borderline personality disorder, conduct disorder, agitation/oppositional behaviors, attention-deficit/hyperactivity disorder (ADHD) and anxiety disorders (F90–F98 and F40–F41); and (4) mood disorders (F30–F39).
We recorded for each patient the type of psychotropic treatment: antipsychotic (AP), antidepressant, benzodiazepines, mood stabilizers, and stimulants. Regarding AP, we recorded type of AP, duration of treatment in months. Given the frequency of polyprescription of APs, we defined “main treatment” as the regular daily treatment one patient received, as opposed to adjuvant symptomatic AP treatment defined by a duration (<15 days) and/or the titration (based on chlorpromazine equivalent) to be negligible regarding the main AP treatment. This included punctual treatment in case of agitation as a few weeks of adjuvant treatment regarding years of main treatment. Otherwise, we considered association of APs as “combination of APs.”
All VDBL and PBL measurements were performed in the same laboratory, using electrochemiluminescent immunoassay. For VDBL we used the Liaison DiaSorin, Stillwater, MN. This assay measures serum 25(OH)D2 and 25(OH)D3 equally well. Intra- and interassay coefficients of variation were <8% and <13%, respectively. We retained 30 ng/mL as the recommended threshold for VDBL. For PBL, we used the Modular E, Roch®. The threshold to definite hyperprolactinemia among boys and girls under 15 years of age is 15 and 20 ng/mL for girls over 15 years of age (Peveler et al. 2008).
Data analysis
We chose to compare patients under aripiprazole, risperidone, and cyamemazine because these three APs are the most commonly used treatment in the department. Aripiprazole and risperidone are commonly used worldwide according to pharmacoepidemiological studies (Governale and Mehta 2010). We added cyamemazine in the analyses as it is the second most commonly used AP in our department. This is in line with recent French pharmacoepidemiological studies (Bonnot et al. 2017; Khouri et al. 2017). We also included in the analysis a group of patients free from AP treatment.
The statistical analysis was carried out using the R software version 3.0.2. For each dependent variable (VDBL and PBL) a total of ten hypotheses were tested. We decided to use a Bonferroni correction by dividing the common level of significance of 5% by 10. Hence the level of significance for each test was set at 0.5%, and all tests were two tailed. In a first step, a descriptive analysis was run. Mean and standard deviation (SD) were used to describe quantitative variables, while frequencies were used for qualitative factors. In a second step, a bivariate analysis was conducted to test for the associations between pairs of variables. Association between quantitative variables was tested using Pearson's correlation, whereas Student's t-test was used for group comparisons (or Mann–Whitney test in case of non-normality—assessed graphically with a histogram). Fisher's exact test was computed to test the association between qualitative factors. Finally, we performed multivariate analyses. Significant variables from the bivariate analysis were entered as predictors in a regression model, with VDBL and PBL as dependent variables.
Results
Between January 2009 and March 2015, from the 986 eligible patients for VDBL assessment and from the 506 eligible patients for the PBL, half did not participate in the study. Nonparticipation was based on puncture rejection, adolescent oppositional behaviors, parents' refusal, family conflict, and children or adolescents admitted for a brief duration (<15 days). In total, 502 patients were enrolled in the study. VDBL was recorded for 484 patients, and PBL was recorded for 205 patients: 187 patients had both measures.
The sample included 165 (33%) females and 337 (67%) males, 13.69 years of age on average (SD = 2.65, median = 13.86). Fifty-one percent of the patients (N = 239) received AP treatment: 113 patients (24%) received risperidone as main treatment, 51 patients (11%) received cyamemazine as main treatment, 40 (8%) received aripiprazole as main treatment, and 35 patients (7%) received other APs or combination of APs (haloperidol n = 8 [2%], olanzapine n = 10 [2%], other, or combination of APs n = 17 [4%]). Data on type of main treatment were missing for 29 patients. Other nonantipsychotic treatments included antidepressants n = 85 (17%), mood stabilizers n = 48 (9.5%), benzodiazepines n = 37 (7%), or stimulants n = 27 (5%). None of the patients had undergone vitamin D treatment before the first measure of VDBL. Fifteen patients (3%) had a history of bone fractures. Regarding clinical diagnoses 297 patients (59%) showed behavioral impairments, 122 patients (24%) had mood disorders, 115 patients (23%) had a developmental condition, and 68 patients (13.5%) had psychotic disorders. Diagnoses were not exclusive. The mean BMI was 20.75 (SD = 4.63, median = 19.92). Mean duration of AP treatment was 16 months (SD = 20.39, median = 8).
Vitamin D blood levels
The subsample included 484 patients with 153 (32%) females and 331 (68%) males 13.63 (SD = 2.63, median = 13.80) years of age on average (Tables 1 and 2). Fifty percent of the patients (N = 230) received AP treatment, 110 patients (24%) received risperidone as main treatment, 51 patients (11%) received cyamemazine as main treatment, 36 (8%) received aripiprazole as main treatment, and 33 patients (7%) received other APs or combination of APs (haloperidol n = 8 [2%], olanzapine n = 10 [2%], other or combination of APs n = 15 [3%]). Data on the type of main treatment were missing for 26 patients. Other nonantipsychotic treatments included antidepressants n = 81 (17%), mood stabilizers n = 40 (8%), benzodiazepines n = 37(7%), or stimulants n = 27(5.5%). Fifteen patients (3%) had a history of bone fractures. Regarding clinical diagnoses, 288 patients (60%) showed behavioral impairments, 117 patients (24%) had mood disorders, 114 patients (24%) had a developmental condition, and 64 patients (13%) had psychotic disorders. Diagnoses were not exclusive. The mean BMI was 20.69 (SD = 4.63, median = 19.84). Mean duration of AP treatment was 16 months (SD = 20.68, median = 8).
Serum 25-OH-Vitamin D Levels in Young Psychiatric Inpatients (n = 484) According to Sex, Ethnicity and Disease Category
Significant values are in bold. The level of significance for each test was set at 0.5%.
SD, standard deviation
Regression Analysis Regarding Serum 25-OH-Vitamin D Levels in Young Psychiatric Inpatients (Df = 133, F = 6.43)
Significant values are in bold. The level of significance for each test was set at 0.5%.
SE, standard error.
Table 1 summarizes VDBL levels according to gender, ethnicity, period of the year, and disease category, respectively. VDBL was remarkably low with a mean level at 17.81 ng/mL (SD = 9.55, median = 17.50), under the recommended threshold of 30 ng/mL. Only 51 (11%) among the 484 enrolled patients had a VDBL >30 ng/mL. VDBL was not associated with gender (t = 1.3, p = 0.2007). We confirmed the association with ethnicity (lower VDBL in Black individuals, t = 5.4, p ≤ 0.001) and seasonal effect (higher VDBL with sun exposure). We confirmed a significant difference of VDBL according to the progression of the year with significant differences between the four periods of the year, except between the two first ones (winter compared with spring, trimester 1 vs. trimester 2, p = 0.015), trimester 2 compared with trimester 4 (spring compared with fall, p = 0.042) and the last two periods (summer compared with fall, trimester 3 vs. trimester 4, p = 0.206). We found highest rates during summer time and lower rate during winter time according to the sun exposure. Disease category (Psychotic disorders t = 0.7, p = 0.4911, Behavioral impairments t = −0.7, p = 0.4761, Developmental conditions t = −0.2, p = 0.8738, Mood disorders t = −2.3, p = 0.0198), BMI (Pearson's r = −0.12, p = 0.018), age (Pearson's r = 0, p = 0.93), and duration of treatment (Pearson's r = 0.13, p = 0.048) were not correlated with VDBL.
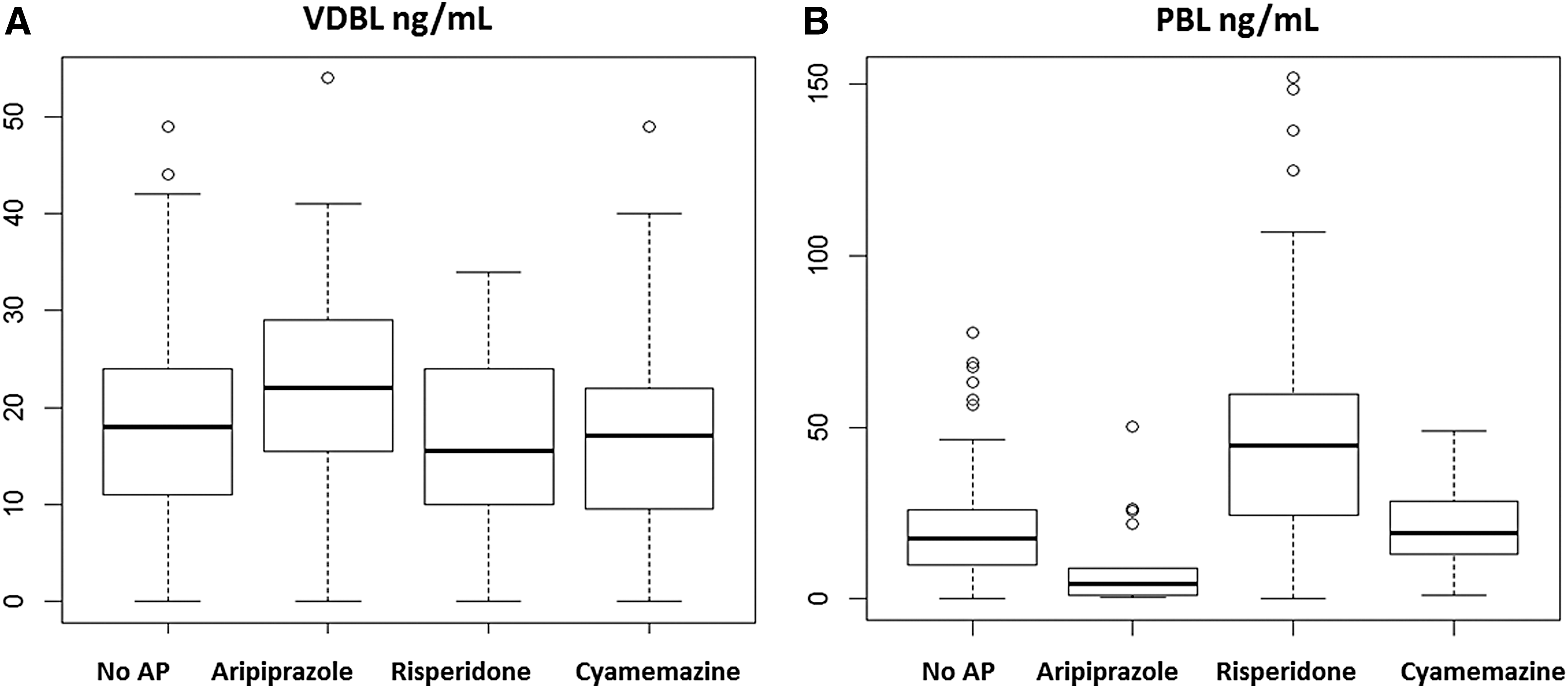
We found no difference between patients treated by AP and without treatment (t = 0.3, p = 0.7944). We found no significant differences regarding treatment type, but a tendency. To avoid the effect of polyprescriptions, we compared only four groups of patients with main treatment prescription: those treated with aripiprazole (n = 36), those treated with risperidone (n = 110), those treated with cyamemazine (n = 51), and those who received no antipsychotic treatment (n = 228). No significant differences between treatment were found regarding VDBL (Fig. 2A; analysis of variance [ANOVA], df = 3, F = 2.434, p = 0.0644). However, there were significantly more patients above the recommended threshold among patients under aripiprazole only compared with patients treated with risperidone or patients without AP treatment (Fisher exact test, p = 0.003).
VDBL
A multivariate regression was carried out to predict the rate of VDBL based on the significant variables found in the bivariate analysis (Table 2). The effects of seasonality (β = 9.4, standard error [SE] = 2.14, p < 0.001 for trimester 3 vs. 1; β = 5.5, SE = 1.85, p = 0.004 for trimester 4 vs. 1) and ethnicity (β = −5.97, SE = 1.74, p < 0.001) remained significant, although the comparison between trimester 3 and trimester 2 did not remain significant: (β = 4.6, SE = 2.14, p = 0.029). The multivariate analysis showed that the effect of treatment remained significant with a lower rate of VDBL among patients treated with risperidone compared with aripiprazole (β = −6.6, SE = 1.95, p < 0.001), and a lower rate of VDBL among patients treated with cyamemazine compared with patients treated with aripiprazole (β = −6.59, SE = 2.15, p < 0.001). There was no difference between risperidone and cyamemazine (β = −0.011, SE = 1.66, p = 0.995) (Fig. 2A).
Prolactin blood levels
The subsample included 205 patients with 63 (31%) females and 142 (69%) males 14.17 (SD = 2.55, median = 2.56) years of age on average (Tables 3 and 4). Fifty-two percent of the patients (N = 113) received AP treatment, 54 patients (28%) received risperidone as main treatment, 20 patients (10%) received cyamemazine as main treatment, 18 (9%) received aripiprazole as main treatment, and 21 patients (11%) received other APs or combination of APs (haloperidol n = 6 [3%], olanzapine n = 3 [2%], other or combination of APs n = 12 [6%]). Data on the type of main treatment was missing for 10 patients. Other nonantipsychotic treatments included antidepressants n = 42 (20%), mood stabilizers n = 31 (15%), benzodiazepines n = 21 (10%), or stimulants n = 13 (6%). Ten (5%) had a history of bone fractures. Regarding clinical diagnoses 124 patients (60%) showed behavioral impairments, 67 patients (33%) had mood disorders, 45 patients (22%) had a developmental condition and 29 patients (14%) had psychotic disorders. Diagnoses were not exclusive. The mean BMI was 20.85 (SD = 4.29, median = 20.15). Mean duration of AP treatment was 13.5 months regarding PBL (SD = 21.16, median = 6).
Prolactin Level in Young Psychiatric Inpatients (n = 205) According to Sex, Ethnicity, and Disease Category
Significant values are in bold. The level of significance for each test was set at 0.5%.
Regression Analysis Regarding Prolactin Levels in Young Psychiatric Inpatients (Df = 79, F = 13.03)
Significant values are in bold. The level of significance for each test was set at 0.5%.
Table 3 summarizes PBL levels according to gender, ethnicity, and disease category, respectively. We found hyperprolactinemia among 121 (60%) of the 205 patients enrolled. As expected, we found a significant association with gender with a higher rate of PBL among females (t = 3.5, p < 0.001). We found a significant association with diagnoses with a higher rate of PBL among patients suffering from psychotic disorders (t = −3.1, p = 0.0046) (Table 3). Age was positively correlated with PBL (Pearson's r = 0.26, p < 0.001). BMI and treatment duration were not correlated with PBL (Pearson's r = 0.05, p = 0.57; Pearson's r = 0.05, p = 0.63, respectively).
Regarding treatment, AP influenced PBL, with a higher rate among patients treated with AP compared with patients free from AP (Fig. 2B, ANOVA, df = 3, F = 19.5, p < 0.001). In details, PBL was significantly higher among patients treated with risperidone compared with patients treated with aripiprazole (post hoc Tukey, p < 0.001), compared with patients treated with cyamemazine (post hoc Tukey, p < 0.001), and compared with patients free from AP (post hoc Tukey, p < 0.001). Also, there were significantly more patients with hyperprolactinemia among patients treated with risperidone compared with patients treated with aripiprazole, cyamemazine, or patients without AP (Fisher exact test, p = 0.005).
A multivariate regression was carried out to predict the rate of PBL, based on the significant variables found in the bivariate analysis (Table 4). The effect of diagnosis did not remain significant for psychotic disorders (β = 10.63, SE = 8.14, p = 0.196). The effects of gender remained significant (β = 33.87, SE = 6.65, p < 0.001) with higher PBL rates in females. Regarding treatment differences, risperidone and cyamemazine were significantly associated with higher rate of PBL compared with aripiprazole (β = 52.38, SE = 7.93, p < 0.001; β = 22.58, SE = 8.73, p < 0.001, respectively). Risperidone was significantly associated with higher PBL compared with cyamemazine (β = 29.8, SE = 6.66, p < 0.001).
Discussion
The three main findings of this study are: (1) up to 89% (n = 433) of the inpatients had a VDBL under the recommended threshold. (2) Up to 60% (n = 121) of the inpatients had hyperprolactinemia. (3) Aripiprazole has a safer profile compared with other APs regarding both hormonal risk factors for osteoporosis confirming that all SGAs do not have the same AE profiles (Cohen et al. 2012).
Regarding VDBL deficiency, our results confirm previous analyses in a subset of these data (N = 136) (Bonnot et al. 2011). Age, gender, BMI, duration of treatment, and disease category were not associated with vitamin D risk factors in this sample. Ethnicity and low sun exposure remained risk factors for vitamin D deficiency, and there is no difference between patients taking AP and patients free from treatment as found previously (Cavalli-sforza et al. 1994). In our previous study on a subset of these data (Bonnot et al. 2011), we failed to find an association between AP medication and VDBL. In the current sample, large enough with 484 patients enrolled, we found a significant association with treatment in the multivariate regression model. Aripiprazole appears to have a safer profile compared with risperidone and cyamemazine. This is not in line with adult studies that found no influence of SGAs (Hummer et al. 2005), but to our knowledge, no study investigated in detail each compound in a sample large enough to have statistical power.
We found a high proportion (60%, n = 121) of hyperprolactinemia among inpatients. As expected, we found a significant association with gender, even if the pathological threshold is 5 ng/mL higher in girls over 15 years of age (Peveler et al. 2008). Also, as expected, patients with AP treatment showed higher PBL than patients free from AP treatment. The bivariate analysis showed that PBL rates were influenced by diagnosis categories. But the diagnostic effect did not remain in the multivariate model. The hypothesis that treatment operates as a confounding variable can be proposed.
The most striking result regards the worsened profile of risperidone compared with aripiprazole and cyamemazine and compared with patients free from AP treatments. Aripiprazole and cyamemazine appear to have no or negligible effect on PBL as there is no difference between patients treated with these two APs and patients free from treatment. In agreement with the literature from double-blind controlled trials, patients taking aripiprazole show less iatrogenic hyperprolactinemia (Raffin et al. 2014). One long-term study (30 weeks), including 161 young patients confirmed that aripiprazole decreases PBL (Findling et al. 2013). Despite many studies on risperidone in children and adolescents, its effect on PBL has been poorly reported (Cohen et al. 2012). Three studies assessed PBL changes with risperidone reporting mostly a transitory prolactin increase without any clinical impact (Turgay et al. 2002; Luby et al. 2006; Findling et al. 2013). In the TEOSS study, patients with risperidone showed an average decrease from baseline. Despite this decrease, patients receiving risperidone maintained higher levels than patients in other treatment groups did. Interpretation is difficult as patients were not naive at inclusion in the study (Sikich et al. 2008; Findling et al. 2010).
The interesting profile of aripiprazole may be explained by the specific pharmacologic profile of this compound among SGAs. Aripiprazole is a partial agonist for D2 dopaminergic receptors, which in itself limits the effect of hyperprolactinemia. It is also a partial agonist for 5HT2A receptor, thereby restoring the balance between dopaminergic and serotoninergic systems and retaining biological markers closer to the physiological balance (Besnard et al. 2014; Raffin et al. 2014). Regarding cyamemazine, this treatment is often used as a symptomatic treatment of anxiety and agitation for a short period of time. Complementary analysis confirmed that treatment duration was shorter when patients were treated with cyamemazine compared with other treatments (data not shown).
It is very difficult to define the exact rate of vitamin D deficiency in the general pediatric population, as studies have used different thresholds for vitamin D deficiency, and samples are often small. Vitamin D deficiency occurs commonly among healthy European infants, children, and adolescents (Braegger et al. 2013). However, although we were unable to compare our result to the rate of vitamin D deficiency in the general pediatric population, 89% of vitamin D deficiency is an ultrahigh rate. We cannot say that the high rate we found is due to the psychiatric condition, but we can be concerned by the cumulative risk in this special population.
Indeed, low VDBL combined with hyperprolactinemia potentially have consequences on the health of young patients given that they are risk factors for osteoporosis. Children and adolescents represent a particularly vulnerable population because they will potentially receive AP treatment over longer periods of time and also because they will combine several risk factors of osteoporosis, such as smoking, poor nutrition, lack of exercise, alcohol, or caffeine consumption. As a large majority of inpatients shows vitamin D deficiency, we recommend Vitamin D supplementation (Bonjour et al. 1997; Holick 2006a, 2006b).
Regarding PBL, we question whether current guidelines that recommend not to monitor hyperprolactinemia are legitimate in young patients. Most recommendations are based on the fact that hyperprolactinemia is asymptomatic in most cases. Performing a systematic research of sexual symptoms to estimate hyperprolactinemia among patients receiving AP in day-to-day practice seems enough to assess all short-term and long-term PBL AE (Citrome 2008). A few guidelines recommend to systematically monitor PBL after three months of treatment with risperidone, and if normal, on a yearly basis thereafter in asymptomatic children. Authors precise that prepubertal children may not be symptomatic in case of hyperprolactinemia (Pringsheim et al. 2011; Besnard 2014).
Given that (1) young patients with severe mental illness are at cumulative risk of osteoporosis and (2) osteopenia is reversible when hyperprolactinemia disappears (Biller et al. 1992), it would be necessary to reconsider systematic monitoring of PBL for patients taking AP and not only systematically look for sexual prolactin symptoms. In case of iatrogenic hyperprolactinemia, it appears legitimate to reconsider the use of the AP medication. Alternative strategies could be considered: (1) reducing the dose of SGA as there is some evidence to support that prolactin elevation and prolactin-related side effects are dose dependent for risperidone and olanzapine (Kleinberg et al. 1999; Alfaro et al. 2002); (2) switching to a prolactin-sparing agent (e.g., aripiprazole); (3) if the SGA cannot be switched, consider a specialist consultation for further investigation and management. In case of clinical concern and prolactin-related side effects, consider also specialist consultation for further investigation regarding other causes of hyperprolactinemia and/or amenorrhea (Ho et al. 2011).
Despite some strengths (large number of patients, assessment of other risk factors for VDBL, both PBL and VDBL available for a large subsample of patients, prospective design, and assessment of the hormonal effects of three APs among the most frequently prescribed), the results should be interpreted in light of several limitations. First, the study was cross-sectional and did not control for dosage timing to admission. Second, we did not have a control group to assess VDBL and PBL in a sample of healthy French adolescents. Third, the risk of osteoporosis is only a speculation regarding the current knowledge of the risk factors of osteoporosis in young patients. Only large prospective longitudinal studies in youths or large case–control studies in adults, exposed or not to AP, would give a definitive answer. Fourth, the low rate of enrolment due to the severity of the patients supported in the department may be a bias. Indeed, clinicians might be more likely to insist to assess VDBL and PBL, where there is a clinical concern, even if there is recommendation to assess VDRL and PBL to all the inpatients. Finally, the current study did not investigate other AP AE, meaning that the safer profile of aripiprazole compared with risperidone may not be the same regarding weight gain or extrapyramidal AE.
Conclusions
Youth inpatients with severe mental condition may be at particular risk of osteoporosis. They often combine vitamin D deficiency, other habit risk factors of osteoporosis, and iatrogenic hyperprolactinemia. Because adolescence is a period of bone construction and a critical window of opportunity for maximizing bone mass, some of these risk factors may be prevented first by vitamin D supplementation, and second by an appropriated monitoring of PBL and treatment modification taking into account the clinical particularity of each patient. In terms of treatment decision, aripiprazole appears to have a more interesting hormonal profile than risperidone and cyamemazine.
Clinical Significance
Among 484 young inpatients, 433 (89%) had a VDBL under the recommended threshold (30 ng/mL). Among 502 young inpatients, 121 (60%) had hyperprolactinemia. Vitamin D deficiency and hyperprolactinemia are two hormonal risk factors for osteoporosis. In both models, aripiprazole had a safer profile compared with other APs. Adolescence is a period of bone construction and a critical window of opportunity for maximizing bone mass. We recommend vitamin D supplementation in young patients with severe mental condition. It could be interesting to reconsider regularly monitoring PBL among youth patients treated with other APs than aripiprazole.
Footnotes
Acknowledgments
The authors wish to thank Dr. Rachida Inaoui and Dr. Claudine Laurent-Levinson for their assistance in edits to this article.
Disclosures
During the last 2 years, David Cohen reported past consultation for or the receipt of honoraria from Otsuka, Shire, Lundbeck, Jansen, and Roche. Olivier Bonnot reported past consultation for or the receipt of honoraria from Otsuka, Shire, Orphan Europe, and Actelion. The other authors have no conflict of interest to report.