
Abstract
Background:
Novel interventions for treatment-resistant depression (TRD) in adolescents are urgently needed. Ketamine has been studied in adults with TRD, but little information is available for adolescents. This study investigated efficacy and tolerability of intravenous ketamine in adolescents with TRD, and explored clinical response predictors.
Methods:
Adolescents, 12–18 years of age, with TRD (failure to respond to two previous antidepressant trials) were administered six ketamine (0.5 mg/kg) infusions over 2 weeks. Clinical response was defined as a 50% decrease in Children's Depression Rating Scale-Revised (CDRS-R); remission was CDRS-R score ≤28. Tolerability assessment included monitoring vital signs and dissociative symptoms using the Clinician-Administered Dissociative States Scale (CADSS).
Results:
Thirteen participants (mean age 16.9 years, range 14.5–18.8 years, eight biologically male) completed the protocol. Average decrease in CDRS-R was 42.5% (p = 0.0004). Five (38%) adolescents met criteria for clinical response. Three responders showed sustained remission at 6-week follow-up; relapse occurred within 2 weeks for the other two responders. Ketamine infusions were generally well tolerated; dissociative symptoms and hemodynamic symptoms were transient. Higher dose was a significant predictor of treatment response.
Conclusions:
These results demonstrate the potential role for ketamine in treating adolescents with TRD. Limitations include the open-label design and small sample; future research addressing these issues are needed to confirm these results. Additionally, evidence suggested a dose–response relationship; future studies are needed to optimize dose. Finally, questions remain regarding the long-term safety of ketamine as a depression treatment; more information is needed before broader clinical use.
Introduction
D
Ketamine is an N-methyl-
The current study examined the effects of six serial infusions of intravenous ketamine, given over 2 weeks, as an acute intervention for TRD in adolescents. The first aim was to assess the extent and duration of clinical response. To do this, we assessed for response and remission 1 day following the six infusions, and for responders, we measured duration of response in a 6-week follow-up period. We hypothesized that ketamine treatment would be associated with reduced depression symptoms, and that due to enhanced plasticity evident during development (Ismail et al. 2017), the duration of response would be longer in adolescents than previously reported for adults. For example, in a study of adults with TRD using a protocol of six ketamine infusions over 2 weeks, 5 of 11 responders were still in remission at 4 weeks, and for those that had relapsed, mean time to relapse was 16 days (Shiroma et al. 2014). Therefore, we selected a follow-up period of 6 weekly visits and a final 6-month visit to capture potentially longer duration of response. The second aim was to evaluate tolerability of ketamine in adolescents. We predicted that, similar to low-dose ketamine studies in adults, adolescents would show transient hemodynamic changes and elevations in dissociative symptoms. Third, we explored clinical and demographic predictors of treatment response.
Patients and Methods
Oversight
The study was approved by the University of Minnesota Institutional Review Board. The United States Food and Drug Administration issued an exemption for the study from the need for oversight. The study “Ketamine in Adolescents With Treatment-Resistant Depression” was listed on
Participants
Adolescents with TRD were recruited through community postings and clinical referrals. Inclusion criteria included age 12–18 years, current diagnosis of Major Depressive Disorder, Children's Depression Rating Scale-Revised (CDRS-R) (Poznanski et al. 1985) raw score >40, and treatment resistance defined as a failure to exhibit a satisfactory response to at least two antidepressant medications. Rigor of antidepressant trials was assessed using the Antidepressant Treatment History Form (Sackeim 2001); past trials were considered sufficient if they scored at least a “3” (on a scale of 1 to 4; as an example, a rating of “3” for fluoxetine is 4 weeks or more and dosage 20–39 mg/day, a rating of “4” is 4 weeks or more and dosage ≥40 mg/day), or if the trial was truncated due to intolerance (as opposed to an early decision regarding inefficacy). Current psychotropic medications had to be dose stable for 2 months. If participants opted to discontinue any psychotropic medications before the study, we required a washout period of 2 weeks for mood stabilizers and antipsychotic medications, 4 weeks for antidepressants, and 1 week for stimulants. Exclusion criteria were the presence of a current substance use disorder, a primary psychotic disorder, bipolar disorder, autism spectrum disorder, a history of intellectual disability, a nonpsychiatric neurological disorder, or a significant medical illness.
Pretreatment clinical assessment
Following informed consent (with parents for those under 18 years) and assent (for those 12–17 years), participants were evaluated using the Kiddie Schedule for Affective Disorders and Schizophrenia, Present and Lifetime Version (K-SADS-PL) (Kaufman et al. 1997). Adolescents and parents were interviewed separately by trained clinicians. Clinicians assessed depression using the CDRS-R (based on adolescents and parents) and the Montgomery–Åsberg Depression Rating Scale (MADRS) (Montgomery and Asberg 1979). Both measures were included in the study because the CDRS-R is commonly used as an outcome measure in adolescent depression treatment studies, whereas the MADRS is commonly used in adult depression ketamine studies. Participants completed self-report measures, including the Beck Depression Inventory-II (BDI-II) (Osman et al. 2004), the Snaith–Hamilton Pleasure Scale (SHAPS) (Snaith et al. 1995) and the Temporal Experience of Pleasure Scale (TEPS) (Gard et al. 2006). Intelligence quotient was estimated using the Wechsler Abbreviated Scale of Intelligence (Wechsler 2011). A consensus meeting following the interviews integrated all available clinical information for diagnostic and inclusion finalization.
Ketamine infusions and ongoing assessments
Participants meeting inclusion/exclusion criteria were scheduled for six open-label ketamine infusions over the course of 2 weeks, starting the day after the pretreatment clinical assessment. Before each infusion, the clinician administered the MADRS, the Clinical Global Impressions (CGI) Scale (Guy 1976), and the Clinician-Administered Dissociative States Scale (CADSS) (Bremner et al. 1998); participants completed the BDI-II, SHAPS, and TEPS. Intravenous ketamine (0.5 mg/kg) was infused over 40 minutes, followed by a 2-hour monitoring period. For the first 5 participants, following Shiroma et al. (2014), dosing was based on ideal body weight, defined as follows: for male participants, ideal body weight = 39.0 + [2.27 × (height in inches −60)], and for female participants, ideal body weight = 42.2 + [2.27 × (height in inches −60)]. Since none of these initial participants was responders, due to concern about potential underdosing of this adolescent sample (especially those who are overweight), the dosing strategy was changed to use actual body weight. Vital signs (heart rate, blood pressure, respiratory rate, and oxygen saturation as measured by pulse oximetry) were collected at baseline and every 15 minutes throughout the infusion and monitoring period. The CADSS was repeated directly following the infusion, at 1 and 2 hours postinfusion. Assessment of depression symptoms at 2 hours postinfusion included the MADRS, CGI, and BDI-II. Posttreatment assessment for response was conducted 1 day following the final infusion, and consisted of the CDRS-R, MADRS, CGI, BDI-II, SHAPS, and TEPS. Responders were invited to participate in 6 weekly follow-up visits and a 6-month final visit; during the naturalistic follow-up period, all clinical care was directed by the participants' usual providers.
Outcome measures
The primary outcome measure was percent change in depression symptoms as measured by the CDRS-R. Percent change was calculated using the formula: (baseline raw CDRS-R − posttreatment raw CDRS-R)/(baseline raw CDRS-R − 17) (Tao et al. 2009); treatment response was defined as at least a 50% reduction in depression symptoms. Remission was defined as CDRS-R score ≤28. Relapse was defined as a CDRS score ≥50% of the pretreatment baseline (in other words, surpassing the threshold required to define response). Secondary outcome measures included MADRS, BDI-II, SHAPS, TEPS, and CGI severity scores at posttreatment, and CADSS and vital sign measurements during infusions.
Statistical analyses
Descriptive analyses of demographic and clinical data were conducted using one-sample t-tests and χ2 tests for continuous and categorical variables, respectively. The number of treatment responders was counted. We conducted paired t-tests on the primary and secondary outcome measures. Adverse events were documented. To explore response predictors, we conducted a series of linear regression analyses using CDRS-R percent change scores as the continuous outcome variable to test the following clinical and demographic variables: age, sex, age of depression onset, duration of illness, baseline severity scores (CDRS-R, BDI, SHAPS, and TEPS), number of past medication trials, and history of trauma (a dichotomous variable derived from the K-SADS-PL). Follow-up analyses of significant and trend effects included independent sample t-tests of CDRS-R change between subgroups defined by the presence or absence of the categorical factors identified in the prediction regression analyses and χ2 tests.
Results
Participants
Figure 1 summarizes the study participant flow. Thirteen adolescents completed the clinical trial. Table 1 summarizes their demographic and clinical characteristics.
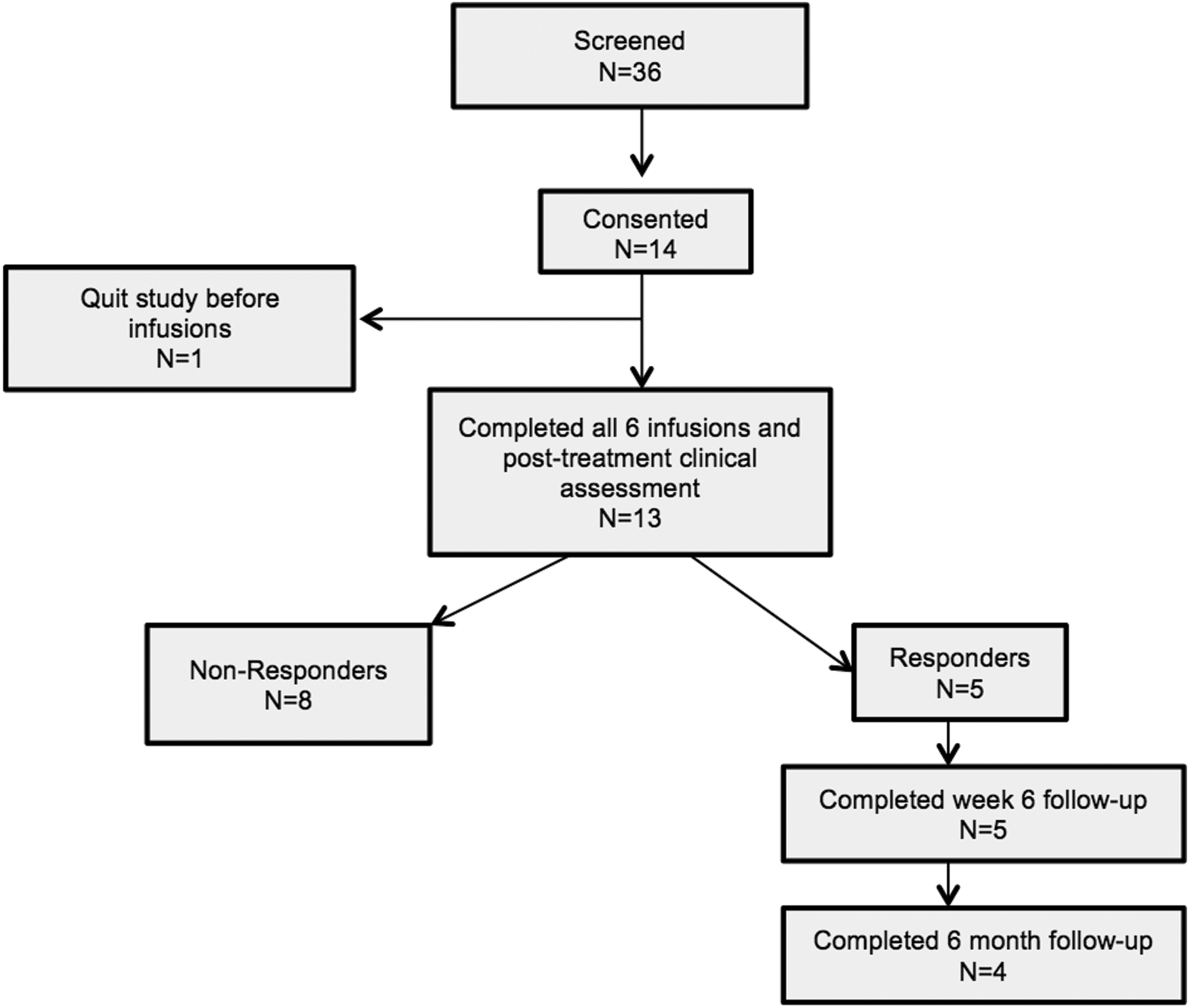
Consort diagram summarizing subject flow through the study. We completed initial screening with parents of 36 adolescents. Four participants were screened out due to presence of exclusionary diagnoses, insufficient antidepressant history, or recent medication changes. Parents of 18 adolescents chose not to participate for a variety of reasons, including travel costs, time burden, and safety concerns. Fourteen adolescents completed the consent process and diagnostic interview; one dropped out before receiving infusions. Thirteen adolescents completed all six infusions and posttreatment assessment. Responders were invited back for follow-up visits to measure time to relapse. All five responders completed the week 6 follow-up visit; four of five responders completed the 6-month visit.
One of the biologically female subjects reported she identified as male.
CDRS-R, Children's Depression Rating Scale-Revised; BDI-II, Beck Depression Inventory-II; MADRS, Montgomery–Åsberg Depression Rating Scale; SD, standard deviation.
Improvement in depression symptoms
Table 2 summarizes the changes from baseline in depression scores for primary and secondary outcome measures on the day following the final infusion. Changes in CDRS-R, MADRS, BDI-II, and CGI were significant; anhedonia symptom changes (SHAPS, TEPS) were not significant. Average CDRS-R percent change was 42.5% (standard deviation [SD] = 31%). Five participants (38%) met criteria for response; three of these responders were also in remission posttreatment, two of whom were still in remission at 6-weeks; a third responder who was not quite in remission at posttreatment did reach remission at 6 weeks; the other two responders relapsed at 1 and 2 weeks, respectively. Four of the five responders returned for the 6-month follow-up visit, of whom two participants were in both response and remission. Supplementary Figure S1 (Supplementary Data are available online at
The CDRS-R was the primary outcome measure of this study.
Baseline SHAPS and TEPS data were missing for one subject.
CDRS-R, Children's Depression Rating Scale-Revised; BDI-II, Beck Depression Inventory-II; MADRS, Montgomery–Åsberg Depression Rating Scale; SHAPS, Snaith–Hamilton Pleasure Scale; TEPS, Temporal Experience of Pleasure Scale; CGI, Clinical Global Impression; SD, standard deviation.
Adverse effects
Transient blood pressure changes were observed (Fig. 2). No significant changes in heart rate, respiratory rate and oxygen saturation were observed. CADSS scores were elevated immediately after each infusion (stronger effects for earlier infusions) but returned to baseline by the 1-hour assessment (Fig. 3). Two participants reported feeling uncomfortable (dysphoria) during the infusion. Three participants reported nausea (one vomited), which was treated with ondansetron. One participant reported hand pain related to repeated intravenous catheter placements that lasted several days following the final infusion. No patients experienced respiratory adverse effects. One participant, who had a high level of suicidal thinking at baseline, reported a high level of suicidality throughout the study. While at posttreatment, she expressed that she felt the medication worsened her suicidal thoughts, the clinical assessments did not reveal a change in suicidal thinking (ceiling effect).
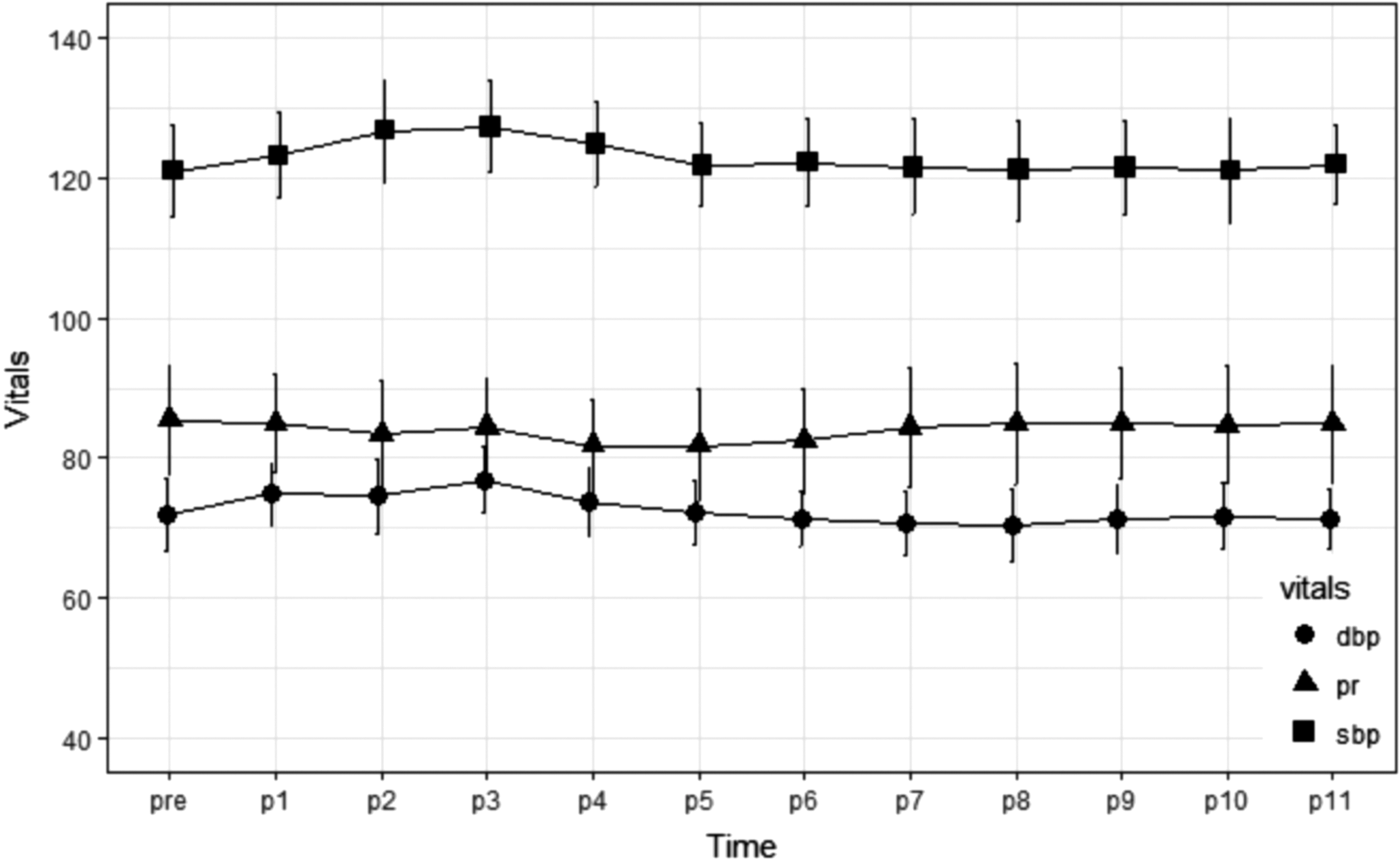
Mean blood pressure and heart rate, averaged over all six infusions. Maximum elevations of systolic blood pressure were at 30 minutes (mean increase from baseline of 6.8 mmHg) and 45 minutes (mean increase 7.3 mmHg) from the beginning of the infusion. Maximum increase in diastolic blood pressure was 5.1 mmHg, 45 minutes from beginning of infusion. There were no elevations in heart rate or blood pressure during the study that required intervention.
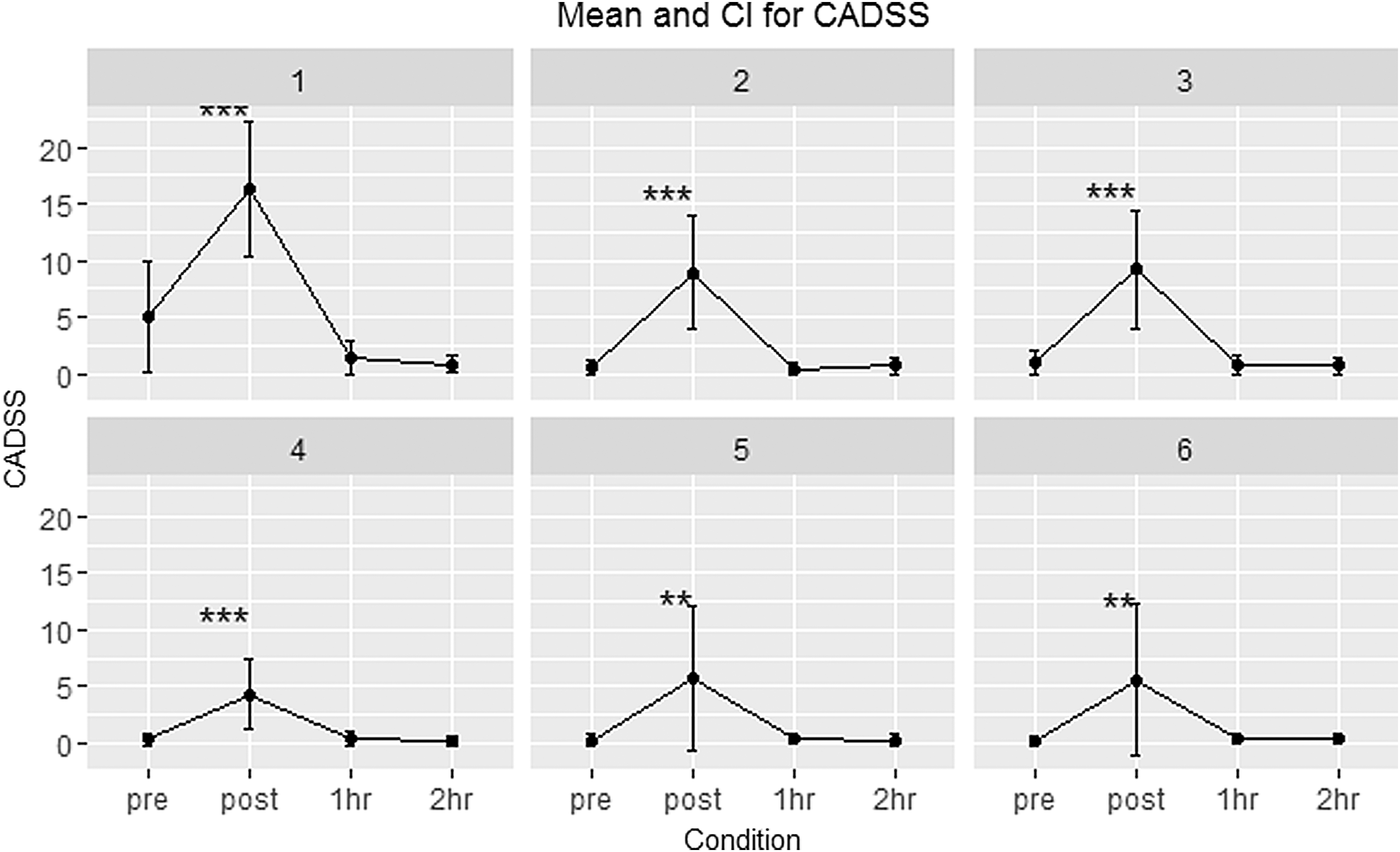
CADSS scores across the six infusions. Total CADSS scores are shown before and immediately after the 40-minute infusion, and 1 and 2 hours later. Significant elevations from baseline are denoted by ***p < 0.01 or **p < 0.05. CADSS, Clinician-Administered Dissociative States Scale.
Exploratory analyses: predictors of clinical response at posttreatment
Significant predictors of response included actual ketamine dose (F = 8.84, p = 0.01) and BMI (F = 6.28, p = 0.03). Dosing strategy (actual versus ideal body weight) had a trend-level effect in predicting clinical response (F = 4.43, p = 0.06); participants receiving actual body weight dosing had greater CDRS-R percent change scores than those receiving ideal body weight dosing (t = 2.3, p = 0.04; mean percent CDRS change for actual body weight group 55% [SD 31%]; mean percent CDRS change for ideal body weight group 22% [SD 21%]). None of the five participants receiving ideal body weight dosing strategy was responders; five out of the eight patients receiving actual body weight dosing were responders (chi squared = 2.79, p = 0.10). Trauma history had a trend (p = 0.15) effect for predicting treatment response; clinical improvement was greater in those without versus those with trauma history (mean CDRS percent change in those without trauma history was 60.2% [SD 26.1%], mean CDRS-R percent change in those with trauma history was 21.9%, [SD 24.2%; t = 2.74, p = 0.02). No significant effects for predicting treatment response were observed for age, sex, intelligence quotient, number of past medications, age of depression onset, duration of current episode, or baseline severity (CDRS-R, BDI-II, SHAPS, TEPS scores).
Discussion
Ketamine research has generated considerable excitement because of its rapid-acting antidepressant effects in adults with TRD (Ibrahim et al. 2011; Murrough et al. 2013; Zarate et al. 2013). To our knowledge, this represents the first report on the use of ketamine as a treatment for adolescent TRD. Since adolescence is a time period notable both for onset of depression and ongoing neurodevelopment (Giedd et al. 1999; Paus et al. 2008; Raznahan et al. 2011) it represents a critical window to intervene and restore healthy developmental trajectories. In this study, six serial infusions of open-label ketamine were associated with a significant decrease in depressive symptoms. Five adolescents (38%) met criteria for clinical response and remission, with three of these responders showing sustained remission at 6 weeks. Ketamine infusions were generally well tolerated. Finally, our results suggest a possible dose–response relationship for ketamine's impact on depression symptoms in adolescents.
The rate of response to ketamine in this adolescent study was lower than what has been observed in adult TRD studies (Fond et al. 2014; Newport et al. 2015; Xu et al. 2016). One reason for this could be developmental; earlier onset of depression tends to be associated with a more severe course (Cullen et al. 2009); when TRD emerges early in life, it may reflect a distinct pathophysiology requiring more extensive treatment to remedy underlying neuropathologies. A second consideration is that in this study, the first five patients (all nonresponders, four overweight) received smaller doses because our initial dosing strategy used ideal body weight. In that subsample, mean dose was 29.3 mg; mean dose divided by actual weight was 0.35 mg/kg. After the switch to dosing based on actual body weight, five of eight participants were responders. Thus, while ideal body weight dosing may be sufficient for adults (Shiroma et al. 2014), this strategy may not be optimal for adolescents. The current findings add to past research showing that rates of response in children and adolescents to other antidepressants do not always match what is observed with adult depression (Lakhan and Hagger-Johnson 2007).
In this study we observed that participants who received higher doses (due to having a higher BMI) had the best responses. This preliminary finding suggests a possible dose–response relationship for ketamine's effect on depression symptoms in adolescents with TRD, adding to previous reports from adults that 0.5 mg/kg was superior to lower doses (0.1–0.4 mg/kg) (Xu et al. 2016) and that dose escalation from 0.5 to 0.75 mg/kg was effective in some patients (Cusin et al. 2017). It is important to note that to achieve a dissociative state, pediatric patients require higher doses (1.5–2.0 mg/kg in comparison to 1 mg/kg for adults (Green et al. 2011), with adolescents having similar requirements as children (Kannikeswaran et al. 2016); therefore, appropriate dose for achieving antidepressant response in adolescents may be similarly higher. Future research is needed to identify the optimal dose for adolescents with TRD.
The optimal schedule for ketamine administration remains unknown. Recent evidence suggests that serial ketamine administrations may be more effective and lasting than single administrations (aan het Rot et al. 2010; Murrough et al. 2013; Shiroma et al. 2014). In one adult TRD study, response rates increased over the six infusions to reach a 92% cumulative response rate (Shiroma et al. 2014). While our results did not support a pattern of progressive improvement over the six infusions (Supplementary Fig. S1), it may be that repeated infusions contributed to the sustained remission observed in three of our subjects. Further research is needed to identify the optimal treatment regimen for acute treatment of adolescent TRD.
Identification of significant predictors of treatment response to ketamine is a critical step toward future personalized medicine approaches. Although a history of trauma was not a significant predictor of response, similar to past research showing that a history of trauma is a negative prognostic indicator of treatment response (Lewis et al. 2010; Shamseddeen et al. 2011), we found that those with a trauma history showed less reduction in depression than those without a history of trauma. Larger samples will be required to more formally test clinical predictors of ketamine response in adolescents.
Similar to past reports (Wan et al. 2015), we found a low rate of adverse events. As expected, ketamine infusions were associated with transient dissociative symptoms and hemodynamic changes. The safety of short-term use of ketamine for anesthesia, analgesia, and sedation in clinical settings is well established (Reich and Silvay 1989). Due to its efficacy and positive safety profile, ketamine is the most commonly administered sedative/analgesic for children in North America undergoing painful emergency department procedures (Green et al. 2011; Bhatt et al. 2017). Following anesthetic doses of ketamine, follow-up studies (up to 4 months) have not identified adverse effects on psychological functioning (Moretti et al. 1984). However, very little is known about the long-term efficacy or safety of ongoing, maintenance ketamine treatments. Currently, the field is limited to a handful of case reports of using maintenance strategies in adults with depression over 1–2 years (Cusin et al. 2012; Hassamal et al. 2015; Messer and Haller 2017). As the field continues to explore ketamine as a treatment for depression, significant knowledge gaps regarding long-term safety of continued ketamine treatment should be addressed (Short et al. 2017).
In this study, we observed a very low rate of attrition (at least during the treatment visits); all of those adolescents who received one infusion went on to complete all six infusions. This is somewhat surprising given the presence of some adverse events as noted above, especially for those adolescents that showed no clinical improvement throughout the study. The low attrition for treatment visits and the first posttreatment clinical assessment could reflect strong commitment to the study from patients and parents based on their intimate knowledge of the importance of research investigating new treatments for adolescent TRD. It could also reflect hopes and expectations on the part of patients and families for what ketamine treatment could deliver, based on the reports around that time in public media avenues on the promise of ketamine for depression. Finally, more than half of our patients that entered our study did not reside locally and had traveled from other locations to participate; the process of setting aside the time and financial investment for travel may have increased the commitment to follow through on the entire study.
When considering ketamine as a treatment for adolescent depression, safety concerns take center stage. One question raised by parents inquiring about our study was about the risk for inducing a substance use disorder. Little information is available to address this question. One study that assessed participants 1 week to 6 months following participation in single-dose ketamine studies found no reports of ketamine cravings, psychological, or medical problems (Perry et al. 2007). Patients with a history of substance abuse may have increased vulnerability to drug cravings as a result of underlying neuroadaptations in reward circuits (Scofield et al. 2016). To limit this risk, our study excluded adolescents with a current (past 6 months) diagnosis of substance abuse disorder. Notably, in the context of drug abuse, ketamine doses ranged from 100 to 2500 mg per use (Liao et al. 2016) (3 to 65 times greater than the average dose in our study). Future research is needed examining long-term risk of low-dose ketamine exposure for inducing or worsening substance abuse. A second safety concern is the possible risk for ketamine-induced neurotoxicity. As reviewed by Zhu et al. (2016), evidence from animals and humans suggest that higher ketamine doses (e.g., 5–160 mg/kg), especially with chronic exposure, can lead to neurotoxic effects; early developmental periods (prenatal and neonatal) have particularly high risk. Since adolescence represents a time period of ongoing neurodevelopment and vulnerability, the risks associated both with treatment and with progression of illness due to ineffective treatment must be carefully assessed and considered together.
Limitations of this study should be considered. First, the single-arm, open label design precludes conclusion that the results are due to drug effect versus expectation effects of (placebo) or regression to the mean. These concerns may be attenuated in this sample: regression to the mean may be less of a concern in participants with a history of severe and persistent depression, and placebo effect could be less in those with multiple past treatment failures. Furthermore, our study's finding of a dose–response relationship may in part ameliorate concerns regarding expectation or regression to the mean. On the other hand, factors such as the requirement of an intravenous catheter and the excitement from the popular press surrounding ketamine during this time period may have enhanced adolescent and parent expectancies. In any case, randomized, placebo-controlled studies are needed to confirm the preliminary findings reported in this study. Second, this study was not designed to identify optimal dose; further work is needed to formally delineate the dose–response relationship in adolescent TRD, and to guide dose optimization in these patients. Third, the small sample size limited the external validity of the study (i.e., our sample may not be fully representative of adolescent TRD) and limited power to examine important potential predictors of response. Finally, this study only examined acute treatment of adolescent TRD, whereas in clinical practice, strategies to sustain response and remission are needed. Future work is needed to address ongoing questions about the efficacy and safety of ketamine as a maintenance treatment, or of other strategies to maintain ketamine-induced clinical improvement.
Conclusion
Novel interventions are urgently needed to address adolescent TRD. Ketamine's biological effects may serve to enhance neuroplasticity (Liu et al. 2017). Given the potentially enhanced neuroplasticity inherent to ongoing development (Ismail et al. 2017), the adolescent period may be particularly amenable to such an intervention. The preliminary results reported here are promising; but large-scale, double-blind, randomized control designs are needed to determine if ketamine is a safe and effective treatment for adolescent TRD. Important questions remain regarding optimal dose, response prediction (patient selection), and long-term safety following acute treatment. Furthermore, in adolescent TRD, relapse and recurrence is the norm; therefore, achievement of acute remission is not sufficient for clinical practice. Before ketamine can be considered for broader clinical use, efficacy and safety data are needed on strategies to sustain ketamine-induced remission. Ultimately, safe and effective strategies to achieve sustained remission during adolescence could restore healthy neurodevelopment and improve outcomes over the lifespan.
Clinical Significance
This study examined open-label intravenous ketamine as an intervention for depression in 13 adolescents who had failed multiple prior treatments. Research in adults with TRD has demonstrated ketamine's rapid antidepressant effects, but this has not been examined in adolescents. Adolescence is notable for depression onset and ongoing neurodevelopment, and represents a critical time for successful intervention. This study provides the first evidence for intravenous ketamine as an intervention for TRD in adolescents. The findings suggest that ketamine may be effective for some but not all adolescents with TRD, and provide preliminary evidence for a dose–response effect.
Footnotes
Acknowledgments
The authors would like to thank the adolescents and families who volunteered to participate in this study. They also gratefully acknowledge the kindness, generosity, and impeccable care of their patients from the nurses and staff at the Pediatric Specialty Care Journey Clinic (University of Minnesota Masonic Children's Hospital) where the ketamine infusions took place.
This research was supported by the National Institutes of Health's National Center for Advancing Translational Sciences (UL1TR002494), the Biotechnology Research Center (P41 EB015894), the NINDS Institutional Center Core Grants to Support Neuroscience Research (P30 NS076408), the High Performance Connectome Upgrade for Human 3T MR Scanner (1S10OD017974-01), and the University Foundation, Amplatz Scholarship.
Disclosures
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.