
Abstract
Objectives:
Attention-deficit/hyperactivity disorder (ADHD) is often treated with psychostimulants. Psychostimulants' adverse effects on body mass index standard deviation score (BMI-sds) and height in children/adolescents with ADHD have been reported. However, literature is inconsistent, and it is unclear whether the observed effects are dosage- and/or BMI-dependent. Therefore, the aim of this retrospective observational study is to evaluate the influence of psychostimulants on BMI-sds and height-sds in a pediatric cohort with ADHD from an outpatient clinic, and to study the correlation between psychostimulant dosage and BMI-sds and height-sds change.
Method:
Participants ≤18 years of age diagnosed with ADHD who started with psychostimulants (methylphenidate) were studied. Changes in BMI-sds and height-sds over an 18-month treatment period were assessed in subgroups according to baseline BMI-sds, gender, and age. Furthermore, correlations between BMI-sds, height-sds, and psychostimulant dose were studied.
Results:
In total, 298 participants [median age 9.8 years, height-sds 0.0, BMI-sds 0.5, psychostimulant dosage 0.5 (0.2–1.4) mg/kg/day] were analyzed, with an underweight, overweight, and obesity prevalence of 5%, 21%, and 7%, respectively. After 18 months of treatment a significant decline in BMI-sds (−0.4) and height-sds (−0.2) was observed. These effects were consistent in all subgroups except for no change in BMI-sds in the underweight subgroup and no change in height-sds in the overweight subgroup. Medication dosage was weakly correlated with change in BMI-sds [r = −0.3 (−0.9 to +0.5); p < 0.01] and height-sds [r = −0.2 (−0.4 to −0.1); p = 0.01].
Conclusion:
After 18 months of psychostimulant treatment, a significant decline in BMI-sds and height-sds was observed. However, the correlation with psychostimulant dosage was weak, and the decline was not observed in all subgroups. Therefore, further studies on the etiology of BMI-change are warranted, particularly with regard to the ADHD symptoms.
Introduction
A
ADHD is seen in all weight categories as in the general population, although a recent review and meta-analysis show a 40% higher prevalence of obesity in children/adolescents with ADHD compared with healthy children/adolescents (Cortese et al. 2016). This observation might be explained by differences/variation in expression of ADHD symptoms. It has been suggested that impulsive and inattentive components of ADHD could lead to irregular and dysregulated eating patterns leading to a higher risk of overweight/obesity (Cortese and Castellanos 2014; Khalife et al. 2014; Cortese et al. 2016; Nigg et al. 2016). In addition, it has been described that children with ADHD spend less time practicing sport and spend more time watching TV (Lingineni et al. 2012). The (momentary) hyperactivity could therefore be not enough to reduce the risk of overweight/obesity. Consequently, body mass index (BMI) might be a reflection of the variability of ADHD symptoms.
Psychostimulants are frequently used in the treatment of AHDH and have been associated with weight loss due to their known negative effect on appetite (Barkley et al. 1990; Efron et al. 1997; Swanson et al. 2006; Waring and Lapane 2008; Poulton et al. 2013; Schwartz et al. 2014; Gungor et al. 2016). However, a decrease in body weight is not observed in all studies (Biederman et al. 2010; Dubnov-Raz et al. 2011; Fliers et al. 2013; Cortese et al. 2016), and some even reported a higher obesity prevalence in those under psychostimulant treatment (Erhart et al. 2012; Racicka et al. 2015).
Psychostimulants have also been associated with the reduction of growth velocity and target height (Faraone et al. 2008). Although literature is inconsistent, some studies report growth suppression during treatment (Poulton and Cowell 2003; MTA Cooperative Group 2004; Charach et al. 2006; Swanson et al. 2006; Dura-Trave et al. 2012; Germinario et al. 2013; Powell et al. 2015), while others did not (Biederman et al. 2010; Dura-Trave et al. 2012; Harstad et al. 2014). On the contrary, it has been suggested that the effect of psychostimulants on height attenuates over time and is therefore of no clinical significance (Poulton and Cowell 2003; Charach et al. 2006; Dura-Trave et al. 2012; Germinario et al. 2013; Powell et al. 2015).
From the foregoing, it appears that there is no consistency in the association between psychostimulant treatment and weight reduction and/or growth suppression in pediatric populations with ADHD. In addition, it seems unclear whether medication dosage is influencing the association and whether there are differences between BMI-categories. Therefore, the aim of this retrospective observational study is to evaluate the influence of psychostimulants on BMI standard deviation score (BMI-sds) and height-sds over an 18-month treatment period, in a pediatric cohort with ADHD visiting an outpatient clinic. In addition, the correlation between psychostimulant dosage and BMI-sds and height-sds change is evaluated.
Method
Study design and subjects
This retrospective observational study was approved by the Medical Ethics Committee of the St. Antonius Hospital, Nieuwegein/Utrecht, the Netherlands (Z16.059). As the data were obtained from routine clinical care and anonymized, written informed consent was not required. All patients who visited the pediatric outpatient clinic of the St. Antonius Hospital between January 2008 and July 2016 were screened for the diagnosis treatment combination code (DBC-code) “ADHD.” Patients were included if they were aged ≤18 years, diagnosed with ADHD, and started with psychostimulants (methylphenidate) for the first time, and did not use any additional psychiatric medication.
Measurements
A diagnosis of ADHD was established by a psychologist and/or pediatrician based on criteria of the Diagnostic and Statistical Manual (DSM) IV/5 (American Psychiatric Association 2000, 2013), using questionnaires and observations by care givers and teachers. A distinction was made between the predominantly inattentive and predominantly combined type of ADHD. Baseline (T = 0) was defined as the start of psychostimulant treatment, which was titrated and (as needed) adjusted according to national guidelines, with a maximum of 2 mg/kg/day (Landelijke Stuurgroep Multidisciplinaire Richtlijnontwikkeling in de GGZ 2007; Nederlands Kenniscentrum voor Farmacotherapie bij Kinderen 2017).
Collected baseline data were as follows: date of birth, gender, type of disease (i.e., predominantly inattentive, predominantly combined), date of methylphenidate start, type of methylphenidate (i.e., immediate or sustained release), medication dosage (mg/kg/day), and weight and height. Participants with incomplete data at baseline were excluded. Data gathered up to 18 months after treatment start were as follows: date of visit, type of methylphenidate, medication dosage, and weight and height. Since participants did not visit the pediatric outpatient clinic at predetermined time points, a window was created to define the time of visit at T = 18 months (i.e., day 540, range 480–600 days). Participants were excluded from analysis if the follow-up visit took place outside the defined time window or if data at 18 months were incomplete. In addition, data after 6 (day 180, range 120–240) and 12 months (day 360, range 300–420) of psychostimulant treatment were gathered.
Weight and height were measured using a digital scale (Seca, Hamburg, Germany) with an accuracy of 0.05 kg and a digital stadiometer with a precision of 0.1 cm (DGI 250D; De Grood, Nijmegen, the Netherlands), respectively. BMI and the corresponding age and gender adjusted BMI-sds and height-sds, were calculated according to national growth charts using the TNO growth calculator for professionals (TNO 2010). Participants were classified into four subgroups defined by baseline BMI-sds, that is, underweight (BMI-sds ≤−1.1), normal weight (BMI-sds >−1.1 to ≤1.1), overweight (BMI-sds >1.1 ≤2.3), and obesity (BMI-sds >2.3). In addition, participants were classified into children (≤10 years) and adolescents (>10 years).
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics, version 24 (IBM SPSS Statistics, Chicago, IL). Anticipating that the number of participants in the underweight and obese subgroup could be limited, all data were reported as median with range for continuous data or as frequencies with percentage for categorical data. Differences between the BMI subgroups were compared using the Kruskal–Wallis test for continuous data, and the chi-squared test for dichotomous data. In addition, comparisons between males versus females and children versus adolescents were performed using the Student's t-test. Differences in BMI-sds, height-sds, and psychostimulant dosage between T = 0 and T = 18 were analyzed using the paired t-test/Wilcoxon signed-rank test and were conducted for all participants and separately for the subgroups.
Finally, a multivariable linear regression analysis was conducted to assess the influence of psychostimulant dosage on both BMI-sds and height-sds change. Potential confounders (i.e., age, gender, type of disease, type of methylphenidate, and baseline BMI-sds) were retained in the final regression model if they influenced the coefficient of interest with more than 10%. All results were considered significant at a α-level of 5%.
Results
Figure 1 shows that 1294 patients were screened for inclusion. A total of 558 participants were included, of which 298 were analyzed. Characteristics of participants excluded for analysis were not significantly different from participants analyzed (Supplementary Table S1; Supplementary Data are available online at
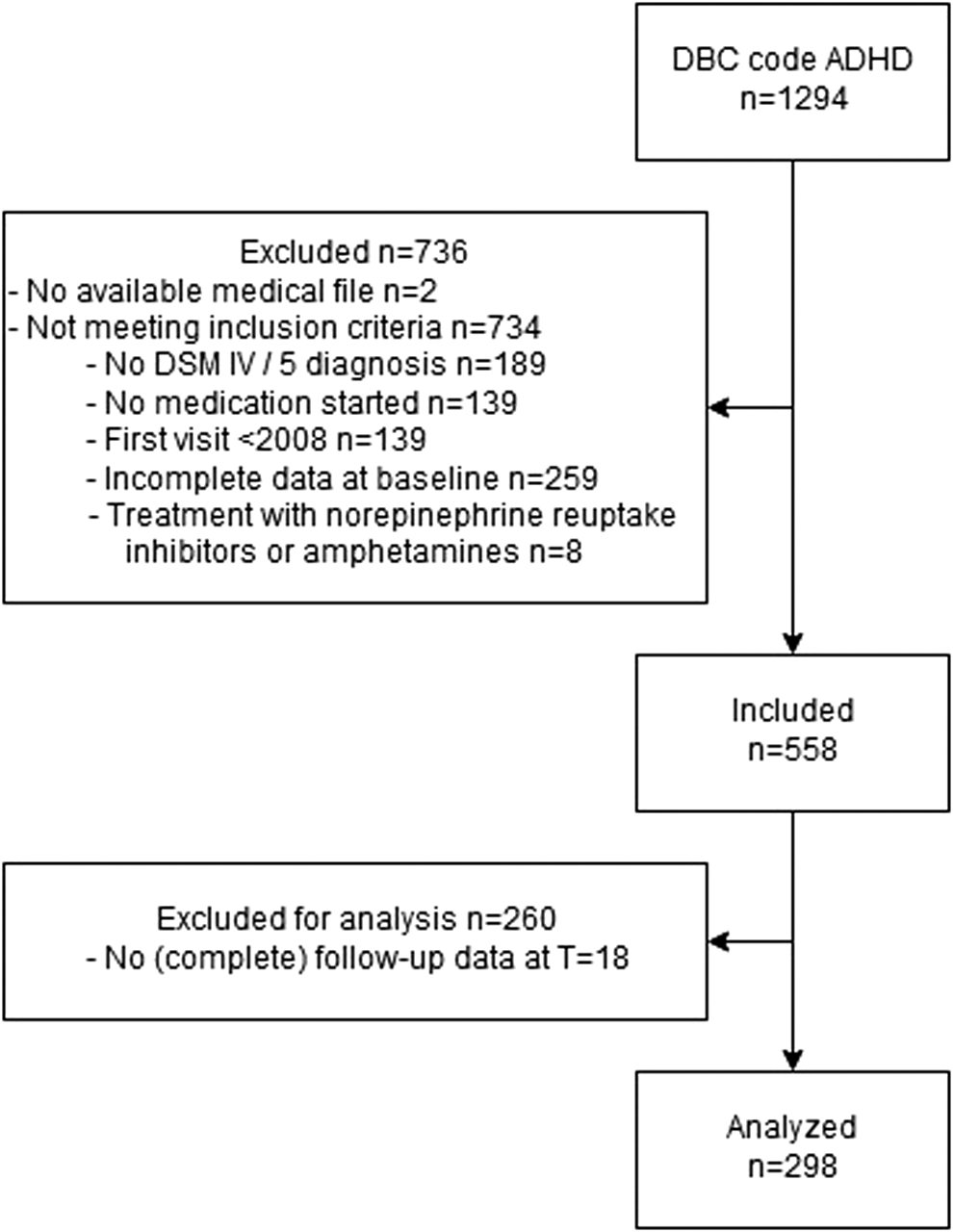
Flowchart of the study population.
Table 1 shows the baseline demographics of participants, who were primarily boys (72%). Five percent of the participants were classified as underweight, 66% as normal weight, 21% as overweight, and 7% as obese. The BMI subgroups differed significantly in height-sds. Overweight and obese participants had a significant higher height-sds in comparison with underweight (p = 0.04, p = 0.04) and normal weight (p = 0.01, p = 0.04) participants. The predominantly combined type of ADHD was diagnosed in 65% and the predominantly inattentive type in 35% of the participants. In 79%, immediate release methylphenidate was first prescribed. The BMI subgroups differed significantly in medication dosage (mg/kg/day), as overweight participants received a significantly lower medication dosage in comparison with underweight and normal weight participants (p < 0.01, p = 0.01).
p-Values in bold are significant at <0.05.
Data presented as number (%) or median with range. p-Values for Kruskal–Wallis test (continuous data) and χ2 test (categorical data).
BMI, body mass index; IR, immediate release; NW, normal weight; O, obesity; OW, overweight; sds, standard deviation score; SR, sustained release; UW, underweight.
Males were significantly more often diagnosed with the predominantly combined type of ADHD in comparison with females (71% vs. 52%; p < 0.01). No differences were observed in anthropometric measurements except for height velocity which was significantly lower in females (6.5 vs. 5.2; p < 0.01) (Supplementary Table S2). Children were significantly more often diagnosed with the predominantly combined type of ADHD (77% vs. 51%; p < 0.01) and used more frequent immediate release psychostimulants (85% vs. 70%; p < 0.01) in a higher dosage (0.6 vs. 0.5 mg/kg/day; p = 0.01) compared to adolescents. By definition, significant differences were observed in age, height, weight, and BMI. No differences were observed in height-sds, BMI-sds, or height velocity (Supplementary Table S3).
Figure 2a shows the observed differences in BMI-sds after 18 months of psychostimulant treatment for the total population, for which a significant decrease was observed (p < 0.01). In the normal weight, overweight, and obese subgroup, a significant decrease was observed, but not in the underweight subgroup (Table 2). No significant differences were observed in change in BMI-sds between male and female participants (Supplementary Table S2). Children decreased significantly more in BMI-sds compared with adolescents (−0.5 vs. −0.3; p = 0.03) (Supplementary Table S3). At T = 18, significantly less participants were classified as overweight (14% vs. 21%) and obese (4% vs. 7%), and significantly more as underweight (14% vs. 5%). Four percent of the participants were classified in a higher BMI subgroup at T = 18.
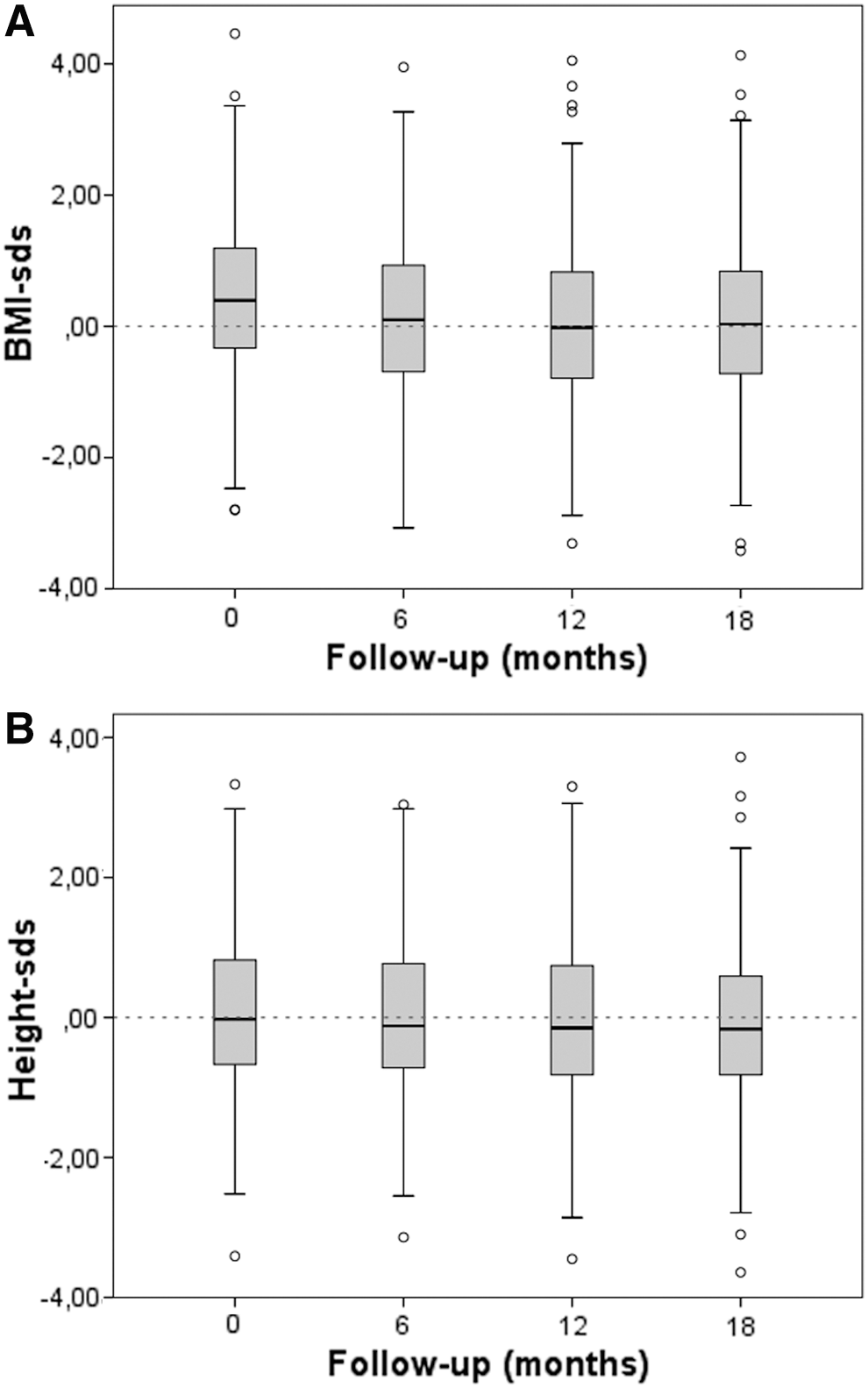
Box plots with median and interquartile ranges of
p-Values in bold are significant at <0.05.
Data presented median with range. p-Values for paired t-test (normally distributed data), Wilcoxon signed-rank test (nonparametric data).
BMI, body mass index; NW, normal weight; O, obesity; OW, overweight; sds, standard deviation score; UW, underweight.
A significant decrease in height-sds was observed in the total population and all subgroups, except the overweight subgroup (Fig. 2b and Table 2). Females decreased significantly more in height-sds in comparison with males (−0.2 vs. −0.1; p = 0.02) (Supplementary Table S2), and children decreased more in height-sds than adolescents (−0.2 vs. 0.0; p < 0.01) (Supplementary Table S3).
A significant increase in medication dosage (mg/kg/day) was noticed over the 18-month treatment period in the total population, and in the underweight, normal weight, and overweight subgroup, while in the obese subgroup no increase was shown (Table 2). No differences in dosage change were observed between males and females (Supplementary Table S2). In children the dosage increased significantly more than in adolescents (0.2 vs. 0.1; p < 0.01) (Supplementary Table S3).
In Figure 3, it is shown that psychostimulant dosage was weakly correlated with change in BMI-sds [r = −0.3 (−0.9 to −0.4); p < 0.01] and height-sds [r = −0.2 (−0.5 to −0.1); p = 0.01]. After adjustment for confounding factors (model BMI-sds change: baseline BMI-sds and type of methylphenidate; model height-sds change: age and type of methylphenidate) in a multivariable linear regression analyses, the correlations did not change [BMI-sds r = −0.3 (−0.9 to 0.5); p < 0.01, and height-sds r = −0.2 (−0.4 to −0.1); p = 0.01).
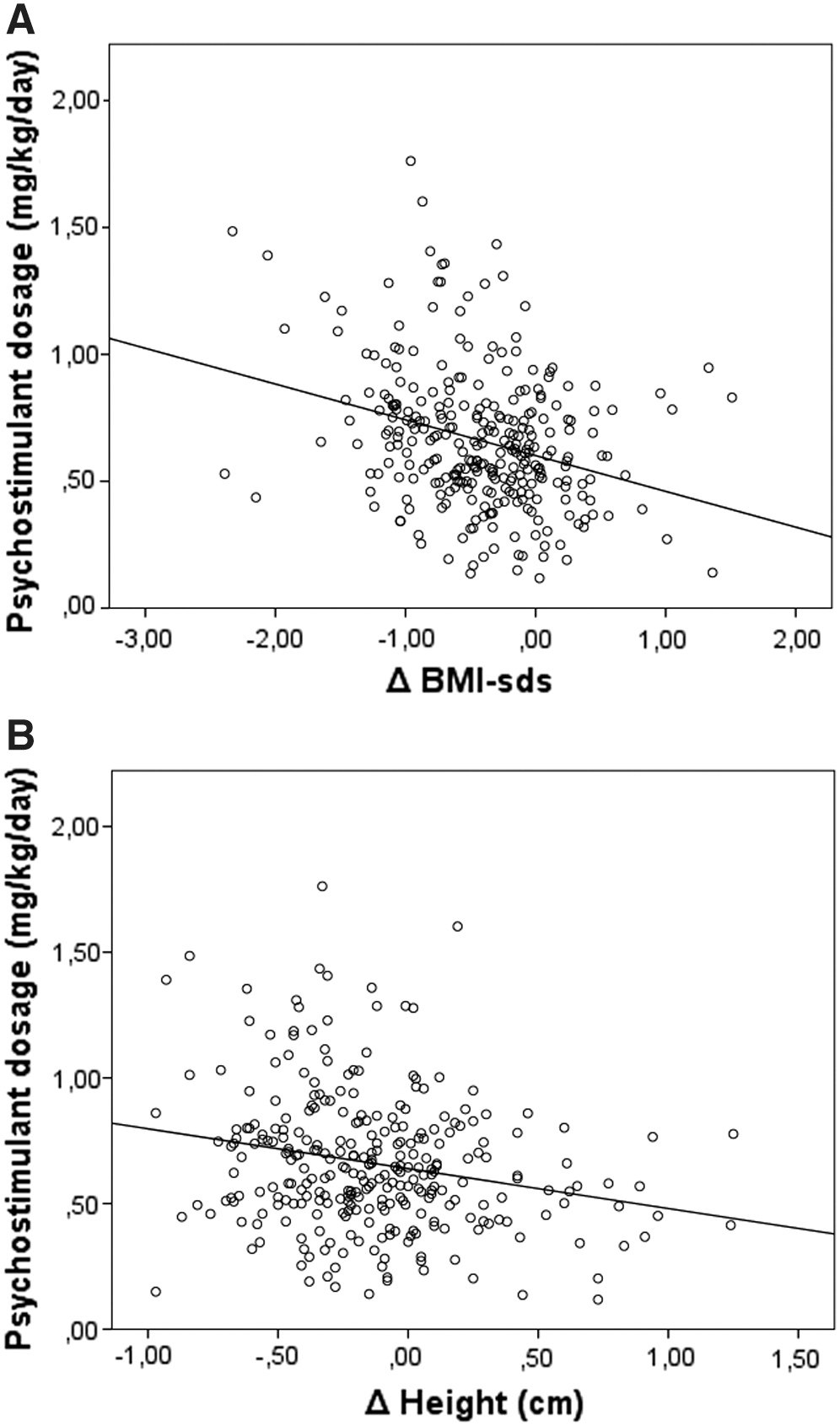
Scatter dots representing the correlation between
Discussion
Psychostimulants are suggested to be associated with weight reduction and growth suppression. As a result of which, there is some restraint in the use of psychostimulants that may lead to a lower quality of life due to untreated symptoms (Poulton and Cowell 2003; MTA Cooperative Group 2004; Charach et al. 2006; Swanson et al. 2006; Faraone et al. 2008; Dura-Trave et al. 2012; Germinario et al. 2013; Poulton et al. 2013; Powell et al. 2015) However, literature is inconsistent and it is unknown whether the observed effects are dosage and/or BMI dependent, as BMI may be a reflection of the variability of ADHD symptoms. Therefore, this retrospective observational study evaluated the influence of psychostimulants on BMI-sds and height-sds over an 18-month treatment period and studied the correlation between psychostimulant dosage and BMI-sds and height-sds change.
In the current study, a higher prevalence of overweight (21% vs. 9%) and obesity (7% vs. 3%) was observed at study start in comparison with the prevalence in the pediatric population of the Netherlands (RIVM 2016). Although 72% of the study population was male, gender did not influence this observation as the prevalence of overweight/obesity in boys and girls is almost equal in the Netherlands (RIVM 2016). The observed prevalence of overweight/obesity in our study is in line with other studies; however, it should be mentioned that there were differences in study designs (Holtkamp et al. 2004; Hubel et al. 2006; Dubnov-Raz et al. 2011; Fliers et al. 2013). One study included participants irrespectively of start of psychostimulant treatment (Dubnov-Raz et al. 2011). Other studies collected their data through a telephone survey, were performed in a small population, or included only males or patients with ADHD of the predominantly combined type (Holtkamp et al. 2004; Hubel et al. 2006). Consequently, a reliable comparison between studies is impossible.
The prevalence of underweight in the current study was comparable with the prevalence in the pediatric population of the Netherlands (RIVM 2016). However, another study performed in the Netherlands reported significantly less underweight in the ADHD population in comparison with the prevalence in the Netherlands (Fliers et al. 2013). This difference might be explained by the fact that they included only children of Caucasian descent with ADHD of the predominantly combined type. Since there was no studied population available to compare our study population with, we compared our analyzed participants with the excluded participants. Because these groups were comparable, it can be concluded that the observed prevalences are in concordance with the pediatric ADHD population of the Netherlands.
Weight and target height reduction are assumed to be adverse effects of psychostimulant treatment. This assumption derived from the fact that psychostimulants increase the dopamine concentration at the synaptic space (Wilens 2006). Dopamine inhibits gastric emptying and is therefore a well-known appetite reducer (Volkow et al. 2011). In addition, dopamine is suggested to inhibit growth hormone, which might cause growth retardation (Faraone et al. 2008). However, literature is inconsistent on the actual effect upon this in daily clinical practice.
In the current study, a reliable comparison between our results and the literature could not be performed due to differences in study populations (i.e., gender, age, and type of disease) (Swanson et al. 2006; Fliers et al. 2013; Poulton et al. 2013), follow-up period (Biederman et al. 2010; Schwartz et al. 2014), and medication use (Dubnov-Raz et al. 2011; Schwartz et al. 2014). In contrast to the studies mentioned above, our study focused on the effect of psychostimulants in the different BMI subgroups. In this study, a significant reduction in BMI-sds after 18 months of psychostimulant treatment was observed, which resulted in fewer participants classified as obese and/or overweight, and more as underweight. However, the decline in BMI-sds was not observed in the underweight subgroup, while they received the highest psychostimulant dosage (mg/kg/day). Furthermore, 4% of the participants were classified in a higher BMI subgroup at the end of the follow-up period.
These observations along with the weak correlation between BMI-sds change and psychostimulant dosage raises the question whether reduction in weight is actually caused by a reduction in appetite induced by psychostimulants. As stated before, a patient's BMI may be a reflection of specific ADHD symptoms associated with weight gain. Reduction in BMI-sds may therefore be related to a reduction of ADHD symptoms rather than a side effect of psychostimulants, which was also suggested in previous studies (Cortese and Castellanos 2014; Khalife et al. 2014; Cortese et al. 2016; Nigg et al. 2016). This is underlined by the fact that the predominantly inattentive subtype of ADHD was more frequently diagnosed in the adolescent and underweight subgroup, in which smaller reductions in BMI-sds were observed. However, we can only speculate on this theory since the symptoms were not systematically reported.
A significant decline in height-sds was observed in the total study population. Although the decline was significant, it was not observed in all subgroups and differences were rather small, which poses the question whether this observation is clinically relevant. However, it should be mentioned that the used dosage may have influenced this observation, as the subgroups with a lower dosage showed a slighter decline in height-sds. Especially, since it can be assumed that a higher dosage of psychostimulants leads to a higher dopamine availability which might result in a greater inhibition of growth hormone and thereby a more pronounced effect on growth (Swanson et al. 2006; Wilens 2006).
Literature is inconsistent in the association between psychostimulants and target height reduction (Faraone et al. 2008). In addition, it has been suggested that the effect of psychostimulants on height attenuates over time and is thereby not affecting the target height (Poulton and Cowell 2003; Charach et al. 2006; Dura-Trave et al. 2012; Germinario et al. 2013; Powell et al. 2015). This could be due to a feedback system resulting in an increase in dopamine receptors in the synaptic space, as a result of which the free dopamine levels returns to the normal level, as described in rats (Faraone et al. 2008). Consequently growth hormone is inhibited only temporarily and has thereby no consistent effect on height velocity and therefore not affecting the target height (Faraone et al. 2008).
We were not able to study the effect on target height, since our participants did not reach their final height during the study period. However, height velocity was within the normal range in all subgroups (Tanner and Davies 1985), and only a weak correlation was observed between psychostimulant dosage and change in height-sds. These findings suggest that the decline in height-sds is not related to psychostimulants, but physiological due to normal variation of growth in height and support the previously mentioned theory. In addition, height velocity is related to nutritional status with reversible growth retardation in underweight and relative growth acceleration in overweight/obesity (Faraone et al. 2008).
In this population-based study, the effect of psychostimulant dosage on BMI-sds and height-sds was systematically evaluated in ADHD patients during a follow-up period up to 18 months. In contrast to previous studies, our study focused on the effect of psychostimulants dosage in different BMI subgroups. Moreover, only naive patients for psychostimulants without additional psychiatric medication were included, whereby bias due to previous pharmacological ADHD treatment was excluded. However, certain limitations due to the retrospective study design must be considered.
First, no controls without psychostimulant treatment were included, since these patients do not have a follow-up at pediatric outpatient clinics in the Netherlands. However, as it may be assumed that children grow according to their own percentile during normal development, height-sds and BMI-sds can be used to evaluate changes in growth over time. In addition, only patients who started with methylphenidate were included, since amphetamines are in general prescribed by a pediatric psychiatrist and not by a general pediatrician. Therefore, no statements could be made on the influence of amphetamines on weight and height change.
Prevalent comorbidities such as depression and conduct disorder could not be taken into account as potential confounder, since these patients are mainly treated at (pediatric) psychiatric clinics in the Netherlands. Furthermore, relatively many participants were excluded for analysis. Some participants were lost to follow-up and others were referred to specialized (pediatric) psychiatric clinics or followed up by the general practitioner. However, as stated before characteristics of participants excluded for analyses were not significantly different from those analyzed. Therefore, results were most likely not affected by the participants lost to follow-up and thus applicable for the entire pediatric ADHD population of the Netherlands. Since symptoms of ADHD were not systematically recorded in medical files, we could not objectify whether medication dosage was adjusted according to symptomatology. In addition, we could not determine which symptoms might play a role in any change in BMI-sds.
Finally, our results might have been influenced by the fact that methylphenidate tablets are only available in fixed dosages, affecting the prescribed dosage in mg/kg/day. This could also explain the relatively lower dosage in the overweight and obesity subgroups. Since many patients are restrained to use multiple tablets to achieve a dosage comparable with other weight categories, especially due to the fear for reduction in appetite and concerns about target height. Impact of above factors on the results cannot be ruled out. Therefore, further studies on the etiology of BMI-change are warranted. Focus on the ADHD symptoms seems to be of particularly relevance.
Conclusion
After 18 months of psychostimulant treatment a significant decline in BMI-sds and height-sds was observed. However, the correlation with medication dosage was weak and the decline was not observed in all subgroups. Therefore, further studies into the etiology of BMI-change are warranted, particularly with regard to the ADHD symptoms.
Clinical Significance
Psychostimulant treatment in patients with ADHD is associated with weight reduction and growth retardation, as a result of which there is some restraint in the use which may lead to a reduction in quality of life. However, reports in literature are inconsistent. Since BMI might be a reflection of the variability of ADHD symptoms, we focused on the effect of psychostimulants dosage in different BMI subgroups. Our data showed that weight reduction and growth retardation were not observed in all BMI subgroups, and were only weakly correlated with psychostimulant dosage. This may imply that psychostimulants are not the primary cause of weight reduction and growth retardation, are therefore safe to use and the fear for side effects can be waived. In conclusion, further studies into the etiology of weight reduction and growth retardation are warranted, particularly with regard to the reduction in ADHD symptoms.
Footnotes
Disclosures
All authors declare that they have nothing to disclose regarding institutional or corporate/commercial relationships going back 36 months, which might pose a conflict of interest regarding publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.