
Abstract
Background:
Inflammation and immune dysregulation have been implicated in the pathogenesis of pediatric-onset obsessive-compulsive disorder (OCD) and tic disorders such as Tourette syndrome (TS). Though few replicated studies have identified markers of immune dysfunction in this population, preliminary studies suggest that serum immunoglobulin A (IgA) concentrations may be abnormal in these children with these disorders.
Methods:
This observational retrospective cohort study, conducted using electronic health records (EHRs), identified 206 children with pediatric-onset OCD and 1024 adults diagnosed with OCD who also had testing for serum levels of IgA. IgA deficiency and serum IgA levels in pediatric OCD were compared with IgA levels from children diagnosed with autism spectrum disorders (ASD; n = 524), tic disorders (n = 157), attention-deficit/hyperactivity disorder (ADHD; n = 534), anxiety disorders (n = 1206), and celiac disease, a condition associated with IgA deficiency (n = 624).
Results:
Compared with ASD and anxiety disorder cohorts, the pediatric OCD cohort displayed a significantly higher likelihood of IgA deficiency (OR = 1.93; 95% CI = 1.18–3.16, and OR = 1.98; 95% CI = 1.28–3.06, respectively), though no difference was observed between pediatric OCD and TS cohorts. Furthermore, the pediatric OCD cohort displayed similar rates of IgA deficiency and serum IgA levels when compared with the celiac disease cohort. The pediatric OCD cohort also displayed the highest percentage of IgA deficiency (15%,) when compared with TS (14%), celiac disease (14%), ADHD (13%), ASD (8%), and anxiety disorder (8%) cohorts. When segregated by sex, boys with OCD displayed a significantly higher likelihood of IgA deficiency when compared with all comparison cohorts except for celiac disease and tic disorders; no significant difference in IgA deficiency was observed between female cohorts. Pediatric OCD subjects also displayed significantly lower adjusted serum IgA levels than the ASD and anxiety disorder cohorts. Adults with OCD were also significantly less likely than children with OCD to display IgA deficiency (OR = 2.71; 95% CI = 1.71–4.28). When compared with children with celiac disease, no significant difference in IgA levels or rates of IgA deficiency were observed in the pediatric OCD cohort.
Conclusions:
We provide further evidence of IgA abnormalities in pediatric-onset OCD. These results require further investigation to determine if these abnormalities impact the clinical course of OCD in children.
Introduction
Obsessive-compulsive disorder (OCD) and tic disorders, such as Tourette syndrome (TS), are two common neurodevelopmental disorders that share a high degree of comorbidity and are characterized by repetitive thoughts, behaviors, or involuntary movements. Multiple lines of evidence suggest that cortico-striatal-thalamic-cortical circuit dysfunction may underlie the symptoms of both disorders (Singer 2013; Wood and Ahmari 2015) though their etiologies remain unknown. Recently, it has been proposed that a post-infectious autoimmune process directed against basal ganglia nuclei may result in OCD (Dale et al. 2005; Bhattacharyya et al. 2009; Nicholson et al. 2012) or tic symptomatology (Martino et al. 2015) in children; this phenomenon is termed Pediatric Autoimmune Neuropsychiatric Disorder Associated with Streptococcal infections (PANDAS) (Swedo et al. 1998), or Pediatric Acute Onset Neuropsychiatric Syndrome (PANS) (Frankovich et al. 2015). While evidence for this mechanism remains incomplete, additional evidence suggests that immune dysfunction may be etiologically related to OCD or tic pathology irrespective of the hypothesized mechanism involved in PANDAS. This includes a recent investigation of microglial activation, assessed by positron emission tomography, reporting increased inflammation in multiple brain regions implicated in OCD pathogenesis in OCD subjects compared with healthy controls (Attwells et al. 2017). Additional support for an inflammatory etiology in these disorders includes a meta-analysis suggesting increased anti-basal ganglia antibodies in OCD (Pearlman et al. 2014), as well as post-mortem brain analyses on patients with TS suggesting an upregulation of multiple immune-related genes in the basal ganglia (Morer et al. 2010; Lennington et al. 2016).
Investigations of immune function in OCD and TS also implicate abnormalities in the peripheral immune function in patients with these disorders. For example, alterations in inflammatory cytokines and monocyte activation have been reported in OCD (Gray and Bloch 2012; Rao et al. 2015; Simsek et al. 2016) and TS (Matz et al. 2012), and two recent studies have demonstrated reduced levels of immunoglobulin molecules in children with OCD/TS compared with healthy controls (Kawikova et al. 2010; Bos-Veneman et al. 2011). In particular, immunoglobulin A (IgA), the most abundantly secreted immunoglobulin in the body and a major constituent of the mucosal immune system, was reduced in the serum of children with comorbid OCD/TS compared with healthy controls (Kawikova et al. 2010), a finding also reported in a case series of patients with TS (Hansen and Bershow 1997). Additionally, two case report series have investigated IgA deficiency in patients presenting to PANDAS/PANS specialty clinics, reporting similar rates of low serum IgA (∼14% of PANDAS/PANS) (Frankovich et al. 2015; Murphy et al. 2015).
Alterations in serum IgA concentrations, collectively termed IgA dysgammaglobulinemia, are of particular interest in OCD/TS, as IgA deficiency may predispose individuals to both recurrent infections and autoimmune conditions (Singh et al. 2014), both of which are implicated in the pathogenesis of OCD and TS (Mell et al. 2005). Deficits in serum IgA, in the context of normal levels of immunoglobulins G and M, are classified by two clinical diagnoses: selective IgA deficiency defined as undetectable (<0.05 g/L) serum levels of IgA, and partial IgA deficiency, defined as serum IgA >0.05 g/L but two standard deviations below the normative mean for age and sex. If deficiencies in IgA production are common or uniquely associated in patients with OCD/TS, it would represent a potential etiological framework for understanding the hypothesized association between infection, inflammation, and psychopathology in these disorders.
To address the hypothesis that IgA dysgammaglobulinemia is associated with pediatric-onset OCD and TS, we utilized the EHRs of a large New England health care system to investigate the rate of IgA deficiency and average serum IgA concentration in children diagnosed with OCD, TS, and other common childhood neuropsychiatric disorders. We also compared children with psychiatric diagnoses against a cohort of children with celiac disease, a common pediatric autoimmune disorder; IgA levels are routinely checked in the celiac disease workup, as IgA deficiency is common in celiac disease (Wang et al. 2011). Finally, we employed a similar analysis to investigate the rate of IgA deficiency in adults diagnosed with OCD compared with pediatric-onset OCD, as investigations into IgA abnormalities in OCD have, to date, been limited to children.
Methods
Description of study cohort
The Partners Healthcare EHR contains sociodemographic data, diagnostic billing codes, laboratory data, and clinical visit information of patients seen in five hospitals and multiple outpatient clinics in the New England area. Patients evaluated at Massachusetts General Hospital (MGH), Brigham and Women's Hospital (BWH), McLean Hospital (MH), Newton Wellesley Hospital (NWH), or North Shore Medical Center (NSMC) were included in the dataset. An electronic medical record query system, built on the i2b2 server platform and termed the Research Patient Data Registry (RPDR), allows for the collection of anonymized medical records through keyword, ICD diagnostic code, and demographic search terms for research purposes; this methodology has recently been used in several large-scale studies of psychiatric patient cohorts (Castro et al. 2015). The MGH/Partners Institutional Review Board approved all aspects of the current study.
EHR query methodology
For the current investigation, we queried the Partners Healthcare EHR for both billing and medical record codes to identify children diagnosed with the following conditions: OCD, TS, autism spectrum disorders (ASD), ADHD, anxiety disorders (excluding OCD), depressive disorders, and celiac disease (Supplementary Table S1 for a full list of ICD 9 and medical record codes used for each diagnostic query). OCD subjects also diagnosed with TS or a tic disorder were excluded from the OCD group, and tic disorder subjects diagnosed with OCD were excluded from the TS group, to independently analyze these frequently comorbid populations. Subjects with OCD or TS were not excluded from the analysis based on additional comorbid psychiatric diagnoses. Subjects with diagnoses of ASD, ADHD, anxiety disorders (excluding OCD), or depressive disorders served as psychiatric comparison populations, and subjects with celiac disease served as a comparison population with a high rate of IgA testing. Subjects in all cohorts were selected without replacement, in that subjects were only included in one cohort based upon the primary diagnosis listed in the EHR, and were not excluded if they also carried a comorbid diagnosis of one of the comparison groups.
Subjects identified from the diagnostic queries were required to meet two criteria: (1) diagnosed between 4 and 18 years of age with the queried clinical diagnoses listed above, and (2) recorded laboratory values for serum IgA between 4 and 18 years of age. Each individual medical record that met these criteria was run through a computer-generated script in which the subjects' birthdate was subtracted from the listed date of the primary clinical diagnosis, generating an age at diagnosis for each subject. Each subject was then run through a second script to calculate the age at which the subjects' IgA values were recorded (herein referred to as “age-at-blood draw”). All subjects with an age-at-blood draw before age 4 were excluded, given that (1) immunoglobulin levels are variable before this age due to environmental factors, such as breast-feeding, and (2) the clinical consensus for diagnosing IgA deficiency is limited to patients aged ≥4 (Cheng et al. 2012; Shakkottai et al. 2012). If an individual subject had more than one recorded value for IgA, the first recorded value was used as the analyzed value for that subject. Only subjects with clinical diagnoses between ages 4 and 18, and an age-at-blood draw between 4 and 18, were included in the pediatric analyses.
The query methodology to identify adult cases followed a similar strategy with the following exceptions. Subjects were included in the adult dataset if they had a recorded diagnosis of OCD after 18 years of age and had an IgA level drawn after the age of 18. As a review of all 1206 records identified using the query methodology was beyond the scope of the current study, there exists the possibility that a portion of these subjects had an onset of OCD before the age of 18 but initiated their care after the age of 18 in the hospital system utilized for this analysis. Subjects with comorbid tic disorders were excluded from the adult OCD dataset. Each subject was run through a computer-generated script to verify that the age of diagnosis and age-at-blood draw was >18 years.
Statistical analysis
To compare the rates of IgA deficiency, as well as the average serum values for IgA, two statistical models were used. All statistical analyses were performed in R Studio version 0.99.896 (The R Foundation for Statistical Computing, Vienna, Austria). Group differences in demographic measures were compared using chi-square tests for categorical variables.
We employed a univariate logistic regression model to calculate the odds ratio (OR) of IgA deficiency in the pediatric OCD cohort compared with each of the comparison cohorts, and to compare the OR of IgA deficiency in pediatric OCD cohort compared with adult OCD cohort. We included subjects from each hospital site in the analysis for this model, and hospital site was included as a covariate. The variable of interest (e.g., normal serum IgA vs. deficient IgA) was determined by the reference values of the hospital site laboratory and recorded as a dichotomous variable (e.g., high, normal, or low) for each subject; the high and normal variables were combined for data analyses, as low IgA was the variable of interest. The determination of IgA deficiency for an individual is based upon the standardized definition of a serum IgA level less than two standard deviations below the mean for age and gender (Shakkottai et al. 2012). As age and gender were already taken into account for the determination of IgA deficiency for each subject, these were not included as covariates in the univariate logistic regression model. To assess the effect of a subject's gender on IgA deficiency status, the sample was segregated by gender, and an additional univariate logistic regression model was employed to assess IgA deficiency among the cohorts.
A univariate linear regression model was used to compare mean IgA values for each diagnostic cohort. In this model each subject's recorded serum level of IgA was analyzed as a continuous variable; Bonferroni correction was used for multiple comparison correction, with p-values <0.05 considered significant. As testing methodology may vary slightly between hospital laboratories, we restricted this analysis solely to subjects who had IgA testing performed at the Massachusetts General Hospital site to minimize variability between subjects. As serum IgA levels differ according to age and gender during childhood, we used a nearest-neighbor matching algorithm (MatchIt Package, R-Studio) to match subjects with pediatric-onset OCD with subjects in the other clinical cohorts based on age-at-blood draw and gender. An analysis of the cohort separated by gender was not included in the current analysis, as these cohorts were unable to be adequately matched following segregation by gender.
Results
Rates of IgA deficiency among pediatric and adult cohorts
The final dataset included subjects from five hospitals and consisted of 3718 pediatric subjects in six clinical diagnosis categories and 1042 adult OCD subjects (Table 1). The demographic results for each of the pediatric cohorts displayed significant differences in age-at-blood draw and gender. The queries for pediatric subjects diagnosed with depressive disorders with a recorded IgA level returned a cohort with <20 subjects; this category was removed from further analyses.
Sociodemographic Data and Hospital Site of Subjects with Obsessive-Compulsive Disorder, Tourette Syndrome, Celiac Disease, Autism Spectrum Disorders, Attention-Deficit/Hyperactivity Disorder, and Anxiety
n/a denotes matching was unable to be performed for this group.
Significant differences in the ORs for IgA deficiency in pediatric OCD were appreciated when compared with ASD (OR = 1.93; CI = 1.18–3.16; p < 0.01) and anxiety disorder cohorts (OR = 1.98; CI = 1.28–3.06; p < 0.01), with pediatric OCD displaying roughly twice the likelihood of IgA deficiency when compared with these cohorts (Table 2). Furthermore, the pediatric OCD cohort displayed the highest percentage of IgA deficiency (15%), when compared with TS (14%), celiac disease (14%), ADHD (13%), ASD (8%), and anxiety disorder (8%, Table 2) cohorts. No significant differences were found in the risk of IgA deficiency when comparing OCD cohort with TS, celiac disease, or ADHD cohorts. Additionally, no significant differences in the risk of IgA deficiency were found when comparing TS cohort with comparison cohorts (Supplementary Table S2).
Rate of Immunoglobulin A Deficiency in a Pediatric-Onset Obsessive-Compulsive Disorder Compared with Other Pediatric Populations and Adult Obsessive-Compulsive Disorder
Odds ratio of IgA deficiency in pediatric OCD cohort compared with indicated comparison cohort.
Chi-square tests were performed to assess differences in the rate of IgA deficiency based upon sex within each clinical cohort; no significant differences were observed (Supplementary Table S3). However, when the pediatric cohorts were segregated by gender and compared, males with OCD were significantly more likely to show deficient IgA when compared with males in all other cohorts, with the exception of celiac disease (Table 2) and TS cohorts, which showed a trend toward significance (p = 0.06; CI = 0.97–4.99). No significant increase in the likelihood of IgA deficiency was observed when female cohorts were compared.
When comparing the rate of IgA deficiency between pediatric and adult OCD cohorts (Table 2), adults with OCD were significantly less likely to display deficient IgA when compared with pediatric-onset OCD (OR = 2.71; CI = 1.71–4.28; p < 0.001).
Serum IgA levels among pediatric cohorts
Serum IgA levels were compared using the matched sample set described above; the TS cohort used in these analyses was smaller than the pediatric-OCD cohort, preventing adequate matching, and was removed from these analyses. The matched sample displayed no significant differences in age-at-blood draw or sex across diagnostic groups (Table 1), indicating sufficient matching.
When comparing adjusted mean values for IgA across pediatric diagnostic groups (Table 3 and Fig. 1), significantly lower adjusted mean IgA values were found for OCD cohort (avg = 119.51 ± 6.26) when compared with ASD (avg = 141.91 ± 6.30; p = 0.04) and anxiety disorder (avg = 147.71 ± 6.27; p < 0.01) cohorts, with moderate effect sizes. No significant differences were observed between pediatric OCD cohort and ADHD or celiac disease cohorts.
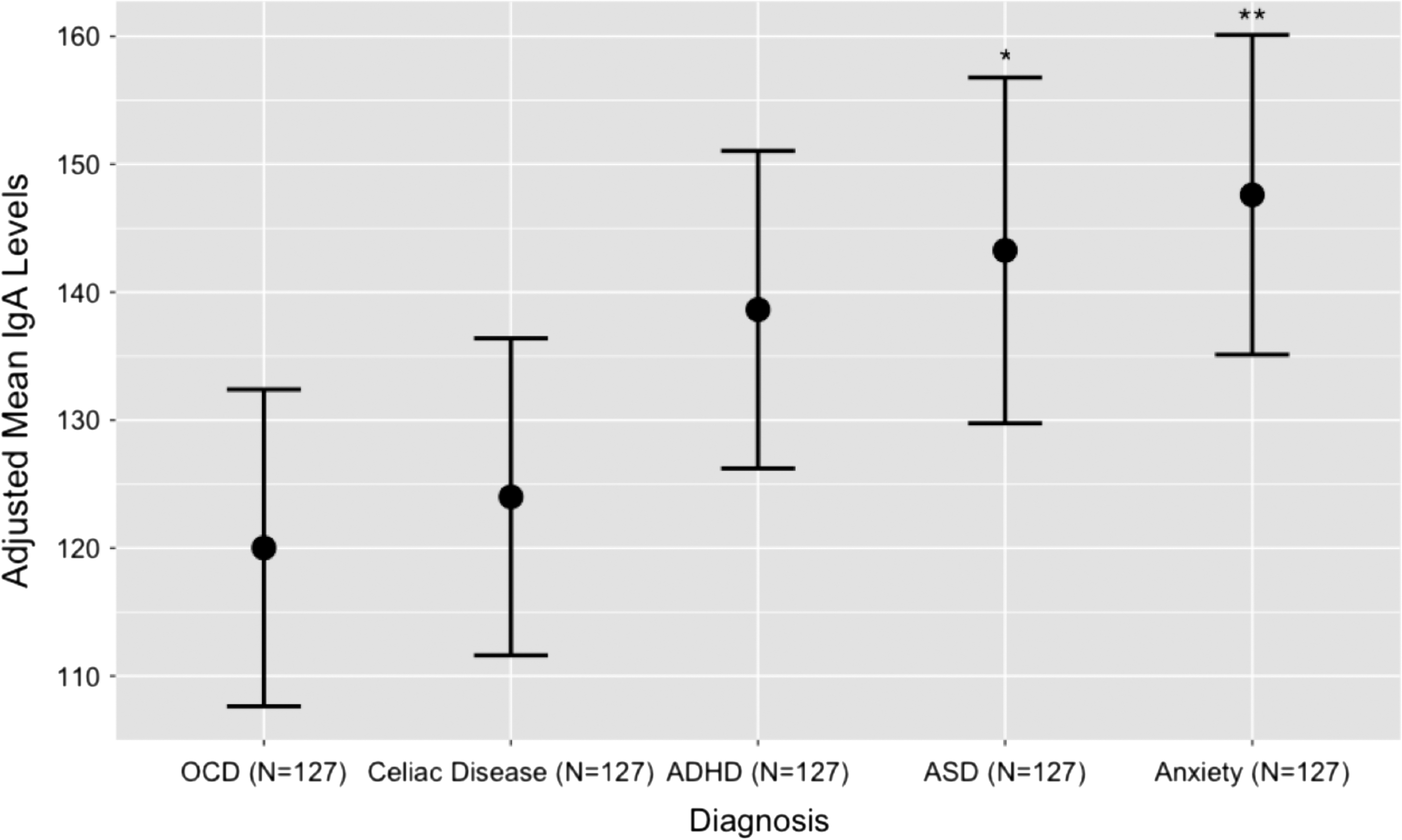
Adjusted mean IgA values in a matched pediatric sample of OCD and additional clinical populations. *p < 0.05, **p < 0.01, denoting significance compared with OCD cohort. OCD, obsessive-compulsive disorder; IgA, immunoglobulin A.
Mean Immunoglobulin A Values in a Matched Pediatric Sample
Matched by age-at-blood draw and gender. TS cohort was excluded due to insufficient matching parameters.
Discussion
Inflammation and autoimmunity have received considerable attention as potential etiologies for childhood OCD and tic disorders. The results presented here, obtained from a sample of EHRs from a large health care system, suggest that children with pediatric-onset OCD display increased rates of deficient IgA and lower mean serum IgA levels when compared with children with other neurodevelopmental or psychiatric disorders. Previous investigations have reported decreased serum levels of IgA in pediatric OCD/TS compared with healthy controls (Kawikova et al. 2010). The current results extend this finding through reporting an association of IgA deficiency in pediatric-onset OCD; apart from genetic syndromes, this represents the first reported association of an immunoglobulin deficiency with a childhood psychiatric disorder, to our knowledge.
Our data also reveal specific risks of deficient IgA with respect to age and gender in OCD. When comparing the rate of IgA deficiency in pediatric-onset OCD with adults with OCD, the pediatric OCD group displayed a fourfold higher likelihood of IgA deficiency. When the risk of IgA deficiency was segregated by gender, we did not appreciate any significant difference in the frequency of IgA deficiency within the pediatric cohorts, such that males with OCD were not significantly more likely to have IgA deficiency than females with OCD. However, when comparing male pediatric cohorts, males with OCD were significantly more likely to show deficient IgA than males in all other cohorts, with the exception of celiac disease and TS cohorts.
Several additional aspects from this study are worth noting. In contrast to earlier studies, deficiencies in IgA were unique to pediatric OCD cohort and were not appreciated in TS cohort; this discrepancy may be due to previous investigations using a population with comorbid OCD and TS (Kawikova et al. 2010) or related to the size of study sample. Furthermore, the pediatric-onset OCD group, both collectively and when separated by gender, showed no significant differences between serum IgA levels or rates of IgA deficiency when compared with celiac disease cohort, a disorder with a high rate of IgA testing and an increased rate of IgA deficiency (Singh et al. 2014).
The differences observed in IgA deficiency rates in male pediatric populations are of interest given the demographics of pediatric-onset OCD. Multiple investigations suggest that boys are more likely to display an earlier age-of-onset of OCD compared with girls, greater clinical severity during childhood, and increased rates of psychiatric comorbidities (Fontenelle et al. 2003; Mancebo et al. 2008; Taylor 2011). Currently, no environmental, genetic, or biological factors have been identified that account for the reported gender discrepancy in OCD. The present study did not find a significant difference in the rate of IgA deficiency in boys (17.8%) versus girls (12.1%) with OCD; however, this difference may approach significance in a larger study cohort. Additionally, the increased likelihood of IgA deficiency in children with OCD compared with adults is of interest, as it is estimated that at least half of all patients with OCD develop symptoms in childhood (Bloch and Storch 2015). Based on the discrepancy reported here in the rates of IgA deficiency by age, longitudinal studies in children with IgA deficiency focusing on the development of psychiatric or behavioral disorders may be warranted.
This study has several limitations. First, as the study was based upon EHR data, no healthy control group was included in the analysis, and we were unable to ensure the accuracy of psychiatric diagnoses for subjects in each cohort. Furthermore, all subjects were required to have an IgA level recorded for inclusion into the analysis. As this is not the standard of care for psychiatric disorders, it suggests that subjects included in the analyses had a cause for having an evaluation of serum IgA, which introduces a bias toward increased rates of immune abnormalities across subjects in all the cohorts included. A detailed reporting of the reason for each subject having an IgA level assessed was beyond the capability of our analysis. Additionally, the results presented here define IgA deficiency by laboratory measurements; a clinical diagnosis of selective or partial IgA deficiency was not possible from this data as it required additional information of each subject's IgG and IgM status. Finally, children with IgA deficiency have been reported to occasionally convert to normal IgA levels in adulthood (Lim et al. 2015), a process that may impact our finding of increased rates of IgA deficiency in children versus adults with OCD.
IgA serves numerous functions in the mucosal immune defense against viral and bacterial pathogens (Pabst et al. 2016), and is the dominant antibody found in mucosal secretions. Mucosal IgA is also recognized as a major contributor to the bacterial composition of the microbiome (Sutherland et al. 2016); microbiome composition was recently demonstrated to directly affect cortical development (Luczynski et al. 2016, and is an area of emerging focus in the etiology of psychiatric disorders (Rogers et al. 2016). While specific genes have been identified that result in IgA deficiency (Castigli et al. 2005), genetic susceptibility in IgA deficiency remains poorly defined (Yel 2010). IgA deficiency is also recognized as a risk factor for the development of autoimmune disease in children (Erkocoglu et al. 2017) and adults (Abolhassani et al. 2015), with these two small-scale studies reporting similar rates of patients with autoimmune conditions (17%). A recent population-based study performed on a Swedish birth cohort study also found significantly increased rates of autoimmune diseases in patients with OCD and tic disorders, including increased rates of inflammatory bowel diseases and scarlet fever (Mataix-Cols et al. 2018), both of which may be impacted by IgA deficiency. Future investigation is warranted to examine the possibility that the increased rates of autoimmunity reported in OCD may be influenced by IgA deficiency.
Currently no data exist to provide a mechanistic link between IgA dysgammaglobulinemia and OCD, though IgA deficiency is associated with recurrent infections, which are hypothesized to be etiologically linked to OCD symptoms in children with PANDAS. Two previous case-control studies have reported increased ORs of streptococcal infections in the 3 (Mell et al. 2005) or 12 (Mell et al. 2005; Leslie et al. 2008) months before new diagnoses of OCD or TS, and a prospective study of PANDAS subjects and OCD/TS controls has reported a twofold risk of streptococcal infections in the PANDAS cohort within the 2-year study period (Kurlan et al. 2008). Additionally, analyses of patients meeting PANDAS/PANS criteria in an outpatient clinic displayed a higher level of reported autoimmune conditions (29%) when compared with those diagnosed with pediatric OCD (1%) (Jaspers-Fayer et al. 2017). IgA levels were not examined in these listed investigations, though a recent case series of patients evaluated in a PANDAS specialty clinic has reported that 14% of patients presenting for treatment displayed IgA dysgammaglobulinemia (Frankovich et al. 2015).
The current results suggest that children diagnosed with OCD may be at a higher risk of immune dysfunction compared with other childhood psychiatric disorders, which warrants further investigation. This association may underlie the observed increase in streptococcal infections reported in the PANDAS subgroup of pediatric-onset OCD, as well as the hypothesized immune dysregulation central to the PANDAS hypothesis. As PANDAS is not currently included in the DSM-5 or ICD coding, we are unable to address the question of immune dysfunction in the PANDAS subgroup in the current investigation. Prospective analyses of immunoglobulins in children with OCD and PANDAS will serve to better estimate the rate of IgA dysgammaglobulinemia in pediatric OCD and determine if IgA status impacts the clinical course of this disorder. Previous longitudinal analyses have suggested that children with either TS or OCD experience an exacerbation of symptoms due to psychosocial stress and newly acquired bacterial infections (Lin et al. 2010); if these phenomena are mediated or exacerbated by IgA dysgammaglobulinemia, this may present a novel area for clinical intervention.
Conclusion
The contribution of the immune system to OCD pathogenesis continues to be a topic of interest and debate, though few biological measures have been identified that provide a direct evidence of this hypothesized etiology. The data presented here suggest that a significant percentage of children with OCD show abnormal immune regulation evident through deficient IgA production. Prospective large-scale studies investigating IgA levels in pediatric OCD and healthy controls will serve to better quantify this association and may define a subset of pediatric OCD patients for which additional analyses of immune function may be warranted.
Clinical Significance
Aberrant immune function has been implicated in the pathogenesis of OCD, as well as PANDAS, though few biomarkers of immune dysfunction have been reported. If these results are replicated, serum IgA values may represent a useful, widely available test to investigate immune dysfunction in this population. Future studies may also inform on whether IgA status impacts the clinical course of OCD in children.
Footnotes
Acknowledgments
Dr. Williams has received research support from the PANDAS Network, a non-profit foundation. Dr. Geller has received grant or research support from the National Institute of Mental Health, Pfizer, Eli Lilly and Co., GlaxoSmithKline, Otsuka, Forest, Shire, and Neurocrine Biosciences. He has received honoraria from the American Academy of Child and Adolescent Psychiatry and the Massachusetts General Hospital Psychiatry Academy. He has served on the speakers' bureau of Eli Lilly and Co.
This work was conducted with support from Harvard Catalyst, The Harvard Clinical and Translational Science Center (National Center for Research Resources and the National Center for Advancing Translational Sciences, National Institutes of Health award UL1 TR001102), and from Harvard University and its affiliated academic health care centers. The content is solely the responsibility of the authors and does not necessarily represent the official views of Harvard Catalyst, Harvard University, and its affiliated academic health care centers, or the National Institutes of Health.
Disclosures
No competing financial interests exist.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
Supplementary Table S3
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.