
Abstract
Objective:
Fluoxetine is an effective and well-tolerated pharmacological treatment for children and adolescents with major depressive disorder (MDD). However, a high percentage of patients do not respond. There is a substantial genetic contribution to this variable clinical outcome. Based on previous genetic results of our group and given the lack of pharmacogenetics studies of antidepressant response with a long follow-up period, we evaluated the influence of single nucleotide polymorphisms (SNPs) in genes related to the serotonergic pathway on remission and recovery in children and adolescents diagnosed with MDD after 12 months of initiating fluoxetine treatment.
Methods:
The assessment was performed in 46 patients. All of them were visited at least once a month during the 12-month follow-up. Psychiatrists interviewed patients and their parents to explore clinical improvement. A total of 75 genotyped SNPs in 10 candidate genes were included in the genetic association analysis with remission and recovery. Bonferroni correction for multiple testing was applied to avoid false positive results.
Results:
The HTR2A rs7997012 SNP was significantly associated after Bonferroni correction with clinical improvement. Particularly, the homozygotes for the major allele (GG) showed the highest percentage of remitters and the highest score reductions on the Clinical Global Impressions-Severity (CGI-S) scale. Moreover, although the results were on the border of statistical significance, the GG homozygotes also tended to experience fewer readmissions during the follow-up period
Conclusions:
These results provide more evidence of the involvement of genetic variants related to the serotonergic pathway in the antidepressant response. Studies with larger cohorts are needed to integrate all relevant variants into clinical predictors of antidepressant response.
Introduction
M
Together with psychological treatment, antidepressants are widely used in young populations in which the rate of prescription has increased over time (Bachmann et al. 2016). Fluoxetine is currently the only selective serotonin reuptake inhibitor (SSRI) approved by the European Medicines Agency for the treatment of MDD in children above the age of 8 and in whom psychological treatment has not been effective (Kratochvil et al. 2006; Hetrick et al. 2007). Fluoxetine has been shown to be effective and well tolerated for the long-term treatment of MDD in children and adolescents (Emslie et al. 2004; TADS 2009).
However, there is important interindividual variability in clinical responses to antidepressants and a high percentage of patients, some 30%–40%, do not respond to the pharmacological treatment (Kato and Serreti 2010). In this scenario, the prediction of clinical outcomes is needed to achieve better improvement and prognosis through individualized treatment. Unquestionably, there is a substantial genetic contribution to antidepressant response. In fact, common variants across the human genome were estimated to explain 42% of individual differences in clinical response to antidepressants (Tansey et al. 2013).
There has been significant pharmacogenetics research into MDD in recent years (Kato and Serretti 2010; Niitsu et al. 2013; Fabbri et al. 2016). Although findings are encouraging, they are highly inconsistent, mainly due to differences between studies in terms of many important variables such as ethnicity, age, diagnosis, antidepressant treatment, or clinical outcome measurement, which is a common weakness in the pharmacogenetics field. However, genetically guided prescribing of antidepressants is promising and has the potential to reduce a trial-and-error clinical strategy and improve patient outcomes (Singh and Bousman 2017). In fact, there are already some commercial antidepressant pharmacogenetics tests available, based on results from candidate gene studies. Although some industry-sponsored clinical trials have been completed with positive results, more randomized controlled trials will be necessary to confirm the real usefulness of such testing (Fabbri et al. 2016; Singh and Bousman 2017).
Bearing this in mind, candidate gene studies are still needed to provide evidence of the most relevant variants involved in clinical response, especially in children and adolescents as pharmacogenetics studies of antidepressants are scarce in these populations (Blázquez et al. 2012). In previous studies of our group, in which polymorphisms present in genes related to the pharmacokinetics of fluoxetine were evaluated, CYP2D6 polymorphisms were associated with the plasma fluoxetine/norfluoxetine ratio, but not with clinical improvement (Gassó et al. 2014). These results were consistent with the fact that fluoxetine plasma levels do not determine clinical response (Blázquez et al. 2014). At the pharmacokinetics level, only genetic variants in ABCB1, which could determine fluoxetine brain bioavailability, appears to play a role in clinical response after 12 weeks of fluoxetine treatment (Gassó et al. 2014).
At the pharmacodynamics level, we assessed a wide range of candidate genes related to different pathways and only genetic markers directly related to serotonin were associated with antidepressant response in child and adolescent patients (Mas et al. 2016). There are many other evidences of the significant impact of genetic variability in the serotonergic system on both adolescent depression (Xia and Yao 2015) and the response to antidepressant drugs (Porcelli et al. 2011; Helton and Lohoff 2015). Particularly, we found that genetic and epigenetic variants in the 5-hydroxytryptamine receptor 1B (HTR1B) and tryptophan 5-hydroxylase 2 (TPH2) genes were associated with clinical improvement after a 12-week fluoxetine treatment in children and adolescents with different psychiatric diagnoses (Mas et al. 2016; Gassó et al. 2017a, 2017b).
Interestingly, we also prospectively followed up those patients with MDD for 12 months, to assess remission and recovery rates 1 year after the index episode (Blázquez et al. 2016). Our results showed that around 30% of patients did not remit and more than 40% did not recover. Based on our previous genetic results and given the lack of pharmacogenetics studies of antidepressant response with a long follow-up period, the aim of this study was to evaluate the influence of polymorphisms in nine genes related to the serotonergic pathway on remission and recovery after fluoxetine treatment in children and adolescents diagnosed with MDD, after a 12-month prospective follow-up.
Methods
Patients and clinical assessment
A total of 83 children and adolescents aged between 10 and 17 years of age receiving fluoxetine treatment for the first time were recruited in the Child and Adolescent Psychiatry and Psychology Service of the Institute of Neuroscience at the Hospital Clinic in Barcelona. Patients and their parents were interviewed using the Spanish version (Ulloa et al. 2006) of the semi-structured diagnostic interview K-SADS-PL (Schedule for Affective Disorders and Schizophrenia for School-Age Children-Present and Lifetime Version) (Kaufman et al. 1997), with the aim of assessing current and past psychopathology.
The patients were diagnosed with MDD, obsessive compulsive disorder, or generalized anxiety disorder (GAD), according to the Diagnostic and Statistical Manual of Mental Disorders-IV (DSM-IV) (American Psychiatric Association 1994) and have been included in previous studies by our group (Blázquez et al. 2014; Gassó et al. 2014, 2017a; Mas et al. 2016; Gassó et al. 2017b). The present study is based on a 12-month prospective follow-up of those patients diagnosed with MDD who were treated with fluoxetine for at least 12 weeks (Blázquez et al. 2016). A total of 54 subjects met the inclusion criteria, but 8 refused to participate (the main reason being lack of contact with mental health services). So, a total of 46 patients were therefore included in the follow-up study.
All patients were visited at least once a month in the child and adolescent psychiatry and psychology service during the 12-month follow-up. Psychiatrists interviewed patients and their parents to explore the compliance to fluoxetine treatment, functioning and depressive symptoms of patients according to the DSM-IV diagnostic criteria for MDD (American Psychiatric Association 1994).
Patients were classified as remitters if they did not fulfill the criteria for MDD and achieved full functioning for at least 2 weeks as reported in medical records of the patient's monthly assessment during the 12-month follow-up period (Frank et al. 1991). Recovery was considered as full remission, which was defined as a period of at least 2 months in which patients did not fulfill the criteria for MDD and achieved full functioning (Frank et al. 1991). Recovery was determined at the end of the12-month follow-up according to medical records of the patient's monthly assessment and the K-SADS-PL interview administered to patients and their parents to assess the current diagnosis at 12 month. As proposed by Frank et al. (1991), individuals were classified as remitted or recovered patients independently of the pharmacological treatment they received.
Information on the severity of the illness was obtained at baseline, before initiating fluoxetine treatment, and after 12 months of follow-up, using different scales: the Children's Depression Inventory (CDI) (Kovacs 1992), the Clinical Global Impressions-Severity scale (CGI-S) (Guy 1976), and the Global Assessment of Functioning scale (GAF) (Luborsky 1962) or the Children's Global Assessment Scale (CGAS) (Shaffer et al. 1983). Data regarding number of readmissions (admissions in the inpatient unit) and suicide attempts were also collected.
The study was conducted in accordance with the Declaration of Helsinki and all the procedures were approved by the hospital's Ethics Committee (Approval Number: 2010/5823). Written informed consent was obtained from all parents and verbal informed consent was given by all subjects following an explanation of the procedures involved.
Sample preparation
Blood samples from participants were collected in EDTA (K2EDTA BD Vacutainer EDTA tubes; Becton Dickinson, Franklin Lakes, NJ). Genomic DNA was extracted using the MagNA Pure LC DNA isolation Kit III and an LC MagNA Pure system (Roche Diagnostics GmbH, Mannheim, Germany). The concentration and quality of DNA were measured spectrophotometrically using a NanoDrop™ 2000 (Thermo Fisher Scientific, Surrey, United Kingdom).
Genes, single nucleotide polymorphism selection, and genotyping
In a previous pharmacogenetic study of our group focused on fluoxetine pharmacodynamics (Mas et al. 2016), genes in different pathways directly or indirectly related to the fluoxetine and other antidepressant drugs response or related to the pathophysiology of major depression and other mood disorders were selected, based on clinical, experimental, and/or pharmacogenetics evidences. Based on our previous significant results with genetic markers directly related to serotonin (Mas et al. 2016; Gassó et al. 2017a, 2017b), only the previously selected genes involved in the serotonergic pathway (synthesis and metabolism: TPH1, TPH2, MTHFR, MAOA; transport: SLC6A4; and receptors: HTR1A; HTR1B; HTR2A; HTR2C; HTR3A) were included in the present study.
A total of 78 single nucleotide polymorphisms (SNPs) in 10 candidate gene regions (covering target loci and upstream and downstream regions) were selected following one of three strategies: (1) previously reported genetic associations mainly with antidepressant drug treatment or with risk of developing depression and other mood disorders; (2) tagging analysis (as implemented in Haploview 4.2) at an r
2 threshold of 0.8 to capture 98% of the most common HapMap phase II variants based on the CEU panel (minor allele frequency (MAF) >0.1; range 91%–100% for individual genes); and (3) suspected SNP functionality according to data published in the Ensembl (
Furthermore, a total of 9 SNPs in HTR1B and TPH2 were also included because they were specifically located in transcription factor binding sites, and could therefore be responsible for altered gene expression (Gassó et al. 2017a, 2017b). These polymorphisms were genotyped using TaqMan genotyping assays (Applied Biosystems, Foster City, CA) on a 7500 Real-Time PCR System (Applied Biosystems, Warrington, United Kingdom).
A total of 12 SNPs were excluded from the present analysis because they (1) failed the genotyping quality control (HTR1B rs6298, TPH2 rs2171363, and SLC6A4 rs25533); (2) were out of Hardy–Weinberg equilibrium (MTHFR rs4846052 and HTR3A rs10891613); or (3) showed MAF values less than 0.1 (MTHFR rs17037425, MTHFR rs17421560, TPH2 rs120074175, TPH2 rs11178997, HTR2A rs3125, HTR2A rs6314, and SLC6A4 rs4251417). Ultimately, 75 validated SNPs in the 10 candidate genes were analyzed (Supplementary Table S1; Supplementary Data are available online at
Statistics
Sample size and statistical power calculations were performed using the Quanto 1.2 software. These calculations were based on allele frequencies from 1000 genomes of population genetics data (
Means and standard deviations were computed for continuous variables using IBM SPSS statistics 20 software. The SNPassoc R package was used for the genetic association analysis (González et al. 2007). The best model of inheritance was selected using the Akaike information criterion. The SNP data were checked for any departure from Hardy–Weinberg equilibrium. To estimate the independent contribution of each SNP to remission and recovery, we assessed genotype frequencies by means of multivariate methods based on logistic regression analysis, with the analysis adjusted for the CDI basal score. To avoid false positive results, the Bonferroni correction (0.05/number of comparisons) for multiple testing was applied (75 SNPs assessed in remission and recovery: 150 comparisons; significant p-value ≤0.00033).
As secondary analysis, we evaluated the effect of the associated SNP (HTR2A rs7997012) on clinical improvement as assessed by changes in CDI, CGI-S, and GAF/CGAS scores by using general linear models. The analysis was adjusted for the corresponding basal score after fluoxetine treatment obtained for each scale assessed. We also assessed whether the SNP was associated with the number of readmissions and suicide attempts. The Bonferroni correction was also considered in this analysis (one SNP assessed in CDI, CGI-S, GAF/CGAS, number of readmissions, and suicide attempts: five comparisons; significant p-value ≤0.01). The genetic analysis was adjusted for the corresponding basal scale scores, because of their previously reported significant effect on remission and recovery (Bázquet et al. 2016), and on clinical improvement (Mas et al. 2016). The genetic analysis was not adjusted for any other sociodemographic (age and gender) or clinical (comorbidity, comedication, and fluoxetine dose) variables as they were not associated with remission or recovery.
Results
Demographic and clinical data are shown in Table 1. All patients were diagnosed with moderate or severe MDD. The majority of patients were women (78%) and almost all of them had a comorbid diagnosis (98%), with anxiety and eating disorders the most common (89%). The mean baseline scale score obtained before initiating fluoxetine treatment was high for both CDI and CGI-S, and low for GAF/CGAS, in accordance with the pathological condition of the patients. There were improvements of around 50% in all scale scores after the 12-month follow-up.
Before initiating fluoxetine treatment.
Admisions in the inpatient unit.
CDI, Children's Depression Inventory; CGI-S, Clinical Global Impressions-Severity; GAF/CGAS, Global Assessment of Functioning/Children's Global Assessment Scale.
Fluoxetine doses administered at baseline (20.7 ± 6.5 mg/day) and after 12 months (22.0 ± 16.9 mg/day) were similar. A high percentage of patients maintained the fluoxetine treatment throughout the follow-up (85%), with the fluoxetine doses increasing slightly from baseline (21.5 ± 7.0 mg/day) to month 12 (28.5 ± 13.1 mg/day). Only three patients changed to a different antidepressant treatment (sertraline) due to a lack of pharmacological response or side effects. Some patients, about 20%, received comedication including antipsychotics and mood stabilizers.
A total of 32 patients (70%) were remitters who did not fulfill the criteria for MDD and achieved full functioning for at least 2 weeks during the 12-month follow-up period. A total of 26 patients (56%) recovered: they did not have an MDD diagnosis at the end of the 12-month follow-up period. These patients had not experienced depressive symptoms and had achieved full functioning at least during the last 2 months of follow-up. All recovered patients have been also classified as remitters. As previously reported (Blázquez et al. 2016), both remitted and recovered patients showed better functioning and lower severity at 12 months, as indicated by their significantly lower CDI and CGI-S, and higher GAF/CGAS scores at the end of the follow-up period. Moreover, these patients had fewer readmissions and suicide attempts (admissions in the inpatient unit), which may also reflect the fact that they had a better course of disease and treatment response.
The genetic analysis showed a significant association after Bonferroni correction between the rs7997012 polymorphism located in the 5-hydroxytryptamine receptor 1A (HTR2A) gene and remission (Fig. 1 and Supplementary Table S1). It should be noted that nominal p-values from 0.0005 to 0.02 were observed for another five HTR2A polymorphisms (rs9567736, rs9567737, rs17288723, rs9534511, and rs6313; Supplementary Table S1). As shown in Table 2, remitted patients showed higher frequencies of homozygotes for the major allele (GG, 53% vs. 7%) and lower frequencies of both heterozygotes (GA, 44% vs. 57%) and homozygotes for the minor allele (AA, 3% vs. 36%) than nonremitted patients (OR = 9.1; p-value = 0.0002, under the log-additive model). Similar frequency distributions were found for recovered and nonrecovered patients, but significance was not reached (OR = 2.3; p-value = 0.08, under the log-additive model).

Genetic association results for remission and recovery under the log-additive model. The x-axis shows the 75 validated SNPs in the 10 serotonin-related candidate gene regions ordered by chromosome position. The y-axis indicates –log of the likelihood ratio tests computed, adjusting the analysis for CDI basal score obtained before initiating fluoxetine treatment. The horizontal dashed lines at –log (p) 1.30 and 3.48 correspond to nominal p-values of 0.05 and 0.00033, respectively. HTR1A, 5-hydroxytryptamine receptor 1A; HTR1B, 5-hydroxytryptamine receptor 1B; HTR2A, 5-hydroxytryptamine receptor 2A; HTR2C, 5-hydroxytryptamine receptor 2C; HTR3A, 5-hydroxytryptamine receptor 3A; MAOA, monoamine oxidase A; MTHFR, methylenetetrahydrofolate reductase; SLC6A4, Solute carrier family 6 member 4; TPH1, tryptophan 5-hydroxylase 1; TPH2, tryptophan 5-hydroxylase 2. CDI, Children's Depression Inventory; SNP, single nucleotide polymorphism.
Statistical analysis was adjusted by Children's Depression Inventory (CDI) basal score. Genetic analysis under the log-additive model. p-value in bold is significant after Bonferroni correction.
CI, confidence interval; HTR2A, 5-hydroxytryptamine receptor 2A; OR, odds ratio.
In agreement with this, changes in scale scores from baseline to 12 months of follow-up gradually increased with the number of G alleles (0, 1, or 2) of the HTR2A rs7997012 genotype (Fig. 2). Significant differences in CGI-S score changes were found between the three genotypes (mean ± SE: GG, 2.9 ± 0.4; GA, 2.1 ± 0.3; AA, 0.5 ± 0.5; p-value = 0.008, under the log-additive model), with homozygotes for the major and minor allele showing higher and lower clinical improvement, respectively. Although the same trend was observed for score changes in CDI (mean ± SE: GG, 14.4 ± 1.1; GA, 12.7 ± 2.3; AA, 6.2 ± 4.5; p-value = 0.06, under the log-additive model) and GAF/CGAS (mean ± SE: GG, 28.9 ± 4.0; GA, 21.8 ± 4.1; AA, 13.3 ± 8.0; p-value = 0.06, under the log-additive model), these differences were not significant.
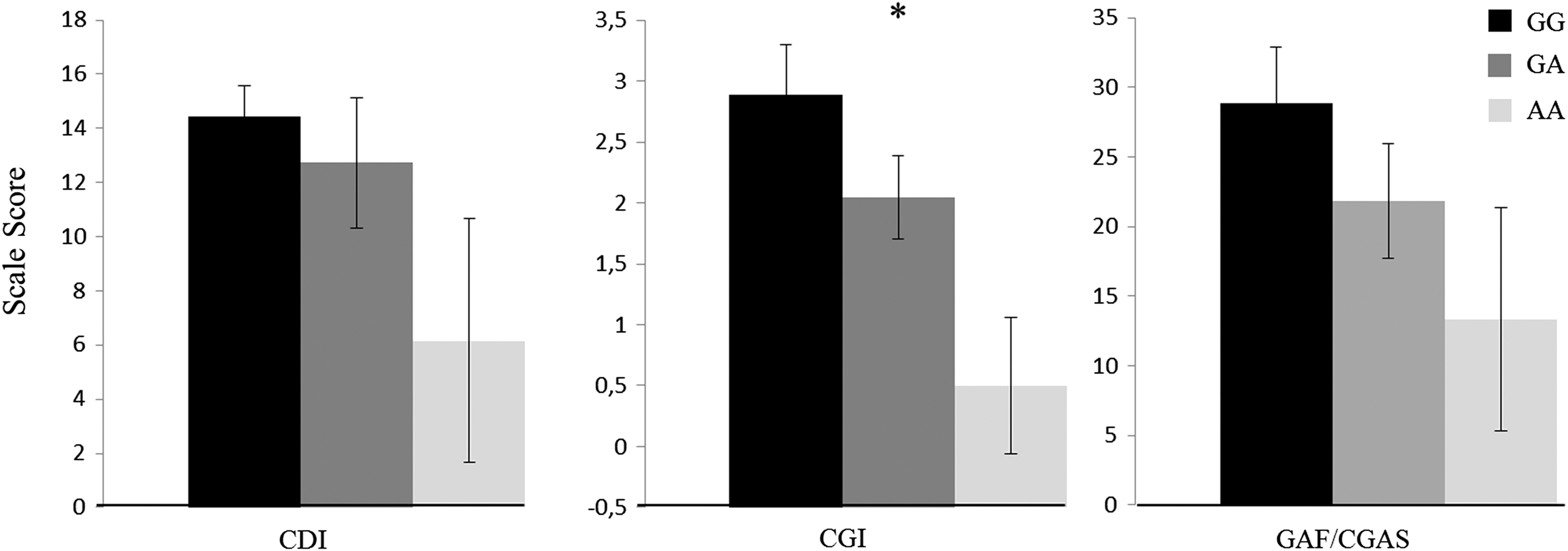
Effect of HTR2A rs7997012 on clinical improvement measured by differences between baseline and 12-month scale scores. Scale scores show decreases in the CDI and CGI-S, and increases in the GAF/CGAS scales. Higher scale scores indicate higher improvement. The analysis was adjusted for the corresponding baseline score obtained before initiating fluoxetine treatment. Results are expressed as means ± SEM. *p-value = 0.008, under the log-additive model. CGI-S, Clinical Global Impressions-Severity; GAF/CGAS, Global Assessment of Functioning/Children's Global Assessment Scale.
Finally, GG homozygotes showed a trend to experience fewer readmissions than allele A carriers (mean ± SE: GG, 0.11 ± 0.07; GA, 1.2 ± 0.4; AA, 1.0 ± 0.5; p-value = 0.013, almost significant after Bonferroni correction). There were no differences in the number of suicide attempts among the genotypes (mean ± SE: GG, 0.4 ± 0.2; GA, 0.4 ± 0.2; AA, 1.2 ± 0.8; p-value >0.01).
Discussion
The results of this study provide more evidence of the involvement of genetic variants related to the serotonergic pathway in the antidepressant response. Particularly, the HTR2A rs7997012 was associated with remission and clinical improvement after fluoxetine treatment in children and adolescents diagnosed with MDD who were prospectively followed up for 12 months. While the homozygotes for the major allele (GG) showed the highest percentage of remitters and the highest score reductions on the CGI-S scale after the 12-month follow-up, the homozygotes for the minor allele (AA) were those who showed the lowest percentage of remitters and the lowest score reductions on the CGI-S scale. Moreover, although the results were on the border of statistical significance after Bonferroni correction, the homozygous GG patients also tended to experience fewer readmissions (admissions in the inpatient unit) during the follow-up period.
The rs7997012 SNP is located in intron 2 of the HTR2A gene, which codes for the postsynaptic serotonin 2A receptor (5-HT2A). To the best of our knowledge, there are no studies of the impact of this polymorphism on receptor activity. However, the SNP could influence central serotonergic transmission, as it has been associated with the binding potential of the serotonin transporter, which suggests that either a direct or an indirect functional relationship exists between the transporter and 5-HT2A systems (Laje et al. 2010). This would support the multiple reports of evidences of the impact of rs7997012 on response to pharmacological treatment with SSRIs in patients with MDD.
The first evidence was found in the Sequenced Treatment Alternatives for Depression (STAR*D) study involving 1953 patients in which 768 SNPs in 68 candidate genes were genotyped. The HTR2A rs7997012 was the top SNP associated with citalopram response. Specifically, individuals who were homozygous for the minor allele (AA) showed more favorable outcomes (McMahon et al. 2006). Later evidence further supported the involvement of this SNP in antidepressant response, but with the opposite genotype (GG) associated with greater clinical improvement (Horstmann et al. 2010; Lucae et al. 2010), which is in line with our results. In fact, results from recent meta-analyses have shown that GG homozygotes and G allele carriers experienced better antidepressant responses (Niitsu et al. 2013; Lin et al. 2014).
Furthermore, the AA genotype has been nominally associated with antidepressant treatment resistance in another study (Noro et al. 2010). Interestingly, Lohoff et al. (2013) also reported an association between the G allele and better antidepressant outcomes in patients diagnosed with GAD and treated with venlafaxine. All of these results support the hypothesis that HTR2A rs7997012 is involved in the response to antidepressant drugs independently of the underlying DSM-IV diagnostic category.
Together with the solute carrier family 6 member 4 (SLC6A4), gene that codifies the serotonin transporter, HTR2A represents the top serotonergic gene that has been associated most with the pharmacogenetics of MDD (Fabbri and Serretti 2015). Besides rs7997012, other HTR2A polymorphisms, including rs6311 (1438A/G) and rs6313 (102T/C) have also been shown to be involved in the antidepressant response (Horstmann and Binder 2009; Lin et al. 2014), and with susceptibility to MDD (Zhao et al. 2014). However, these variants were not significantly associated in the present study (rs6311: p-value = 0.06; rs6313: p-value = 0.02).
Depressed patients often have increased 5-HT2A receptor densities, suggesting that this receptor may play an important role in the pathophysiology of MDD (Shelton et al. 2009). It is important to note that the mode of action of SSRIs includes the modulation of 5-HT2A, as downregulation of this receptor occurs after pharmacological treatment with these antidepressant drugs. Moreover, 5-HT2A antagonists generate antidepressant-like effects, which may explain why the use of atypical antipsychotics augments the clinical response to SSRIs in treatment-resistant patients (Artigas 2013; Fakhoury 2016).
It should be noted that HTR2A rs7997012 did not reach significance when we assessed clinical improvement in children and adolescents with different psychiatric diagnoses after 2–3 months of initiating fluoxetine treatment (Mas et al. 2016). Although statistical power was higher in the previous study because a larger number of patients were included, only nominal p-values <0.05 were detected for this and other HTR2A polymorphisms.
There is much evidence that supports the claim that polymorphisms in different genes related to the serotonergic pathway, including other serotonin receptors and enzymes involved in neurotransmitter bioavailability, play a role in antidepressant response (Kato and Serreti 2010; Helton and Lohoff 2015). In fact, recent research by our group has also associated genetic and epigenetic variants in the HTR1B and TPH2 genes with antidepressant response after 12 weeks of fluoxetine treatment in children and adolescents with different psychiatric diagnoses (Mas et al. 2016; Gassó et al. 2017a, 2017b). Besides genetic polymorphisms, epigenetic and gene expression modifications are increasingly being explored to identify useful genetic biomarkers for the prediction of antidepressant response (Lin and Tsai 2016; Belzeaux et al. 2017; Lisoway et al. 2017).
The main limitation of this study is the small sample size, which limits the association of genetic variants that might have smaller effects on clinical response, and also make the results more questionable, especially when the genotype groups include very few subjects that reduce the statistical power increasing probability of a Type I error. To avoid false positive results, Bonferroni correction was applied, which is the most conservative correction for multiple testing as comparisons are computed independent of each other. Moreover, the number of tests we considered included all SNPs and clinical outcomes assessed, which notably reduced the Bonferroni-corrected p-value. However, several SNPs in each gene were in high linkage disequilibrium and the clinical variables were highly correlated.
It is important to highlight the homogeneity of our cohort in terms of age, diagnosis, ethnicity, and antidepressant treatment, as all the participants were young (children and adolescents) Caucasians diagnosed with MDD. All of them had received antidepressant treatment for the first time, specifically fluoxetine, for at least 12 weeks and most of them maintained treatment with this antidepressant drug for the 12-month follow-up period. Therefore, important confounders that can lead to stratification in other similar studies were avoided in this research. Another important strength is the prospective design, together with the long follow-up period, as the vast majority of studies assess clinical response within the first 3 months of starting antidepressant treatment.
The fact that some patients could have received comedication could have somehow affected their clinical improvement, even though no differences were detected. Finally, it should be noted that other important serotonergic genes not studied here could have also influenced the fluoxetine response. Given all these limitations, other studies with independent larger cohorts are needed to replicate and confirm our results.
Conclusions and Clinical Significance
This study provides further support for the involvement of the HTR2A gene in the antidepressant response. Particularly, the rs7997012 SNP was associated with clinical improvement after fluoxetine treatment in children and adolescents diagnosed with MDD who were prospectively followed up for 12 months. These results may be useful to develop clinical predictors of antidepressant response to provide individualized treatment to achieve better improvement and prognosis. As other genetic and epigenetic variants in serotonergic genes also appear to be involved, studies with larger cohorts are needed to integrate all these relevant variants into the clinical predictors.
Footnotes
Acknowledgments
The authors thank the Language Advisory Service at the University of Barcelona for article revision. The authors also thank all subjects and their families for the time and effort spent on this study.
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.