
Abstract
Objective:
Children and adolescents with attention-deficit/hyperactivity disorder (ADHD) frequently have comorbidities that are potential indications for antipsychotics (APs). Some studies have suggested that the combined use of methylphenidate (MPH) and APs is increasing in this population group. Longitudinal analyses and in-depth investigations on the substance level are lacking. This study aimed to estimate the cumulative proportion of concomitant AP/MPH use in children and adolescents with ADHD over a follow-up of up to 9 years and to describe patient characteristics stratified by specific AP drug.
Methods:
Based on claims data, concomitant AP/MPH use was identified among 67,595 children and adolescents with ADHD starting MPH treatment between 2005 and 2013. Characteristics and diagnoses—including those indicating appropriateness of AP use according to approved indications and/or guidelines—were examined at the time of first AP/MPH combination therapy. In addition, subsequent use of AP/MPH combination therapy was evaluated.
Results:
The cumulative proportion of individuals with any AP/MPH combination therapy rose to over 6% within 9 years after initiating MPH. The most frequent APs first used in combination with MPH were risperidone (72%), pipamperone (15%), and tiapride (8%). Percentages of psychiatric hospitalization in the year preceding the first combination therapy with MPH were 33%, 43%, and 19%, respectively. The proportion of individuals with potentially appropriate use was high (>72%) in risperidone/MPH and tiapride/MPH and low (15%) in pipamperone/MPH combination users. Conduct disorders and tic disorders were frequent in users who were prescribed MPH with risperidone and tiapride, respectively. One-quarter of patients with AP/MPH combination therapy were one-time-only combination users.
Conclusion:
Our study suggests that a considerable proportion of children and adolescents with ADHD receive MPH in combination with APs and that this is a factor not only during the first years of MPH treatment. ADHD guidelines should specify algorithms concerning the use of AP medication.
Introduction
A
Antipsychotics (APs) are often prescribed off-label to individuals with ADHD and comorbid conduct disorders (Bachmann et al. 2014). ADHD children suffering from conduct disorders may present severely aggressive behavior, which, in turn, can justify drug therapy with APs (Taylor et al. 2004; NICE 2017). According to the treatment recommendations for the use of APs for aggressive youth (TRAAY), even combinations of psychotropic medications, including an AP, are deemed appropriate (Pappadopulos et al. 2003). Some cross-sectional and short-term observational studies have shown that APs and stimulants such as MPH are increasingly prescribed concomitantly (Safer et al. 2003; Comer et al. 2010; Sikirica et al. 2013; Betts et al. 2014). However, the percentage of concomitant prescribing after starting MPH treatment with a long follow-up is not known.
Evidence for drug-drug interactions regarding efficacy and safety of AP/MPH combination therapy varies depending on the individual AP drug. This, however, is often contrary to the information given to prescribers. For example, the Summary of Product Characteristics (SPCs) for MPH in European countries notes that caution is recommended for concomitant use with APs in general (CHMP 2009), without drug-specific statements. Hence, a physician who decides to prescribe an AP in combination with MPH might assume that there are no crucial differences in the safety profiles of different APs. Conversely, the European Union (EU)-harmonized wording in the SPC of risperidone explicitly states that the combination with MPH had no effect on the pharmacokinetics and efficacy of the drug (EMA 2008). Most national and international ADHD guidelines either do not focus on combinations with APs at all (NICE 2016) or only on the AP class level (Pappadopulos et al. 2003; Pliszka et al. 2006). Few guidelines give drug-specific recommendations (Kutcher et al. 2004; Taylor et al. 2004; Döpfner et al. 2007). Little is known about which APs are prescribed to ADHD patients in combination with MPH.
Our study aimed to (1) estimate the proportion of children and adolescents (aged 0–17 years) diagnosed with ADHD who ever received AP/MPH combination therapy over a 9-year follow-up after initiating MPH, (2) investigate which AP drugs were primarily used in combination with MPH, (3) describe the characteristics of the patients depending on the AP used in combination with MPH, and (4) describe and compare the characteristics of patients with versus without subsequent AP/MPH combination therapy.
Materials and Methods
Study design and data source
This study was designed as a cohort study and was based on the German Pharmacoepidemiological Research Database (GePaRD) covering the years 2004 to 2013, that is, the most recent year that was available at the time of analysis. GePaRD consists of claims data from more than 20 million members of statutory health insurance (SHI) providers across Germany. The database includes information on demographics, hospitalizations, physician visits, and drug treatment. Hospital data contain diagnoses, therapeutic/diagnostic procedures, and the dates of admission and discharge. In this study, the admission date along with the main and secondary discharge diagnoses were used as characteristics for hospital diagnoses. Outpatient data comprise quarterly diagnoses and procedures with an exact date. All diagnoses are coded according to the International Classification of Diseases and Related Health Problems, 10th Revision, German Modification (ICD-10-GM). Drug data include the anatomical-therapeutic-chemical (ATC) code and the defined daily dose (DDD). Data in GePaRD have been shown to be representative for the German population regarding sex, age, hospitalizations, and prescriptions (Pigeot and Ahrens 2008; Schink and Garbe 2010a, 2010b).
Cohort definition
The cohort included children and adolescents aged <18 years diagnosed with ADHD who started MPH treatment between 2005 and 2013. ADHD diagnoses were identified by the ICD-10 codes F90.0, F90.1, F90.8, F90.9, or F98.8 from the baseline period. These ICD-10 codes were used in a recent study to identify ADHD patients in German health insurance data (Bachmann et al. 2017). Individuals with an atomoxetine (ATX) prescription before the initial MPH prescription or with prescriptions of lisdexamfetamine (LIS) or dexamfetamine (DEX) at any time were excluded since these drugs played a minor role in clinical practice during the study period. Cohort entry was defined as the first outpatient MPH dispensation after a baseline period of at least 1 year without any MPH dispensation. Cohort exit was defined as insurance end due to any reason (including death), end of the year the cohort member turned 17 years, or end of the study period, whichever came first. To analyze the period following the first AP/MPH combination therapy, individuals were followed up after the AP/MPH combination therapy.
MPH exposure
MPH exposure started on the date of dispensation of the drug from the pharmacy. The duration of each MPH dispensation was estimated by the number of dispensed DDDs, since dose information is not recorded in GePaRD. Overlapping exposure periods were considered continuous treatment and combined into one MPH exposure period.
Combination therapy of APs and MPH
Outpatient AP drug dispensations during follow-up were identified based on ATC codes starting with N05A, except lithium (Bachmann et al. 2014). They were classified as AP/MPH combination therapy if the AP dispensation occurred during an MPH exposure period and at least 14 days before MPH exposure ended. The last 14 days were excluded to avoid misclassifying switches as concomitant use. The dispensation date of the first AP/MPH combination therapy was identified and will hereafter be referred to as the index date. It was ascertained whether the AP and the most recent MPH prescription were issued by different medical practices (by comparing the respective registration numbers) and whether the AP was dispensed on the same day as MPH.
Diagnoses related to AP/MPH combination therapy
To assess coexisting morbidities possibly related to the AP/MPH combination therapy, diagnoses were ascertained across three quarters (the quarter of the index date, the preceding, and the following quarter). Comorbidities included, among others, on- and off-label indications for MPH and/or APs. In addition, potentially appropriate AP use was examined for the three most frequently used APs. It applied if any AP-specific diagnosis was recorded that might justify on- and off-label use of the AP. These diagnoses were identified from the respective SPCs, from guidelines (Roessner et al. 2011; NICE 2017), and other literature (Canitano and Scandurra 2008; Roessner et al. 2013).
Further characteristics
Psychiatric hospitalizations were ascertained for the year preceding the index date and were defined as such if there was at least one main or secondary psychiatric diagnosis (ICD-10 F00-F99). ATX use was ascertained from the index date going back to the initial MPH prescription (i.e., cohort entry).
Statistical analyses
The time from cohort entry until the first AP/MPH combination therapy was determined with a Kaplan-Meier estimate. The cumulative proportion of patients with AP/MPH combination therapy over a 9-year follow-up was thus 1 minus the Kaplan-Meier estimate. The analysis was done overall and stratified by sex. Characteristics and comorbidities of patients with AP/MPH combination therapy were shown stratified by the first concomitantly used AP. In addition, characteristics were shown for patients with at least 1 year of follow-up after the first AP/MPH combination therapy, stratified by subsequent use of AP/MPH combination therapy within 1 year. To identify statistical differences between groups, Pearson's χ2 test at a 5% α level was used. All statistical analyses were conducted using SAS version 9.3.
Ethical approval
The use of SHI data for scientific research is regulated by the Code of Social Law in Germany. All involved SHIs and the competent authorities approved the use of the data for this study; no ethical approval was necessary. Informed consent of the involved insurants was not required by law since this study was based on pseudonymous data.
Results
Study cohort
After applying all inclusion and exclusion criteria, the final study cohort comprised 67,595 children and adolescents with a diagnosis of ADHD, who initiated MPH therapy (Fig. 1). The proportion of males was 77% and the mean age was 10.1 years.
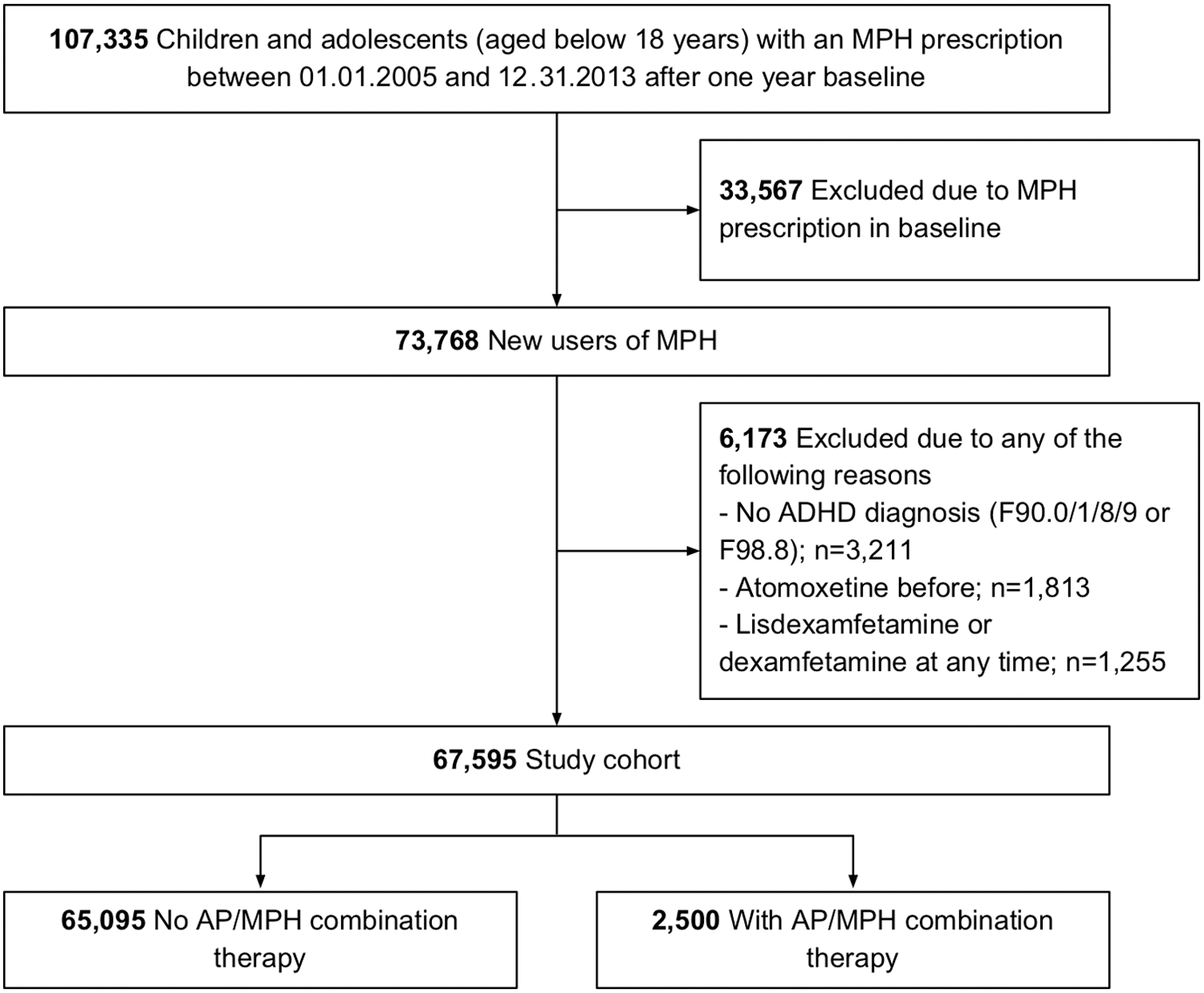
Flowchart of study cohort development. ADHD, attention-deficit/hyperactivity disorder; AP, antipsychotic; MPH, methylphenidate.
Proportion and types of AP/MPH combination therapy
The cumulative proportion of newly MPH-treated children and adolescents with ADHD, who received at least one AP/MPH combination therapy, rose to almost 2% within the first year after MPH initiation and was over 6% after 9 years (Fig. 2). Of all AP/MPH combination users (n = 2500), the most frequent APs that were first used in combination with MPH included risperidone (71.6%; n = 1790), pipamperone (14.8%; n = 371), tiapride (7.6%; n = 190), chlorprothixene (1.6%; n = 41), melperone (1.6%; n = 39), quetiapine (1.2%; n = 29), and aripiprazole (0.9%; n = 22). A total of 24 AP/MPH combination users received more than 1 AP on the first date of combination use. These patients and those with rarely used APs (use by <50 patients) were assigned to “other APs” for the characterization of users with AP/MPH combination therapy.
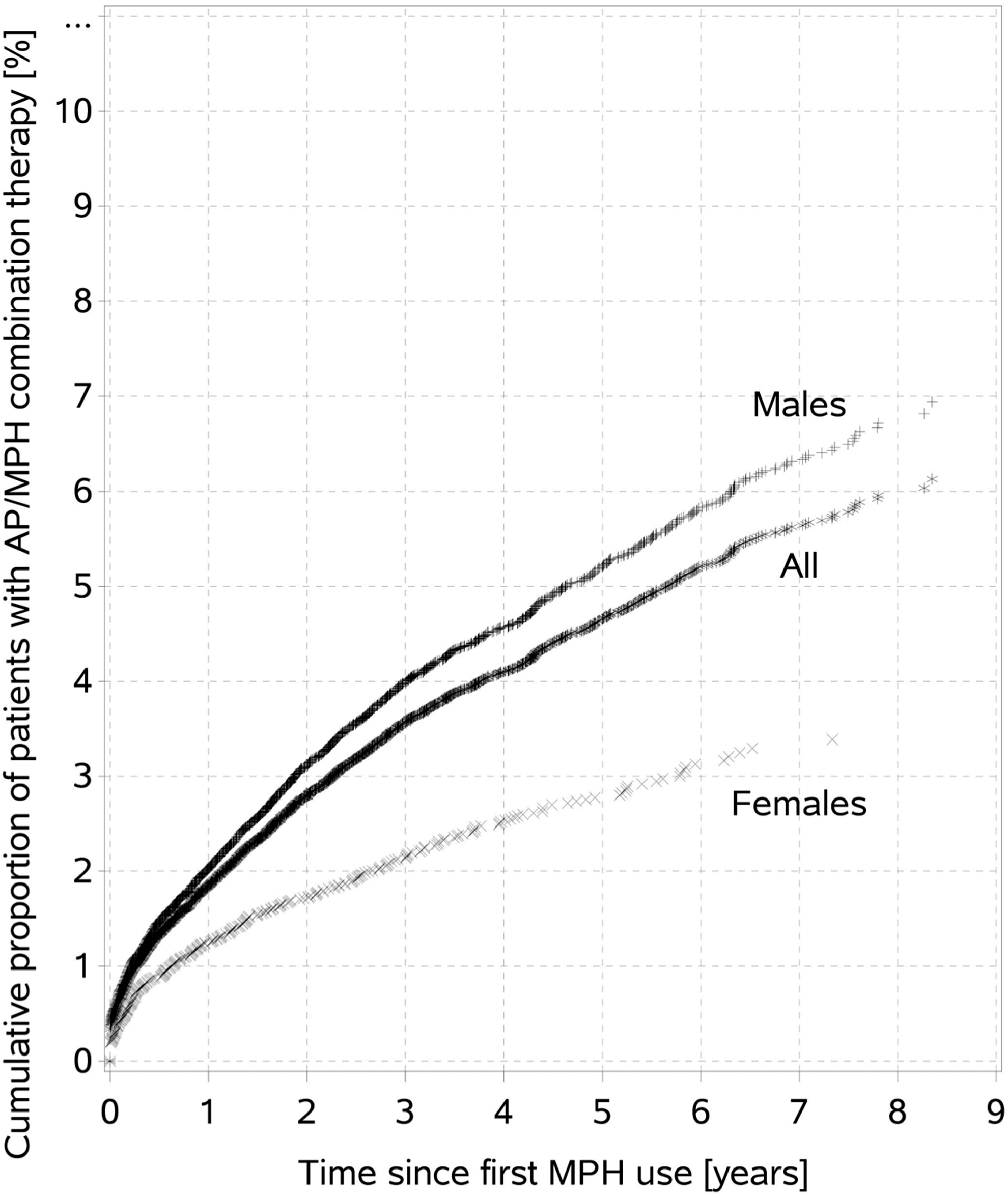
Long-term analysis on the proportion of children and adolescents diagnosed with attention-deficit/hyperactivity disorder with AP and MPH combination therapy by time since first MPH use. AP, antipsychotic; MPH, methylphenidate.
Characteristics of users with AP/MPH combination therapy
Most of the patients received the first AP/MPH combination therapy in the age group 7–11 years and few were younger than 7 years (Table 1). Percentages of psychiatric hospitalization were highest for users of “other APs” (45%), followed by pipamperone users (43%), risperidone users (33%), and tiapride users (19%).
Only if used as monotherapy, that is, not with a second AP, otherwise assigned to “Other APs.”
With at least one main or secondary psychiatric diagnosis (ICD-10 F00–F99).
ADHD, attention-deficit/hyperactivity disorder; AP, antipsychotic; ATX, atomoxetine; HCC, healthcare center; ICD-10, International Classification of Diseases and Related Health Problems, 10th Revision; MPH, methylphenidate.
Compared to risperidone, pipamperone, and “other APs,” tiapride was predominantly prescribed by child psychiatrists and pediatricians. Pipamperone (10%) and “other APs” (15%) were more often prescribed by general practitioners than risperidone and tiapride (each below 8%). In 12% to 18% of the cases, the prescriptions of the first concomitantly used AP and the most recent MPH were issued by different medical practices.
Tiapride users had substantially higher numbers of tic disorders (73%) than users of all other APs (<11%, Table 2). Any conduct disorder was, in particular, present in concomitant users of MPH and risperidone or pipamperone (about 68% each), but less often with tiapride (37%). There was a potentially appropriate diagnosis for the use of risperidone or tiapride in more than 72% of users of those APs. This was the case for only 15% of pipamperone users.
Only if used as monotherapy, that is, not with a second AP, otherwise assigned to “Other APs”.
Exclusively related to the nine below-mentioned comorbidities.
According to license and/or guidelines. ICD-10 codes included for risperidone: F20, F31, F60.2/3/8, F63, F84, F90.1, F91, F92, and F95; for pipamperone: G47, F51, R45.0/1/4, and R46.3; for tiapride: G10, G24.0/4, and F95.
AP, antipsychotic; ICD-10, International Classification of Diseases and Related Health Problems, 10th Revision; MPH, methylphenidate; NA, not applicable.
Eighty percent (n = 2006) of the patients could be followed for at least 1 year after the first AP/MPH combination therapy. Of these, 25% (n = 494) did not have any subsequent AP/MPH combination use within 1 year. Compared to those with any subsequent AP/MPH combination therapy within 1 year, patients with a one-time-only AP/MPH combination therapy more often received pipamperone, were more frequently female, and suffered less frequently from tic disorders or any conduct disorders (Table 3). In addition, percentages of prior psychiatric hospitalizations were lower.
Among those with at least 1 year of follow-up after the first AP/MPH combination therapy (total n = 2006).
Hospitalization with at least one main or secondary psychiatric diagnosis (ICD-10 F00–F99).
AP, antipsychotic; ICD-10, International Classification of Diseases and Related Health Problems, 10th Revision; MPH, methylphenidate.
Discussion
In this study, we investigated the extent of combination therapy with APs and MPH among children and adolescents with ADHD over a maximum follow-up of 9 years after initiating MPH treatment. During this long observation period, over 6% of all MPH-treated children and adolescents with ADHD ever received AP/MPH combination therapy. APs used in combination with MPH were mainly limited to risperidone, pipamperone, and tiapride. Users who were prescribed a combination of MPH with risperidone or pipamperone were frequently diagnosed with conduct disorders, whereas those with tiapride often had comorbid tic disorders. Mental retardation, developmental delay, and pervasive developmental disorders—typical other neurodevelopmental disorders co-occurring with ADHD—were also frequent diagnoses in users of AP/MPH combination therapy.
Proportion of users with AP/MPH combination therapy
Compared to a study by Sikirica et al. (2013), which was based on patient chart reviews, our results show a similar frequency of combination therapy involving an AP and ADHD medication. Their study found a prevalence of concomitant AP use of 3% in Germany, which is in accordance with our estimate at about 2 years after starting MPH treatment. Also, Sikirica et al. found frequencies of comorbidities, particularly behavioral disorders, similar to ours. In our study, the cumulative proportion of children and adolescents receiving an AP in combination with MPH did not reach a plateau, but continuously rose in the long term. That is, AP/MPH combination therapy is a factor not only during the first years of ADHD treatment but may also be relevant in later years.
Drug-specific results regarding APs used in combination with MPH
A systematic review published in 2013 summarized evidence on the efficacy and tolerability of AP and stimulant combination therapy in children and adolescents with ADHD and disruptive behavior disorders (Linton et al. 2013). Risperidone was used as the AP in four of nine included studies. The efficacy of the risperidone/MPH combination therapy compared to monotherapy in treating aggression and hyperactivity could not clearly be shown; however, the combination was well tolerated. A later published placebo-controlled study showed improvement in aggressive child behavior when risperidone was added to stimulant treatment (Aman et al. 2014). In our study, risperidone was the most commonly prescribed AP in combination with MPH. It was used presumably for “any conduct disorder” as defined in our study, which included oppositional defiant disorders and required aggressive, dissocial, and/or defiant behavior according to ICD-10. The fact that conduct disorders are licensed indications for risperidone in conjunction with the positive wording regarding combined risperidone/MPH use in the SPC of risperidone (EMA 2008) makes the decision to prescribe risperidone in combination with MPH plausible. However, to date, still too little is known, particularly about the long-term safety of this combination therapy.
The high percentages of tic disorders among tiapride/MPH combination therapy users suggest that it was rather used for this comorbidity. This is in accordance with the European (German) guideline for tic disorders, which includes the combination of MPH and an AP (tiapride) in children and adolescents with tics and coexisting ADHD (Rothenberger et al. 2007; Roessner et al. 2011). According to a more recent review, ATX (milder cases) or risperidone/stimulant combination therapy (more severe cases) is recommended for these patients (Roessner et al. 2013). ATX is also recommended in the above-mentioned guidelines as an alternative for tic disorders. In our study, patients with combined tiapride/MPH use had the highest percentage of ATX use before the first combination therapy. Our results considering tiapride/MPH combination therapy are therefore in accordance with the guideline recommendations in most of the respective cases.
Evidence for combining MPH with pipamperone is lacking and we found no studies about risks and benefits of this combination. Therefore, the considerable proportion of patients with this combination (about 15%) is surprising and should be further investigated. Among other reasons, the prescribing physicians might have chosen pipamperone and not risperidone—for patients with similar mental and physical conditions—as risperidone is not licensed for long-term therapy or for children with a normal intelligence quotient. Our results suggest that the spectrum of comorbidities in pipamperone/MPH users is comparable to users of risperidone/MPH combination therapy. However, compared to the latter, pipamperone/MPH combination therapy was more often prescribed subsequent to psychiatric hospitalization. This could suggest that pipamperone/MPH combination users were affected more severely and/or that they needed urgent treatment. However, pipamperone, in contrast to risperidone, is neither licensed nor recommended for conduct disorders and only 15% of pipamperone users had any potentially appropriate diagnosis. The higher percentage of one-time pipamperone/MPH combination therapy users in our study might either indicate lack of efficacy and/or tolerability, or an immediate therapy response. Our data do not permit conclusions on these aspects.
Characteristics of physicians prescribing AP/MPH combination therapy
Compared to prescribers of APs in the general population of children and adolescents (Bachmann et al. 2014), the proportion of child and adolescent psychiatrists was higher in our study (42% versus 28%), whereas pediatricians were equally frequent and general practitioners were about 50% less frequent. This shift from primary care physicians to specialized physicians for APs prescribed in combination with MPH is encouraging since such very complex treatment approaches should ideally be supervised by a specialist in childhood/adolescent behavioral disorders, as already recommended for MPH monotherapy throughout the EU (CHMP 2009).
General practitioners were slightly more often prescribers of an initial pipamperone/MPH combination therapy than was the case with risperidone or tiapride. This might be explained by the fact that the approval of pipamperone is generally not restricted, for example, to a minimum age. In addition, as this AP has been available for more than 50 years, nonspecialists might consider it established and safe. However, using pipamperone in combination with MPH is not the best treatment option according to the available evidence, as mentioned above. We determined that in about 16% of all cases where pipamperone was first used as AP/MPH combination therapy, the AP and the most recent MPH treatment were prescribed by different practices. In those cases, it is possible that the AP prescriber did not know about current MPH treatment. However, one should be able to take for granted that physicians routinely ask the parents/carers about current medical treatments.
Strengths and limitations
The main strength of our study is the underlying health claims database, which represents about 20% of the German population. This data source allowed us to analyze rare treatment combinations. Importantly, as the database contains multisectoral data on the individual patient level, combination therapies were identified independent of prescribers and parents. This erases recall bias and provides information about combination therapies potentially unknown to the treating physicians. Moreover, we had few exclusion criteria, which facilitated a genuine image of medical care. Thus, our results can be considered representative for the drug-treated ADHD population younger than 18 years in Germany.
Another strength is that we did not automatically stop the analysis after patients discontinued MPH treatment. Instead, gaps between MPH use periods were allowed. This appeared necessary since children and adolescents with ADHD frequently interrupt stimulant medication even if discontinuation is not recommended (Thiruchelvam et al. 2001). In addition, prescribers of MPH have been advised since 2009 to institute withdrawal trials at least once yearly to reevaluate the long-term usefulness of the treatment (CHMP 2009). This advice might have led to an increase in MPH interruptions.
Some limitations ought to be noted. Generally, claims data are less detailed than clinical data (Schneeweiss and Avorn 2005). It should be noted that the claims data offer information on filled prescriptions rather than the real intake by the patients. Since GePaRD does not contain the length of each prescription, we had to calculate the length of MPH exposure periods based on dispensed DDDs. We did not evaluate trends over time as that would have been outside the scope of the investigation. As for diagnoses, in some cases, solely basing definitions of mental disorders on ICD codes is challenging compared to using the Diagnostic and Statistical Manual of Mental Disorders, which includes more information.
Conclusions
Overall, the prescribers' AP drug choices seem to be in accordance with current guidelines in most children and adolescents with ADHD, who received risperidone or tiapride in combination with MPH. However, it remains unclear whether the duration of their use—for example, risperidone should only be used for short-term management of severely aggressive behavior—was appropriate and whether the users were adequately monitored. A considerable proportion of patients received pipamperone/MPH combination therapy despite no evidence on its efficacy and tolerability. Physicians should be informed about the lacking evidence on pipamperone/MPH combination therapy and that, if any, risperidone should be considered the AP of first choice in combination with MPH. However, more randomized controlled trials and epidemiological studies to prove the efficacy and safety of risperidone/MPH combination therapy would be valuable to confirm the suggested positive evidence. Our study found a considerable amount of AP/MPH combination therapy in children and adolescents with ADHD, suggesting a need for the inclusion of drug-specific statements concerning psychotropic combination therapy in ADHD guidelines, particularly for patients with comorbid psychiatric disorders.
Clinical Significance
This population-based study found that a relatively high number of MPH-treated children and adolescents with a diagnosis of ADHD receive additional treatment with APs. AP/MPH combination therapy is a factor not only during the first years of MPH treatment but may also be relevant in later years. Although the prescribers' AP drug choices seem to be in accordance with current guidelines in most of the cases, still a considerable proportion of patients receive APs despite a lack of evidence on their use in combination with MPH.
Footnotes
Disclosures
O.S., D.E., and O.R. are working at the Leibniz Institute for Prevention Research and Epidemiology—BIPS. Unrelated to this study, BIPS occasionally conducts studies financed by the pharmaceutical industry. Almost exclusively, these are postauthorization safety studies (PASS) requested by health authorities. The studies and the resulting publications are not influenced by the pharmaceutical industry. E.G. has been consultant to Bayer, Schering, Nycomed, Teva, GSK, Takeda, Astellas, and Novartis in the past. T.B. served in advisory or consultancy roles for Actelion, Hexal Pharma, Lilly, Medice, Novartis, Oxford outcomes, PCM scientific, Shire, and Viforpharma; received conference support or speaker's fees by Medice, Novartis, and Shire; is/has been involved in clinical trials conducted by Shire and Viforpharma; received royalties from Hogrefe, Kohlhammer, CIP Medien, and Oxford University Press. All authors declare that this work is unrelated to the above grants and relationships.
Acknowledgments
The authors would like to thank all SHI providers, which provided data for this study, namely the German SHIs AOK Bremen/Bremerhaven, DAK-Gesundheit, hkk Krankenkasse, and Techniker Krankenkasse (TK).