
Abstract
Background:
Monitoring “real world” dispensation patterns over time is important to build the evidence base for safe and efficient use of psychotropic drugs. In this study, we aimed to comprehensively examine the patterns of psychotropic drug dispensations in patients with Tourette and chronic tic disorders (TD/CTD) in Sweden between 2005 and 2013.
Methods:
A cohort of 6979 TD/CTD patients was identified through the Swedish National Patient Register. Their drug dispensation patterns, collected in the Swedish Prescribed Drug Register, were examined between July 1, 2005 and December 31, 2013. Frequencies of drug dispensations were further stratified by gender and comorbidities. Additionally, differences in the patterns of dispensation in children and adolescents versus adults in the last year of the follow-up were examined, as well as the time trends of the dispensations over the 8-year study period.
Results:
A total of 5299 (75.9%) TD/CTD patients were dispensed at least one drug during the study period. The most frequently dispensed medications were attention-deficit/hyperactivity disorder (ADHD) drugs (53.8%), antidepressants (50.7%), hypnotics/sedatives (41.7%), and antipsychotics (41.5%). Most of the medicated patients (72.1%) were dispensed more than one drug during the study period. Patterns of dispensation varied according to patient's gender, associated comorbidities, and age group. Dispensation of quetiapine and aripiprazole, antiadrenergics, ADHD drugs, antiepileptics, and hypnotics/sedatives and anxiolytics (particularly the nonbenzodiazepine types) significantly increased over time, whereas dispensation of antidepressants, typical antipsychotics, and benzodiazepine-based anxiolytics significantly decreased over the study period.
Conclusions:
Long-term monitoring of these drug dispensation patterns and the study of both their beneficial and adverse effects is warranted.
Introduction
T
Treatment strategies for TD/CTD may differ depending on the impairment associated with the tics and the presence of comorbid conditions (Debes et al. 2010). Mild cases with low levels of impairment may benefit from a “wait and see” strategy, psychoeducation, and reassurance (Murphy et al. 2013). However, in cases with more severe levels of impairment, an active intervention should be considered (Roessner et al. 2011). Evidence-based interventions for the treatment of TD/CTD include both behavior therapy and pharmacological treatment (Hollis et al. 2016).
Drug trials in TD/CTD are scarce, based on small sample sizes, have generally short-term follow-up periods (Farag et al. 2015), and rarely account for the presence of comorbidities (Whittington et al. 2016). Consequently, current clinical guidelines for TD/CTD are mainly based on expert consensus rather than on rigorous controlled treatment studies (Müller-Vahl and Roessner 2011; Roessner et al. 2011; Verdellen et al. 2011; Pringsheim et al. 2012; Steeves et al. 2012; Murphy et al. 2013). This leads to a lack of consistency across different treatment guidelines, especially regarding pharmacological treatments. For example, while the European clinical guidelines (Roessner et al. 2011) recommend risperidone as first-line treatment, followed by clonidine and aripiprazole, the Canadian guidelines (Pringsheim et al. 2012) recommend clonidine and guanfacine as first treatment options, and the German guidelines (Rothenberger et al. 2007) recommend sulpiride and tiapride. The Food and Drug Administration (FDA) in the United States (US) has to date only approved haloperidol (Shapiro et al. 1989), pimozide (Shapiro and Shapiro 1984), and aripiprazole (Sallee et al. 2017) for the treatment of tic disorders. In Sweden, clinicians are encouraged to follow the recommendations by the European guidelines (Roessner et al. 2011), but only haloperidol is approved for the treatment of tic disorders (Andrén 2017).
In an attempt to understand the prescription practices for CTDs in the “real world,” a handful of studies have previously evaluated use of psychotropic medication in children and adolescents with TD/CTD. In a Danish clinical cohort of 314 children and adolescents with TD, 60.5% had received pharmacological treatment, mainly methylphenidate (61%) and risperidone (29.5%). Additionally, clonidine, pimozide, and serotonin reuptake inhibitors (SRIs) were prescribed in about 20% of the children (Debes et al. 2009). Farag et al. (2015) examined the prescribing patterns of 400 TD patients seen over a 10-year period in a specialized clinic in the United Kingdom. The most frequently used drugs were aripiprazole (64%), clonidine (40%), risperidone (30%), sulpiride (29%), and haloperidol (20%).
Bachmann et al. (2015) studied the psychopharmacological prescriptions of 7058 children and adolescents with tic disorders for the years 2006 and 2011 in the largest German health insurance fund. Of these, 1499 (21%) had at least one prescription of psychotropic medication in 2011, although this percentage was age related and increased from 4.9% in individuals 0–4 years of age to 36.6% in15–19 years of age. The highest frequency of prescription was found in TD (52% in 2006 and 53% in 2011). ADHD drugs (methylphenidate and atomoxetine) were the most prescribed medications, followed by antipsychotics. In 2011, prescriptions of atypical antipsychotics were higher and prescriptions of typical antipsychotics were lower than in 2006.
Olfson et al. (2011) examined the use of medication in tic disorders over the course of 1 year in privately and publicly insured youth from the U.S. population. The results showed that the privately insured group of patients was mainly treated with antiadrenergic agents (36%), followed by antidepressants (35%), antipsychotics (33%), and psychostimulants (32%), whereas in the publicly insured group, antipsychotics were the most commonly prescribed medication (54%). However, most of these previous studies employed retrospective data from medical charts, had short follow-up times, or focused on specific populations (e.g., only children and adolescents).
This Swedish population-based study aimed to prospectively investigate the patterns of psychotropic drug dispensations in children and adults with TD/CTD during a period of 8 years. As a secondary aim, we also examined the influence of gender, comorbidities, age group, and time trends in the dispensation patterns of this group. Monitoring of such “real-world” dispensation practices over time is vitally important to build the evidence base for safe and efficient use of psychotropic drugs.
Methods
The study was approved by the Regional Ethics Review Board in Stockholm (2013/862-31/5). The requirement for informed consent was waived because the study was register based and the included individuals were not identifiable at any time.
Swedish national registers
Using the unique national identification numbers assigned to Swedish citizens as key and recoded for anonymity (Ludvigsson et al. 2009), we linked several Swedish population-based registers. The Total Population Register contains demographic information on individuals registered as Swedish inhabitants. The National Patient Register (NPR) comprises information on all inpatient care (from 1969) and outpatient specialist services (from 2001) in Sweden. Diagnoses in the NPR are based on the International Classification of Diseases (ICD), eighth (ICD-8; 1969–1986), ninth (ICD-9; 1987–1996), and tenth (ICD-10; 1997–2013) revisions. The Prescribed Drug Register (PDR) was introduced in July 2005 and includes a record for all medications dispensed in Sweden (registered using Anatomical Therapeutic Chemical [ATC] codes) and the corresponding dosage. The PDR has full coverage of the Swedish population. The Cause of Death Register and the Migration Register were used to exclude those individuals who were not alive or had emigrated from Sweden during the study period.
Patient cohort
Patients with a diagnosis of TD or CTD (ICD-8 code 306.2; ICD-9 code 307C; ICD-10 codes F95.0 [transient tic disorder], F95.1 [chronic motor or vocal tic disorder], F95.2 [TD], F95.8 [other tic disorders], or F95.9 [unspecified tic disorder]) between January 1, 1969 and December 31, 2013 were identified from the NPR. A previously validated algorithm, described in detail in Rück et al. (2015) was used. This approach results in nearly perfect interrater reliability and highly valid diagnoses.
Identified individuals with a diagnosis of TD/CTD who were living in Sweden during the period July 1, 2005 and December 31, 2013 were included in the study. Lifetime comorbid diagnoses of ADHD, OCD, PDD, depressive, anxiety, conduct, and nonorganic sleep disorders were identified. We excluded patients who had a lifetime diagnosis of any of the following comorbid conditions that may confound the usual patterns of prescription in TD/CTD: organic mental disorders, epilepsy, schizophrenia spectrum disorders, or bipolar disorder. ICD codes of the included and excluded comorbidities are shown in Supplementary Table S1 (Supplementary Data are available online at
Drug dispensation outcomes
Drugs affecting the central nervous system were identified from the PDR according to the ATC classification system (codes N01-07) and included ADHD drugs, antidepressants, antipsychotics, anxiolytics, hypnotics/sedatives, antiadrenergic agents, antiepileptics, anesthetics, analgesics, antiparkinson drugs, and other nervous system drugs (ATC codes are listed in Supplementary Table S2).
Statistical analyses
Analyses were primarily descriptive (i.e., counts of different classes of drugs according to their ATC codes during the study period). Frequencies of drug dispensations were further stratified by gender and comorbidities. Examining the role of comorbid disorders in the dispensation patterns was particularly relevant since the PDR does not specify the indication of the drugs dispensed. Additionally, the dispensation patterns in children and adolescents (<18 years) versus adults (≥18 years) in the last year of the follow-up (2013) were examined. Individuals turning 18 in 2013 were left out to allow for mutually exclusive age groups. Results were expressed as odds ratios (ORs) and 95% confidence intervals (CI).
Annual trends of the dispensation patterns were examined for each year from 2006 to 2013. Data from 2005 were not analyzed, as PDR covers only 6 months in 2005. The relative change (RC) is reported in percentages, with positive values corresponding to over time increases and negative values corresponding to decreases. Cochran–Armitage tests for trend were used to assess whether there was a trend in annual prevalence or proportions of each class of medication across time, with two-sided p-value <0.05 supporting the trend hypothesis.
Results
Study cohort
A total of 7889 TD/CTD cases were identified in the period from January 1, 1969 to December 31, 2013, of which 910 were excluded due to the comorbidities listed above. Of the final 6979 included patients, 77.3% (n = 5397) were male. A large majority (n = 5702; 81.7%) had at least one lifetime comorbid diagnosis (Supplementary Table S3).
Drug dispensation patterns in TD/CTD
The majority of TD/CTD patients (n = 5299; 75.9%) were dispensed at least one drug during the study period (July 1, 2005 to December 31, 2013). Medicated (n = 5299) and unmedicated (n = 1680) individuals had a similar gender distribution (77.34% vs. 77.32% of men, respectively; Chi-square = 0.0001, p = 0.9905). Compared with unmedicated individuals, medicated individuals were older (64.89% vs. 46.16% of patients older than 18 at the end of the follow-up, respectively; Chi-square = 173.56, p < 0.0001) and had a higher percentage of any psychiatric comorbidity (81.68% vs. 30.18%, respectively; Chi-square = 1589.43, p < 0.0001).
Among the 5299 medicated TD/CTD cases, the most frequently dispensed medications were ADHD drugs (53.8%), antidepressants (50.7%), hypnotics/sedatives (41.7%), and antipsychotics (41.5%). Other commonly dispensed drugs were anxiolytics (36.5%), analgesics (33.3%), antiepileptics (13.5%), other nervous system drugs (5.2%), anesthetics (5.1%), antiparkinson drugs (3.6%), and antiadrenergic agents (3.4%; Table 1).
The sum of percentages exceeds 100% because most patients were on more than one class of drugs during the study period.
SNRI, serotonin–norepinephrine reuptake inhibitors; SRI, serotonin reuptake inhibitors; TD, Tourette disorder; CTD, chronic tic disorder.
Gender
The same proportion of males and females (75.9%) were dispensed medications during the study period (4098 of 5397 males, 1201 of 1582 females). However, the dispensation patterns were different according to the gender. ADHD were more likely to be dispensed to males, compared with females (OR = 0.52). Conversely, females were more likely than males to be dispensed analgesics (OR = 1.93), all groups of antidepressants (OR = 1.74), anxiolytics (OR = 1.72), benzodiazepine-based hypnotics (OR = 1.77), antiepileptics (OR = 1.54), anesthetics (OR = 1.53), and antiparkinson drugs (OR = 1.54). Additionally, females were also more likely to be dispensed certain antipsychotics, such as typical antipsychotics (OR = 1.45), quetiapine (OR = 1.33), and aripiprazole (OR = 1.28; Table 2).
Significant ORs are highlighted in bold.
Males are the reference category.
Selective serotonin reuptake inhibitors (SSRIs) and clomipramine.
Venlafaxine and duloxetine.
Antidepressants other than SRIs or SRNIs.
CI, confidence interval; OR, odds ratio; SNRI, serotonin–norepinephrine reuptake inhibitors; SRI, serotonin reuptake inhibitors.
Comorbidities
The dispensation patterns for each group of comorbidities in the medicated individuals with TD/CTD are detailed in Supplementary Table S4.
As expected, individuals diagnosed with ADHD and/or PDD were more likely to be dispensed ADHD drugs, compared with those TD/CTD cases without these comorbidities (OR adjusted for sex [ORa] = 62.26 and ORa = 1.63, respectively).
Patients with comorbid anxiety disorders, depressive disorders, and OCD were more likely to get any type of antidepressants (ORa = 7.58, ORa = 11.24, and ORa = 6.74, respectively), anxiolytics (ORa = 5.31, ORa = 3.86, and ORa = 1.98, respectively), and atypical antipsychotics (ORa = 1.92, ORa = 1.83, and ORa = 2.11, respectively). These patients were also more likely to receive both nonbenzodiazepine and benzodiazepine-based anxiolytics and hypnotics/sedatives and antiepileptics.
TD/CTD patients with conduct disorders and nonorganic sleep disorders were more likely to receive ADHD drugs (ORa = 4.14 and ORa = 1.87, respectively), anxiolytics (ORa = 1.22 and ORa = 1.75, respectively), and hypnotics (ORa = 1.52 and ORa = 6.38, respectively), particularly the nonbenzodiazepine-based group.
Age group
During the year 2013, ADHD drugs (including methylphenidate and atomoxetine), antiadrenergic agents (including clonidine), and nonbenzodiazepine-based hypnotics were more likely to be dispensed to children and adolescents with TD/CTD, compared with the adults in the same cohort (OR = 0.13, OR = 0.16, and OR = 0.45, respectively; Table 3). On the other hand, antidepressants, antipsychotics (both typical and atypical), anxiolytics, benzodiazepine-based hypnotics, antiepileptics, analgesics, antiparkinson drugs, and other central nervous system drugs were more likely to be dispensed in adults, compared with the pediatric group (Table 3). There were no differences in the dispensation of the broader group of hypnotics/sedatives, anesthetics, and some specific atypical antipsychotics, namely aripiprazole and olanzapine.
Significant ORs are highlighted in bold.
Individuals who were younger than 18 during 2013 were classified as children and adolescents, whereas those who were 18 or older during 2013 were classified as adults. Individuals turning 18 during 2013 were excluded from these analyses.
Adjusted for gender. Children and adolescents is the reference category.
CI, confidence interval; OR, odds ratio; SNRI, serotonin–norepinephrine reuptake inhibitors; SRI, serotonin reuptake inhibitors.
Polypharmacy
The majority of TD/CTD patients that were on medication were dispensed more than one drug during the study period (n = 3822, 72.1%; Fig. 1). Among those that were dispensed only one medication, ADHD drugs were the most dispensed (41.6%), followed by analgesics (20.4%), antidepressants (13.1%), antipsychotics (11.9%), and other drugs (12.9%). The group of other drugs included anxiolytics, hypnotics/sedatives, anesthetics, antiadrenergic agents, antiepileptics, and other central nervous system drugs, and all of them were dispensed to less than 5% of the medicated individuals. Among those patients that were dispensed multiple drugs, the most common combination was the dispensation of ADHD drugs and hypnotics/sedatives (19.5% of the medicated patients), followed by ADHD drugs and antipsychotics (11.8% of the medicated patients).
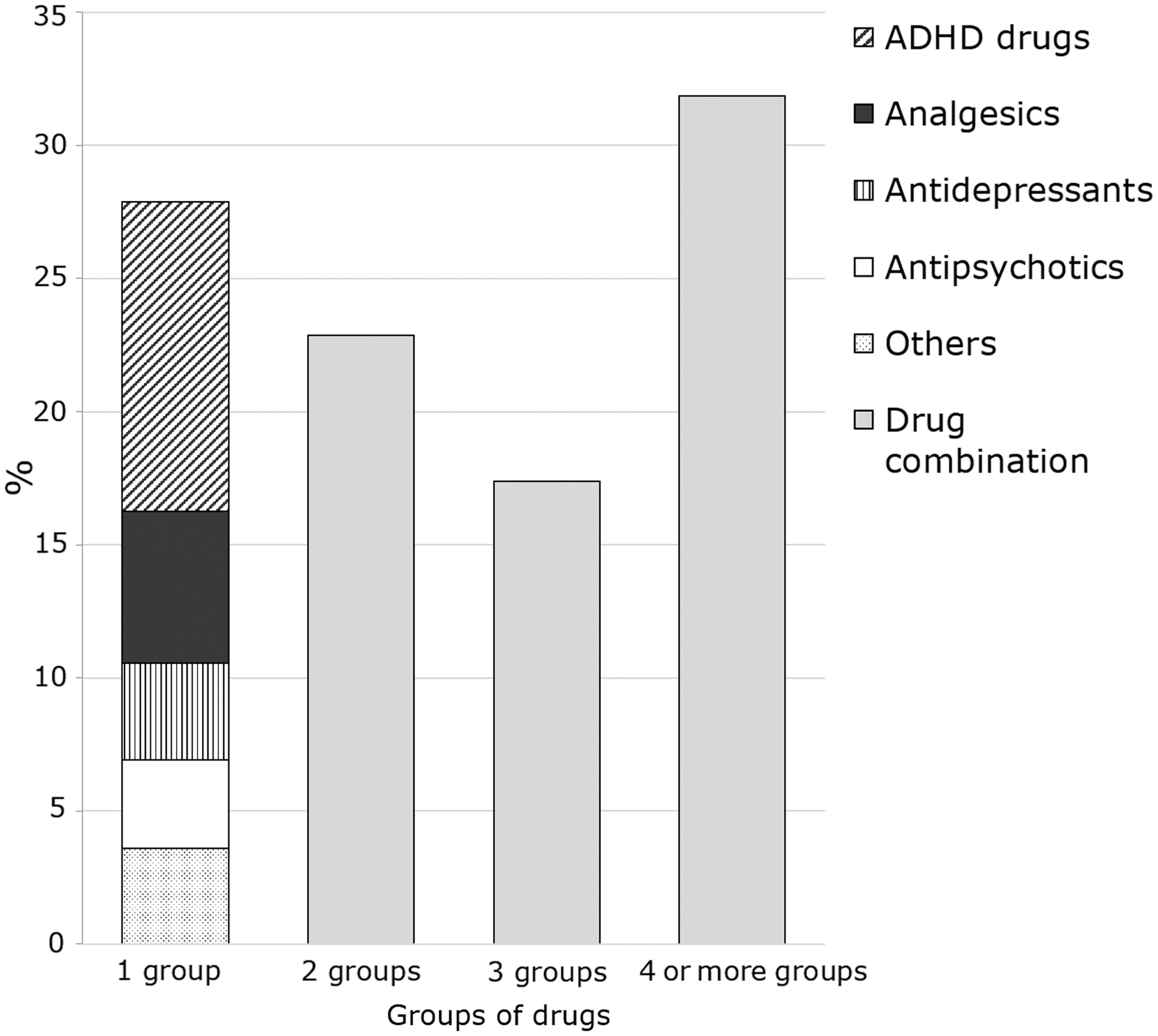
Percentage of medicated individuals with Tourette/chronic tic disorders that were dispensed one, two, three, or four or more groups of drugs during the 8-year study period (July 1, 2005 to December 31, 2013). For those that were on only one group of drugs, the medication is specified.
Time trends
Dispensation of some atypical antipsychotics significantly increased over time (RC for quetiapine = 227.8%; RC for aripiprazole = 167.2%). A significant increase was also noticeable for antiadrenergics (RC = 81.3%); ADHD drugs (RC = 51.1%); hypnotics/sedatives and anxiolytics, particularly the nonbenzodiazepine-based types (RC = 70.5% and RC = 29.3%, respectively); antiepileptics (RC = 26.5%); and antidepressants other than SRIs or serotonin–norepinephrine reuptake inhibitors (SNRIs) (RC = 12.9%). Conversely, dispensation of antidepressants, particularly SRIs and SNRIs, antipsychotics, particularly typical, but also some atypical such as ziprasidone or risperidone, benzodiazepine-based anxiolytics, anesthetics, and other central nervous system drugs decreased over the study period (Table 4).
Significant relative changes are highlighted in bold.
Discussion
This pharmacoepidemiological study provides a picture of the “real world” dispensation patterns in children and adults with TD/CTD at the Swedish national level during an 8-year study period. Out of a sample of almost 7000 TD/CTD patients, three quarters were dispensed at least one drug during the study period. Importantly, most of the medicated patients (72.1%) were dispensed more than one drug during the study period.
Consistent with typical specialist clinic-based samples and previous pharmacoepidemiological studies (Debes et al. 2009; Olfson et al. 2011; Bachmann et al. 2015; Farag et al. 2015), a large majority of patients had at least one lifetime comorbidity (81.7%), ADHD being the most common (46.7% of TD/CTD patients). In line with this, the most commonly dispensed medications were ADHD drugs. The second most dispensed drugs were antidepressants–also unsurprising given the rates of comorbidity with anxiety disorders, depressive disorders, and OCD. Antipsychotics (mainly atypical) and antiadrenergic drugs, which are the main evidenced-based pharmacological treatments for tic disorders, were dispensed to 41.5% (37.9% for atypical, 11.2% for typical) and 3.4% of the medicated patients, respectively.
These percentages are similar to those found in two previous European pharmacoepidemiological studies (Debes et al. 2009; Bachmann et al. 2015), including the high dispensation of ADHD drugs and the low dispensation of antiadrenergics. Conversely, Farag et al. (2015) found clonidine to be the second most prescribed medication (60%) in their 2015 study in the United Kingdom, and Olfson et al. (2011) found antiadrenergics to be the first prescribed treatment for TD among privately insured patients (36%) and the second among publically insured patients (42%) in the United States. Recent studies (Murphy et al. 2013; Whittington et al. 2016) recommend antiadrenergics as first-line medication for tics in TD, especially in younger populations. The balance between clinical benefits and adverse effects favors antiadrenergic drugs over atypical antipsychotics, which are considered as a second option due to the risk of metabolic effects and tardive dyskinesia (Pena et al. 2011).
The reasons for the low dispensation rates of antiadrenergics in our sample could be related to the lack of consensus between guidelines (i.e., Canadian and U.S. guidelines recommend antiadrenergics, whereas European guidelines recommend antipsychotics as first-line treatments for tics), the off-label use of these drugs in TD/CTD patients without ADHD (i.e., guanfacine and clonidine are only indicated for patients diagnosed with ADHD), and differences across countries in the approval of these drugs (i.e., guanfacine was only approved for the treatment of ADHD in Sweden in 2016; Huss et al. 2016). Additionally, a handful of studies have not supported the efficacy of antiadrenergics in tic disorders (Murphy et al. 2017) or have shown efficacy only in TD/CTD individuals with comorbid ADHD (Weisman et al. 2013), which may also contribute to the heterogeneous pattern of prescription of these drugs across countries and studies and probably the lack of approval by the FDA for TD/CTD.
Our results showed that females, compared with males, were more likely to be dispensed drugs from any group, except for ADHD drugs, which were more dispensed among males, in line with the gender distribution of the disorder. The reasons for this are unclear, but it may be that the diagnostic threshold for diagnosing tic disorders in girls is particularly high, resulting in an overrepresentation of severe or complex female patients in our cohort.
As expected, ADHD drugs were more likely to be dispensed to patients with comorbid ADHD, conduct disorders, and sleep disorders, conditions which tend to co-occur. Methylphenidate, the most dispensed drug in our cohort (48.3% of the medicated patients) has shown to be efficacious and safe to treat ADHD, also when appearing with conduct disorders (Sinzig et al. 2007), with or without TD/CTD (Cohen et al. 2015; Ganos et al. 2017). A large percentage of TD/CTD patients also received antidepressants, anxiolytics, and hypnotics/sedatives, particularly females and those with comorbid anxiety, depression, sleep disorders, and OCD. These findings are consistent with pharmacoepidemiological studies of other psychiatric disorders, such as OCD. For example, Isomura et al. (2016) found that OCD patients with psychiatric comorbidities had between three- and five-fold increased odds of dispensation of other classes of drugs in addition to the evidence-based treatments for OCD (SRIs).
Regarding the time trends, we found that the dispensation of some atypical antipsychotics (quetiapine and aripiprazole) increased over time, in line with other studies (Bachmann et al. 2015; Halfdanarson et al. 2017). In turn, typical and some atypical antipsychotics (ziprasidone and risperidone) decreased over time, probably due to their worse profile and tolerability compared with the newer atypical antipsychotics. In line with the anti-benzodiazepine campaigns developed in Scandinavian countries aiming at decreasing the overprescription of these drugs due to their potential risk of chronic use (Clay et al. 2013), we found a decrease in prescriptions of benzodiazepine-based drugs and an increase in nonbenzodiazepine-based hypnotics/sedatives and anxiolytics. Dispensation of ADHD drugs also increased by over 50% over time. Contrary to the study by Bachmann et al. (2015), dispensation of antidepressants decreased over the study period.
Most patients (72.1%) were dispensed more than one drug during the study period and up to one third of the cohort received four or more groups of drugs. This pattern, consistent with previous research (Farag et al. 2015), may reflect the high complexity in the management of tic disorders, partly due to the high rates of comorbidity, given that combination and augmentation strategies are often required according to which primary symptom is being treated (Robertson 2000). Additionally, TD/CTD patients appear refractory to many treatments and idiosyncratic responses are frequently found (Farag et al. 2015). Nevertheless, the results may also reflect the lack of uniform prescription practices and highlights the need for more evidence-based treatment-controlled studies. Finally, the high rates of dispensed drugs in patients with TD/CTD may be associated with the limited availability of behavioral therapy in clinical settings (Whittington et al. 2016; Ganos et al. 2017).
The strengths of this study include the use of the world's largest population-based cohort of patients with TD/CTD of all ages, the full population coverage of all drug dispensations, and the relatively long follow-up study period, which allowed us to examine time trends at a national level. Additionally, the diagnostic validity and reliability of the TD/CTD diagnoses in the Swedish national registers is high (Rück et al. 2015).
However, this study is not without limitations. The main limitation is that the Swedish PDR does not contain information regarding the indication of each dispensation, meaning that it is not known whether the dispensed drugs have been prescribed for the treatment of tics or for a comorbid condition. To minimize this problem, we excluded patients with lifetime diagnosis of organic mental disorders, schizophrenia spectrum disorders, bipolar disorder, or epilepsy, conditions that may mask the usual patterns of prescription in TD/CTD.
Additionally, our definition of polypharmacy did not allow to establish with certainty whether the drugs dispensed during the 8-year study period were taken concurrently or sequentially. Another possible limitation is that our cohort does not represent the totality of all TD/CTD patients in Sweden. This is because many sufferers may not seek help, the incomplete coverage of the register until 2001, and those patients diagnosed by general practitioners and other nonspecialists are not included. Thus, while the patients included in our cohort resemble other patients recruited from specialist tic disorder clinics around the world, it is possible that our results do not generalize to less complex patient samples. Our analyses are based on dispensation data and, thus, we cannot be certain that prescriptions that were collected were actually used. Finally, Swedish registers do not contain information of nonpharmacological treatments.
Conclusions
Over three-quarters of patients with TD/CTD in Swedish specialist settings, received at least one type of medication during the study period and, of those, over 70% received multiple classes of drugs over a period of 8 years. A range of clinical variables, notably psychiatric comorbidity, influence what classes of drugs are dispensed to this patient group, in line with the widely held view that comorbidities are often more problematic for the patients than the tics themselves.
Clinical Significance
Long-term monitoring of the drug dispensation patterns in patients with TD/CTD is warranted as is the systematic study of both their potentially beneficial and adverse effects.
Footnotes
Acknowledgments
This research is funded by grants from the Stockholm County Council. Dr. Marta Carulla-Roig was funded by the Alicia Koplowitz Foundation.
Disclosures
Prof. Mataix-Cols and Dr. Fernández de la Cruz receive royalties for contributing articles to UpToDate, Wolters Kluwer Health. Prof. Hellner has served as a speaker for Shire and has received a grant from the research foundation of Svenska Spel (the state owned gambling company in Sweden). Prof. Larsson has served as a speaker for Eli-Lilly and Shire and has received research grants from Shire. The other authors report no financial relationships with commercial interests.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.