
Abstract
Objective:
The aim of this pilot study was to explore the feasibility and proof of concept of triple chronotherapy (TCT) as a nonpharmacological adjunctive treatment in the acute management of depression in the adolescent population.
Methods:
Thirty-one adolescents with nonpsychotic moderate-to-severe depression were included in the study. The 4-day TCT intervention comprised one night of sleep deprivation followed by 3 days of sleep phase advancement and daily bright light therapy. Primary outcomes were feasibility and depression, as measured by the Hamilton Depression Scale-17 (HAMD-17). Secondary outcomes included severity of illness, anxiety, self-harm, insomnia, and suicidality.
Results:
Twenty-nine (94%) adolescents completed the 4-day TCT intervention. Twenty-six (84%) of the 31 enrolled patients experienced a reduction in depressive symptoms of at least 50% from baseline; 24 (77%) achieved remission, defined as a HAMD-17 score less than 8. The mean depression score was severe before the start of the intervention (
Conclusions:
This pilot study determined TCT to be a feasible, safe, rapid, and potentially effective adjunctive treatment for depression in the adolescent population.
Introduction
A
Chronotherapy, defined as the therapeutic manipulation of sleep–wake cycles, is a promising approach for the treatment of adolescent depression. The study of chronotherapeutic interventions as an adjunctive treatment for depression began in the 1970s, when investigators noted a rapid, although transient, antidepressant response to sleep deprivation (Pflug and Tolle 1971). Another chronotherapeutic technique, bright light therapy, has consistently shown benefit in the treatment of seasonal affective disorders (Nussbaumer et al. 2015). Its use in the treatment of nonseasonal unipolar and bipolar depression has also shown promising results (Tuunainen et al. 2004; Al-Karawi and Jubair 2016).
Combination chronotherapeutics, such as triple chronotherapy (TCT), have also been trialed with some demonstrated efficacy. TCT is an approach that combines sleep deprivation, bright light therapy, and sleep phase advancement in the acute treatment of depression (Martiny et al. 2012; Benedetti et al. 2014; Martiny et al. 2015). One of the first open label TCT studies enrolled 143 consecutive patients; of the 141 adults who completed the study, a significant acute antidepressant response was found in up to 70% of patients with bipolar depression and a sustained response in up to 55% of patients at 1 month (Benedetti et al. 2014). A more recent randomized control trial of 75 adults with unipolar or bipolar disorder used an abbreviated protocol that included one night of sleep deprivation, three nights of sleep phase advancement, and bright light therapy in each of the four mornings of the intervention. This study demonstrated similar, accelerated antidepressant responses along with a decrease in suicidality and improved sleep quality (Martiny et al. 2015).
Although evidence is growing for the use of TCT to manage acute depression and suicidality in adults, studies in the adolescent population are lacking. It was hypothesized by Gest et al. (2014) that the use of chronotherapy in adolescents could be an effective treatment modality, and researchers were urged to explore this area. In 2016, Gest et al. compared combined sleep deprivation and bright light therapy to bright light therapy alone in adolescents and found a significant antidepressant response to bright light therapy alone, but no significant benefit was gained with the addition of one night of total sleep deprivation. Sleep phase advancement was absent in this study (Gest et al. 2016). No studies were found that examined the use of comprehensive TCT in adolescents.
This pilot study was designed to explore the feasibility and proof of concept of TCT as a nonpharmacological adjunctive treatment in the acute management of depression in the adolescent population. Secondary outcomes included exploring the effect of TCT on anxiety, self-harm, insomnia, and suicidality.
Methods
Sample
Patients invited to participate in the study were aged 12 to 17 years and were experiencing a nonpsychotic moderate-to-severe depressive episode with concurrent suicidality and insomnia. Patients were diagnosed by a child-adolescent psychiatrist using Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5) criteria. Participating patients met criteria for admission to the 18-bed Psychiatric Youth (ages 6–17) Inpatient Unit during July 2016–March 2017. Criteria for admission included high risk for imminent harm to self or others and severely impaired functioning in the home, school, or community setting. Patients who agreed to participate in the TCT intervention provided informed assent with parent or guardian consent. Exclusion criteria were active psychosis, being in a mixed or manic affective state, history of seizure disorder, and pregnancy. TCT was an adjunctive treatment to standard medication management and therapy. Criteria for study withdrawal included patients who fell asleep for more than 30 minutes during the period of sleep deprivation, seizure activity during the TCT intervention, or request to be withdrawn from the study. The study was approved by the local Institutional Review Board.
Procedures
Patients were recruited from adolescents admitted with moderate-to-severe unipolar or bipolar depression (HAMD-17 score 14 or above) to the Psychiatric Youth Inpatient Unit. After an initial assessment, the inpatient psychiatrist briefly explained the TCT intervention to the patient and family or guardian. Upon consent, nursing staff reviewed the procedure with the patient and family, outlining the treatment schedule.
Inpatient staff partnered with patients throughout the 4-day protocol. Patients underwent one night of sleep deprivation beginning on the day of admission, followed by three nights of sleep phase advancement. During sleep deprivation, adolescents interacted 1:1 with a staff nurse, playing a variety of games and exercising. The TCT schedule was as follows: Day 0: One night of total sleep deprivation Day 1: Sleep at 6 pm. Day 2: Awaken at 1 am. Sleep at 8 pm. Day 3: Awaken at 3 am. Sleep at 10 pm. Day 4: Awaken at 5 am; discharge following light therapy
On the mornings of days 1–4 patients received bright light therapy from 7:00 am to 7:30 am using a 10,000 lux light box. Upon discharge patients were given a light box and strongly advised to continue the maintenance sleep schedule, sleeping from 10 pm to 6 am, and bright light therapy at 7:00 am daily for 30 minutes. Patients were scheduled for follow-up outpatient appointments at 1 week and 1 month following hospital discharge.
Measures during the inpatient stay and follow-up appointments assessed for depression, global functioning, adverse childhood experiences (ACEs), anxiety, suicidality, self-harm, and insomnia. Board certified child and adolescent psychiatrists and psychiatric nurses completed or facilitated patients in completing all measures.
Instruments
Hamilton Depression Scale-17 (HAMD-17). The HAMD-17 is a modified version of the 21-item observer-rated Hamilton Depression Scale. This 17-item multidimensional scale measures depression in both adults and adolescents with the following cut points: score 0 to 7 = normal; score 8–13 = mild depression; score 14–18 = moderate depression; score 19–22 = signs of severe depression; and score ≥23 = severe depression. Depression response is defined as a reduction in depressive symptoms of at least 50%; remission was defined as a HAMD-17 score of less than 8. The HAMD-17 has been validated for use in the adolescent population; internal reliability of the HAMD-17 ranges from 0.46 to 0.97, and 10 studies report estimates ≥0.70 (Bagby et al. 2004; Lachal et al. 2012).
Clinical Global Impressions (CGI). The CGI is a three-item tool that measures severity of illness, global improvement, and efficacy index which compares therapeutic effect with side effects. The first two items have a 7-point observer-rated scale. Severity of illness ranges from “1” (normal) to “7” (among the most extremely ill patients); global improvement ranges from “1” (very much improved) to “7” (very much worse). The third item, efficacy index, considers patient improvement and medication side effects from “1” (vast improvement with no side effects) to “16” (unchanged or worse and side effects that outweigh the therapeutic effect). Because the validity and reliability of the CGI vary due to required memory recall, it is suggested that other measures be used in conjunction with the CGI, which this study has done (Forkmann et al. 2011). In addition, this study used the CGI only during the acute 4-day intervention; therefore, recall should not be a significant problem.
ACE Questionnaire. ACE is composed of 10 “yes” or “no” patient-reported questions, each asking whether or not the patient experienced an ACE. Three categories of ACEs are included: (1) types of abuse; (2) types of neglect; and (3) types of family dysfunction. Internal consistency has been reported at α = 0.83 for the sexual abuse scale and α = 0.57 for the physical/emotional abuse scale (Meinck et al. 2017).
Screen for Child Anxiety Related Emotional Disorders (SCARED-5). The SCARED-5 is a reduced version of the 41-item SCARED tool used to measure anxiety in children and adolescents. Higher scores indicate more anxiety. The selected 5 items have shown similar psychometric findings to the full-scale SCARED. It has been validated in the assessment of anxiety in adolescents; internal consistency ranges from 0.68 to 0.90 (Birmaher et al. 1999).
Insomnia Severity Index (ISI). The ISI is a 7-item self-report questionnaire assessing the nature, severity, and impact of insomnia. A 5-point Likert scale is used to rate each item with “0” indicating no problem and “4” indicating a very severe problem, yielding a total score ranging from 0 to 28. The total score is interpreted as follows: absence of insomnia (0–7); subthreshold insomnia (8–14); moderate insomnia (15–21); and severe insomnia (22–28). A cutoff score of 10 was optimal (86.1% sensitivity and 87.7% specificity) for detecting insomnia cases in the community sample. In the clinical sample, a change score of −8.4 points (95% CI: −7.1 to −9.4) was associated with moderate improvement as rated by an independent assessor after treatment. The ISI is considered to be a clinically useful tool as a screening device or as an outcome measure in insomnia treatment research. The ISI has been validated for use in the adolescent population; internal consistency is reported at 0.90 (Chung et al. 2011).
Columbia-Suicide Severity Rating Scale (C-SSRS). The C-SSRS (risk assessment version) is a multidimensional instrument that assesses suicidal ideation, intensity of ideation, and suicidal behavior. It has been validated in the assessment of suicidality in adolescents; internal consistency ranges from 0.73 to 0.95 (Posner et al. 2011). Suicidal ideation was assessed in this study and rated as positive or negative.
Self-Harm Likert Scale. The literature revealed only retrospective tools to measure nonsuicidal self-injury in adolescents. In lieu, a Likert scale was used daily to measure urges to self-harm. Patients were asked, “On a scale of 0 to 10, how strong are your urges to harm yourself? Zero represents no urges at all, and 10 represents an unbearable urge to harm yourself.”
Daily Patient Assessment. The registered nurse caring for the patient conducted a daily assessment of mood, affect, behavior, suicidal ideation, homicidal ideation, self-harming behaviors or thoughts, and side-effects related to the treatment according to unit standards.
Data analysis
Feasibility was measured as the ability to recruit and retain adolescents for the study. Success was set for 80% of enrolled patients to complete the TCT intervention and inpatient measures and 50% for follow-up measures. The low follow-up goal was set due to the difficulty of maintaining contact with this rural, mentally ill population.
Wilcoxon's Signed Rank test was used to evaluate a reduction in depression through pairwise comparisons at each time point compared to Day 0 (i.e., baseline and before treatment). Descriptive statistics was used to compare differences between each time point for all other outcomes, including anxiety, urge to self-harm, suicidality, and sleep. Means and standard deviations or frequencies and percentages were calculated, depending on the characteristic of the measurement associated with each outcome. Before data collection, four 1-hour training sessions were conducted to establish inter-rater reliability between clinicians administering the HAMD-17 during the TCT intervention. Online training cases were evaluated by five raters (two child adolescent psychiatrists and three nurses board certified in psychiatry); raters had 60% agreement initially and then agreement improved for subsequent cases to 100% agreement. Other measures were routinely collected by staff and did not require additional training. All analyses were performed using SAS statistical software version 9.4 (SAS Institute, Cary, NC) and SPSS version 22.0 (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0; IBM Corporation, Armonk, NY).
Results
Feasibility
Thirty-six patients were screened for study eligibility; 5 declined participation due to lack of motivation to complete the study. The remaining 31 patients agreed to undergo the TCT intervention. One patient was removed because of deviations in the protocol schedule. One patient was removed due to difficulty staying awake throughout the sleep deprivation phase. Twenty-nine (94%) completed the intervention and associated inpatient measures; 17 of 29 (58%) completed 1-week measures; 16 of 29 (55%) patients completed 1-month follow-up measures (Fig. 1).
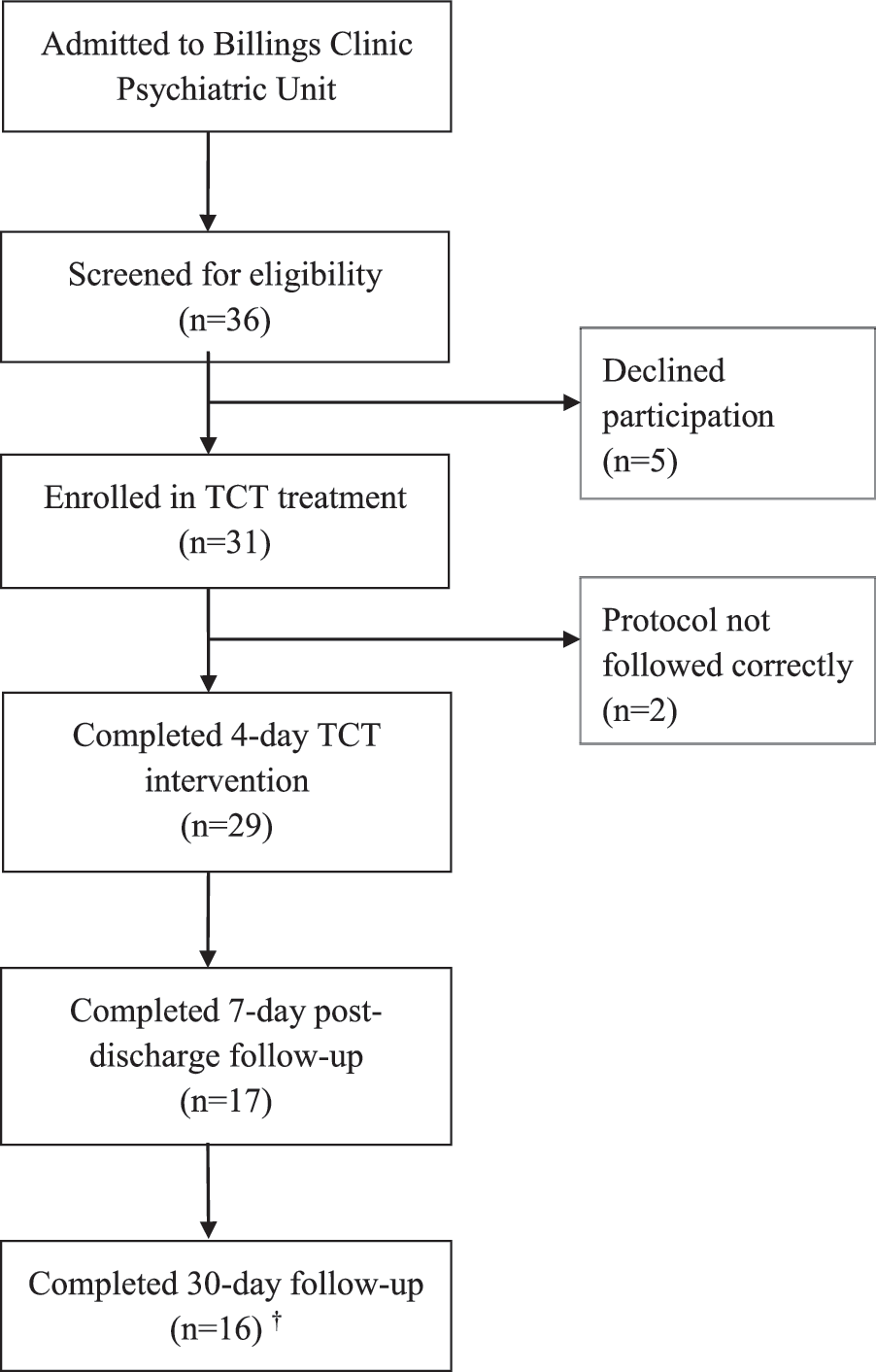
TCT Consort Flow Diagram. †13 patients completed both 7-day postdischarge and 30-day follow-ups. TCT, triple chronotherapy.
Sample
The mean age of adolescents was 15.5 years (±1.0); the majority was female (71%) and Caucasian (87%). All but one patient had a diagnosis of major depressive disorder; two had a diagnosis of bipolar disorder. The sample is described in Table 1. Forty-eight percent of patients received medication management before the intervention; 94% received medications during the TCT intervention. The majority of prescribed agents were antidepressants. Sleep aids were not given during the intervention (Table 2). Two patient guardians refused medication interventions during the hospitalization but consented to TCT as the primary form of intervention.
One patient positive for amphetamines and taking Adderall; one positive for benzodiazepines and not prescribed; and three positive for cannabis.
ACE, adverse childhood experience; ADHD, attention-deficit/hyperactivity disorder; S.D., standard deviation.
Clinical outcomes
By the end of the 4-day protocol following the final dose of light therapy, 26 (84%) of the 31 enrolled patients responded to the intervention as defined by a reduction in depressive symptoms of at least 50% from their baseline depression score; 24 (77%) achieved remission based on a HAMD-17 score of less than 8. At this time two patients were removed due to deviations from the protocol.
Of the 29 patients who completed the 4-day TCT intervention, 17 returned for a 1-week postdischarge follow-up. Of these patients, 76% (n = 13) maintained a clinical response, and 35% (n = 6) remained in remission. At 1-month follow-up, 16 patients completed the HAMD-17. Of these 16 patients, 13 had completed the 1-week postdischarge HAMD-17, and 3 had completed only the 4-day HAMD-17. Sixty-three percent (n = 10) maintained a clinical response, and 50% (n = 8) remained in remission. The overall scores of the patients are depicted in Figure 2, indicating that the levels of depression had decreased from baseline to 1-month follow-up. Initial response and follow-up mean depression scores as reported by the HAMD-17 are included in Figure 3A and B, respectively. The mean depression score was reported as severe before the start of the intervention (
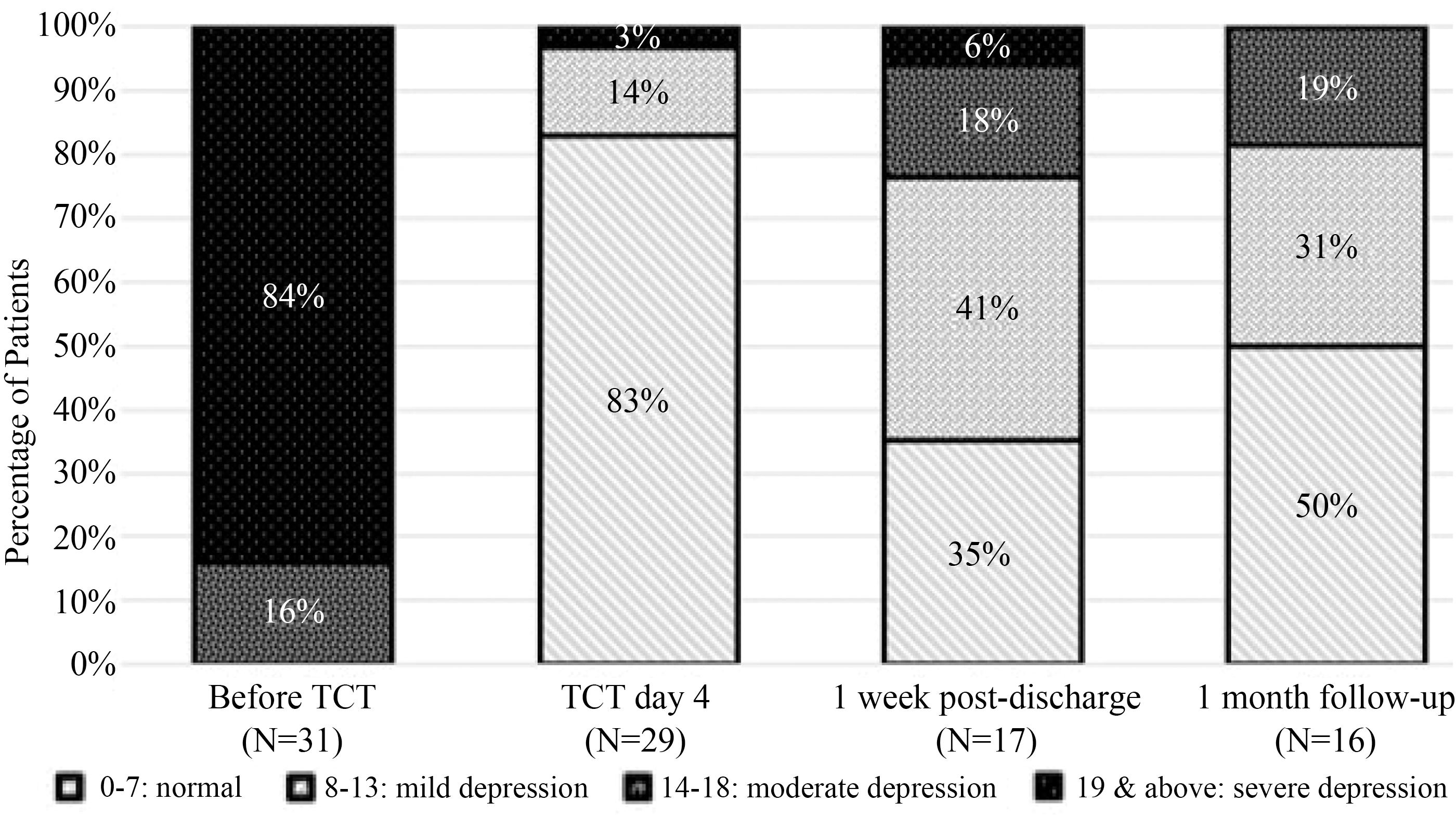
Levels of Depression Symptom over Time. A total of four levels of depression symptom were identified using HAMD-17: normal (score 0–7), mild depression (score 8–13), moderate depression (score 14–18), and severe depression (score 19 and above). HAMD-17, Hamilton Depression Scale-17; TCT, triple chronotherapy.
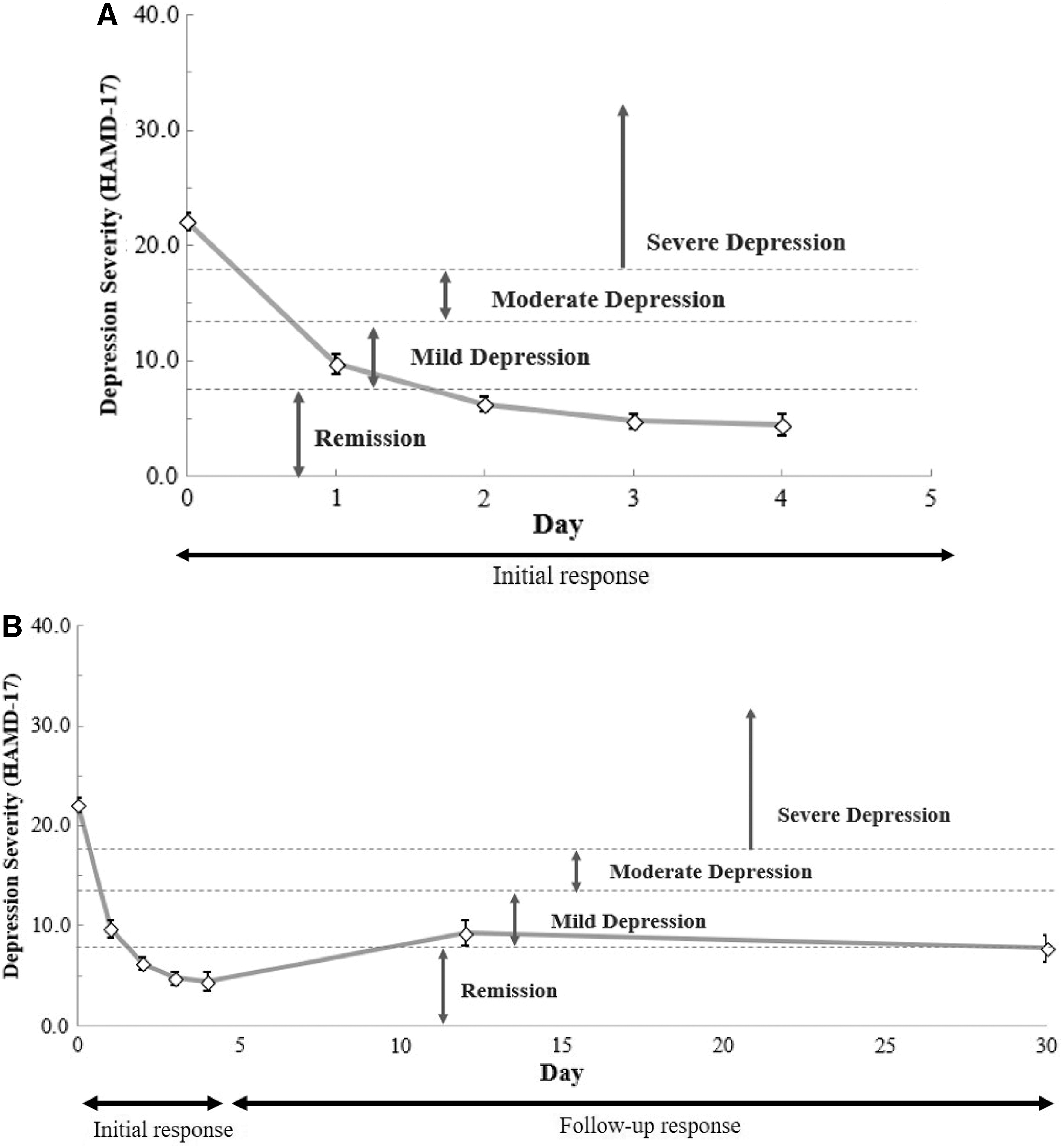
Antidepressant Response: Mean Score of HAMD-17.
Severity of illness (CGI-S) improved from a mean of 5.3 (±0.5) at baseline to 3.1 (±0.7) following the TCT intervention (p < 0.0001). Global improvement (CGI-I), rated as per the adolescent psychiatrist, had a mean score of 1.57 ± 0.74; the proportion of patients who were “very much to much improved” was 96.6%; specifically, 28 of the 29 patients who completed the intervention. The mean efficacy index score was 5 ± 2.54 (standard deviation 2.54) indicating a moderate therapeutic effect. The most common side effect was somnolence, particularly during the period of sleep deprivation. An increased risk for triggering a manic episode or a seizure was postulated; however, neither of these adverse events was reported. Longitudinal comparisons for each secondary outcome in the study (anxiety, self-harm, suicidality, and insomnia) also improved. Over the 4-day intervention, mean anxiety scores decreased from 5.1 ± 2.6 to 3.3 ± 3, insomnia scores decreased from 16 ± 6.1 (moderate insomnia) to 4.5 ± 4.6 (no insomnia), self-harm urge scores decreased from 5.2 ± 3.5 to 0.9 ± 2.1, and the percentage of patients reporting suicidal ideation decreased from 100% to 10%. Each of these measures sustained the marked response through the 1-week and 1-month follow-up periods. Clinical outcomes are included in Table 3.
Wilcoxon Signed-Rank Test: a p ≤ 0.05; b p ≤ 0.01. No statistical test applied to Suicidality across follow-up measures.
CGI-S, Clinical Global Impressions-Severity of Illness Scale; C-SSRS, Columbia-Suicide Severity Rating Scale; HAMD-17, Hamilton Depression Scale-17; ISI, Insomnia Severity Index; SCARED-5, Screen for Child Anxiety Related Emotional Disorders; S.D., standard deviation; TCT, triple chronotherapy.
Comparison of patients lost to follow-up (L-FU) (n = 9) and those who did FU (n = 20) indicated that one of nine L-FU was a nonresponder according to the CGI global improvement item (>2). The other eight responded to treatment. Depression scores were similar at baseline. On Day 4 the L-FU group exhibited increased depression, 6.56 ± 7.99 compared with 3.45 ± 4.33 FU group. One L-FU patient outlier in the L-FU group had a depression score of 23 at baseline and 25 on Day 4, which shifted the mean of the L-FU group. Mean age was the same in both groups. Rurality was the largest contributor to L-FU. Seven of the nine (77.8%) L-FU patients lived outside of the urban hospital county compared with 5 of 20 (10%) in the FU group.
Discussion
This was the first study to use adjunctive TCT in adolescents who were experiencing a moderate or severe depressive episode. This pilot study determined TCT to be a safe, rapid, and potentially effective adjunctive treatment for depression in the adolescent population. The 4-day TCT intervention resulted in an 84% response rate, and 77% of adolescents achieved remission of depressive symptoms.
Sixty-three percent of active participants in the study maintained a 1-month response, and half of the patients (50%) maintained remission. This rapid initial response to TCT makes it a particularly promising intervention in the acute treatment of depression and suicidality, yielding response and often remission in a matter of days rather than the 4 to 8 weeks traditionally associated with antidepressant treatment alone (Fochtmann 2010).
TCT was determined to be safe and well-tolerated in adolescents. Daytime somnolence was the most commonly reported side effect. Only one patient dropped out of the study due to inability to stay awake. No episodes of mania were noted. The 4-day TCT protocol of sleep–wake cycle manipulation and bright light therapy was easily adapted to an inpatient youth psychiatric setting. While 5 adolescents declined enrollment in the study, 29 of the 31 patients (94%) who did enroll completed the 4-day TCT intervention. Patient motivation to adhere to the rigorous protocol was supported by psychiatric nurses and other team members who spent one-on-one time with the patients to ensure successful completion of the intervention.
Because this is the first study to examine the use of TCT in adolescents, no adolescent studies are available for comparison; however, these results are consistent with findings from similar studies targeting adult patients with unipolar and bipolar depression (Wu et al. 2009; Echizenya et al. 2013; Benedetti et al. 2014; Sahlem et al. 2014). One of these studies by Echizeyna et al. (2013) found that 8 of 13 (62%) patients with treatment-resistant depression responded to TCT and maintained a response at Day 20, which was very similar to our 1-month response rate of 76%.
One randomized controlled trial in adults compared TCT (n = 32) to medication only (n = 17). The addition of TCT resulted in a significant decrease in depression at day 7 (p = 0.007) and week 7 (p = 0.02) (Wu et al. 2009). Response and remission rates were defined the same as in our study, but these rates were not reported, making comparison difficult. The largest trial in the literature by Benedetti et al. examined 143 adult patients with major depressive disorder; 23% of participants had attempted suicide, and 83% were drug resistant. The intervention resulted in a 70% response rate; 55% sustained response at 1 month. Response rates in this study were slightly higher at 1 month (63%). Remission was not reported in the Benedetti study (Benedetti et al. 2014).
The rapid response to TCT in reported studies makes it a particularly promising intervention in the acute treatment of depression and suicidality. Additional adjunctive treatments and augmentation strategies which accelerate traditional antidepressant treatment are emerging. Ketamine is one acute intervention, and the mechanism of its rapid antidepressant response is theorized to occur in the glutamatergic pathway (Abdallah et al. 2016; Feifel 2016). In addition, ketamine, as well as lithium and melatonin, may affect circadian rhythm which could impact depressive symptoms (Noguchi et al. 2016; Yoshikawa and Honma 2016; Duncan et al. 2017; Sun et al. 2017). A major limitation of ketamine is its potential hallucinogenic and dysphoric adverse effects. Newer areas of research must address safe and effective treatments, which can lead to a more rapid response in acute and emergent depression (Maalouf and Brent 2012). The use of chronotherapeutic interventions such as sleep deprivation, sleep phase advancement, and bright light therapy has some evidence in treating depression in adults with few side effects and may offer a safe and effective nonpharmacological adjunct treatment for depression in the adolescent population (Heiler et al. 2011).
For two patients in this study, antidepressants were clinically indicated but not started due to lack of parental consent. Both patients achieved a robust response to treatment with TCT alone. TCT may offer a safe nonpharmacological treatment for patients who do not want or cannot tolerate pharmacological interventions. In addition, parents and guardians appear to be especially pleased to be offered a nonpharmacological alternative to augment the standard treatment of depression.
These conclusions need to be considered in the context of the study limitations, including small sample size, lack of randomization or a control group, and other associated interventions, including hospitalization and medications. Despite coordination between inpatient and outpatient teams, loss to follow-up was a challenge in this study. The study hospital is a major referral center in the rural northwest region of the United States, with some patients traveling over 10 hours to receive treatment. Despite these factors, follow-up with 30-day measures by over half of the enrolled patients was achieved. Seven of nine patients L-FU lived outside of the urban hospital area and had to travel more than 60 miles each way to receive care.
Most patients were receiving group therapy and concurrent medication management for depression in the milieu. It is therefore possible that improvements were, in part, because of those interventions. Medications, including mood stabilizers, stimulants, and other medications (e.g., hydroxyzine), could potentially have an acute response for depression. Six patients who were not previously on these agents received them during hospitalization, which could have led to acute improvements. While 42% of the patients were receiving antidepressants on admission, 90% were discharged with antidepressants; the response to these agents as noted typically takes 4 to 8 weeks.
Given the ease of administration, lack of significant side effects, and inexpensive nature of the intervention, further study is warranted. Randomized controlled trials with combined adjunctive TCT and standard treatment compared to standard treatment alone are needed in the adolescent population. Research that examines the longitudinal effectiveness of adjunctive TCT and standard treatment compared to standard treatment alone is also warranted. Martiny et al. (2015) conducted a randomized controlled trial with the longest follow-up period of 29 weeks; however, they compared two adjunctive therapies, daily exercise and a variation of TCT. Inclusion of a usual treatment group would be important to control for the improvement seen with pharmacotherapy, group therapy, the structured hospital setting, and family therapy that are standard psychiatric care.
We believe that developmental and individual considerations regarding the sleep cycle warrant further study as well. Determining an adolescent's pattern of sleep before initiation of the TCT could allow the intervention to be individually tailored, which could improve adherence following discharge. For example, most adolescents do not prefer to rise early, and yet light therapy is administered at 7:00 am each day. School schedules must also be considered, and most are not conducive to adolescent sleep patterns. It would be interesting to test whether weekend sleep-in times would interfere with the sustainability of the response. The use of melatonin in the TCT protocol would also be a consideration for future studies based on the knowledge of its involvement in the sleep cycle. Further study may illuminate the interrelationships among sleep disorders, circadian rhythm, depression, and suicidality.
Conclusions
This innovative study found the use of TCT to be a potentially effective and safe option for the acute management of adolescent depression. Future trials using a randomized controlled design are essential to further clarify its impact.
Clinical Significance
While evidence-based treatments for the management of depression in adolescents exist, social stigma, perception that depression can be self-managed without treatment, and side effects of antidepressants all pose treatment barriers. Moreover, the two most widely used evidence-based treatments, antidepressants and cognitive behavioral therapy, have medium-to-small effect sizes, and a significant need exists to develop more effective strategies to manage depression in adolescents. This pilot study determined TCT to be a safe, rapid, and potentially effective adjunctive treatment for depression in the adolescent population. The 4-day TCT intervention resulted in an 84% response rate, and 77% of adolescents achieved remission of depressive symptoms at 1 month. Rapid initial response to TCT makes it a particularly promising intervention in the acute treatment of depression, yielding response and often remission in a matter of days rather than the 4 to 8 weeks traditionally associated with antidepressant treatment alone.
Footnotes
Disclosures
No funding was received for this study. Dr. Brant discloses that she is on the speaker's bureau for Genentech and Insys, but that role has no influence on this study. No conflicts of interest exist for the other authors.