
Abstract
Objective:
To perform a systematic review and meta-analysis of studies investigating predictors of medication adherence in children and adolescents with severe mental illness (SMI).
Method:
A systematic literature search was conducted in PubMed/MEDLINE, Web of Science, and PsycINFO from 1980 through October 1st, 2017, for original peer-reviewed articles that investigated predictors of adherence to psychopharmacologic treatment among children (≤18-years-old) with a primary psychotic disorder, bipolar disorder, depression, recent suicide attempt, or psychiatric hospitalization. Effect sizes (ESs) for individual predictors were extracted and combined using DerSimonian-Laird random-effects meta-analysis. Meta-regression and moderator analyses were conducted to investigate subgroups. This review complied with Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement guidelines.
Results:
A total of 28 studies (n = 180,870) met inclusion criteria; 65.9% (±20.9%) of children and adolescents with SMI were medication adherent. Adherence was associated with patient and family attitudes toward care, adherence to psychotherapy, and insight. Nonadherence was associated with illness severity, substance use, and attention-deficit/hyperactivity disorder. Heterogeneity was moderate-to-large for most ES estimates (I 2 > 50%). Age, sex, underlying diagnosis, and study methodology emerged as significant moderators.
Conclusion:
Medication nonadherence among youth with SMI is highly prevalent. Children and adolescents with more severe illness and higher comorbidity burden are at greater risk for nonadherence. Positive interpersonal care processes and adherence to nonpharmacological treatment may be protective. These findings inform development of a risk profile for nonadherence among youth with SMI. Future prospective research is needed to address the shortcomings in the existing literature and inform interventions to improve adherence.
Introduction
N
For youth with severe mental illness (SMI), pharmacotherapy is an essential component of treatment (Moreno et al. 2007) and ongoing maintenance therapy is indicated for lessening the rate of relapse of psychotic and bipolar disorders (McClellan 2013). Antidepressant treatment for at least 6 to 12 months is recommended for depressed youth whose symptoms do not respond adequately to psychotherapy (McClellan et al. 2007). For youth with SMI, long-term adherence to pharmacotherapy becomes tied to the maintenance of mental health (Munson et al. 2010). Nevertheless, among children and adolescents with SMI, the mean percentage of treatment time in full adherence is similar to that of youth with other chronic medical illnesses (e.g., 56% for antipsychotic and 53% mood stabilizer/anticonvulsant medications) (Patel et al. 2005), and adherence with long-term treatment decreases as the duration of treatment increases (Stine 1994). An improved understanding of the predictors of nonadherence in pediatric populations with SMI presents an opportunity to evaluate a highly prevalent and modifiable (susceptible to behavioral intervention), contributor to pediatric healthcare expenditures (McGrady and Hommel 2013). Contrary to other more stable predictors of healthcare use, nonadherence is potentially modifiable with behavioral intervention, and thus it is of clinical significance.
Findings from prior research examining predictors of psychotropic medication nonadherence among children and youth are mixed, and likely influenced by wide variation in study designs and methods. There are multiple challenges to understanding adherence among youth with SMI. First, measurement of adherence is variable and nonadherence is variably defined. Rates of adherence may be assessed by self-report or patient diaries (Burns et al. 2009), physician reports (Dean et al. 2011), parent reports (Pogge et al. 2005; DelBello et al. 2007; Munson et al. 2010; Gearing et al. 2016), pill counts (Bernstein et al. 2000; Nakonezny et al. 2010), electronic measures (e.g., recordings of dispensed medications), serum or urine assays (Dailey et al. 2005), pharmacy and medical chart records (King et al. 1997; Sleath et al. 2010; Bhowmik et al. 2013), and biological markers (Drotar et al. 2007). Definitions of adherence also vary between studies (e.g., 100% vs. 80% vs. 50% of doses). Such variation has produced a heterogeneous body of research.
Second, there are many possible predictors of adherence, and independent investigations have varied in the type of predictors assessed. Predictors of patient adherence include demographic variables (age, race, ethnicity, gender, and socioeconomic status) (Ghaziuddin et al. 1999; Yazdi et al. 2008; Sleath et al. 2010; Hui et al. 2014), comorbid conditions (anxiety disorders, attention-deficit/hyperactivity disorder (ADHD), substance abuse disorders, and chronic medical disorders) (Yazdi et al. 2008; Fontanella et al. 2011; Stewart and Baiden 2013; Goldstein et al. 2016), type of treatment (medication class and dosage, and treatment complexity) (Cornblatt et al. 2007; Fontanella et al. 2011), side effects (Pogge et al. 2005), patient attitudes (self-efficacy, medication attitudes, and fear of rehospitalization) (Pogge et al. 2005; Molteni et al. 2014; Pérez-Garza et al. 2016), parent attributes (family dysfunction, family history of mental illness, and family beliefs surrounding treatment) (Coletti et al. 2005; Pérez-Garza et al. 2016), severity of illness and syndromic recovery (Coletti et al. 2005; DelBello et al. 2007), concurrent psychotherapy (Evans-Lacko et al. 2010), and interpersonal factors (positive relationship with clinician and contact with providers) (Patel et al. 2005; Fontanella et al. 2011; Pérez-Garza et al. 2016).
Multiple recent narrative and systematic reviews have attempted to synthesize this literature (Hack and Chow 2001; Hamrin et al. 2010; Staton 2010; Iizuka and Hodes 2015; Leclerc et al. 2015; Häge et al. 2016). However, to our knowledge, no quantitative meta-analytic investigation has ever been conducted. Empirical investigation of predictors of nonadherence is paramount to the development of data-driven models of pediatric adherence. To more clearly delineate factors related to psychotropic medication nonadherence, we conducted a systematic review and random-effects meta-analysis of studies that assessed predictors of medication adherence among children and adolescents with SMI. We define SMI as a primary diagnosis of a psychotic disorder, affective disorder (major depressive disorder or bipolar disorder), recent suicide attempt, or recent psychiatric hospitalization. We anticipated a high degree of heterogeneity between studies given the substantive and methodologic variation of the preexisting literature. Thus, we also aimed at exploring potential sources of heterogeneity by subgroup analyses and meta-regression. We sought to identify variables associated with patient adherence. Of note, the included studies varied on methodology, including whether the variable of interest was antecedent to measured adherence. Thus, although the term predictor is used, no causal or unidirectional inference is made.
Method
We conducted a meta-analysis of empirical studies measuring predictors of psychotropic medication adherence among children and adolescents with SMI. The study methodology followed a protocol consistent with other published meta-analyses of predictors of patient adherence (e.g. DiMatteo et al. 2000) and was defined, as below, a priori to data collection. We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines (Moher et al. 2009). The proposed methodology was registered in PROSPERO (Booth et al. 2013) in anticipation of analyses (Registration No.: CRD42017083252). Studies were selected using strict eligibility criteria and predefined constructs. The literature was screened for eligibility and selected for inclusion by two independent reviewers.
Search strategy
We conducted a systematic search of PubMed/MEDLINE, Web of Science, and PsycINFO databases from 1980 through October 1st, 2017. The literature search was restricted from 1980 onward to utilize the operationalized diagnostic criteria for psychotic and mood disorders of the Diagnostic and Statistical Manual of Mental Disorders, 3rd Edition (American Psychiatric Association 1980). The reference lists of eligible studies were tracked by Google Scholar and reviewed for further relevant studies. We used a two-component search term string combined with the Boolean operator AND: (1) terms classifying medication adherence and (2) terms classifying SMI. Terms of each component within (1) or (2) were linked with “OR.” Using the Boolean operator NOT, we excluded studies of adults (unless data for children or adolescents were reported separately), animal studies, case studies, abstracts, books and book chapters, and non-English language journals. The thesaurus of the respective database was utilized to modify terms included in our search (schizophreni* OR schizoaffective OR psychosis OR psychotic OR bipolar OR manic OR mania OR depress* OR mood) AND (adhere* OR compliance) AND (adolesc* OR child*) (Supplementary Table S1; Supplementary Data are available online at
Study selection
We included English-language peer-reviewed empirical journal articles published from 1980 to 2017 that fulfilled the following inclusion criteria: (1) peer-reviewed articles where a sample size N was reported (therefore, dissertations, prepublication drafts, non-peer-reviewed journal articles, and book chapters were not included), (2) medication adherence to a prescribed psychopharmacological treatment regimen was measured, (3) quantitative articles where an effect size (ES) (or statistic from which an ES could be computed) was reported measuring the association of a predictor and psychopharmacological medication adherence, (4) studies in which adherence was empirically assessed, and (5) studies in which the design controlled for discontinuation of medication secondary to provider recommendation. We applied the following exclusion criteria: (1) studies that included children without SMI, (2) studies that only assessed medication adherence to nonpsychopharmacologic treatment regimens, (3) studies that only assessed adherence to psychotherapy, (4) studies that included participants from another age group (unless data were reported separately for children <18 years old).
Data extraction
The following items were extracted from each study: general information (author(s), year of publication, and year of data collection), sample size (size of adherent and nonadherent group), sample characteristics (age, gender, ethnicity, nationality, and socioeconomic status of participants), type of SMI (depression, bipolar disorder, psychotic disorder, or mixed), method of assessment of SMI (e.g., structured interview and preexisting diagnosis) and method of assessment of patient adherence (self-report, peer report, family report, physician report, pharmacy record, electronic medical record, insurance claim, or drug blood level), and criteria for categorical measures of adherence (e.g., 50%, 80%, or 100% of doses). For each study, we recorded a list of variables for which an association (or lack of association) with patient adherence was reported. Where reported, we extracted data on frequency of comorbid disorders.
Statistical analyses
Studies were combined if at least three independent data sets included the same predictor of patient adherence. Studies used different measurement methods and varied in their reporting of continuous and dichotomous data. For studies reporting continuous measures, standardized mean difference estimates, of difference in adherence between groups, were used as ES estimates (e.g., mean age of adherent participants vs. mean age of nonadherent participants). For studies reporting dichotomous measures, odds ratios (ORs) and standard error of log ORs were computed. For each study, we considered a two-by-two contingency table of medication adherence (adherent vs. nonadherent) and predictor (e.g., male vs. female). As converting from continuous to dichotomous data is less prone to errors (compared with dichotomous to continuous conversions) (Cox 1972), studies reporting standardized mean differences were then converted to ORs using the method described by Cox and Snell (1981).
To pool ES estimates, we used the DerSimonian-Laird (D-L) (Dersimonian and Laird 1986) inverse-variance weighted random-effects method of meta-analysis. The random-effects model of meta-analysis is the most generalizable and robust model of cumulative effect statistic, accounting for variability between studies and allowing for generalization beyond the sample population (Rosenthal 1991). The natural logarithmic transformation of OR and the standard error of the log OR were used to compute the pooled OR. As our analyses focus on prevalence, the 95% confidence intervals (CIs) reported for each pooled OR are reported along with the regression coefficient to represent the interval estimate of each population parameter. The Cochran Q, the weighted sum of the squares of the deviations of each study ES estimate from the overall estimate, and an assessment of heterogeneity of the included studies (Dersimonian and Laird 1986; Rosenthal 1991; Egger et al. 1997) were included in the D-L pooling method (Dersimonian and Laird 1986). To evaluate for publication bias, Begg's and Egger's tests (Harbord et al. 2009) were conducted, along with visual inspection of funnel plots for asymmetry.
Heterogeneity among included studies was quantified with the I 2 statistic, which measures the percentage of variation between studies secondary to heterogeneity rather than chance (Egger et al. 1997). As we expected heterogeneity between studies to be high, we anticipated subgroup and meta-regression analyses to identify sources of variation. We considered the following sources of heterogeneity in univariate meta-regression analyses: year of publication, type of SMI (psychotic disorder, bipolar disorder, major depressive disorder, or mixed sample), mean age, gender (percentage female), ethnicity (percentage white), and medication (percentage of study population prescribed antipsychotics, mood stabilizers, or antidepressants). The meta-regression analyses were run such that studies with more precise parameters (measured by sample size and 95% confidence interval [CI]) had a greater weight. Covariates were included in the meta-regression analyses when at least 75% of the included studies contained information on the covariate. The significance level was defined as alpha of 0.05.
Analyses were conducted with Stata IC Version 15.1 (StataCorp, College Station, TX) metan package (Sterne et al. 2008) and the Statistical Package for the Social Sciences (SPSS) 25.0 (IBM Statistics, Chicago, IL).
Results
Initial search of PubMed/MEDLINE, Web of Science, and PsycINFO databases yielded 14,601 records. Following application of initial exclusion criteria, 5283 articles were screened. After removal of duplicates, 550 unique full-text articles were reviewed for eligibility. Finally, 33 original studies met criteria for inclusion with report of prevalence data. Of these, 28 original studies provided ESs, or statistics from which an ES could be computed. The PRISMA flowchart for study selection is presented in Figure 1.

PRISMA flowchart of included studies. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Characteristics of included studies
The included studies (k = 28) provided data from 180,783 participants consisting of 543 youth with psychotic disorders (k = 6), 1744 with depressive disorders (k = 3), 6170 with bipolar disorders (k = 8), and 172,413 with mixed psychiatric conditions (k = 11). The mean age (weighted by N) of participants was 12.3 years (SD ±0.47). Participants were 45.4% female (data available for 27 studies) and 54.3% Caucasian (data available for 18 studies). The four diagnostic groups (psychotic disorders, depressive disorders, bipolar disorders, and mixed psychiatric) did not significantly differ in age (F(3,22) = 1.52, p = 0.23), sex (F(3,23) = 1.64, p = 0.21), and ethnicity (F(3,14) = 2.97, p = 0.07). Screening of the included studies yielded unique 59 predictors of patient adherence, of which 18 predictors were meta-analyzable with an ES reported in k ≥ 3 independent datasets. Table 1 presents summary statistics for each predictor of adherence. Descriptions of predictors and characteristics of included studies are presented in Supplementary Table S2 and Supplementary Table S3, respectively.
Statistically significant results are in bold.
ESs for the individual test measures are in the original test direction (i.e., an OR greater than one indicates that adherence is higher in the group of interest, whereas an ES smaller than zero indicates that the adherence is decreased).
DerSimonian-Laird random effects pooled OR with lower and upper 95% CI.
p < 0.05.
p-value in Egger test for publication bias.
ES, effective size; CI, confidence interval; OR, odds ratio.
Comorbid conditions
Alcohol use
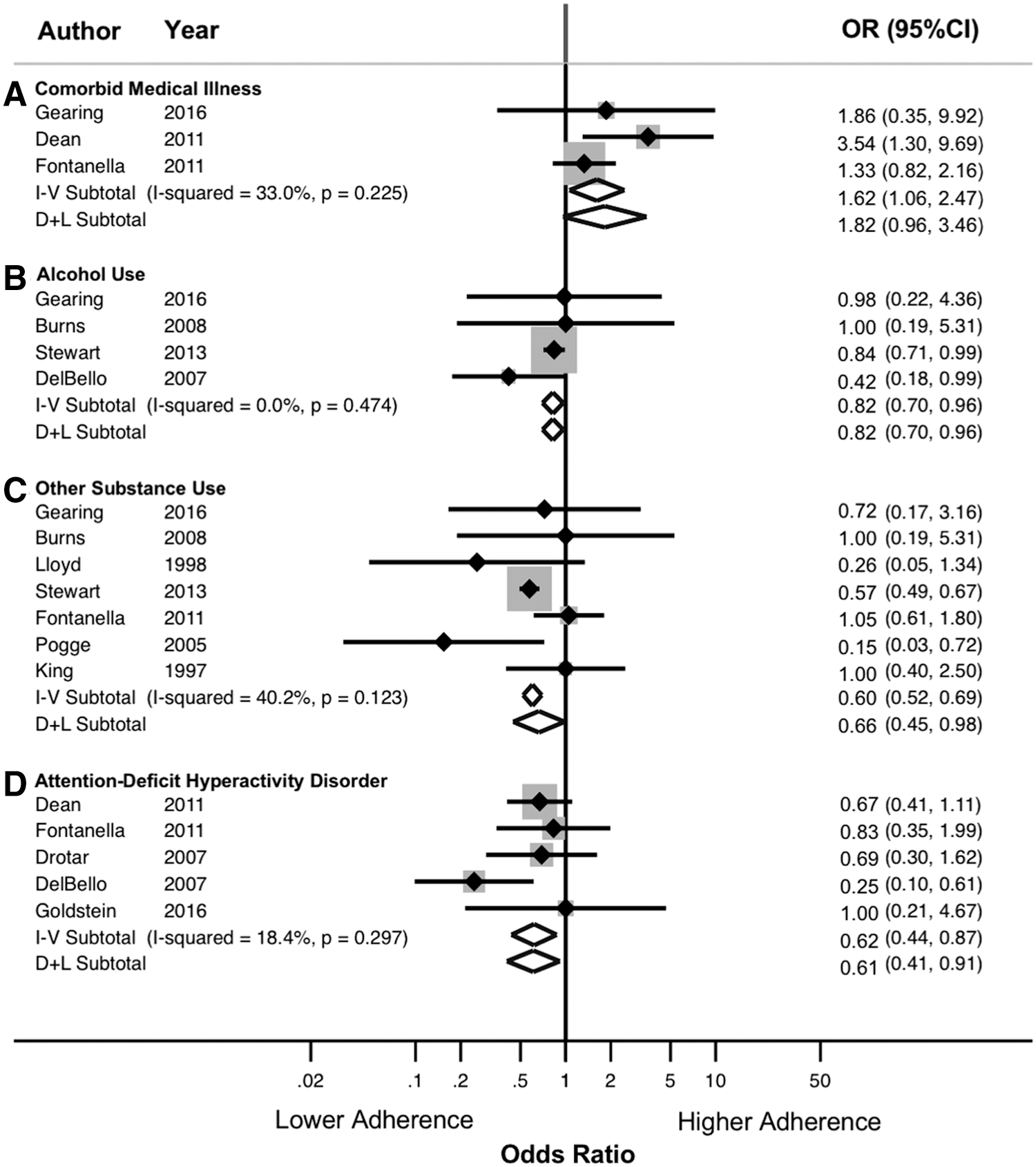
Four studies provided a separate ES for the relationship between alcohol use and medication adherence. Youth with an alcohol use disorder were at significantly higher risk of medication nonadherence compared with those without an alcohol use disorder (D-L Pooled OR 0.82; 95% CI 0.70–0.96, k = 4) (Table 1 and Fig. 2A). Heterogeneity was low (I 2= 0.00%). Subgroup analyses suggested that the relationship between alcohol use and adherence was moderated by diagnosis, wherein studies of youth with psychotic disorders tended to find a negative relationship between alcohol use disorders and adherence. However, this relationship did not reach statistical significance for studies with youth with bipolar disorders or mixed psychiatric diagnoses (Supplementary Table S5).
Forest plots for ORs and 95% CIs for
Substance use
Seven studies provided extractable data for comorbid substance use. Youth with comorbid substance use were at significantly higher risk for nonadherence compared to youth without comorbid substance use (D-L Pooled OR 0.66; 95% CI 0.45–0.98, k = 7) (Table 1 and Fig. 2B). Heterogeneity was moderate (I 2 = 40.2%). Subgroup analyses suggested that substance use was associated with poorer adherence in studies that considered mixed psychiatric diagnoses, but not in studies of patients with psychotic or depressive disorders. Furthermore, substance use was associated with poorer adherence in studies that defined adherence by child self-report, but not in studies that defined adherence by parent report, pill count, or combination measures. Among studies defining adherence as child self-report, heterogeneity was low (Supplementary Table S5).
Attention-deficit/hyperactivity disorder
Youth with comorbid ADHD were at significantly higher risk for nonadherence (D-L Pooled OR 0.61; 95% CI 0.41–0.91, k = 5) (Table 1). Figure 2C presents the forest plot for this meta-analysis. Heterogeneity was low (I 2 = 18.4%). The increased risk was not moderated by sample size, gender, ethnicity, or mean age of the sample (Supplementary Table S4). Subgroups of studies (when divided by diagnosis and measure of adherence) were not significantly different (Supplementary Table S5, Supplementary Material).
Medical illness
Three studies provided extractable data for comorbid medical illness. Heterogeneity was low (I 2 = 33.0%). No significant difference in adherence between youth with and without comorbid medical illness was observed (Table 1 and Fig. 2D). Meta-regression and subgroup analyses were not statistically significant (Supplementary Tables S4 and S5).
Treatment characteristics
Antipsychotic medications
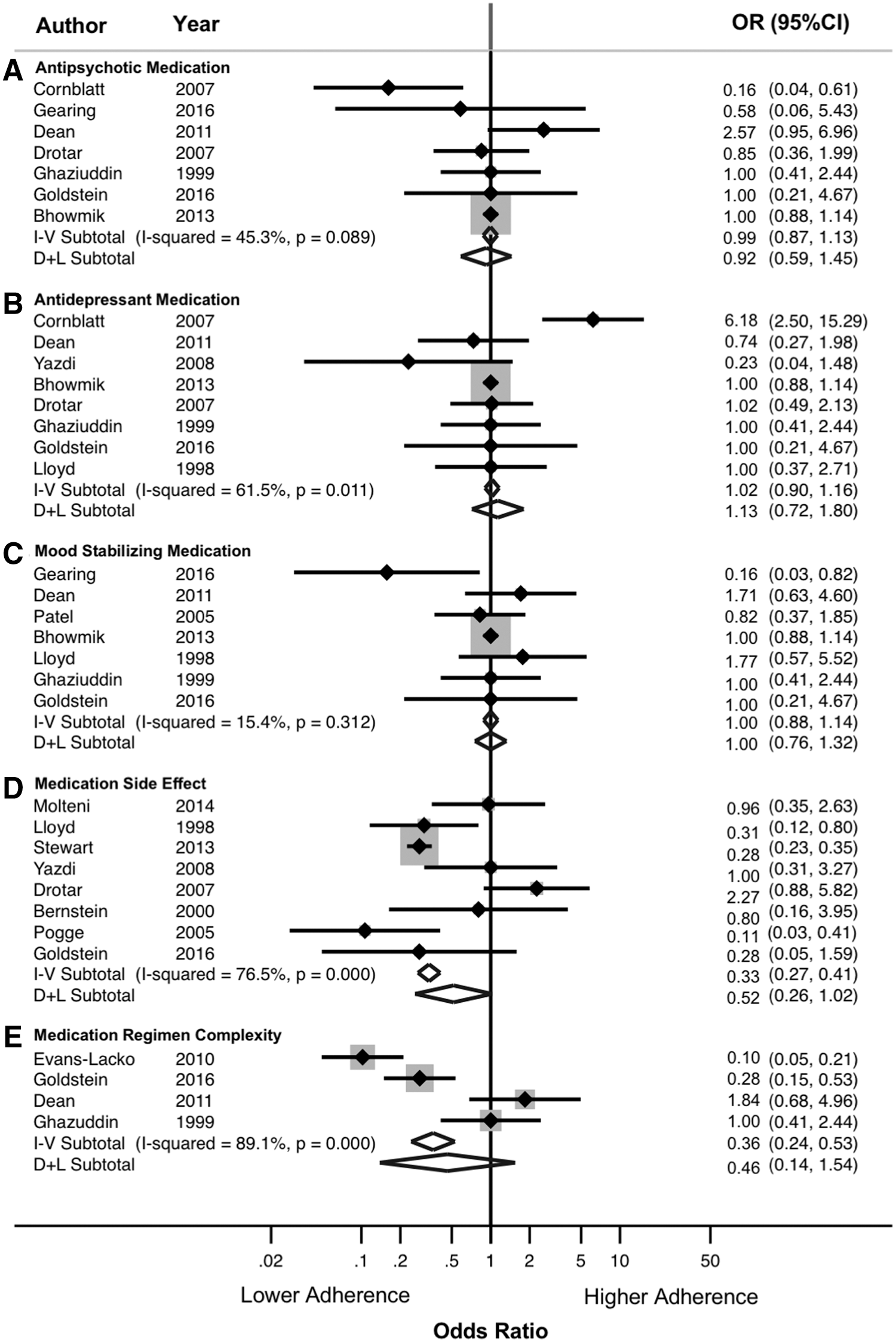
Seven studies provided extractable data for antipsychotic medications. Heterogeneity was moderate (I 2 = 45.3%) (Table 1). No significant difference in adherence between youth treated with antipsychotic medication and those treated with other psychotropic medications was observed (Fig. 3A). Subgroup analyses suggest that studies with patients with psychotic disorders tended to find a negative relationship between antipsychotic medication use and patient adherence (i.e., being prescribed an antipsychotic was associated with nonadherence) (Supplementary Table S5).
Forest plots for ORs and 95% CIs for
Antidepressant medications
Seven studies provided extractable data for antidepressant medications. Heterogeneity was moderate (I 2 = 61.5%). No significant difference in adherence between youth treated with antidepressant medication and those treated with other psychotropic medications was observed (Table 1 and Fig. 3B). Meta-regression and subgroup analyses were not significant. Of note, one study was excluded from this analysis (Fontanella et al. 2011) as the study compared types of antidepressant medications, rather than comparing antidepressant medication with another class of psychotropic medication.
Mood-stabilizing medications
Seven studies provided extractable data for mood-stabilizing medications. Heterogeneity was low (I 2 = 15.4%). No significant difference in adherence between youth treated with mood stabilizer medication and those treated with other psychotropic medications was observed (Table 1 and Fig. 3D). Meta-regression and subgroup analyses were not significant.
Medication side effect
Eight studies provided extractable data on rate of nonadherence among youth who experienced side effects of medications compared with youth who did not experience side effects. Experiencing side effects tended to be associated with increased risk of medication nonadherence (D-L Pooled OR 0.52, 95% CI 0.26–1.02, k = 8) (Table 1 and Fig. 3E). Heterogeneity was high (I 2 = 76.5%). Meta-regression analyses suggested that sample size and patient age moderated this relationship, wherein smaller studies and those with younger patients tended to find a stronger relationship between medication side effects and adherence (Supplementary Table S4). Although medication side effects were a risk factor for nonadherence among all diagnostic subgroups, this effect only reached significance for studies with mixed psychiatric samples. Moreover, studies in which patient adherence was operationalized as child self-report tended to demonstrate that medication side effects were associated with increased risk of nonadherence. However, this relationship was not significant for studies that defined adherence by other means (Supplementary Table S5).
Medication regimen complexity
Four studies provided extractable data on medication regimen complexity. No significant difference in adherence was observed between youth treated with more complex medication regimens compared with youth with less complex medication regimens (Table 1 and Fig. 3F). Heterogeneity was high (I 2 = 89.1%). Subgroup analyses suggest that medication regimen complexity is associated with higher risk for nonadherence among studies of patients with bipolar disorder. However, this relationship was not significant for studies with other diagnostic groups (Supplementary Table S5).
Interpersonal care processes
Patient attitudes about treatment
Eight studies provided extractable data on patient attitudes toward treatment. Youth with more positive attitudes toward treatment experienced higher rates of adherence compared with youth with less positive attitudes (D-L Pooled OR 3.41; 95% CI 1.50–7.77, k = 8) (Table 1 and Fig. 4A). Heterogeneity was high (I 2 = 77.9%). Meta-regression analyses suggested that study sample size moderated this relationship, wherein smaller studies tended to find that positive patient attitudes were associated with medication adherence. Subgroup analyses suggested that positive patient attitudes were associated with lower risk for nonadherence among studies that defined adherence by combination measures.

Forest plots for ORs and 95% CIs for
Family attitudes about treatment
Six studies provided extractable data on family attitudes about treatment. Youth from families with positive attitudes toward treatment experienced higher rates of medication adherence compared with youth from families with negative attitudes (D-L Pooled OR 2.82; 95% CI 1.79–4.45, k = 6) (Table 1 and Fig. 4B). Heterogeneity was high (I 2 = 80.0%). Egger test for publication bias was significant (p = 0.002). Meta-regression analyses suggested that sample size, gender, and age moderated this relationship. Studies with smaller samples, higher percentage of male patients, and younger patients tended to find that positive family attitudes toward treatment were associated with medication adherence (Supplementary Table S4). Subgroup analyses suggested that positive parent attitudes toward treatment are associated with higher adherence, and that this relationship remained significant when studies were divided into subgroups based on measure of adherence (with the exception of blood-level measures, which did not reach significance) (Supplementary Table S5).
Patient insight
Three studies provided extractable data on patient insight. Youth with more insight experienced higher rates of adherence compared with youth with less insight (D-L Pooled OR 3.60; 95% CI 1.40–9.10, k = 3) (Table 1 and Fig. 4D). Heterogeneity was high (I 2 = 87.9%). Meta-regression analyses suggested that study sample size moderated this relationship, wherein smaller studies tended to find that patient insight was associated with medication adherence (Supplementary Table S4). Subgroup analyses suggested that patient insight was associated with higher adherence among studies that defined adherence by combination measures and among studies that investigated mixed psychiatric populations (Supplementary Table S5).
Positive relationship with clinician
Three studies provided extractable data on patient relationship with clinician. Youth with more a positive clinician–patient relationship experienced higher rates of adherence compared with youth with a less positive relationship (D-L pooled OR 5.92; 95% CI 1.73–18.55, k = 3) (Table 1 and Fig. 4C). Heterogeneity was moderate (I 2 = 53.7%). Meta-regression analyses suggested that patient age moderated this relationship, wherein studies with older patients tended to find that positive relationship with clinician was more strongly associated with medication adherence (Supplementary Table S4).
Demographics
Age
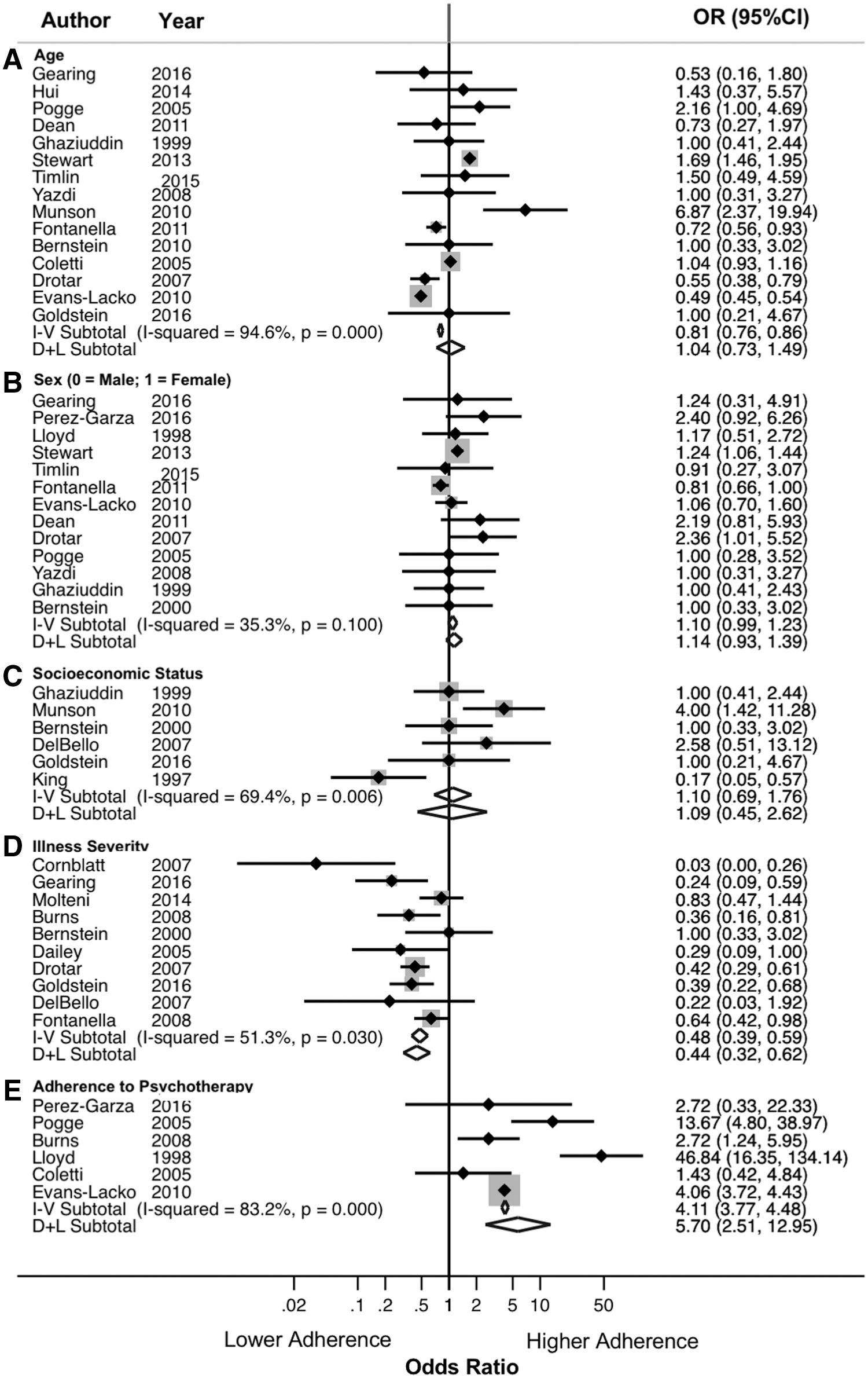
Overall, age was not significantly associated with medication adherence (k = 16) (Table 1). However, heterogeneity for the pooled OR was high (I 2 = 95.0%); thus, further analyses were conducted to identify methodological and substantive sources of heterogeneity. Figure 5A displays a forest plot of this meta-analysis. Meta-regression analyses indicated that gender moderated this relationship, wherein studies with a higher percentage of female participants found that older children were more likely to be adherent, compared with studies with fewer female participants (Supplementary Table S4). Subgroup analyses suggested studies operationalizing adherence as child self-report tended to find that older children were more likely to be adherent. However, studies that operationalized adherence by pill count or blood level tended to find that younger children were more likely to be adherent (Supplementary Table S5).
Forest plots for ORs and 95% CIs for
Sex/gender
Males and females did not differ significantly in rates of medication adherence (k = 12) (Table 1 and Fig. 5B). Heterogeneity was moderate (I 2 = 35%). Subgroup analyses suggest that studies with mixed psychiatric samples tended to find female patients to be more adherent than male patients; however, this relationship did not reach significance for studies investigating youth with psychotic disorders or bipolar disorders. Only one study assessed the relationship between gender and adherence in depressive disorders. In addition, studies that defined adherence as child self-report tended to find that female gender was positively associated with adherence (Supplementary Table S5).
Socioeconomic status
Six studies provided extractable data for socioeconomic status (k = 6) (Table 1 and Fig. 5C). No significant difference between youth of high and low socioeconomic status was observed. Heterogeneity was moderate to high (I 2 = 69.4%). Meta-regression and subgroup analyses were not significant (Supplementary Tables S4 and S5).
Illness severity
Eleven studies provided extractable data for illness severity. Youth with more SMI were less likely to be adherent to medication (D-L Pooled OR 0.44; 95% CI 0.32–0.62, k = 11) (Table 1 and Fig. 5D). Of note, studies varied in methodology with regard to timing of measure of illness severity relative to measure of medication adherence. Heterogeneity was moderate (I 2 = 51.3%). Subgroup analyses suggested that more severe illness was associated with lower adherence among studies that investigated youth with bipolar disorder (this relationship did not reach significance for studies investigating youth with depressive and psychotic disorders). Subgroup analyses also suggested that more severe illness was associated with lower adherence among studies that used combination measures of adherence (Supplementary Table S5).
Adherence to psychotherapy
Six studies provided extractable data on youth adherence to psychotherapy. Youth who were adherent to psychotherapy appointments experienced higher rates of medication adherence compared with youth who were not adherent to psychotherapy appointments (D-L Pooled OR 5.70; 95% CI 2.51–12.95, k = 6) (Table 1 and Fig. 5E). Heterogeneity was high (I 2 = 83.2%). Meta-regression analyses and subgroup analyses were not significant (Supplementary Tables S4 and S5).
Discussion
This meta-analysis provides evidence that nonadherence among youth with SMI is highly prevalent and specific variables associated with patient adherence are identifiable. Comorbid conditions, interpersonal care processes, illness severity, and adherence to psychotherapy emerged as predictors of adherence, although with residual heterogeneity. Patient demographics and class of prescribed medication are less predictive of adherence. Primary diagnosis and methodologic variables moderated predictors of adherence. These results are consistent with previous systematic reviews suggesting that adherence to psychotropic medication is multifactorial, and that many factors predicting adherence are modifiable (Hamrin et al. 2010; Leclerc et al. 2015). Previous studies have synthesized the literature using qualitative means, and conclusions regarding the influence of patient, environment, medication, family, and illness-related factors have been previously been limited by the methodologic and substantive variability of the preexisting literature (Häge et al. 2016). By contrast, the results of this meta-analytic investigation suggest that specific factors predicting psychotropic medication adherence among children and adolescence can be clearly identified.
This analysis has several limitations. First, heterogeneity of extracted ESs was high. Heterogeneity among studies of adolescent adherence to psychotropic medication has previously been cited as a limitation to synthesis of the literature (Häge et al. 2016). Therefore, potential sources of heterogeneity across studies were identified using random-effects meta-regression and subgroup analyses. Of note, results from meta-regressions should be interpreted cautiously due to the probability of type I error (Higgins and Thompson 2004). Meta-regression analyses allowed for investigation of the potential influence of patient-related factors that were not directly investigated with ES estimates in individual studies (e.g., ethnicity). Our results suggested that, for many predictors, patient age, gender, and sample size contributed to heterogeneity of ES estimates. In addition, meta-regression analyses suggested that ethnicity of the patient sample did not significantly modulate ES estimates, for any of the 18 predictors of adherence investigated in this analysis. These results support the notion put forward by previous literature, that studies of child and adolescent adherence are indeed heterogeneous in methodology and sample characteristics. Despite subgroup analysis, heterogeneity remained high for a few predictors of adherence (including adherence to antidepressant treatment, adherence to psychotherapy, and socioeconomic status). Therefore, in these cases, findings should be interpreted cautiously, and future prospective studies are needed to investigate the impact of these variables on adherence.
This study is correlational, and no causal inferences can be made. For example, illness severity is negatively associated with adherence. This may suggest that more severely ill patients are more likely to be nonadherent, and/or nonadherent patients are less likely to experience syndromic recovery. Moreover, the effects observed in our exploratory analyses may be confounded with other variables. Previous literature has suggested that the relationship between gender and adherence may be confounded with psychiatric comorbidity, such as comorbid substance use (Coldham et al. 2002). In our analyses, comorbid substance use was a significant risk factor for nonadherence. Gender did not significantly modulate this relationship. However, the converse could not be investigated, as studies reporting the relationship between gender and adherence did not report rates of comorbid substance use. Therefore, our conclusions are limited in that included studies did not provide consistent data on covariates.
The definition of adherence varied across studies, a limitation raised by other meta-analyses and systematic reviews of patient adherence (DiMatteo et al. 2000; Simpson et al. 2006). Our subgroup analyses suggest that the measure of patient adherence (patient report, parent report, blood level, pill count, and combination measure) explains ES heterogeneity for multiple predictors of adherence. For example, studies measuring adherence by patient report tended to find that older children were more adherent; however, studies measuring adherence by more objective measures (pill count or blood level) found that older children are less likely to be adherent. This may suggest that older children have a higher likelihood of reporting adherence to medication, but may not actually be more adherent.
In addition, our results suggest that diagnosis may account for variability in patient adherence. Comorbid ADHD, alcohol use, and substance use significantly increased risk of medication nonadherence among youth with SMI. Moreover, underlying primary diagnosis (i.e., psychotic vs. affective disorder) modulated predictors of adherence. For example, medication regimen complexity did not significantly predict nonadherence. However, when studies were divided by diagnosis, medication regimen complexity was associated with increased risk of nonadherence among patients with bipolar disorder. Of note, included studies were limited to those investigating youth with serious mental illness so as to mitigate heterogeneity of included studies and focus on a subset of patients at high risk for rehospitalization and acute service utilization. Our finding that underlying diagnosis moderates predictors of adherence suggests the importance of future work targeting youth with other disorders, including neurodevelopmental, obsessive-compulsive, and anxiety disorders.
Furthermore, medication type did not significantly predict adherence, except among studies investigating youth with psychotic disorders, which found that antipsychotic medications were associated with greater risk of nonadherence compared with other medications. These results suggest that the intersection of comorbidity profile and underlying primary psychiatric illness is important in understanding risk of nonadherence. Moreover, all studies investigated oral medications and none of the included studies identified predictors of adherence to long-acting injectable or depot medications.
Finally, measures addressing family-level factors varied across studies and merit further investigation. Our results suggest that family attitudes toward psychiatric treatment are significantly associated with rates of adherence, wherein youth from families with more positive attitudes experience higher levels of medication adherence. These results are consistent with previous studies of general pediatric populations (e.g., Drotar and Bonner 2009), emphasizing the role of family attitudes in improving medication adherence. Studies were highly heterogeneous and ES estimates were modulated by sample size, gender, age, and measure of adherence. Moreover, Egger's test of publication bias was significant upon pooling of studies that investigated family attitudes toward care, suggesting that statistically positive findings are more likely to be published, and therefore included in the meta-analysis. Therefore, these findings should be interpreted with caution and future prospective research in this area is needed. As this study focused on medications prescribed by mental health providers, further studies are needed to investigate predictors of adherence to psychopharmacologic regimens prescribed in primary care pediatric and integrated care settings.
Of note, previous systematic reviews of predictors of adherence among youth with SMI have included a mixture of adolescent and young adult patients. Our meta-analysis was restricted to children (younger than 18 years), thus allowing a more precise estimate of variables associated with adherence in this population. Furthermore, this meta-analysis includes twice the number of studies of previous systematic reviews (Timlin et al. 2015; Häge et al. 2016).
Conclusion
Medication nonadherence among youth with SMI is widespread. This analysis suggests that children and adolescents with more severe illness and greater comorbidity burden are at high risk for nonadherence. Positive patient and family perceptions of care and adherence to nonpharmacological treatment may be protective. Our findings inform development of a risk profile for nonadherence in this population.
Adherence has emerged as a critical factor in outcomes for patients with SMI. Children and adolescents experience a unique set of psychosocial and clinical experiences that vary significantly from adult populations. Children and adolescents with SMI are an especially high-risk population, for which a solid understanding of adherence is fundamental to ensuring appropriate treatment. Future prospective studies should investigate the intersection of family, individual, and sociodemographic variables with the goal of guiding interventions to improve pharmacologic treatment adherence for this population.
Clinical Significance
This meta-analysis has several research implications. First, our results indicate that comorbid ADHD and substance use increase risk for medication nonadherence among youth with SMI. Thus, appropriate treatment of these comorbidities may reduce risk for nonadherence. Second, modifiable interpersonal care processes, such as patient and family attitudes toward care and patient insight, significantly predict patient adherence. Third, in this analysis, demographic variables were not significantly associated with risk of nonadherence; however, age and sex did significantly modulate the relationship between predictors and rates of adherence. Therefore, more prospective studies are necessary to precisely define these relationships. There was a scarcity of data on patient race/ethnicity reported in included studies. Fourth, the literature on patient adherence would benefit from uniformity among the terminology for deviations from prescribed pharmacologic therapies. Finally, our results suggest that adherence to psychotherapy is associated with rates of medication adherence, although current studies have significant residual heterogeneity. Future research should seek to identify correlates of adherence to nonpharmacological treatment.
Footnotes
Acknowledgments
We would like to thank the UCLA Statistical Consulting Group for their help throughout the course of the work.
Disclosures
J.B.E. has nothing to disclose. No financial relationships exist with any pharmaceutical company. Dr. Zima has received research funding over the last 2 years from the Illinois Children's Healthcare Foundation, Patient-Centered Outcomes Research Institute, State of California Department of Healthcare Services, Mental Health Services Act, and Behavioral Health Centers of Excellence for California (SB852). No financial relationships exist with any pharmaceutical company.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.