
Abstract
Objectives:
Disruptive mood dysregulation disorder (DMDD) is characterized by nonepisodic irritability and has a high rate of comorbidity with attention-deficit/hyperactivity disorder (ADHD). This is the first study to explore the effects of aripiprazole combined with methylphenidate on clinical symptoms and cognitive functions in patients with DMDD and ADHD.
Methods:
Patients with DMDD and ADHD (the DMDD–ADHD Group, n = 24; aged 7–17 years) completed a 6-week, open-label trial of aripiprazole and methylphenidate. The pre- and posttreatment outcome measures included the parent-rated Swanson, Nolan, and Pelham Scale—version IV, Child Behavior Checklist, and self-reported Beck Youth Inventories-II, as well as a neuropsychological battery composed of the Children's Color Trail Test and Conner's Continuous Performance Test. The comparison group consisting of patients with ADHD (the ADHD Group, n = 27) was recruited to investigate the differences in clinical and neuropsychological profiles between the two groups at baseline.
Results:
The DMDD–ADHD Group showed worse irritability, disruptive behaviors, anxious/depressed symptoms, and social problems relative to the ADHD Group at baseline assessments. The combination treatment significantly improved irritability, externalizing symptoms, depression, anxiety, attention, social problems, and reaction time variability. The effect sizes of reductions in parent-rated irritability, oppositional defiant symptoms, and inattention were comparable (Cohen's d = 1.26, 1.11, and 1.40, respectively).
Conclusions:
This pilot study showed the tolerability of the aripiprazole/methylphenidate combination by patients with DMDD and ADHD and its efficaciousness for treating clinical symptoms and for improving cognitive function. Further randomized, controlled, cross-over studies are needed.
Introduction
D
Emerging literature suggests that the longitudinal course, family history, and pathophysiology of DMDD are distinct from those of bipolar disorder (Leibenluft 2011). In addition, evidence from follow-up studies also differentiates DMDD from disruptive behavior disorders by its longitudinal association with unipolar depression and anxiety (Vidal-Ribas et al. 2016). Clinically, youths with DMDD display challenging symptoms leading to significant impairments, including social difficulties, school suspension, and mental health service (Copeland et al. 2013; Deveney et al. 2015). The unique etiological underpinnings of DMDD and the proneness of patients with DMDD to long-term psychiatric adverse outcomes indicate a specific therapeutic strategy as early as possible for these youths with severe irritability and related risky behaviors.
Irritability and aggression in the context of attention-deficit/hyperactivity disorder (ADHD) may respond to methylphenidate (Shaw et al. 2014). However, the use of methylphenidate monotherapy for treating youths with DMDD and ADHD had its limitations in previous studies. First, the magnitude of the effect sizes for improvement of irritability was only approximately half of that for improvement of ADHD symptoms (The MTA Cooperative Group 1999; Fernández de la Cruz et al. 2015; Baweja et al. 2016). Moreover, children with ADHD and comorbid severe aggression may need adjunctive medications to achieve symptom remission (Blader et al. 2009; Aman et al. 2014). Since most previous clinical trials in patients with ADHD assessed irritability as a secondary outcome measure and did not recruit patients with the diagnosis of DMDD, youths with severe irritability similar to those with DMDD may not respond to methylphenidate adequately.
Second, methylphenidate did not show superiority to community care in reducing internalizing symptoms and social problems (The MTA Cooperative Group 1999), which often occur with irritability and are burdensome to patients with DMDD. Third, methylphenidate may induce irritability and mood lability in children and adolescents with ADHD (Manos et al. 2011), and that may exacerbate the baseline symptoms of DMDD. Accordingly, medication other than methylphenidate monotherapy is indicated for the treatment of patients with DMDD and ADHD.
Well-supported evidence showed that atypical antipsychotics decrease irritability and aggression in children and adolescents, especially those with autism spectrum disorders (ASDs) (Scotto Rosato et al. 2012). Moreover, one open-label study showed positive effects of low-dose risperidone on irritability and global functioning in youths with severe mood dysregulation (Krieger et al. 2011). Those findings imply that atypical antipsychotics may be effective pharmacological treatments for youths with DMDD. Although the long-term metabolic adverse effects of antipsychotics are a concern for both clinicians and parents (Correll and Blader 2015), interim use of these medications should still be considered for those youths with severe irritability and accompanying safety issues or significant dysfunctioning.
Aripiprazole is well tolerated in pediatric patients and showed efficacy for aggression comparable to that of risperidone (Scotto Rosato et al. 2012). It is also indicated for depression in adults with the proposed pleiotropic mechanism on regulation of monoamine transmission (Han et al. 2015). Since youths with chronic irritability are prone to co-occurring depressive symptoms (Copeland et al. 2013), aripiprazole may be a potentially optimal treatment for patients with DMDD.
Children and adolescents with DMDD have an increased risk of psychiatric hospitalization and involvement in juvenile justice (Copeland et al. 2013; Deveney et al. 2015), and also cause their family further stress. Although parents may need to receive parent management training to address irritability and the associated aggressive behaviors of patients with DMDD (Waxmonsky et al. 2016), effective treatments other than behavioral modification in the early phase of the illness might help reduce adverse correlates of DMDD and parental overload.
In view of the high rate of comorbidity between DMDD and ADHD (Copeland et al. 2013; Deveney et al. 2015), we proposed that the aripiprazole/methylphenidate combination would effectively decrease irritability and its co-occurring psychopathology in patients with DMDD and ADHD. In addition, researchers have limited information regarding the neurocognitive profiles of patients with DMDD (Uran and Kilic 2014; Pagliaccio et al. 2017). Therefore, in this present study, we examined the effects of aripiprazole combined with methylphenidate on both clinical symptoms and cognitive functions in youths with DMDD and ADHD.
Method
Study design and subjects
This study was a 6-week, open-label investigation of aripiprazole and methylphenidate in patients with DMDD and ADHD (registered at
Children and adolescents aged 7–17 years and free of any psychotropic medication for at least 12 months were eligible for recruitment in this clinical trial. All of them were screened and recruited at the psychiatric outpatient department of a university hospital in Northern Taiwan between November 2014 and June 2017. Those who met the diagnostic criteria of both DMDD and ADHD according to the DSM-5 were designated the DMDD–ADHD Group. Patients who were diagnosed as having ADHD, but not DMDD, were allocated to the ADHD Group (and served as the baseline control group).
Exclusion criteria were intelligence quotient (IQ) <70, pervasive developmental disorder, bipolar disorder, psychosis, active drug abuse, suicidal ideation, unstable medical illness, known allergic reaction to methylphenidate or aripiprazole, and current pregnancy. Before recruitment, all of the patients and their parents provided written informed consent after the study had been thoroughly explained to them. The study was approved by the Institutional Review Board of Tri-Service General Hospital, National Defense Medical Center, Taipei, Taiwan.
Assessments
Clinical and neurocognitive profiles were compared between the DMDD–ADHD Group and ADHD Group at the initial assessment. All the participants in both groups completed a baseline diagnostic interview based on DSM-5, symptoms severity inventory, and neuropsychological tests, including an intelligence test. The treatment group was assessed by the same inventories and neuropsychological tests again at the end of 6 weeks of treatment.
All diagnostic interviews were administered to prospective subjects and parents individually by two child psychiatrists (C.-B.Y. and P.-Y.P.) and one clinical psychologist (A.-T.F.). Information was gathered from children, parents, and teachers to assess cross-domain impairments associated with DMDD. The confirmed diagnosis of DMDD was based on a consensus of all these three experienced interviewers. Full-scale IQ (FSIQ) was measured by using the Wechsler Intelligence Scale for Children 4th edition-Chinese version (Wechsler 2007).
The subjects' ADHD and oppositional defiant disorder (ODD) symptoms were evaluated by using the Chinese version of the Swanson, Nolan, and Pelham, version IV scale—parent form (SNAP-IV), a 26-item scale derived from Diagnostic and Statistical Manual of Mental Disorders, 4th ed. (DSM-IV; American Psychiatric Association 1994) criteria for the core symptoms of ADHD and ODD (symptoms of inattention, Item 1–9; symptoms of hyperactivity/impulsivity, Item 10–18; symptoms of ODD, Item 19–26) (Gau et al. 2008). The Child Behavior Checklist—Parent Report Form (CBCL), composed of 113 emotional, behavioral, and social problem items, was used to measure the subjects' internalizing and externalizing symptoms (Yang et al. 2001). The Chinese version of the Beck Youth Inventories—second edition (BYI-II) is a self-report scale for assessing anxiety, depression, anger, disruptive behavior, and self-concepts in youths between ages of 7 and 18 years old (Cho et al. 2009).
In addition, all patients underwent neurocognitive function evaluations using the Conners' Continuous Performance Test II Version 5 (CPT-II) and the Children's Color Trails Test (CCTT). The CPT-II is a computer-administered visual paradigm to measure processes related to attention, response inhibition, signal detection, and other aspects of executive function (Conners 2000). The CCTT measures sequencing, visual scanning, graphomotor skills, and executive control in children based on their concepts of number and color (Llorente et al. 2003).
The primary outcome efficacy measure was a subscale of irritability generated from parent-rated SNAP-IV by summing up three ODD items: “Loses temper,” “Is touchy or easily annoyed by others,” and “Is angry and resentful.” This measurement has been applied in previous literature to evaluate treatment effects in individuals with irritability (Fernández de la Cruz et al. 2015). In the current study, this parent-reported irritability scale showed high internal consistency (Cronbach's alpha = 0.90). For its convergent validity, we examined the correlation between this measurement and a scale consisting of items describing irritability drawn from the CBCL (Stringaris et al. 2012). Items in the CBCL-derived scale included “Stubborn, sullen, or irritable,” “Sudden changes in mood or feeling,” and “Temper tantrum or hot temper.” The correlation between these two scales was high (Pearson's correlation r = 0.80).
Assessments of drug safety during the treatment period were based on records of adverse events spontaneously reported either by patients or parents at week 2 and 6. The Simpson–Angus Scale, Barnes Akathisia Rating Scale, and the Abnormal Involuntary Movement Scale were applied for assessments of extrapyramidal symptoms (EPS). The change in body weight from initial to endpoint was used to assess the metabolic effects of the treatment.
Pharmacological intervention
Participants were seen by the principal investigator (C.-B.Y.) at baseline and week 2 to titrate the doses of aripiprazole and methylphenidate needed to achieve the greatest symptom reduction and tolerability. Aripiprazole was given at an initial dose of 2.5 mg at bedtime and could be increased to a maximum of 5 mg/day. The decision to start benzhexol hydrochloride for EPS was allowed and based on clinical judgment.
Statistical analyses
All statistical analyses were performed with SPSS software version 17 (SPSS, Inc., Chicago, IL). To compare the baseline characteristics between the two groups, we used the chi-square test or Fisher's exact test for categorical variables and the Student's t test for continuous variables. A mixed model was used to analyze primary and secondary outcome measures for its advantage in dealing with missing values. Potential confounders, including age, gender, FSIQ, medication dosage, comorbidities, and body mass index, were controlled separately.
All tests were two-tailed and p-values of 0.05 or less were considered statistically significant. A Bonferroni correction was made for multiple comparisons in efficacy analyses. Standardized mean difference effect sizes (Cohen's d) of the combination of methylphenidate and aripiprazole were then computed by calculating differences between the baseline and end point means at week 6 and dividing the results by pooled standard deviations (SDs).
Results
Thirty-one patients with DMDD and ADHD were recruited and enrolled as the DMDD–ADHD Group. They were treated with aripiprazole and methylphenidate for 6 weeks (Fig. 1). Two patients dropped out of the study before the treatment. The reasons for screening failure were a physical problem (intracranial cyst) and withdrawal of consent. A total of 29 patients received the pharmacological intervention, but only 24 patients completed the 6-week trial and had analyzable data. Two patients discontinued the study because of adverse events (one due to vomiting and one due to lethargy and dysphoric mood), and three patients were lost to follow-up. All 24 patients in the DMDD–ADHD Group and 27 patients in the ADHD Group completed baseline assessments, including inventories and neuropsychological tests.
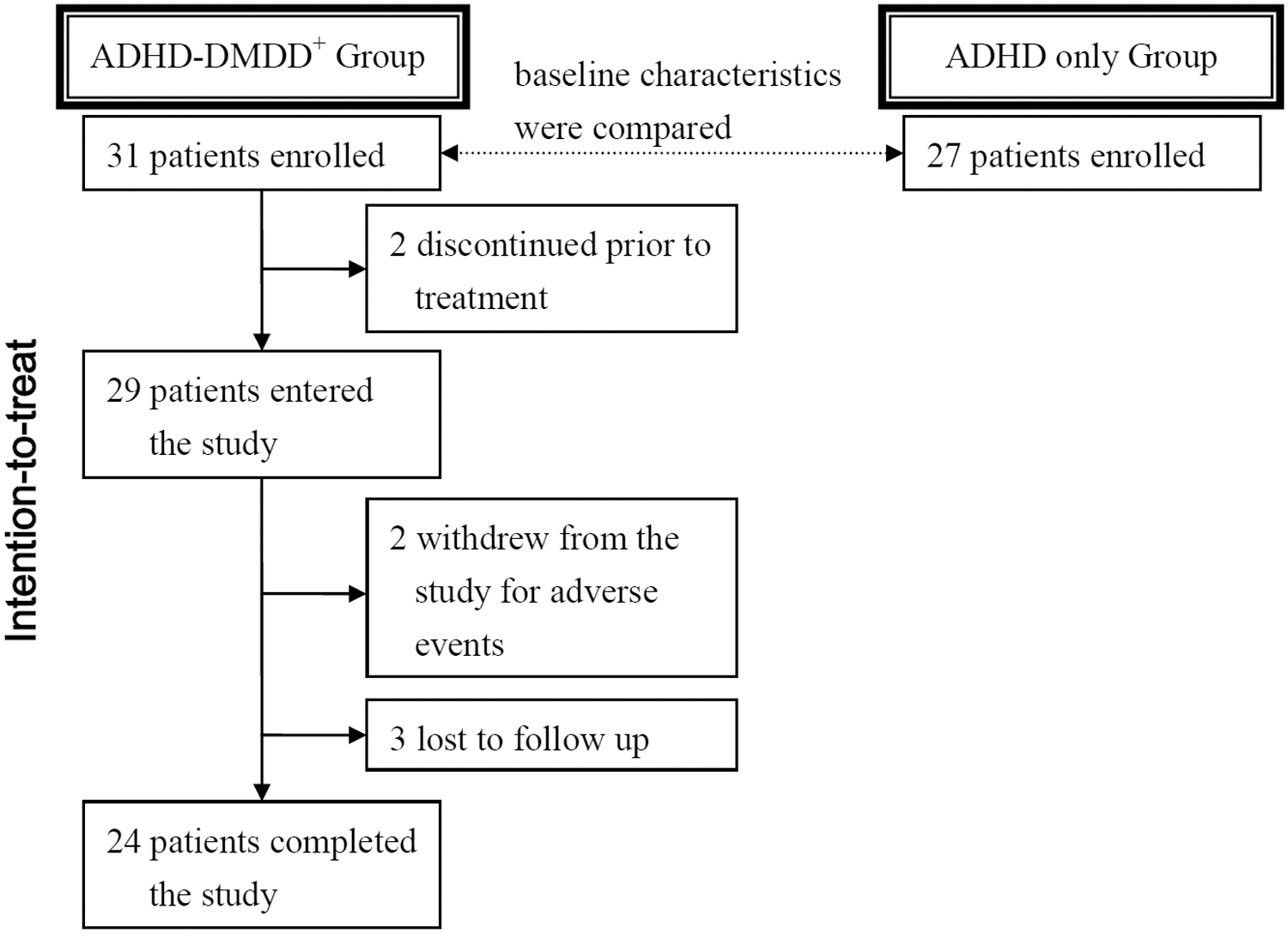
Flow diagram of patient disposition during the study.
Patient characteristics
The characteristics of the sample are presented in Table 1. There were no differences in demographics between the DMDD–ADHD Group (DA) and the ADHD Group (A). Specifically, there were no significant differences in age (mean age in years: DA 10.67 [SD = 2.37], A 10.45 [SD = 2.47], t = 0.35, p = 0.729), gender distribution (% male: DA 83.9, A 81.5, χ2 = 0.06, Fisher exact test p = 1.000), or full-scale IQ (DA 104.20 [SD = 12.41], A 99.07 [SD = 10.56], t = 1.67, p = 0.101). There were also no significant differences in body mass index, comorbidities, and family composition between the two groups.
Fisher's exact test.
DMDD, disruptive mood dysregulation disorder; ADHD, attention-deficit/hyperactivity disorder; IQ, intelligence quotient; ODD, oppositional defiant disorder; SD, standard deviation.
Clinical characteristics
Table 2 shows the comparison of clinical ratings with caregiver-reported and self-reported inventories between the DMDD–ADHD Group and the ADHD Group. The DMDD–ADHD Group had higher irritability and ODD symptoms scores in the SNAP-IV than the ADHD Group, but there was no difference in inattention and hyperactivity symptom scores. T scores of CBCL subscales revealed that patients of DMDD–ADHD Group had more severe symptoms in anxious/depressed mood, social problems, rule-breaking behavior, and aggressive behavior than patients of the ADHD Group. There were no differences in CBCL subscale T scores of withdrawn/depressed symptoms, somatic complaints, thought problems, and attention problems.
Bold values are statistically significant.
SNAP-IV, Swanson, Nolan, and Pelham Scale—version IV; ODD, oppositional defiant disorder; CBCL, Child Behavior Checklist; BYI-II, Beck Youth Inventories-II; CCTT, Children Color Trail Test; CPT-II, Conner's Continuous Performance Test; DMDD, disruptive mood dysregulation disorder; ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation.
Patients with comorbid DMDD and ADHD reported more severe symptoms of angry and disruptive behavior than those with ADHD only by the BYI-II. There were no differences in the BYI-II subscale T scores of self-concept, anxiety, and depression.
Neuropsychological measures of the two groups at baseline are summarized in Table 2. There were no group differences on the Color trails 1 and Color trails 2 time score in the CCTT; however, DMDD–ADHD Group had a significantly lower Interference scores compared with the ADHD Group. On the CPT-II, the DMDD–ADHD Group had a significantly lower Hit-RT-block-change score than ADHD Group. There were no significant group differences on detectability, variability, errors of omission, errors of commission, reaction time, and perseveration.
Medication
At the end of the 6-week treatment, patients in the DMDD–ADHD Group received their final dosage of aripiprazole ranging from 2.5 to 5 mg/day (mean dosage 4.17 [SD = 1.20] mg/day, 0.11 [SD = 0.04] mg/kg/day) and methylphenidate ranging from 10 to 45 mg/day (mean dosage 22.71 [SD = 8.47] mg/day, 0.61 [SD = 0.22] mg/kg/day). One patient received benzhexol hydrochloride 2 mg/day for subjective wrist rigidity after being treated with aripiprazole 5 mg/day.
Efficaciousness
Table 3 presents the changes in inventory scores for the DMDD–ADHD Group from baseline to week 6. Significant improvement was seen at week 6 in all SNAP-IV subscale scores, in six of the eight CBCL subscale scores (i.e., in anxious/depressed symptoms, social problems, thought problems, attention problems, rule-breaking behavior, and aggressive behavior but not in withdrawn/depressed symptoms and somatic complaints), and in three of five BYI-II subscale scores (i.e., in anxiety, depression, and angry).
Bold values are statistically significant.
SNAP-IV, Swanson, Nolan, and Pelham Scale—version IV; ODD, oppositional defiant disorder; CBCL, Child Behavior Checklist; BYI-II, Beck Youth Inventories-II; CCTT, Children Color Trail Test; CPT-II, Conner's Continuous Performance Test; DMDD, disruptive mood dysregulation disorder; ADHD, attention-deficit/hyperactivity disorder; SD, standard deviation; CI, confidence interval.
As presented in Table 3, from baseline to week 6, the CCTT performance score, all measures of the CPT-II, except variability, which showed a statistically significant improvement, and other measures remained unchanged at week 6.
Safety and tolerability
The adverse events of pharmacological treatment are presented in Table 4. The most common side effects were decreased appetite and vomiting. Two patients (6.90%) discontinued due to serious adverse events, including vomiting, lethargy, and dysphoric mood. Throughout the study, there were six reports of EPS, including involuntary facial expression, muscular rigidity, and akathisia. All EPS were of mild intensity and not severe enough to lead to discontinuation. From baseline to week 6, the mean weight change in our sample was 2.67 (SD = 3.94) kg.
AIMS, Abnormal Involuntary Movement Scale; BAS, Barnes Akathisia Scale; SAS, Simpson-Angus Scale.
Discussion
The results of this pilot study showed the efficaciousness of the combination of aripiprazole and methylphenidate in reducing irritability, externalizing symptoms, depression, anxiety, attention, and social problems in youths with DMDD. Given the existing evidence of efficaciousness of aripiprazole in the treatment of aggression in children (Scotto Rosato et al. 2012) and irritability in youths with ASD (Fung et al. 2016), our preliminary findings further demonstrated that when combined with methylphenidate aripiprazole may also reduce the internalizing symptoms which are often concurrent with irritability and disruptive behaviors in youths with DMDD and ADHD.
At baseline, the children of our sample with DMDD and ADHD had more severe irritability, ODD symptoms, and aggressive and rule-breaking behaviors compared to those with ADHD only, although there were no between group differences in the severity of their ADHD symptoms. In addition, patients with DMDD and ADHD exhibited more severe internalizing symptoms, specifically depressed and anxious mood, as well as worse social problems, in line with previous findings in children (Dougherty et al. 2014; Fernández de la Cruz et al. 2015) that irritability is associated with internalizing symptoms and contributes to impairment independently. Since youths with chronic irritability had higher risk of depressive and anxiety disorders as their longitudinal outcomes (Brotman et al. 2006; Stringaris et al. 2009), our findings pointed to the need for early awareness of the co-occurrence of irritability and internalizing symptoms and its implications for treatment.
Regarding the CCTT performance of the two groups at baseline, interference scores were lower in the DMDD–ADHD Group than the ADHD Group. Interference scores reflect the efficiency of rapid switching between two tasks independent of motor speed and visual scanning speed (Arbuthnott and Frank 2000). Given that the DMDD–ADHD Group had higher anxious/depressed symptom score, we speculated that the patients in this group may be more anxious and concerned about their performance during the tests and therefore more aroused and better able to maintain their attention (Harmon-Jones et al. 2013).
The two groups of our sample had comparable CPT-II baseline scores on all measures except Hit-RT-block-change, which was lower in the DMDD–ADHD Group. The score provides information about vigilance and reflects change in reaction time across the duration of the test. Low values indicate that responses became quicker as the test progresses. Our patients with DMDD and ADHD maintained a higher level of vigilance during the test. Greater vigilance might also be compatible with our speculation that affect with higher motivational intensity modulate performance on the CPT-II (Vloet et al. 2010; Ruf et al. 2017).
After 6 weeks of treatment with aripiprazole and methylphenidate, patients with DMDD and ADHD had significant improvement in irritability and ODD symptoms other than ADHD symptoms. In addition, effect sizes of symptom reduction in parent-rated irritability, ODD, and ADHD were comparable. Although aripiprazole had been reported to be an effective treatment for overall aggression in youths (Scotto Rosato et al. 2012) and for irritability in children with ASD (Fung et al. 2016), no previous study demonstrated its efficaciousness for irritability in patients diagnosed with DMDD. To the best of our knowledge, this is the first study to explore the efficaciousness of the aripiprazole/methylphenidate combination in reducing irritability in DMDD patients with comorbid ADHD. Our findings concurred with a previous study showing that low-dose atypical antipsychotic, risperidone, significantly decreased irritability scores in youths with severe mood dysregulation (Krieger et al. 2011).
Compared to a trial of stimulant monotherapy in patients with comorbid DMDD and ADHD, which showed a modest degree of improvement (Baweja et al. 2016), we observed larger reduction in irritability and ODD symptoms, as well as social problems. Since the rate of comorbidity between DMDD and ADHD is high (Brotman et al. 2006; Copeland et al. 2013; Dougherty et al. 2014), effective treatment is urgently needed. The results of our study suggest that aripiprazole combined with methylphenidate might be an efficacious therapeutic choice for this population.
Notably, improvements were also seen in anxious/depressed symptoms in our DMDD-ADHD Group, both in their parent-rated and self-rated inventory scores, although they remained significantly impaired in many domains as indexed by some CBCL scores in (or close to) the clinical range. Previous literature has reported that ADHD patients may exhibit negative change in emotions after receiving stimulant treatments (Manos et al. 2011). Those negative emotions included emotional lability, dysphoria, anxiety, and depressed mood. However, augmentation strategies with low-dose aripiprazole have been approved for the treatment of depression (Berman et al. 2007) and might help improve anxiety symptoms (Pignon et al. 2017). Accordingly, other drugs combined with aripiprazole may be associated with the reduction of anxious/depressed symptoms, as that took place in the current study.
Moreover, analysis of the neuropsychological battery data indicated significant improvement in reaction time variability in the treatment group, which is in line with the generally positive effects of methylphenidate on CPT in children with ADHD (Coghill et al. 2014). This is also the first trial to demonstrate that the aripiprazole/methylphenidate combination improves cognitive function in patients with DMDD and ADHD. The effect sizes of neurocognitive deficits (compared with behavioral symptoms change) in children with ADHD are much smaller (Pievsky and McGrath 2017), and neuropsychological heterogeneity within ADHD samples is high. Thus, the effect of methylphenidate on cognitive function may not be statistically significant in a relatively small sample such as ours. Nevertheless, methylphenidate has been found to improve variability in ADHD more than response inhibition and reaction time (Coghill et al. 2014). Hence, we observed that variability was significantly improved at the end of treatment.
However, we did not observe an improvement in CCTT performance after treatment with aripiprazole and methylphenidate. Our finding is compatible with previous studies showing no effect of methylphenidate on working memory networks (Arbuthnott and Frank 2000; Rubia et al. 2014).
The medication was generally well tolerated throughout the 6-week study, with most adverse effects diminished from baseline to the end of the treatment, except that two subjects discontinued due to intolerable physical or mood symptoms. The results suggested that the combination of aripiprazole and methylphenidate can be safely used in children with DMDD and ADHD. Moreover, low-dose aripiprazole may mitigate common side effects of methylphenidate in children and adolescents, including appetite suppression, growth restriction, sleep disturbances, mood lability, and tics (Thapar and Cooper 2016). EPS and metabolic abnormalities associated with the administration of aripiprazole may be reasons for concern. As for weight gain induced by antipsychotics, close monitoring with early intervention through lifestyle management is currently recommended (Krill and Kumra 2014).
Several limitations of this study need to be addressed. First, the open label design leading to expectancy bias in scoring may inflate observed treatment effects. Besides, we could not rule out any time effect for the lack of a placebo arm. However, this is an exploratory study to examine the efficaciousness and safety of aripiprazole combined with methylphenidate in patients with DMDD and ADHD. It is important to note that not only irritability and disruptive behaviors but also depressed and anxiety symptoms were reduced after treatment, according to both parent-rated and patient-rated inventories, although the possibility of placebo effects with across-the-board improvements still could not be ruled out.
Second, we used the combination of two psychotropic agents as our intervention. Future cross-over studies are needed to definitively confirm the advantages of combination therapy over monotherapy with either medication. The two-arm studies with aripiprazole/methylphenidate combination therapy and methylphenidate monotherapy (added placebo) would also provide information about the differences between these two treatment regimens (Aman et al. 2014). Third, although our sample size is not significantly smaller than sample sizes in previous studies in DMDD patients (Waxmonsky et al. 2008; Dickstein et al. 2009; Krieger et al. 2011), detection of the cognitive effects of pharmacological treatment may require larger studies.
Fourth, all our subjects were recruited from a university hospital clinic. Hence, the representativeness of the study sample and the generalizability of the results should be considered. Fifth, we did not obtain the symptom ratings at regular intervals but only evaluated the subjects' symptoms pre- and posttreatment. Therefore, we did not have enough information regarding the symptom change within the period of treatment. Sixth, for comparisons between groups at baseline, the possibility for type I error may increase due to multiple simultaneous statistical tests. Additional limitation includes short study duration. Further investigation over an extended time frame is merited.
Conclusions
The combination treatment of low-dose aripiprazole and methylphenidate was associated with the significant improvements in both clinical symptoms and cognitive function in patients with DMDD and ADHD. Our findings indicate that aripiprazole/methylphenidate combination may be an efficacious treatment not only for irritability but also for depressive/anxiety symptoms. Further controlled and cross-over trials are warranted given these promising results.
Clinical Significance
This study provides insight into the efficaciousness of aripiprazole/methylphenidate in the treatment of irritability in children with DMDD and ADHD, as well as their impaired cognitive functions and co-occurring internalizing symptoms. For those patients with severe irritability and comorbid emotional problems, our findings offer preliminary evidence of combination of aripiprazole and methylphenidate as an alternative for clinicians to provide early and adequate interventions.
Footnotes
Acknowledgments
The authors thank Dr. Ellen Leibenluft, NIMH, and the patients and their parents for their participation.
Disclosures
No competing financial interests exist.