
Abstract
Objective:
To perform a systematic review of studies of lurasidone in children and/or adolescents and to present a case report aimed to add further insights into its use in clinical practice with youth.
Methods:
We searched the following databases for empirical studies, of any design, focusing on the pharmacokinetics, efficacy, or safety of lurasidone in children and/or adolescents: Pubmed (Medline), OVID (PsycInfo, EMBASE+EMBASE classic, OVID Medline), Web of Knowledge, and
Results:
From a pool of 301 potentially relevant references, we retained 12 pertinent studies (reported in 28 references), including 1 pharmacokinetics study, 1 double blind randomized controlled trial (RCT) for bipolar depression (BD) with 1 related interim analysis study of its extension phase and 1 related external posterior predictive check study, 1 double blind RCT for schizophrenia with 3 related interim analyses of its extension phase, 1 RCT and 1 case report for autism spectrum disorder, and 2 open-label studies focusing on a variety of disorders. Overall, these studies show that lurasidone is significantly more efficacious than placebo, with moderate effect sizes, and is well tolerated for BD and schizophrenia in youth. Published studies in youth have in general used doses up to 80 mg/day. Our case report suggests that high doses of lurasidone (148 mg/day) were well tolerated and might have contributed to substantial functional improvement in a 14-year old girl with psychosis and a previous history of anorexia nervosa, who had not responded to previous antipsychotics (olanzapine, risperidone, aripiprazole).
Conclusions:
There is increasing evidence that lurasidone may be moderately effective and well tolerated for the treatment of BD and psychosis in youth and may have procognitive effects. Our case report suggests that future RCTs should assess the efficacy and tolerability of high doses (>80 mg/day) of lurasidone in youth.
Introduction
L
The aim of this paper is twofold: (1) to conduct the first systematic review of the literature on the pharmacokinetics, efficacy, and safety of lurasidone in children and adolescents; (2) to present a case report that we deem adds further insights into the use of lurasidone in clinical practice with youth.
Systematic Review
Methods
We followed the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Liberati et al. 2009). We searched for empirical studies, of any design, focusing on the pharmacokinetics, efficacy, or safety of lurasidone in children and/or adolescents. The following electronic databases were searched until January 23, 2018, with no language/date/type of document restrictions: Pubmed (Medline), OVID databases (PsycInfo, EMBASE+EMBASE classic, OVID Medline), and WEB OF KNOWLEDGE Databases (Web of science [science citation index expanded], Biological abstracts, Biosis, and Food science and technology abstracts).
The search terms/syntax in PubMed was as follows: lurasidone [tiab] AND (children [tiab] OR child [tiab] OR childhood [tiab] OR adolesc* [tiab] OR youth* [tiab] OR young [tiab] OR early [tiab]) and was adapted for the other databases. Additionally, we searched for possibly relevant unpublished studies in
Results
From an initial pool of 301 possibly relevant de-duplicated citations, we retained a total of 12 pertinent studies, reported in 28 references. The selection study process is showed in the PRISMA flowchart in Figure 1. The study characteristics are reported in Table 1.
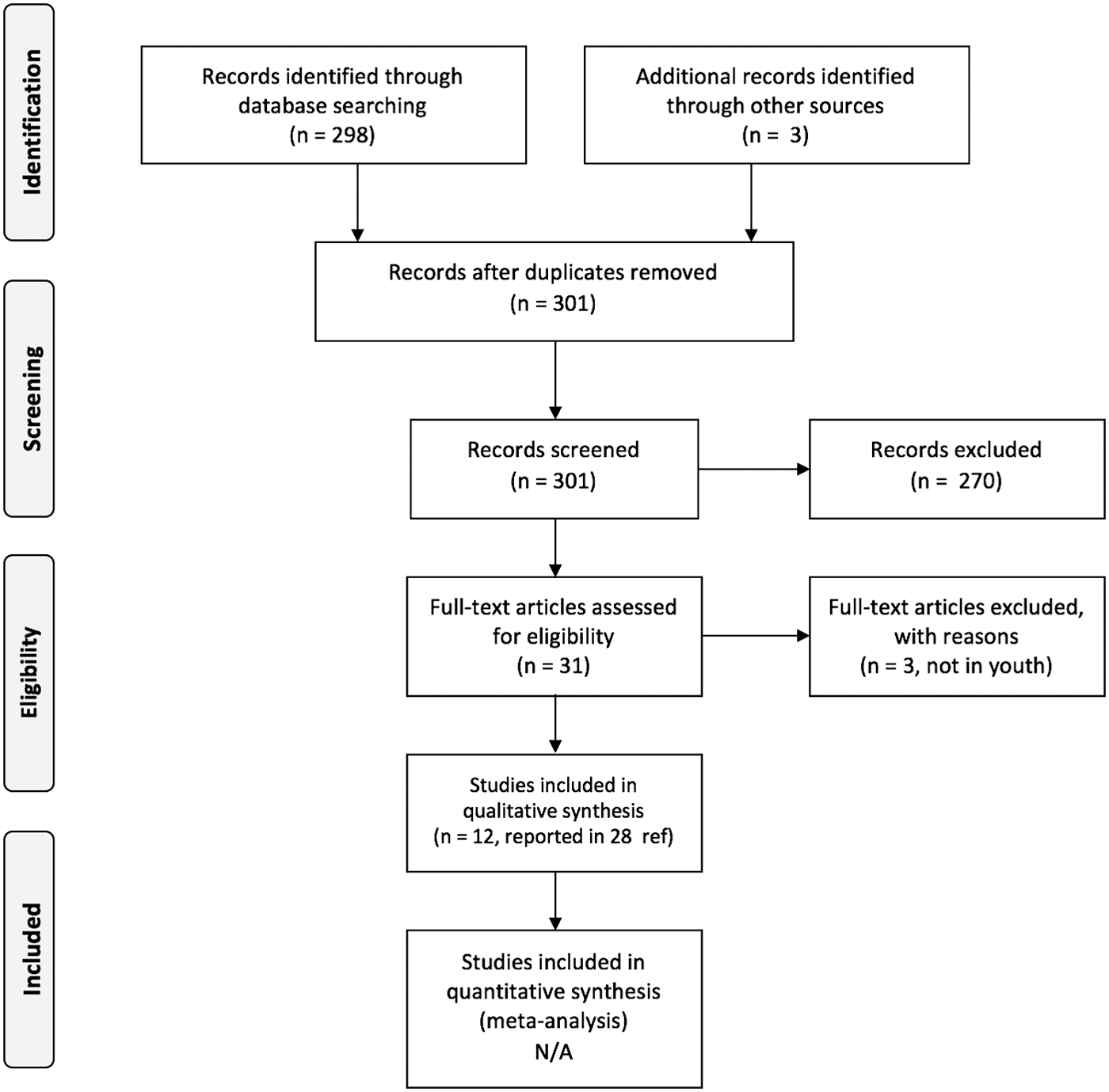
Preferred reporting items for systematic reviews and meta-analyses flowchart.
When available.
AE, adverse event; BD, bipolar depression; NS, not specified; RCT, randomized controlled trial.
In the next sections we present an overview of the studies assessing the efficacy and/or safety of lurasidone across child and adolescent psychiatric disorders, preceded by a section on the pharmacokinetics of lurasidone in youth.
Pharmacokinetics
An open-label study by Findling et al. (2015a,b) assessed the pharmacokinetics of lurasidone in 105 children aged 6–17 with a variety of psychiatric disorders, including schizophrenia spectrum disorder, bipolar spectrum disorder, autism spectrum disorder (ASD), attention-deficit/hyperactivity disorder (ADHD) with aggressive behavior, and Tourette's syndrome. The dose ranged between 20 and 160 mg/day. Of note, this is the only published study, among those retrieved in our systematic review, using daily doses above 80 mg. Cmax and AUC0–24 to lurasidone and its active metabolites showed linear increases across the dose range, especially between the 20-and 80-mg/day doses, while the linear effect attenuated between the 80- and 160-mg/day doses. Median Tmax was 2 h. Overall, the study demonstrated that the pharmacokinetic profile of lurasidone in child and adolescent patients is generally similar to the profile found in adults, with slightly higher exposure levels seen in the 6–9-year-old age group.
Efficacy and tolerability for specific disorders
Bipolar depression
A randomized controlled trial (RCT) was carried out to test the efficacy and safety of lurasidone (20–80 mg/day, mean dose 33.6 mg/day) in 347 children and adolescents with BD. This is a relevant study given the limited evidence for the pharmacological treatment of BD in youth. At endpoint (6 weeks) (DelBello 2017c, DelBello et al., 2017a,b; Goldman et al., 2017a), lurasidone showed statistical superiority compared with placebo on the primary outcome (reduction in the Children's Depression Rating Scale–Revised [CDRS-R] total score), with moderate effect size (p < 0.0001, effect size [ES]: 0.45), as well as on the secondary outcomes (reduction in: Clinical Global Impression-Bipolar Severity [CGI-BP-S]: p < 0.0001, ES 0.44; Pediatric Anxiety Rating Scale [PARS]: p < 0.385, ES: 0.23; Children's Global Assessment Scale [CGAS]: p < 0.001, ES: 0.44; Pediatric Quality of Life, Enjoyment, and Satisfaction Questionnaire: p < 0.0044, ES: 0.32). Improvement in the CDRS-R total score at week 6 was larger in the placebo group for the younger (vs. older) group (17.0 [SD: 1.6] vs. 14.3 [1.5]). The percentage of participants defined as responders (≥50% reduction from baseline to week 6 on the CDRS-R total score) was significantly larger in the lurasidone group compared with the placebo group (59.5% vs. 36.5%; p < 0.0001; number needed to treat [NNT] = 5).
However, the percentage of patients defined as remitted (CDRS-R total score 28, Young Mania Rating Scale total score ≤8, and CGI-BP-S depression score ≤3) was not significantly different between the lurasidone and the placebo group (26.0% vs. 18.8%; p = 0.082; NNT = 14). Significant differences emerged at week 2. In terms of cognitive effects, lurasidone improved processing speed and attention/vigilance subscores at the Cogstate test significantly more than placebo (p < 0.05, both).
In a secondary analysis by Singh et al. (2017), the following CDRS-R items were significantly improved on lurasidone, compared to placebo: (1) impaired school work; (2) difficulty having fun; (3) social withdrawal; (4) sleep disturbance; (5) appetite disturbance; (6) irritability; (7) excessive guilt; (8) low self-esteem; (9) depressed feelings; (10) excessive weeping; (11) depressed facial affect; (12) listless speech; and (13) hypoactivity.
Overall, lurasidone was well tolerated. At least one treatment-emergent adverse event (AE) was reported by 64.0% and 51.7% of participants in the lurasidone and the placebo group, respectively. The most frequent AEs on lurasidone were nausea and somnolence. Serious AEs occurred in two participants in the lurasidone group (fractured humerus; worsening of BD) and four patients in the placebo group (worsening of BD; increased depression severity; psychotic disorder; spontaneous abortion). Changes in body weight and body mass index (BMI) (percentiles and z-scores), as well as in lipid, glucose, and prolactin levels, were not statistically different in the lurasidone and placebo groups, respectively.
In a post hoc analysis by Pikalov et al. (2017), lurasidone, compared with placebo, was associated with significantly greater reductions in CDRS-R scores both in the mixed-features (subsyndromal hypomanic) group (p < 0.01, ES = 0.45) and in the group without mixed features (p < 0.01, ES = 0.45). Additionally, lurasidone was associated with significantly greater effect (vs. placebo) for reductions in CGI-BP-S scores both in the mixed features group (p < 0.001; ES = 0.57) and in the group without mixed features (p = 0.05; ES = 0.30).
The analysis of the study data by Chapel et al. (2017a,b) using external posterior predictive check concluded that, as in adults, higher doses of lurasidone were likely to lead to greater drug-related improvements on the Montgomery-Asberg Depression Rating Scale (MADRS) scores.
With regards to long-term effects, an interim analysis at 28 weeks, including 155 participants, was conducted as part of a 2-year open label extension of the DelBello et al. study, where youth initially randomized to lurasidone continued this treatment, whereas those initially assigned to placebo were switched to lurasidone. On the CDRS-R, mean changes from open-label baseline to week 28 for the lurasidone-lurasidone and placebo-lurasidone groups were 7.3 (SD: 5.1) and 12.5 (10.5), respectively. On the CGI-BP-S, mean changes for lurasidone-lurasidone and placebo-lurasidone groups were: 1.0 (0.7) and 1.2 (0.9), respectively (Chang et al. 2017a).
Thus, lurasidone was associated with continued improvement in depressive symptoms up to 28 weeks. The three most common AEs in the lurasidone-lurasidone and placebo-lurasidone groups, respectively, were headache (22.6 and 16.7%), nausea (12.2 and 16.7%), and anxiety (12.2 and 7.4%). Minimal changes were observed on weight, metabolic parameters, and prolactin levels (Chang et al. 2017b). The analysis of cognitive effects at 28 weeks (Burdick et al. 2017) revealed no deleterious effects of lurasidone (mean change from double blinded phase baseline on the composite Z-score of the Cogstate test for lurasidone-lurasidone and for placebo-lurasidone, respectively, was +0.01 and −0.02 at open-label baseline, and +0.15 and +0.22 at week 28).
Schizophrenia
We retrieved a large double-blind RCT including 327 adolescents with schizophrenia (dose of lurasidone: 40 or 80 mg/day) (Correll 2016; Goldman et al. 2016a,b; Findling 2017a,b; Goldman et al. 2017b,c). In terms of efficacy, lurasidone was statistically superior to placebo on the primary (Positive and Negative Syndrome Scale [PANSS] total score: 40 mg/day: p < 0.001, ES: 0.51; 80 mg/day: p < 0.001. ES: 0.48) and secondary endpoint outcomes (CGI-S: 40 mg/day: p < 0.001, ES: 0.49; 80 mg/day: 0.0015, ES: 0.45); PQ-LES-Q: 40 mg/day: <0.05; 80 mg/day: <0.001; C-GAS: 40 mg/day: <0.01; 80 mg/day: <0.001). An additional analysis focusing on the PANSS subscales (Correll et al. 2017a,b) showed that placebo-adjusted least squares (LS) mean change for lurasidone 40 and 80 mg/day, respectively, were −3.2 (p < 0.001, ES = 0.62) and −3.2 (p < 0.001, ES = 0.60) on the PANSS positive subscale, −1.7 (p = 0.011, ES = 0.41) and −1.6 (p = 0.022. ES = 0.35) on the PANSS negative subscale, −2.8 (p = 0.012, ES = 0.38) and −2.8 (p = 0.011, ES = 0.37) on the PANSS general psychopathology subscale, and −1.1 (p = 0.016, ES = 0.36) and −1.8 (p < 0.001, ES = 0.53) on the PANSS excitability subscale. Around 64% (lurasidone 40 mg/day) and 65% (lurasidone 80 mg/day) of participants were classified as responders (≥20% reduction in PANSS total score) versus 42% in the placebo arm. No significant differences were found in remission rates across study arms.
Overall, lurasidone was well tolerated. The most common AEs with lurasidone were nausea and somnolence. No significant differences between lurasidone and placebo were detected in lipid parameters, glycemic indices, or prolactin levels. No significant differences for LS mean change in body weight and BMI z-score were found between lurasidone 40 mg/day (0.17 kg and −0.02, respectively) or lurasidone 80 mg/day (0.49 kg and 0.00, respectively) compared with the placebo (0.05 kg and −0.03, respectively).
In interim analyses of a 24-month, open-label extension (Correll et al. 2017c,d; Tocco et al. 2017), additional improvements were reported on the total and subscales of the PANSS. Furthermore, lurasidone was generally well tolerated, with minimal impact on metabolic parameters.
Autism spectrum disorder
We found a 6-week double-blind RCT assessing lurasidone 20 mg/day, lurasidone 60 mg/day and placebo in 150 children/adolescents with ASD and irritability, agitation, and/or self-injurious behaviors (Loebel et al. 2016). Lurasidone was not significantly better than placebo on the primary outcome (Aberrant Behavior Checklist Irritability subscale score, or on the majority of the secondary outcomes (social withdrawal and lethargy, stereotypic behavior, hyperactivity and noncompliance, and inappropriate speech ABC subscales; Clinician-rated Clinical Global Impression, Severity [CGI-S], Children's Yale-Brown Obsessive Compulsive Scales). However, lurasidone 20 mg/day was significantly statistically superior to placebo on the CGI improvement scale (CGI-I) (p = 0.035). Discontinuation rates due to AEs were as follows: Lurasidone 20 mg/day, 4.1%; 60 mg/day, 3.9%; placebo, 8.2%. Minimal changes were reported in weight and metabolic parameters.
We also retrieved a case report (Millard et al. 2014) showing an effective outcome for lurasidone being added to other medications in a 13 year old boy with autistic disorder who had significant aggression and temper outbursts. Having previously been tried on risperidone and aripiprazole without positive effect and with significant adverse effects (excessive eating with weight gain and vomiting respectively) this should reduce the chance that what was seen was a placebo effect.
Efficacy and tolerability across several disorders
Wang et al. (2016) reported a retrospective chart review of 56 patients (aged 5–17) admitted to a child crisis and intervention service. Lurasidone (from 32.8 mg to 53.2 mg/day) was used for a variety of conditions/reasons: mood stabilization (75%), mood stabilization and psychosis (10.7%), psychosis (8.9%), hallucinations (3.6%), and delusions (1.8%). Ten patients (17.9%) discontinued lurasidone due to ineffectiveness, and 1 (1.8%) discontinued it due to intolerable side effects. In the 45 patients for whom lurasidone was effective, improvements in symptoms were seen an average of 4.1 days after initiating therapy. As for tolerability, 75% of patients experienced no AEs. The most common AEs were sedation (8 patients), fatigue (4 patients), and muscle stiffness (3 patients). Akathisia occurred in two patients.
We note here that the above mentioned pharmacokinetics study by Findling et al. (2015a,b) focusing on several conditions (including ADHD, bipolar disorder, autism, and psychosis) also reported data on tolerability. In general, the side effect profile was similar to the one reported in adult studies, with somnolence, akathisia, nausea, parkinsonism, and agitation being most common (Citrome, 2011). However, in this study a higher frequency of somnolence— −42% of the sample—was found, which has also been found when other atypical antipsychotic agents have been used in children. The other most common AEs seen were sedation, nausea, and vomiting. Around 70% of the reported AEs were mild or moderate in intensity. The most common dose to lead to severe AEs being reported was 80 mg/day, with severe side effects reported in the 120 mg group and none reported in the 160 mg group. Important findings were low rates of movement disorders, no clinically significant changes in weight, and no changes on blood tests or ECG.
We also retrieved an additional unpublished study in
Case Report
We discuss now the case of a 14 year old girl presenting with psychosis, having recovered from an eating disorder. Miss A was first admitted to an adolescent inpatient unit at the age of 14 for anorexia nervosa. She presented with a BMI of 15, with amenorrhea for 6 months before the admission. She described a fear of gaining weight and was avoiding fatty foods. She also described feeling low in mood. At this time she described an anorexic voice that told her not to eat certain foods. The voice was perceived as sounding like her and was experienced as coming from inside her head. Two weeks before admission to the inpatient unit, she was commenced on olanzapine 5 mg/day. After 5–6 days her mother felt that there had been an improvement in Miss A's experience of voices as she was no longer calling out against them in the morning.
During the admission, Miss A gained weight appropriately up to a healthy weight and engaged in psychology sessions to address her anorexic cognitions. However, her anorexic voices were still present at discharge, although to a lesser extent, and she was still on olanzapine 2.5 mg/day, which had been halved from the 5 mg that she was taking at the start of the admission. The plan was that it should be continued for a short time and then stopped.
After discharge, Miss A continued well for a month or so but then started to experience symptoms of low mood. She was commenced on 20 mg/day of fluoxetine, which appeared to have some benefit initially. Unfortunately, a couple of months later, Miss A began to experience increased voices and also visual hallucinations relating to terrorists, seeing figures hiding behind trees, and planes dropping bombs and also described being able to smell the smoke from the bombs and feel the heat being generated. This led to Miss A being very fearful to leave the house, which resulted in her being unable to attend school or her sporting activities.
In the outpatient clinic, the dose of her olanzapine was increased with a noticeable increase in her sedation but no obvious benefit to her symptoms. Due to the level of distress and concerns about her safety, she was admitted again to an inpatient unit. At the time of assessment, Miss A met criteria for a diagnosis of early onset psychosis (schizophrenia criteria). In fact, she had persistent delusions about terrorists being after her and about food and fluids being poisoned. Furthermore, she was experiencing auditory, visual, tactile, and olfactory hallucinations which she was convinced were real and led to a significant change in her behavior—hiding from bombs and terrorists and avoiding drinking tap water or food that was not packet wrapped. Additionally, in the previous few months she had withdrawn socially, being less interested in her sporting activities or being in contact with friends either in person or online. She also had significant symptoms of low mood. It was difficult to establish which symptoms started first, but it appeared that the psychotic symptoms with paranoia were most predominant at the time of assessment.
After the admission, the dose of olanzapine was increased further to 20 mg. However, this led to severe sedation, which made it very difficult for her to function. She was therefore changed to risperidone. Although there had been some improvement noted on risperidone 3 mg/day, she had also had some extrapyramidal side effects, with stiffness and discomfort in the shoulders, and she had also had several nose bleeds, which she had not previously been troubled with. Her prolactin was significantly elevated (>25 ng/mL). She was therefore started on low-dose aripiprazole (5 mg/day), which she tolerated well, with the aim to control the psychotic symptoms and decrease prolactin levels.
In view of the listed side effects with only a small amount of improvement in mental state, her dose of risperidone was not increased any further. It was therefore decided to try transitioning her to aripiprazole as the sole antipsychotic. Miss A managed this transition well, and the dose of aripiprazole was gradually increased up to 25 mg/day, with improvements reported with each increment. Miss A engaged well in education on the unit and started to gradually have more weekend home leave with a gradual increase in her activities. Although she was managing to do more in terms of seeing friends and going back to her sporting activities, she still found it very difficult to be outside, worrying more about terrorists and airplanes at these times. She continued to report that the voices were continuously present, although she became more able to ignore them and distract herself. Aripiprazole was generally well tolerated although she did experience significant sedation, going to bed early and sleeping during the daytime. However, some of the daytime sleeping was to avoid experiencing the voices. She also experienced some restlessness and increased appetite with consequent weight gain, although her weight always remained just within the healthy range.
Although Miss A had made significant progress, she seemed to plateau, but then, during her end of secondary school examinations, she started to deteriorate. She had an increase in voices telling her not to take her medications, as they were poisoned, which led to her missing several doses. She appeared much more agitated and anxious. In view of these symptoms she did not continue with her examinations, as it was apparent that the stress was having a significant detrimental impact on her mental health. It was therefore decided to try a different antipsychotic.
In view of the fact that Miss A was anxious about her self-image with some residual eating disorder cognitions, she was keen to have a medication that would not lead to significant weight gain. Miss A had also experienced significant sedation with olanzapine, risperidone, and aripiprazole. Quetiapine was considered, but in view of the propensity for weight gain and likely sedation, this was not preferred. Lurasidone was therefore considered in view of the evidence (available only from studies in adults at the time Miss A was treated) that it has the least propensity to lead to weight gain, that it is as effective as quetiapine for psychosis in adults, and because of it possible precognitive effects (Loebel et al. 2013).
As lurasidone is not licensed for use in children and adolescents in the United Kingdom, it was prescribed off license with parents and young person being informed and consenting.
Considering the previously experienced extrapyramidal side effects with risperidone, lurasidone was started concurrently with procyclidine. In view of the limited experience with lurasidone in adolescent patients as well as Miss A's previous sensitivity to side effects, the starting dose of lurasidone was cautiously set at 18.5 mg, which is half of the adult starting dose. It was then titrated up by 18.5 mg every 3–4 days up to a dose of 74 mg while reducing the aripiprazole.
At around this point, Miss A experienced a significant deterioration in her mental health without an apparent trigger, with strong voices telling her that food, fluids, and medications were all poisoned. This led to Miss A having very little to eat or drink and missing several doses of lurasidone. Despite a lot of support and persuasion, Miss A would not eat or drink adequately or take her medications. The option of intramuscular medication or giving nutrition and medication via a nasogastric (NG) tube was considered. Miss A consented to a NG tube being passed, and medications and nutrition were given for a week. The dose of lurasidone continued to be increased every 1–2 weeks up to the maximum dose of 148 mg. There was some improvement seen in terms of Miss A's interaction with her peers and parents, but the auditory hallucinations telling her that medication and food and fluids were poisoned persisted. Due to the need for the NG tube, Miss A was not able to go on home leave for 3 weeks. A depot medication was considered, but the ultimate decision was to persist with lurasidone until the optimum dose was reached. Motivated by the desire for leave, she tried going without the NG tube and generally managed the leave well. After Miss A had been on lurasidone 148 mg for just over a week (6 weeks since it was commenced in total), her mental state improved significantly, with a reduction in her voices, with them still being reported to be present but Miss A was not distressed by them and was able to ignore them. The improvement seemed very rapid but appeared genuine, with Miss A managing to go on a weekend camping trip without apparent difficulties or anxiety. In previous months this situation would have been intolerable. At the point of discharge, around 4 weeks after being on maximum dose lurasidone, Miss A and her parents were reporting that she was the most well that she had been in the past 2 years, with no significant side effects apart from a little nonimpairing sedation. She had been regularly reviewed for side effects, particularly checking for those known to be commonly associated with lurasidone, such as akathisia and extrapyramidal side effects, but all of these were denied and not evident.
From the point of view of weight gain, Miss A lost around 3 kg during the time that she was not eating or drinking much. When she was well again her weight increased. At discharge she was 0.5 kg heavier than when she started the lurasidone (8-week period) but still at the top of her healthy weight range (25th–75th BMI percentile). Comparing this to aripiprazole, in the 2 months when Miss A was taking aripiprazole alone, she initially lost 1 kg when risperidone was stopped completely and then gained 2.1 kg over the 2 months until the lurasidone was introduced.
Discussion
At the time this case was presented to our team, evidence was not available for the efficacy of lurasidone for psychosis in adolescents, although the adult literature had suggested that it is similar in efficacy to risperidone and is superior to quetiapine, with improved cognitive effects (Loebel et al. 2013). Indeed, lurasidone in adults has been found to significantly improve neurocognitive performance compared with quetiapine, even after accounting for sleepiness effects (Harvey et al. 2016), and there is preliminary evidence that it improves cognition in euthymic patients with bipolar I disorder (Yatham et al. 2017).
Lurasidone had also been found to be effective for depression in schizophrenia in adults at doses of 80 mg and above (Nasrallah et al. 2015). With the above studies (DelBello et al. 2017a; Goldman et al. 2017b) in adolescents now available, there is increasing evidence for the efficacy of lurasidone in schizophrenia in adolescents, as well as positive effects on mood in BD, with results indicating a dose-related improvement. It is a shame that neither the BD nor the schizophrenia in adolescents study used doses any higher than 80 mg, as while they both demonstrated a significant response, neither study indicates that a significant number of young people entered remission.
However, the United Kingdom British National Formulary indicates 148 mg/day as maximum recommended dose. The present case report indicates that symptoms were greatly reduced several weeks after the patient being established on the dose of 148 mg, which was generally well tolerated. There are possible reasons why doses above 80 mg were not included in the RCT studies, since more side effects had been experienced with doses above 120 mg in a previous study (Findling et al. 2015a). However, to inform clinical practice it would be helpful if further research does include higher doses as a dose response effect is suggested in the study by DelBello et al. (2017a).
While lurasidone was used after having tried three other antipsychotics in the present case, given the recent available evidence we wonder to what extent lurasidone would be a reasonable choice for first line use in BD or psychosis, particularly in young people who are concerned about weight gain. In our view, the other important reason to consider lurasidone for the treatment of psychosis is the fact that young people with schizophrenia are likely to need to remain on medication for long periods of time, meaning that being treated with an agent with few metabolic or weight effects has the potential for significant health benefits and cost savings in the longer term, even though it is more costly in the short term. Indeed, cost–benefit analyses have been carried out for the use of lurasidone versus aripiprazole for schizophrenia in adults and show that lurasidone is a cost effective option with significant potential savings in terms of reduced hospitalizations, weight gain, and diabetes along with the costs that these imply (Rajagopalan et al. 2016).
Conclusions
An increasing body of research indicates that lurasidone in children and adolescents displays similar pharmacokinetics and side effects to those seen in adults and is efficacious, with moderate effect sizes, for BD and schizophrenia in adolescents. Interim analyses of open label extension studies suggest possible continued benefit and improvement in symptoms. Additionally, while current evidence does not support the first or second line use of lurasidone for irritability in autistic disorder, the case report would suggest that there may be benefits to individuals when other evidence based treatments have been exhausted. Furthermore, lurasidone should be considered for its possible precognitive effects.
The present case report suggests that doses of lurasidone higher than those used in published RCTs in youth may be needed to achieve near remission of symptoms. As this may well be the case for other adolescents with psychosis, the present case report suggests that further research using an RCT design followed by an open label extension should explore the efficacy and tolerability of high doses of lurasidone for youth over a sustained period of time.
Clinical Significance
There is increasing evidence that lurasidone is moderately effective and well tolerated for the treatment of BD and psychosis in youth. Doses higher than 80 mg/day could be considered, but additional evidence is needed.
Footnotes
Disclosures
No competing financial interests exist.