
Abstract
Objective:
Parasomnias are common in childhood but there is no established treatment for parasomnias. The aim of this study was to (1) report on the outcome of using L-tryptophan to manage parasomnias in children and (2) examine sleep architecture and subjective psychological/sleep symptoms in children with parasomnia.
Method:
A retrospective analysis was conducted of charts of children (3–18 years old) who underwent polysomnographic testing and were diagnosed with primary parasomnia. Study patients were either prescribed L-tryptophan (daily dose range: 500–4500 mg, mean dose of 2400 mg) to manage their parasomnias or administered no treatment whereby parents/guardians declined treatment. Questionnaires assessing sleep and psychosocial symptoms were administered at the initial clinical consultation and a follow-up parasomnia outcome questionnaire was administered over the phone to parents/guardians.
Results:
One hundred and sixty-five children (106 boys, 59 girls) received a sleep diagnosis of primary parasomnia. A significantly (p < 0.001) higher proportion (84%) of children taking L-tryptophan experienced improvements in their parasomnia symptoms compared with those (47%) who chose not to use L-tryptophan. Polysomnography revealed that children with parasomnias had an altered sleep architecture based on age-related normative values. Children with a diagnosis of parasomnia were also subjectively more fatigued and endorsed more depressive symptoms.
Conclusions:
This study finds that parasomnias in children are not benign and that treatment with L-tryptophan provides a favorable outcome. Children diagnosed with parasomnia had altered sleep architecture, were more fatigued, and endorsed depressive symptoms. This study supports the need to diagnose and treat parasomnias in children.
Introduction
N
The overall opinion from existing literature is that childhood parasomnias are not of significant concern since they are self-limiting (Kotagal and Chopra 2012; Pelayo and Yuen 2012). Although most parasomnias in children resolve spontaneously by age 12 years (Kotagal and Chopra 2012), an exact figure of the percentage of children having parasomnias that persist into adolescence and adulthood is unknown. Thus, although parasomnias may be benign for some children, this is certainly not the case for all. Furthermore, parasomnias that persist into adolescence may cause “significant stress and are often indicative of underlying psychopathology” (Vgontzas and Kales 1999).
Presumably, as the majority of adolescents are chronically sleep restricted (Roberts et al. 2011), any additional sleep disturbance is poorly tolerated, but it is unclear whether the psychopathology could be cause or effect, or just a co-occurrence with the parasomnias. It is notable that a recent publication focusing on adult sleepwalkers (Lopez et al. 2013) indicates that symptoms started at the age of 9 years on average and lead to complaints of greater levels of daytime sleepiness, fatigue, insomnia, mood disorders, and poorer quality of life as compared with controls.
Neuropsychological and sleep sequelae have been widely reported in association with childhood parasomnias. Bruxism, a parasomnia that has been well studied in children, is associated with greater somatic complaints, separation anxiety, increased anxiety, nervousness, unhappiness, temper outbursts, hyperactivity, and inattention (Guilleminault et al. 2003; Herrera et al. 2006; Petit et al. 2007).
Parasomnias in children have also been linked to increased rates of physical illness, delayed toilet training, behavioral disturbances, adjustment problems, learning difficulties, and greater sleep fragmentation (Herrera et al. 2006). Similarly, Guilleminault et al. (2003) reported that 61% of children with parasomnias had either a sleep breathing disorder or restless legs, whereas Kahn et al. (1989) reported an association between parasomnias and a spectrum of sleep difficulties lasting longer than 6 months. Evidence also exists for an association between sleep difficulties experienced by children resulting in parental daytime somnolence and negative impact on parental daytime function (Boergers et al. 2007).
There are no FDA-approved therapies for the management of NREM parasomnias in children. Medications that have been used “off-label” for treatment of parasomnias in children and adolescents include benzodiazepines, antidepressants (selective serotonin reuptake inhibitors and tricyclic antidepressants), and clonidine (a centrally acting alpha-agonist) (Schnoes et al. 2006; Kotagal and Chopra 2012; Pelayo and Yuen 2012).
There are no randomized, placebo-controlled trials of pharmacologic interventions for pediatric parasomnias and most studies on the efficacy of treatment have been conducted in adults (Pelayo and Yuen 2012). Furthermore, the mentioned pharmaceutical agents are all associated with multiple side effects that are of particular concern when administered to children. Parents are understandably reluctant for their children with parasomnia to be treated with these pharmaceutical agents. Cognitive behavioral therapy (CBT) has been used with limited success for the management of night terrors (Sadeh 2005) but is not widely available for children, and there is no evidence for CBT efficacy in managing other parasomnias.
L-tryptophan is an essential amino acid that is not synthesized by the body and is obtained through the diet. L-tryptophan at a dose of 1 g or more has sleep-promoting properties. It increases total sleep time and the amount of slow wave sleep, while reducing sleep onset latency and wake time after sleep onset (Hartmann and Spinweber 1979). L-tryptophan has been used successfully to treat symptoms of insomnia in adults (Brown et al. 1979) and a case study from our group revealed that treatment with L-tryptophan, titrated to a dose of 4500 mg daily for 4 weeks, decreased sleep fragmentation and reduced excessive daytime sleepiness in a patient with Prader–Willi Syndrome (Lee et al. 2011).
L-tryptophan has been reported to have few and relatively benign side effects including tremor, nausea, and dizziness, generally only encountered when taken at higher doses (70–200 mg/kg) or in association with SSRIs (Fernstrom 2012). We conducted a study in adults (Levitan et al. 2000), combining a therapeutic dose of a selective serotonin reuptake inhibitor with L-tryptophan 2000 mg daily for treatment of major depressive disorder in adults. Theoretically, such a combination could have led to serotonin syndrome but we noted no significant side effects. Importantly, L-tryptophan, unlike benzodiazepines, SSRIs, or TCAs, improves sleep without disrupting normal sleep architecture (Spinweber et al. 1983).
Children attending Youthdale Child and Adolescent Sleep Centre in Toronto, Canada, present with a wide spectrum of sleep difficulties, including NREM parasomnia. L-tryptophan has been prescribed to date only as a general sleep aid. Children in our clinic have achieved a beneficial response to L-tryptophan for the treatment of insomnia, and the impression was gained that a lower dose of L-tryptophan reduced or eliminated parasomnias. Consequently, we wished to investigate specifically the possible effects that this product might exert on NREM parasomnias. The favorable drug profile of L-tryptophan, in addition to being a natural substance, makes it a more acceptable treatment option for parents and caregivers.
The objectives of this study were to determine whether L-tryptophan administration leads to symptom improvement with NREM parasomnia. A secondary aim was to examine sleep architectural variables in children and adolescents with NREM parasomnias to assess sleep and psychosocial characteristics in children and adolescents with a diagnosis of parasomnia.
Methods
Ethics approval for this study was obtained from the Centre for Addiction and Mental Health Research Ethics Board. A total of 2142 charts of children with sleep disorders from the Youthdale Child and Adolescent Sleep Centre in Toronto were reviewed for this retrospective study. From those charts we selected 165 charts of boys and girls between the ages of 3 and 18 years who had a clinical diagnosis of NREM parasomnia. For this naturalistic study, children with all types of NREM parasomnia were included. Patients who were included in the study had either been prescribed treatment with L-tryptophan (daily dose range: 500–4500 mg, mean dose 2400 mg, as per clinical determination) or administered no treatment wherein parents/guardians declined treatment.
The diagnosis of NREM parasomnias was made by an experienced sleep physician and based on clinical history together with supportive evidence from a polysomnographic (PSG) sleep study and the exclusion of other sleep disorders, including nocturnal epilepsy. The majority of children diagnosed with NREM parasomnias presented most commonly with a history of enuresis, night terrors, somniloquy, or somnambulism.
Data from an overnight PSG sleep study and questionnaires were collected during this study. At the time of the initial clinical assessment, patients and their parents/guardians had responded to a questionnaire battery that included the Pediatric Daytime Sleepiness Scale (Drake et al. 2003), the Swanson, Nolan, and Pelham–IV Questionnaire (SNAP-IV) (Swanson 1992) assessment for attention-deficit/hyperactivity disorder (ADHD) symptoms, the Centre for Epidemiologic Studies in depression scale modified for children (CES-DC) (Faulstich et al. 1986), and the Screen for Child Anxiety Related Emotional Disorders (Birmaher et al. 1997).
In addition, a follow-up interview was administered over the phone to assess the status of parasomnia symptoms in those children prescribed L-tryptophan and in those for whom no treatment was given. The questions in this interview were conceived by the study team consisting of three experienced sleep physicians and a clinical researcher, and were formulated to mirror questions that would have been raised at the follow-up clinical assessment. For this study, an improvement of parasomnia symptoms was defined as either a reduction in frequency of occurrence or a total resolution of symptoms, and a worsening of parasomnia symptoms was defined as an increased frequency of symptoms.
No sample size determination was conducted for this study. A sample size calculation based on prevalence was not possible given the large range of frequency of occurrence of parasomnias (9%–84%) and the fact that this naturalistic study included children with all types of parasomnia symptoms. Group averages for the sleep architectural variables and scores on the questionnaires were compared with normative values. Children were divided into gender and batched into age groups (3–5, 6–9, 10–12, 13–15, and 16–18 years) to facilitate comparison with historical normative sleep architectural values (van den Bossche and de Weerd 2007; Williams et al. 2013). Based on the hypothesis that the group of children taking L-tryptophan would have a higher frequency of those with improvement in symptoms, chi square analysis was utilized to test for deviations of observed frequencies from expected frequencies.
Results
Charts from 106 (65%) boys and 59 (35%) girls (total group: 165) with a primary sleep disorder diagnosis of NREM parasomnias were reviewed for this study. The sleep studies of these children were conducted between the years 2007 and 2013. The average age of children is boys 10 ± 4 years (range 3–18) and girls 11 ± 4 years (range 4–18). Ninety-nine (60%) parents of 165 children diagnosed with NREM parasomnia were administered the follow-up parasomnia outcome interview; the parents/guardians of the remaining 66 children either declined participation in this study or were lost to follow-up. Types of NREM parasomnias more commonly observed included confusional arousals, somnambulism/nocturnal movement, sleep terrors, bruxism, and somniloquy.
PSG sleep data are given in Table 1. The data are grouped by gender and separated into age groups, and are expressed as means with standard deviation (SD). The PSG findings in these children were compared with age-matched reported normative values. Table 2 indicates how the sleep architectural variables in the study group compared with age-matched normative values.
Polysomnographic values, grouped by gender and separated into age groups, are expressed as means with standard deviation (SD) below.
TST, total sleep time; SOL, sleep onset latency; S1, stage 1 sleep; S2, stage 2 sleep; SWS, slow wave (stage 3) sleep; REM, rapid eye movement sleep; SE, sleep efficiency.
Sixty-nine (70%) of the 99 children had been prescribed L-tryptophan. Forty-four (64%) had continued to take L-tryptophan when the follow-up questionnaire was administered, whereas 25 (36%) had discontinued taking L-tryptophan. The remaining 30 children (30% of the 99 included in the study) had not been prescribed any treatment; 1 was unable to afford L-tryptophan, 5 were advised against taking L-tryptophan by their pediatrician, and 24 parents/guardians declined using a treatment or felt it was not needed. The latter group of 30 children served as a comparison group for those taking tryptophan. Table 3 details the status of the parasomnia symptoms in the 99 children whose parents/guardians responded to the follow-up parasomnia outcome questionnaire.
Daytime sleepiness and/or fatigue were the most commonly reported side effects.
A comparison of the 44 children taking L-tryptophan versus the 30 who declined use of L-tryptophan noted that the vast majority (84%) of children taking L-tryptophan showed improvements in their parasomnia symptoms compared with less than half (47%) of those who chose not to use L-tryptophan; chi square testing revealed this difference to be significantly different (p < 0.001). Furthermore, compared with those taking L-tryptophan, significantly more of those who declined use of L-tryptophan experienced a worsening of symptoms (30% of those who declined L-tryptophan versus 9% of those taking L-tryptophan, p < 0.001).
Lastly, significantly more (p = 0.003) of those who declined L-tryptophan treatment (23%) saw no improvement in their parasomnia symptoms when compared with those children taking L-tryptophan (7%). The children whose parents/guardians reported had discontinued use of L-tryptophan due to side effects (the only side effect symptoms endorsed were daytime sleepiness and/or fatigue) reported no further serious adverse side effects.
A chart review of all 165 children with the primary sleep diagnosis of NREM parasomnia was conducted. The majority of children with parasomnias had reduced total sleep time (boys 3–15 years, p < 0.05; girls 6–15 years, p < 0.03) and an elevated arousal index (boys 3–15 years, p < 0.04; girls 6–18 years, p < 0.02). In addition, 29% (n = 17) of girls and 44% (n = 44) of boys were found to have mild obstructive sleep apnea (OSA) (apnea hypopnea index, AHI 1.5–5) and one girl and three boys had moderate OSA (AHI 5–10) OSA. Lastly, two girls and six boys were found to have elevated periodic limb movements (PLMs) with a PLM index >5. Children with either OSA or PLM were treated as per clinical standard of care.
The psychosocial and sleep questionnaire battery was completed by 60 children and their parents/guardians at the time of the initial sleep consultation. Based on the questionnaires, both girls and boys diagnosed with NREM parasomnia were observed to report increased symptoms of depression and fatigue based on established cutoff scores for the CES-DC (Faulstich et al. 1986) and fatigue severity scales (Krupp et al. 1989) (Table 4). The frequency distribution of the CES-DC scores presented in Figure 1 demonstrates that a large proportion (n = 31, 53%) of the children scored above the cutoff of 15 (Faulstich et al. 1986) for this scale; this elevated score is indicative of symptoms of depressed mood.
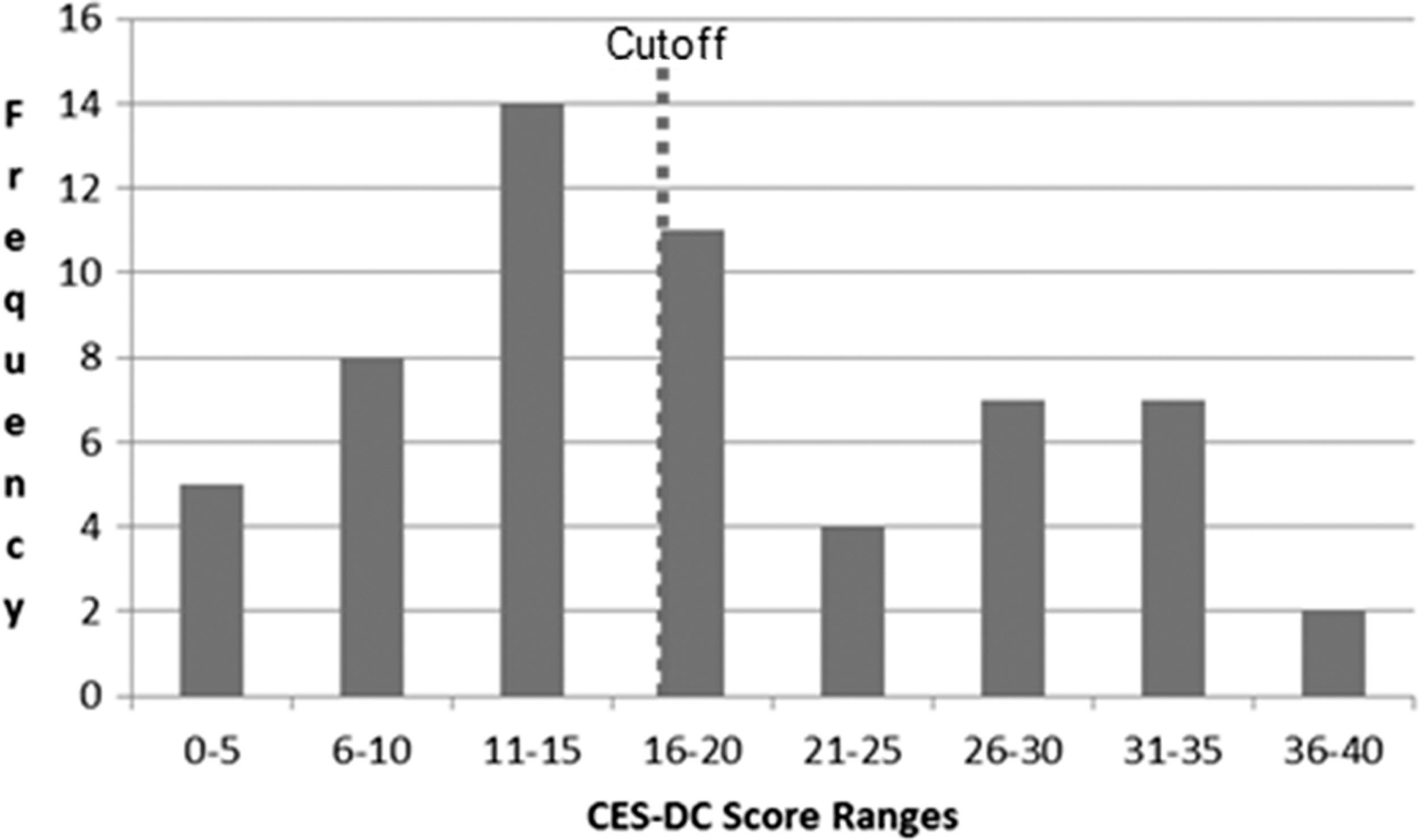
Range and frequencies of CES-DC scores. The ranges of the CES-DC scores are presented on the x-axis and the frequency distribution is presented on the y-axis. The dashed vertical line signifies the cutoff (>15) for the CES-DC. CES-DC, Centre for Epidemiologic Studies in Depression–children's version.
Indicates questionnaire scores that exceed the cutoff values.
PDSS, pediatric daytime sleepiness scale; FSS, fatigue severity scale; CES-DC, Centre for Epidemiologic Studies in depression–children's version; SNAP-IV, SNAP-IV teacher and parent rating scale for ADHD symptoms.
Discussion
Although NREM parasomnias are a significant problem for adults, such as leading to poor sleep and a greater risk of self-injury (Zadra and Pilon 2011), NREM parasomnias have hereto been viewed as benign in children (Kotagal and Chopra 2012; Pelayo and Yuen 2012). To the contrary, the sleep architectural changes noted in the children with parasomnias in this study indicate more problematic sleep compared with that of normal children. Furthermore, Li et al. (2008) have demonstrated that parasomnias in children are significantly and positively associated with a greater risk of accidental injury to the child. Perhaps of even greater importance, parasomnias in children have been linked to learning difficulties, behavioral disturbances, increased rates of physical illness, delayed toilet training, adjustment problems, and greater sleep fragmentation (Herrera et al. 2006).
Therefore, although most cases of childhood NREM parasomnias may currently be viewed as being benign, the available evidence would suggest otherwise. The abovementioned issues (Herrera et al. 2006) may impact negatively on a child's educational potential with irreversible long-term consequences regarding career prospects and eventual overall integration into the community.
The findings of this study substantiate that parasomnias in children are not benign. The majority of children in our study had disturbed sleep architecture; this finding contrasts with previous reports that parasomnias have no deleterious impact on sleep quality or duration (Petit et al. 2007). For some children, parasomnias were seen in association with another sleep disorder. Furthermore, questionnaire assessment revealed symptoms of depression and fatigue among children with parasomnias. The latter observation concurs with a recent study documenting the functional impairment in adults with NREM parasomnias (Lopez et al. 2013).
The retrospective nature of this study cannot determine causation, and the lack of an age- and gender-matched control group limits generalizability of the study, but our findings still suggest that sleep architecture is disrupted in most children with parasomnias. The strong association between disturbed sleep and poor academic performance and problem behaviors in children has been well documented in the literature (Gruber et al. 2012b). Given that these formative years of childhood are particularly crucial for social and academic learning, physicians need to reconsider withholding a largely innocuous treatment for a disorder that can disrupt cognitive and intellectual development, particularly if that disorder leads to difficulties at school or home, or persists into adolescence.
This study supports the standard guidelines (Aurora et al. 2012) and recommendations (Kotagal and Chopra 2012) that children with NREM parasomnias be screened for comorbid sleep disorders, particularly OSA and PLMS, but may be taken to raise the issue of whether a more rigorous approach to the investigation of parasomnias in children needs to be taken. Intellectual and learning issues have been reported in children with parasomnias, and poor sleep can mimic pediatric problems, including ADHD-like symptoms, academic difficulty, and problem behaviors (Goll and Shapiro 2006; Gruber et al. 2012b). Amelioration of sleep problems has been shown to improve quality of life, reduce problem behaviors, and improve attention and learning (Gruber et al. 2012a). Effectively controlling parasomnias may, therefore, potentially lead to an overall improvement in academic function and social behavior.
Overall, treatment with L-tryptophan led to parental reports of a reduction in symptoms of NREM parasomnia that was almost twice as much as that seen in children who were untreated. About 1 in 10 children had side effects (daytime sleepiness and/or fatigue) that led to the discontinuation of L-tryptophan. Our findings are in line with a study assessing the efficacy of L-5-hydroxytryptophan (2 mg/kg bedtime) for night terrors that reported a 1-month improvement in night terror symptoms in >90% of their 31 study patients, and this improvement persisted in the majority of patients past the 6-month mark (Bruni et al. 2004).
Our study employed L-tryptophan; 5-hydroxytryptophan that is the direct precursor of serotonin and an intermediate in the synthesis of melatonin, whereas L-tryptophan is the direct precursor of 5-hydroxytryptophan. One benefit of L-tryptophan over 5-hydroxytryptophan is that it is perceived as a more natural product and as such may be more acceptable to parents and caregivers. In addition, administration of 5-hydroxytryptophan may cause nausea and vomiting in children (Ryan et al. 1992); the article by Bruni et al. (2004) did not specifically mention any side effects, just that they were not severe enough to warrant a variation in the study schedule.
The action of L-tryptophan for the management of parasomnias in children remains to be elucidated and there is very little new literature on the pharmacotherapeutics of L-tryptophan for sleep. One possible mechanism of L-tryptophan action is by the reduction in arousals during sleep. L-tryptophan has demonstrated efficacy for the management of awakenings and middle insomnia in older individuals (Wyatt et al. 1970; Hartmann et al. 1983). Spinweber (1983) proposed that unlike sedating agents that result in carryover sleepiness and alter sleep architecture, L-tryptophan improves sleep not by inducing sleepiness but by “deactivation of the wake state.” Hence, there is an absence of side effects with long-term use of L-tryptophan at low doses, specifically, no CNS depression, no memory or concentration impairment, and no motor retardation (Linnoila et al. 1980). In addition, others have reported a lack of tolerance and sustained efficacy of L-tryptophan with long-term treatment (Steinberg et al. 1981).
L-tryptophan is a metabolic precursor in the serotonin pathway (Esteban et al. 2004). Serotonin plays an important role in the regulation of sleep (Dugovic 2001; Monti and Jantos 2008). Others have demonstrated that administration of 5-hydroxytryptophan improves sleep quality in those with insomnia by increasing the amount of REM sleep (Wyatt et al. 1971; Guilleminault et al. 1973; Soulairac and Lambinet 1977). Whether serotonin could have a direct effect on reducing parasomnias is not known. To the contrary, selective serotonin uptake inhibitors have been reported to cause bruxism (Wise 2001; Winocur et al. 2003).
Melatonin is metabolized from tryptophan through 5-hydroxytryptamine serotonin (Moore et al. 2000; Zheng et al. 2004) and dietary L-tryptophan has been shown to promote melatonin secretion at night (Fukushige et al. 2014). Melatonin is a chronobiotic regulating sleep–wake rhythms and not a sleep-promoting agent (Arendt and Skene 2005). However, there is a case report of melatonin being used to manage parasomnias in children (Ozcan and Donmez 2014); the exact mechanism of melatonin action in reducing parasomnias remains unclear.
The purpose of this study is to explore options and guide research on future pharmacologic management of parasomnias in children. A primary limitation is that L-tryptophan is not an FDA or Health Canada recognized treatment for the management of parasomnias or sleep disorders in children. To date, there is a lack of evidence-based studies demonstrating the safety and efficacy of L-tryptophan in children. Consequently, the study authors do not endorse over-the-counter administration of L-tryptophan to children. L-tryptophan should be administered to children only after thorough clinical assessment and solely under a physician's supervision. An incident such as the eosinophilia myalgia syndrome that occurred in the United States in 1989 (Mayeno and Gleich, 1994) as a result of impurities introduced during the fermentation process of a single manufacturer producing L-tryptophan emphasizes the need for strict monitoring to ensure the purity and safety of natural health products.
A second limitation of this study is that there is a wide range of parasomnias, each with their own psychopathology and consequence. That is, some parasomnias such as night terrors may be more psychologically distressing to children, whereas other parasomnias such as bruxism may have more of a physical impact. This study only looked at frequency of occurrences and did not specifically examine the baseline symptoms in each child and whether there was a difference in the intensity (mental or physical) of that symptom. Another limitation is the large percentage (40%) of children lost to follow-up. However, this is a naturalistic study conducted in a pediatric sleep clinic in a large urban center where due to the large catchment area, such a large loss to follow-up is not uncommon.
Lastly, parents/guardians who reported that their children/wards stopped taking L-tryptophan due to side effects of sleepiness or fatigue were invited to attend a follow-up clinical appointment but the details of the side effects were not explored in any detail in this research study.
Conclusions
This article has detailed the negative impact of untreated parasomnia in children and adolescents. There is no primary treatment indication to address parasomnias in the pediatric population and this article provides preliminary evidence that L-tryptophan is an effective and safe medication to manage pediatric parasomnia. Given the positive findings of this study, the next step needs to be a well-designed, randomized, placebo-controlled investigation of the treatment efficacy of L-tryptophan versus placebo for treatment of parasomnias in children and adolescents. Such a study will also be required to allow for a systematic assessment of side effects and should also incorporate a thorough assessment of mood and daytime symptoms, including measures of daytime functioning.
The major contribution of this article is to describe for the first time a safe and effective treatment for parasomnias in children and the marshalling of evidence that parasomnias in children are not trivial. However, this study is not without limitations. Follow-up clinical sleep assessments were not conducted and the study relied on parents' reports of outcome in their children. In addition, the retrospective nature of this study does not allow for any exploration of cause or effect, merely association.
Clinical Significance
Parasomnias are a common occurrence in children, but most pharmacological treatments for parasomnia have been investigated only in adults. This article proposes that L-tryptophan is safe and effective for the management of parasomnias in children.
Footnotes
Acknowledgments
The authors received no external funding to conduct this study. The authors' time was paid for by the following institutions: Youthdale Treatment Centres, the Youthdale Child and Adolescent Sleep Centre, and the University Health Network.
Dr. Chung served as the statistical expert for this research.
Disclosures
Drs. van Zyl and Shapiro are shareholders in the company, ZeeMag. ZeeMag has applied for a patent for L-tryptophan as a treatment for NREM parasomnia.
Drs. Chung and Shahid have no conflicts of interest to report.