
Abstract
Objectives:
Medication nonadherence constitutes a major problem in adolescent psychiatry. Previous studies have identified various factors associated with nonadherent behavior. The aim of this study is to explore adolescents' health beliefs and subjective perceptions relating to psychotropic medication, and to statistically link these to reported medication adherence.
Methods:
The findings presented in this study are part of the multicenter SEMA study (Subjective Experience and Medication Adherence in Adolescents with Psychiatric Disorders). Patients 12–18 years of age were included, who had been treated with a psychotropic medication for at least 2 weeks. The validated MARS (Medication Adherence Rating Scale) and the QATT (Questionnaire on Attitudes Toward Treatment) were used to measure adherence, and a qualitative semi-structured interview was conducted to examine patients' subjective experiences and perceptions. A conventional content analysis was conducted, and Fisher's exact tests were performed to analyze group differences between completely adherent and not completely adherent patients.
Results:
A total of 64 patients were included in the study. 40.6% (n = 26) were classified as not completely adherent. Distribution patterns of answers to 7 out of 64 questions showed statistically significant group differences between completely and not completely adherent patients. Patients with lower adherence reported the following: feeling worse after taking medication; a lower sense of self-efficacy concerning the improvement of their symptoms; a less trustful physician–patient relationship; a worsened attitude toward medication after experiencing adverse events/“side effects”; less support from their relatives; and fewer individuals in their family who were fully informed about their condition.
Conclusions:
To our knowledge, this is the first interview-based study to investigate subjective experiences and health beliefs of adolescents with psychiatric disorders and to correlate these findings with rates of medication adherence. The study results will be useful for the development of tools and approaches to increase medication adherence, for example, psychoeducation programs and personalized treatment concepts.
Introduction
A
In child and adolescent psychiatry, several studies concerning rates of medication adherence and its impact have been conducted.
In the NIMH Collaborative Multisite Multimodal Treatment Study of Children with ADHD (MTA), 24.5% of attention-deficit/hyperactivity disorder (ADHD) patients overall were found to be nonadherent in an analysis using saliva samples as an assessment measure, and only 53.5% of the participants were adherent at all four time points of measurement (Pappadopulos et al. 2009). In the COMPLY study, which also investigated children and adolescents with ADHD, authors found medication nonadherence rates of 32.5% for nonstimulant (atomoxetine) medication and 25.8% for psychostimulant medication, which increased slightly over time (Wehmeier et al. 2015). In previous studies concerning medication adherence to psychotropic medication in adolescents, nonadherence rates ranged from 6% to 62% (Häge et al. 2018), demonstrating that nonadherence to medication is a clinically relevant problem in this population.
Adherence can be measured in various ways, for example, using medication possession ratios (the ratio of the number of days for which a patient is supplied with medication to the total number of days in a predefined time period), saliva samples, interviews with patients and/or parents, and self-report questionnaires (Pappadopulos et al. 2009; Gajria et al. 2014; Häge et al. 2018). To date, no standard assessments for medication adherence have been established, and due to inconsistent definitions of adherence and varying assessment approaches, cross-study comparisons appear to be rather difficult (Häge et al. 2018).
Several studies have investigated reasons for medication nonadherence in children and adolescents, mostly focusing either on a specific diagnosis or on one type of psychotropic medication. For example, medication nonadherence has been associated with adolescents' subjective beliefs about their medication, the experience of adverse events (“side effects”), and the type of prescribed medication (Ferrin et al. 2012; Gajria et al. 2014; Wang et al. 2016; Emilsson et al. 2017). There is currently no validated intervention program for enhancing medication adherence in adolescents with psychiatric diagnoses that is routinely applied in clinical practice. This is probably related to the complexity of the phenomenon and to the poor understanding of causes of medication nonadherence. Nevertheless, interventions such as motivational interviewing have been reported to improve adherence rates in clinical studies (Hamrin and Iennaco 2017). To identify the range of reasons for adolescents' medication nonadherence and to generate adequate intervention programs, it is important not only to examine specific factors more closely but also to gain a broader understanding of the subjective experiences, health beliefs, thoughts, and perceptions of this subgroup.
This study therefore aimed to explore cross-disorder factors influencing adherence and nonadherence to psychotropic medication in adolescent patients suffering from psychiatric disorders. We conducted a comprehensive survey of adolescents' health beliefs, perceptions of their own course of disease, experienced symptoms and physician–patient relationship, their individual appraisal of positive effects from psychotherapy and/or medication, thoughts on adverse events, and thoughts on disease-related interactions with their friends and families. We further sought to relate these findings to patients' reported medication nonadherence to statistically link subjective perceptions to nonadherent behavior, and thus gain a better insight into aspects associated with medication nonadherence.
Methods
The findings reported in this study are part of the multicenter SEMA study (Subjective Experience and Medication Adherence in Adolescents with Psychiatric Disorders), which explored the subjective experience of adolescents with psychiatric disorders, their health beliefs, and the association thereof with medication adherence.
Study centers that contributed data to these findings were the Department of Child and Adolescent Psychiatry and Psychotherapy at the Central Institute of Mental Health, University of Heidelberg, in Mannheim and the AWO (Arbeiterwohlfahrt; Workers' Welfare Association) Psychiatric Center in Königslutter am Elm and its connected outpatient clinics in Wolfsburg and Braunschweig (Germany). The study protocol was approved by the Ethics Committee II of the Medical Faculty Mannheim, University of Heidelberg (May 2014). Data collection took place from September 2014 to July 2016.
Study population
Inclusion criteria were as follows: patients' age between 12.0 and <18.0 years; psychotropic medication for a psychiatric disorder, which had been prescribed for at least 2 weeks at the time of inclusion; and a general medical condition that allowed participation. Both outpatients and inpatients were included. Participants and their parents/legal guardians received informed assent/consent documents explaining the study and its potential risks and benefits. Informed assent and consent forms were signed before inclusion. In addition to the participating adolescent, one parent/legal guardian as well as the treating physician were asked to take part in this study by filling out a questionnaire.
Assessments
Six different instruments, quantitative and qualitative, were used for data acquisition in the SEMA study.
To collect data on the subjective experience of illness and course of disease, a qualitative semistructured interview was conducted. The interview was based on the approach used in an earlier pilot study by our research group (Märker et al. 2011). It comprises 72 items concerning 4 main topics: course of disease (11 items), treatment (27 items), physician–patient relationship (16 items), and family/environment (18 items).
Adherence to medication was self-assessed by the participants using items 1–4 of the patient-reported Medication Adherence Rating Scale (MARS), which was developed for use in adult psychiatric patients and consists of 10 self-rated questions (Thompson et al. 2000). A higher number of positive items correspond to a higher level of nonadherence.
Adherence to medication was also reported by the attending physician and one parent using an adherence rating scale, which assessed the assumed percentage of medication accurately taken by the patient in the last 2 weeks.
The patient and the parent version of the Questionnaire on Attitudes Toward Treatment (QATT) by Ferrin et al. (2012) was applied. The QATT aims to identify the specific attitudes that contribute to treatment adherence (Ferrin et al. 2012). It was translated from English into German; the German version is currently being validated as part of the SEMA study.
This study focuses on results of the interview, MARS, and part of the patient version of QATT. All instruments were employed in the German language. All participants underwent one study session, during which they were first interviewed (30–60 minutes) by one of the investigators. Subsequently, they filled out their version of the QATT and MARS individually.
Definitions
Patients' adherence status was defined by considering a combination of the MARS and QATT patient version results. Patients who fulfilled at least one of the following criteria were classified as not completely adherent: Positive findings in the MARS (two or more positive items out of four) Having ended a treatment of their own volition (as reported in the QATT) Not having taken all of their prescribed medication in the week before the investigation (as reported in the QATT)
Patients who did not fulfill any of these criteria were defined as completely adherent.
Content analysis
As a first step, a conventional content analysis was conducted. This method was used because it aims to describe a phenomenon on which existing research literature is limited, as is the case in this study (Hsieh and Shannon 2005). The researcher avoids using predetermined categories and instead develops them directly from the text data (Kondracki et al. 2002), which has also been described as inductive category development (Mayring 2014). Text data of responses to each question of the interview were initially read repeatedly to gain an overview of the thematic areas of the answers (Tesch 1990). Next, words and short phrasings capturing essential thoughts were highlighted, and labels were established for categories reflecting several of these “key thoughts” (Morgan 1993; Miles and Huberman 1994). The text data were reviewed and matched to these categories; during this process, they were readjusted, for example, a new category was developed if text data did not fit into the existing categories, and categories were combined if they resembled the same concept or key thought (Morse and Field 1995). After the final coding scheme had been established, an independent second rater also matched the text data, and the interrater agreement was measured using Cohen's kappa coefficient. A kappa >0.6 to 0.8 was interpreted as “substantial” agreement and >0.8 as “almost perfect” agreement (Landis and Koch 1977). Categories of questions with low interrater agreement were discussed by the raters, whereupon the category system was revised if necessary and the text data were independently matched again.
Statistical methods
Student's t-tests and chi-square tests were conducted to compare completely adherent and not completely adherent patients according to baseline demographic characteristics. Furthermore, Fisher's exact tests were used to analyze the group differences between completely adherent and not completely adherent patients, concerning the distribution pattern of answers to the interview. Statistical significance was set at the 5% level. Statistical analyses were conducted using SPSS (IBM SPSS Statistics 24).
Results
Study population
In total, n = 64 patients were included in the study. Twenty-nine (45.3%) were male and n = 35 (54.7%) were female. Forty-five (70.3%) of the adolescents were inpatients, while n = 19 (29.7%) were outpatients. The mean age was 15.1 years (range 12.01–17.11 years). The five most common main diagnoses (according to ICD-10) were affective disorder (n = 29), hyperkinetic disorder (n = 9), obsessive compulsive or anxiety disorder (n = 9), paranoid schizophrenia (n = 4), and anorexia nervosa (n = 4). The mean period of treatment with psychotropic medication was 4.12 months (range 0.5–36.0 months). Ten (15.6%) patients had been taking their medication for 2–4 weeks, n = 40 (62.5%) for 1–3 months, and n = 14 (21.9%) for more than 3 months.
There were no statistically significant differences between completely adherent and not completely adherent patients concerning age, gender, and the type of treatment (inpatient or outpatient status).
Adherence
All 64 participants filled out the MARS and QATT scales. Thirty-eight (59.4%) participants were classified as completely adherent and n = 26 (40.6%) as not completely adherent. In the group of not completely adherent patients, n = 12 showed two or three positive items on the MARS. N = 16 patients had not taken their medication as prescribed in the week before the investigation, and n = 9 had already ended a treatment of their own volition.
Conventional content analysis
Sixty-four out of 72 items were independently matched to developed categories, while 8 items could not be matched to categories due to a high heterogeneity of the given answers. Nine of the items were rematched due to low interrater agreement. Forty-three items had an interrater reliability measured with Cohen's kappa of >0.8 (almost perfect), 17 items with a kappa of >0.6 to 0.8 (substantial), and 4 items with a kappa >0.4 to 0.6 (moderate). One of the items was matched to two categories, 13 were matched to three categories, 27 were matched to four categories, 19 were matched to five categories, and 4 were matched to six categories. Figure 1 provides an example of Conventional Content Analysis of item 4a.
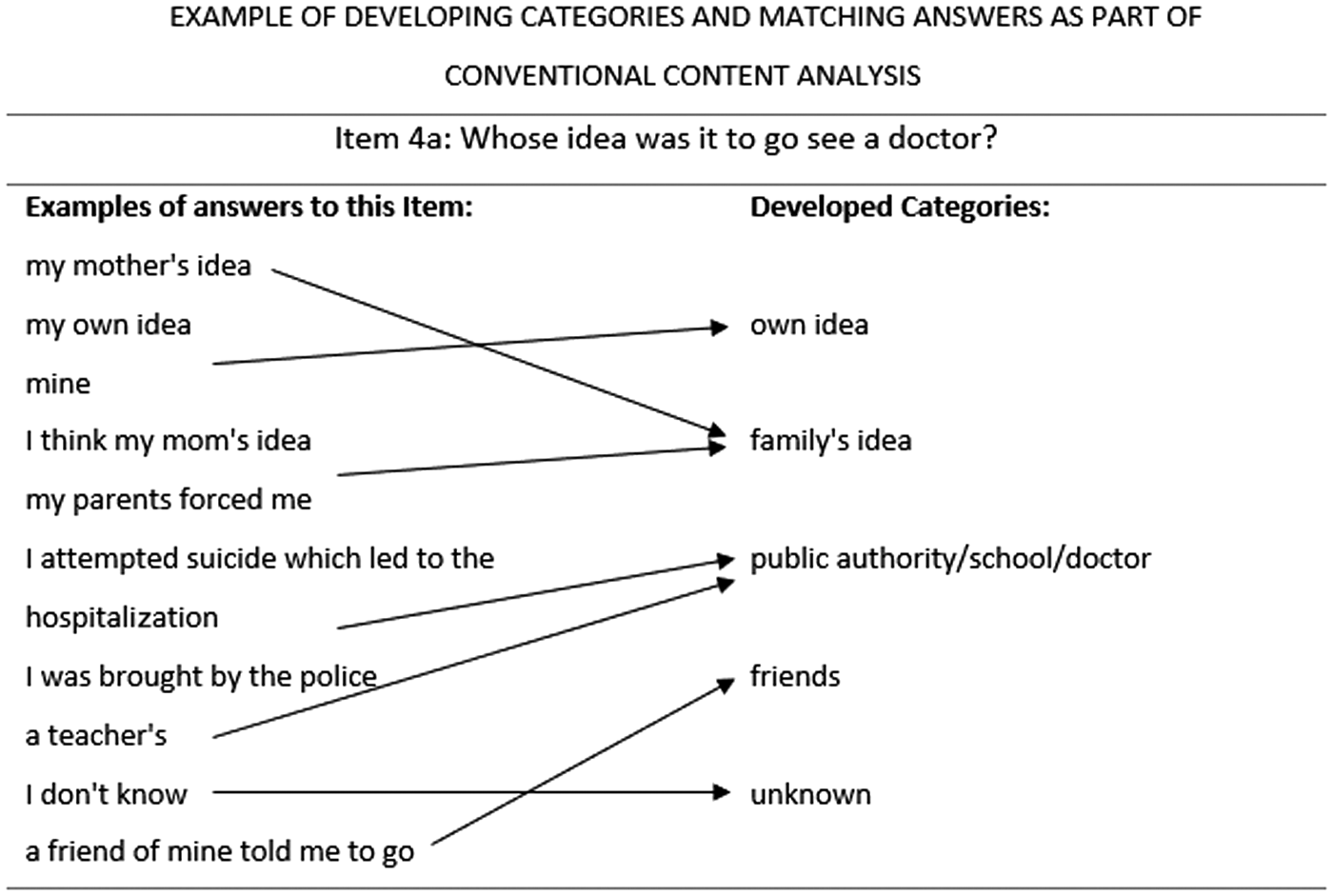
Conventional content analysis. Left: scanning answers for key thoughts/categories, right: developing category names, arrows: matching answers to categories.
Factors associated with not completely adherent behavior
Distribution patterns of answers to seven items showed statistically significant group differences between completely adherent and not completely adherent patients. Not completely adherent patients more likely reported a deterioration due to medication, a negative change of attitude toward medication due to experienced side effects, a lack of the ability to improve symptoms on one's own, a constricted physician–patient communication, a relationship of partial or no trust between patient and physician, limited family's knowledge about their disorder, and uncertainty about family members' wish for them to get better. See Tables 1 and 2 for more detailed information on these items.
No.: number of item in the interview; Fisher's exact test: level of significance set at 5%; Cohen's kappa: measurement of interrater agreement in conventional content analysis; kappa >0.8: substantial agreement, kappa >0.6 to 0.8: moderate agreement, kappa >0.4 to 0.6: low agreement.
SEMA 123: Patient ID.
“Do you feel the same or worse compared to not taking the medication?”
“How did your opinion on medication change due to the side effects?”
“Do you believe there is something you can do yourself to improve the problems you are facing?”
“Do you tell your physician about your difficulties in everyday life, school and family?”
“Do you sufficiently trust your physician to openly tell him/her about your problems?”
“Do your parents, siblings, grandparents, and other relatives know about your disorder?”
“Do your parents, grandparents, and siblings want you to get better?”
SEMA, Subjective Experience and Medication Adherence in Adolescents with Psychiatric Disorders.
In contrast, distribution patterns of answers to 57 items showed no statistically significant group differences between completely adherent and not completely adherent patients. The topics of these items were knowledge about the disorder, concept of the cause of disease, independent wish to visit a doctor, wish for improvement of disease, knowledge about psychotherapy and/or medication, individual appraisal of positive effects from psychotherapy and/or medication, number of experienced side effects of medication, psychoeducation about medication and the therapy process, frequency of physician–patient contact, other adolescents' knowledge about the patient's disorder, negative feedback from others about psychotropic medication, and being teased because of the disorder.
Discussion
To our knowledge, this is the first interview-based study to investigate subjective experiences and health beliefs of adolescents with psychiatric disorders and to correlate these findings with medication adherence. We were able to gain a comprehensive understanding of adolescents' thoughts on their course of disease, including issues experienced due to their disorder, thoughts on risks and benefits of their treatment, and perceptions on the matter of side effects. We also increased the insight into the subjective physician–patient relationship and disease-related struggles with family, friends, and the environment.
In this study with adolescent psychiatric patients, compared to completely adherent patients, the group of not completely adherent patients could be characterized as more likely to report feeling worse after taking medication, to describe a lower sense of self-efficacy concerning the improvement of their symptoms, and/or to perceive a less trustful physician–patient relationship. Furthermore, this group was more likely to state that their attitude toward medication worsened after experiencing “side effects,” that they subjectively felt less support from their relatives, and/or they had fewer individuals in their family who were fully informed about their condition.
We discovered 40.6% of not completely adherent patients, which is in line with reported nonadherence rates for adolescents with psychotropic medication in previous studies (which applied different assessment approaches and definitions of [non]adherence), ranging from 6% to 62% with a median of 33% (Häge et al. 2018).
As little to no research exists on several of the factors found to be associated with not completely adherent behavior in our study, the comparability of our findings with existing literature is limited.
In accordance with previous findings, our study supports the hypothesis that adolescents' beliefs about their medication are more important for their real-life adherence than are objective benefits and risks of their medication (Ferrin et al. 2012; Charach et al. 2014).
We assumed a strong negative association between adherence and worsening of condition after taking medication, but no strong positive association between adherence and clinical improvement. This issue has been investigated by several studies, but the evidence is inconsistent.
In a systematic literature review, Gajria et al. (2014) reported that one of the most frequent reasons why children and adolescents display medication nonadherence was a suboptimal response to the medication. Pogge et al. (2005) found no association between the rating of medication as “being helpful” and the level of adherence, whereas others reported opposite findings (Patel et al. 2005).
In contrast to Stewart and Baiden (2013) and Emilsson et al. (2017), in our study population, we did not observe that the experience of adverse events (side effects) in response to any medication ever taken by a participant was a potential predictor of not completely adherent behavior. Nevertheless a worsened opinion about medication due to experienced adverse events (side effects) was statistically significantly associated with incomplete medication adherence (Stewart and Baiden 2013). This illustrates that the subjective evaluation of and attitude toward medication is of greater importance for a patient's adherence than the objective experience of adverse events.
Furthermore, our data suggest that—besides efficacy and tolerability—family-related factors are of particular relevance for adherent behavior. We observed that factors such as a lack of support from the patient's family and less knowledge of the family about the patient's disorder were related to not completely adherent behavior. Other family-related factors associated with medication nonadherence, like parental perceptions of medication as not being helpful, or having a dysfunctional relationship with family members, were reported by Burns et al. (2008) and Stewart and Baiden (2013).
The findings of our study need to be interpreted in the context of several limitations. As most of our adolescent participants were treated as inpatients, this may have increased the reported rate of medication adherence, since there is a greater monitoring of drug ingestion in this hospital setting. Furthermore, only patients who agreed to participate were included in the study; thus, we interviewed a pre(self-)selected group of most likely more motivated adolescents, which may also have biased the results. Indeed, clinical experience suggests that adherence in voluntarily participating patients is higher than in routine clinical practice. As was the case in previous studies, we chose a self-report measure of medication nonadherence instead of an objective measurement. As the influence/impact of social desirability is assumed to be high, especially for the issue of medication adherence, we have to consider that participants may have withheld important information. Moreover, we only analyzed patients' (self-reported) adherence at one point of time, whereas their behavior concerning adherence might change over the course of treatment. We did not conduct an analysis of subgroups, for example, with respect to specific disorders or certain types of medication, since the amount of available data appeared to be insufficient.
Despite these limitations, a specific strength of our study was the qualitative interview with open questions, due to which a variety of thematic areas was surveyed. Subjective results are more likely to accurately reflect a complex area such as medication (non)adherence and its associated factors, compared to questions with predetermined answers. By using a qualitative approach and conventional content analysis, we avoided imposing preconceived theoretical perspectives and allowed for new insights to emerge directly from the text data instead (Kondracki et al. 2002). Knowledge generated from the analysis was developed from the collected interview data and is primarily based on the participants' subjective perceptions. Our results are not only valid for one psychiatric disorder but also can be seen as cross-disorder factors associated with medication adherence behavior. With n = 64 participants, we were able to analyze a relatively large data set compared to other qualitative trials with text data analyses.
Conclusions
This study adds valuable aspects to the existing knowledge regarding reasons for incomplete medication adherence in adolescents with psychiatric diagnoses. The importance of a trustful physician–patient relationship for an improved adherence was emphasized, whereas the experience of adverse events/side effects played a subordinate role. These findings imply, for example, that intensive relationship-building between patient and treating/prescribing physician can also contribute to reducing the high amount of adequately prescribed, but not accurately taken, psychotropic medication. Furthermore, we were able to identify a number of parameters characterizing the group of patients with reduced adherence to medication (feeling worse after taking medication; lower sense of self-efficacy concerning the improvement of symptoms; a less trustful physician–patient relationship; attitude toward medication worsened after experiencing adverse events/“side effects”; less support from relatives; and fewer individuals in the family who were fully informed about a patient's condition).
Nevertheless, additional research into the factors considered in this study, possibly in larger study samples, is required. Once greater knowledge has been gained about reasons for nonadherence to psychotropic medication, the development of tools and approaches to increase medication adherence appears essential, for example, in terms of important elements of psychoeducation programs and personalized treatment concepts. It is hoped that this study will stimulate further investigation in this field.
Clinical Significance
This study adds valuable aspects to the knowledge regarding reasons for incomplete medication adherence in adolescents with psychiatric diagnoses. The results indicate that certain factors contribute to an increased or decreased medication adherence. These are beliefs about the effectiveness of medication, thoughts about adverse events/side effects, self-efficacy, trustful physician–patient relationship, and family support. Consequently, it may prove useful in clinical practice to address these factors when initiating and monitoring treatment with psychopharmacological medications.
Footnotes
Disclosures
K.M. has served as investigator in clinical trials conducted by Lundbeck, Shire, Sunovion, and Teva, plus in EU FP7 program and Horizon 2020-funded projects. R.W.D. has received compensation for serving as consultant or speaker, or he or the institution he works for has received research support or royalties from the organizations or companies indicated: EU (FP7 Programme), U.S. National Institute of Mental Health (NIMH), German Federal Ministry of Health/Regulatory Agency (BMG/BfArM), German Federal Ministry of Education and Research (BMBF), German Research Foundation (DFG), and Volkswagen Foundation; Boehringer Ingelheim, Ferring, Janssen-Cilag, Lilly, Lundbeck, Otsuka, Servier, Shire, Sunovion/Takeda, and Theravance. Dr. Dittmann own Eli Lilly stock. A.H. has served as investigator in clinical trials conducted by Janssen-Cilag, Otsuka, Shire, Servier, Lundbeck, Sunovion, and Teva plus in BMBF and EU FP7 program and Horizon 2020-funded projects. He has received conference travel support and compensation for serving as consultant or speaker by E. Lilly and Shire. All other authors report no potential conflicts of interest.
Acknowledgments
The authors would like to thank all patients and parents who participated in this study, as well as the participating clinicians in Mannheim, Wolfsburg, Braunschweig, and Königslutter. Special thanks to Joachim Niemeyer for helping with the recruitment process immensely by providing a second study center.