
Abstract
Objective:
Methylphenidate and atomoxetine are efficacious in reducing core symptoms of attention-deficit/hyperactivity disorder (ADHD), but little is known about their efficacy in improving emotional/behavioral problems among youths with ADHD.
Methods:
One hundred sixty drug-naïve youths with DSM-IV-defined ADHD, aged 7–16 years, were recruited and randomly assigned to osmotic-release oral system methylphenidate (OROS-methylphenidate; n = 80) and atomoxetine (n = 80) in a 24-week, open-label, head-to-head clinical trial. The primary efficacy measure was parent-reported Child Behavior Checklist (CBCL), and the secondary efficacy measures included Youth Self Report (YSR) and Strengths and Difficulties Questionnaire (SDQ), which was based on the ratings of parents, teachers, and subjects.
Results:
For CBCL, both methylphenidate and atomoxetine groups showed significant improvement in all scores at weeks 8 and 24 except Somatic Complaints in the atomoxetine group. For SDQ, both treatment groups showed significant improvements in the Hyperactive and Conduct subscales for parent ratings, and the Externalizing subscale for teacher ratings at week 24. Methylphenidate was associated with greater improvements in Aggressive Behavior and Somatic Complaints of CBCL and in Conduct subscale of self-reported SDQ at week 24 compared with atomoxetine.
Conclusions:
Our findings provide evidence to support that both methylphenidate and atomoxetine were effective in improving a wide range of emotional/behavioral problems in youths with ADHD after 24 weeks of treatment, with greater improvement in aggressive behavior, somatic complaints, and conduct problems in the methylphenidate group.
Introduction
A
Methylphenidate and atomoxetine are the only two medications approved for treating youth and adults with ADHD in many countries, and Taiwan as well (Ni et al. 2013). Methylphenidate, a dopamine and noradrenaline reuptake inhibitor, promotes the release of stored dopamine from presynaptic vesicles (Volkow et al. 2005) and is recognized as the first-line treatment for ADHD for decades worldwide. Atomoxetine is a highly specific inhibitor of presynaptic norepinephrine transporter, with little affinity for other neurotransmitter transporters or receptors (Garnock-Jones and Keating 2009). Clinical trials have shown that both methylphenidate and atomoxetine treatments are associated with clinically meaningful and comparable effectiveness in improving the core symptoms of ADHD across situations (Kratochvil et al. 2002; Shang et al. 2015). In contrast, results for the effectiveness of methylphenidate and atomoxetine in improving emotional/behavioral problems in patients with ADHD are mixed. For example, although several studies observed no significant effects on emotional control after treatment with methylphenidate (Biederman et al. 2011), others documented the effectiveness of methylphenidate in improving emotional dysregulation (Kutlu et al. 2017). Some trials showed a significant reduction in anxiety and depression after treatment with methylphenidate in patients with ADHD (Bouffard et al. 2003); others found no change (Kuperman et al. 2001), and still others demonstrated an increase in anxiety and depressive symptoms (Spencer et al. 2005). A clinical trial demonstrated that atomoxetine is not superior to placebo in reducing oppositional problems (Bangs et al. 2008), whereas other studies showed positive findings for the efficacy of atomoxetine in improving oppositional behaviors (Dittmann et al. 2011). Given the remarkable variability in methods across pharmacological studies on ADHD (Faraone et al. 2006), further clinical trials are required to examine the efficacy of methylphenidate and atomoxetine in the treatment of emotional/behavioral problems in youths with ADHD.
Numerous rating scales are available for measuring the emotional/behavioral symptoms associated with ADHD in different settings. Compared with narrowband scales, broadband scales such as Children Behavior Checklist (CBCL) and Strength and Difficulties Questionnaire (SDQ) are better for a comprehensive assessment of the emotional/behavioral symptoms associated with ADHD. However, only a few studies have used the CBCL (Wang et al. 2013) and SDQ (Gelade et al. 2016) as outcome measures for treatment studies. For example, a previous report showed no improvement in emotional/behavioral symptoms measured by CBCL after treatment with methylphenidate in youths with ADHD (Wang et al. 2013). A clinical trial demonstrated that methylphenidate is associated with significant improvement in the total score of teacher-rated SDQ, but no improvement on parent-rated SDQ (Gelade et al. 2016).
Given that the emotional/behavioral symptoms influence the psychosocial functions and disease course of ADHD, a direct comparative trial is required to identify the therapeutic effect of methylphenidate and atomoxetine on the emotional/behavioral problems in youths with ADHD. The present study aimed to directly compare the effectiveness of methylphenidate and atomoxetine in improving a wide range of emotional/behavioral problems in drug-naïve youths with ADHD in a head-to-head, open-label, 24-week randomized clinical trial.
Methods
Participants
We recruited drug-naïve youths, aged between 7 and 16 years, who met the DSM-IV diagnostic criteria for ADHD, as assessed by the investigator's clinical evaluation and confirmed using the Chinese version of the Schedule for Affective Disorders and Schizophrenia for School-Age Children–Epidemiological Version (K-SADSE) (Gau et al. 2005). We excluded participants who had comorbid conditions with bipolar disorders, psychosis, any substance abuse, autism spectrum disorders, intellectual disability (Full-Scale Intelligence Quotient score <80), or had serious medical conditions such as cardiovascular disease, history of seizure, or prior electroencephalogram abnormalities related to epilepsy, or had ever used any psychotropic medications before the study. The details have been reported elsewhere (Shang et al. 2015).
Study design and procedures
This study had been approved by the Research Ethics Committee of the National Taiwan University Hospital, Taiwan (IRB ID, 200812153M;
During the 24-week, open-label, head-to-head randomized clinical trial, participants were assigned to either the osmotic-release oral system (OROS)-methylphenidate or atomoxetine group at a 1:1 ratio according to computer-generated random sequence. Participants were assessed seven times at baseline (visit 1), week 2 (visit 2), week 4 (visit 3), week 8 (visit 4), week 12 (visit 5), week 16 (visit 6), and week 24 (visit 7). At visit 1, participants started taking medication with OROS-methylphenidate (an initial dosage of 18 mg per day, administered as a single morning dose) or atomoxetine (an initial dosage of 0.5 mg/kg per day, administered as once-daily dose). Drug dosage would be titrated based on treatment response and adverse effects at visits 2–7 (weeks 2–24) depending upon clinical response and adverse effects. The maximal dose was 54 mg daily for OROS-methylphenidate or 1.2 mg/kg daily for atomoxetine.
Parent-reported CBCL and Youth Self Report (YSR) were gathered at baseline (visit 1), week 8 (visit 4), week 16 (visit 6), and week 24 (visit 7). Parent-, teacher-, and self-reported SDQ were gathered at each visit, from visit 1 through visit 7.
Efficacy measure
Our primary efficacy measure was parent-reported CBCL, and the secondary outcomes were YSR and SDQ.
CBCL and YSR
The CBCL is a parental questionnaire used to measure the emotional/behavioral problems in youths aged 4–18, and the YSR is administered to adolescents aged 11–18 to obtain self-reports about their emotional/behavioral problems (Achenbach and Dumenci 2001). Each item is scored 0 if not true, 1 if somewhat or sometimes true, and 2 if very true or often true. Eight emotional/behavioral scales were created for both the CBCL and YSR, including Anxious/Depressed symptoms, Attention Problems, Aggressive Behaviors, Delinquent Behaviors, Social Problems, Thought Problems, Somatic Complaints, and Withdrawn.
The Chinese versions of CBCL and YSR have been shown to have good validity and reliability (Yang et al. 2001; Shang et al. 2006), and these two scales have been widely used to measure emotional/behavioral problems in Taiwanese youth populations (Chen et al. 2017).
Strengths and Difficulties Questionnaire
The SDQ, a 25-item screening questionnaire, has been designed to assess a broad area of emotions and behaviors of youths (Goodman 1999). Each item is rated on a three-point Likert scale (0 = not true, 1 = somewhat true, and 2 = certainly true). There are three versions of the SDQ for ratings by self, parents, and teachers. Our previous work on the Chinese version of SDQ identified four subscales in the parent version (prosocial, conduct, internalizing, and hyperactive), four subscales in the teacher version (peer/prosocial, externalizing, internalizing, and inattention), and five subscales in the self-report (prosocial, conduct, hyperactive, peer problems, and emotion) (Liu et al. 2013).
Statistical analyses
Baseline demographic characteristics and assessment of emotional/behavioral problems were presented in mean scores and SD for continuous variables, and number and corresponding percentage for categorical variables. The t-scores of CBCL, YSR, and SDQ were used to present the severity of emotional/behavioral problems. The t-score was defined as multiplying the z-scores by 10 and adding 50, with a mean of 50 and a SD of 10. We used the intent-to-treat principle for missing data in the statistical analysis, and the last-observation-carried-forward method was applied to missing data or patient dropout. Hierarchical linear mixed-effects models were employed to address the lack of statistical independence of repeated measurements of the same participants over time. Cohen's d was used to compute the effect size for the comparisons of scores of CBCL, YSR, and SDQ between week 8 and baseline and between week 24 (last observation) and baseline, with the small, medium, and large effect sizes being d = 0.2 to <0.5, >0.5 to <0.8, and >0.8, respectively. In particular, both intercepts and slope (time) effects in the linear mixed model with time-dependent variables were treated as random effects, to account for variations among subjects in baseline values, and slopes for individual trajectories of changes in emotional/behavioral problems over visits, in addition to the main treatment and fixed time effects of the two treatment groups. To test the difference in the slope of change between the two treatment groups, the interaction terms between visits × drugs were tested. The alpha value was preselected at the level of p < 0.05.
Results
Sample description and medication
Of the 174 patients screened, 160 were enrolled and randomly assigned to atomoxetine (n = 80) or methylphenidate (n = 80) groups. Among them, 80 patients with atomoxetine and 76 patients with methylphenidate had complete data on CBCL. Given that YSR was only applied to patients aged 11 years or more, 54 patients treated with atomoxetine and 51 patients treated with methylphenidate had complete data on YSR (Fig. 1). There were no statistically significant group differences in demographic characteristics and baseline severity of emotional/behavioral problems except that the methylphenidate group had higher Peer/Prosocial scores of teacher-reported SDQ compared with the atomoxetine group (Table 1).
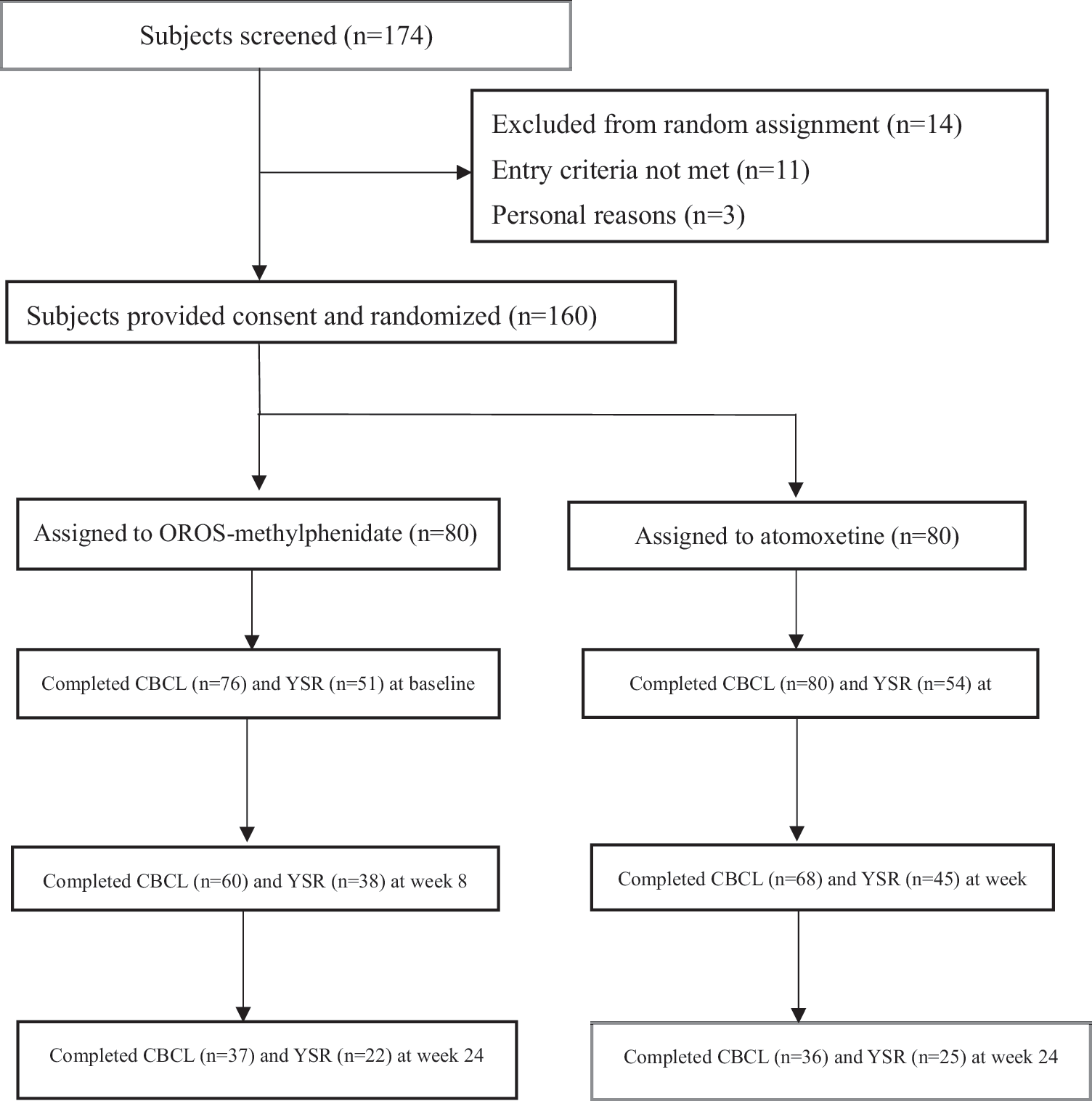
Flowchart of the randomization procedure. CBCL, Child Behavior Checklist; YSR, Youth Self Report.
Demographics and Baseline Emotional/Behavioral (t-Score) Between the Two Treatment Groups
CBCL, Child Behavior Checklist; YSR, Youth Self Report; SDQ, Strengths and Difficulties Questionnaire.
p < 0.05.
For the OROS-methylphenidate group, the mean administered dose was 20.45 (SD = 6.76) mg/day or 0.64 (SD = 0.19) mg/kg per day at week 2 (visit 2), 24.91 (SD = 9.65) mg/day or 0.75 (SD = 0.24) mg/kg per day at week 4 (visit 3), 26.38 (SD = 11.32) mg/day or 0.79 (SD = 0.28) mg/kg per day at week 8 (visit 4), 27.98 (SD = 11.77) mg/day or 0.84 (SD = 0.3) mg/kg per day at week 12 (visit 5), 27.02 (SD = 11.83) mg/day or 0.81 (SD = 0.32) mg/kg per day at week 16 (visit 6), and 27.83 (SD = 12.44) mg/day or 0.82 (SD = 0.34) mg/kg per day at week 24 (visit 7). For the atomoxetine group, the mean administered dose was 26.09 (SD = 9.07) mg/day or 0.78 (SD = 0.28) mg/kg per day at week 2 (visit 2), 27.94 (SD = 9.74) mg/day or 0.84 (SD = 0.33) mg/kg per day at week 4 (visit 3), 29.37 (SD = 8.23) mg/day or 0.89 (SD = 0.31) mg/kg per day at week 8 (visit 4), 31.39 (SD = 9.12) mg/day or 0.93 (SD = 0.31) mg/kg per day at week 12 (visit 5), 31.68 (SD = 8.76) mg/day or 0.95 (SD = 0.31) mg/kg per day at week 16 (visit 6), and 31.74 (SD = 10.34) mg/day or 0.98 (SD = 0.28) mg/kg per day at week 24 (visit 7). Regarding adverse events, vomiting (p = 0.017), somnolence (p < 0.001), and dizziness (p = 0.009) were reported more often for atomoxetine, while insomnia (p = 0.035) was reported more often for OROS-methylphenidate. The details have been reported elsewhere (Shang et al. 2015).
Efficacy on CBCL
Both treatment groups showed significant improvements in all the eight scales of CBCL from baseline to week 8 and from baseline to week 24 except Somatic Complaints in the atomoxetine group (Table 2). Compared with the atomoxetine group (Table 2), the methylphenidate group had greater improvements in Aggressive Behavior (p = 0.003) and Delinquent Behavior (p = 0.009) from baseline to week 8, and in Aggressive Behavior (p = 0.032) and Somatic Complaints (p = 0.008) from baseline to week 24. In addition, the methylphenidate group had lower scores in Attention Problems (Fig. 2B) at week 8 (Cohen's d = 0.35) and week 16 (Cohen's d = 0.55), and Social Problems (Fig. 2D) at week 16 (Cohen's d = 0.57) compared with the atomoxetine group. There were significant effects of the drug × visit interactions on the Aggressive Behavior (p = 0.013), Delinquent Behavior (p = 0.041), and Somatic Complaints (p = 0.003) (Fig. 2A, C, E). There were no effects noted for the interactions of drug × visit on the Anxious/Depressed, Attention Problems, Social Problems, Thought Problems, and Withdrawn.
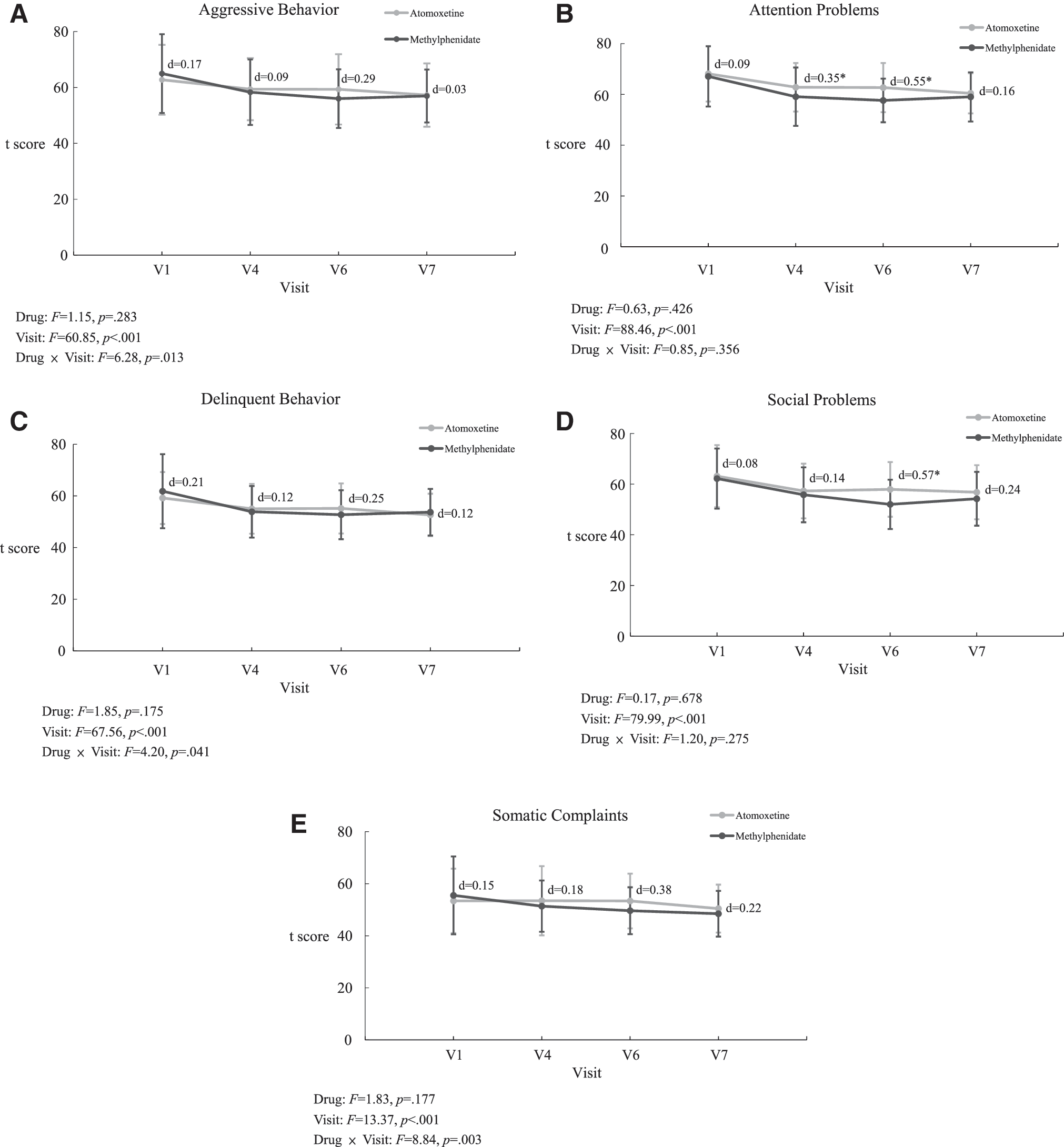
Improvements in the emotional/behavioral scores of CBCL in youths with ADHD randomly assigned to treatment with either methylphenidate or atomoxetine.
Change in Child Behavior Checklist and Youth Self Report from Baseline to Weeks 8 and 24 (Endpoint) in the Two Treatment Groups
p < 0.05.
p < 0.01.
p < 0.001.
Efficacy on YSR
Both treatment groups showed significant improvements in the YSR scores from baseline to week 8 and from baseline to week 24 except Anxious/Depressed (weeks 8 and 24) and Thought Problems (week 8) in the atomoxetine group, and Delinquent Behavior (week 8), Somatic Complaints (weeks 8 and 24), and Thought Problems (week 8) in the methylphenidate group (Table 2). The analysis of mean changes in the YSR scores (Table 2) revealed no significant differences between the two treatment groups from baseline to week 8 and from baseline to week 24.
Efficacy on SDQ
From baseline to week 24, both treatment groups showed significant improvements in the Hyperactive and Conduct subscales for parent ratings and the Externalizing subscale for teacher ratings (Table 3). For the self-report, the Emotion and Conduct problems improved with methylphenidate treatment at week 24, and the Hyperactive problems improved with atomoxetine treatment at week 24. Compared with the atomoxetine group, the methylphenidate group had greater improvements in the self-reported Conduct subscale (p = 0.041) at week 24.
Change in Strengths and Difficulties Questionnaire from Baseline to Weeks 8 and 24 (Endpoint) in the Two Treatment Groups
p < 0.05.
p < 0.01.
p < 0.001.
Discussion
To our best knowledge, this is the first head-to-head, randomized, long-term treatment study to prospectively compare the effects of methylphenidate and atomoxetine on a wide range of emotional/behavioral problems in drug-naïve youths with ADHD. We found that both treatments are efficacious in reducing the severity of emotional/behavioral problems measured by CBCL, YSR, and SDQ. Compared with atomoxetine, methylphenidate is associated with greater improvements in Aggressive Behavior and Somatic Complaints of CBCL and in the Conduct subscale of self-reported SDQ from baseline to week 24. In contrast to an observational study showing no effect of short-acting methylphenidate on the behavioral problems measured by CBCL in youths with ADHD (Wang et al. 2013), our randomized clinical trial using OROS-methylphenidate once daily provided strong evidence to support that emotional/behavioral problems are reduced by treatment not only with methylphenidate but also with atomoxetine.
Our results showed the large effect of treatment with methylphenidate in the realm of attention problems (Cohen's d = 0.7 at week 8 and 0.8 at week 24), consistent with an average effect size of 0.8 in prior reports (Conners 2002). Previous studies have demonstrated the effects of methylphenidate (Conners 2002; Sinzig et al. 2007) and atomoxetine (Schwartz and Correll 2014) on externalizing symptoms associated with ADHD, including aggressive, oppositional, and conduct problems. Meta-analytic reviews in assessing the impact of methylphenidate (Connor et al. 2002) reported a weighted mean effect size of 0.84 for overt and 0.69 for covert aggression-related behaviors in ADHD, consistent with our findings in the Aggressive Behavior subscale of CBCL for methylphenidate (Cohen's d = 0.6 at week 8 and 0.68 at week 24). In contrast, although atomoxetine is effective in reducing the core symptoms of ADHD, a relatively small effect size of 0.33 was found for disruptive problems (Schwartz and Correll 2014), consistent with our findings in the Aggressive Behavior subscale of CBCL for atomoxetine (Cohen's d = 0.24 at week 8 and 0.37 at week 24). A systemic review reported a moderate-to-large effect for methylphenidate and a small effect for atomoxetine on oppositional behavior, conduct problems, and aggression in youths with ADHD (Pringsheim et al. 2015). Animal studies have shown that aggressive behaviors in mice are associated with the altered function of dopamine transporter (Yu et al. 2014). Taken together, converging evidence supports that methylphenidate demonstrates a greater magnitude of treatment effect for aggressive spectrum symptoms in youths with ADHD compared with atomoxetine. Future studies are needed to explore the factors associated with the differential effects of methylphenidate and atomoxetine on aggression.
Similarly, our findings demonstrated the effectiveness of both methylphenidate and atomoxetine in improving the externalizing problems assessed by a parent- and teacher-rated SDQ at week 24, including Hyperactive, Conduct, and Externalizing subscales. No significant improvement in parent- and self-rated Prosocial subscale was observed after 24-week treatment with methylphenidate or atomoxetine, whereas atomoxetine is associated with improvement in teacher-rated Peer/Prosocial subscale at weeks 8 and 24. Our previous work has shown the effectiveness of atomoxetine in children with ADHD in improving interactions with peers and teachers (Shang and Gau 2012). The literature documents the importance of teacher ratings on treatment response in youths with ADHD (Lavigne et al. 2012), and a lack of reports from teachers may result in the inadequate assessment of treatment effects (Miller 1999).
For internalizing symptoms, our findings showed a similar efficacy of methylphenidate and atomoxetine in reducing Anxious/Depressed symptoms measured by CBCL in youths with ADHD, with effect sizes ranging from 0.31 to 0.44. Previous studies demonstrated the efficacy of atomoxetine on anxiety symptoms associated with ADHD, with an effect size of 0.4 (Geller et al. 2007). In addition, clinical trials showed that symptoms of anxiety and depression in patients with ADHD improved after treatment with methylphenidate (Mattos et al. 2013).
The Somatic Complaints subscale of CBCL, one of the internalizing problems, is intended to assess the physical symptoms with no medical basis, and psychiatric disability may accentuate the incidence of somatic complaints in children with ADHD (Egger et al. 1999). Previous studies showed that parent-rated somatic complaints improved after treatment with methylphenidate (Rapport et al. 2002) in youths with ADHD, consistent with our findings. Youths with ADHD experience significant distress at home and in school, owing to inherent difficulties with this disorder, and may internalize this distress as physical complaint (Rapport et al. 2002). Further studies are needed to examine whether improved performance at home and in school associated with methylphenidate treatment corresponds with reductions in parent-rated somatic complaints in youths with ADHD.
In our present study, changes in YSR scores also showed significant improvements in emotional/behavioral problems from baseline to week 24 for both methylphenidate and atomoxetine, except the Anxious/Depressed subscale for atomoxetine and the Somatic Complaints subscale for methylphenidate, inconsistent with parent ratings of treatment response measured by CBCL. Although youths are valuable informants about their own emotional/behavioral problems (Klimkeit et al. 2006), previous studies analyzing ratings on CBCL and YSR showed better parent–youth agreement for externalizing problems than internalizing problems (Rescorla et al. 2017). For example, youths may report more anxious symptoms with higher degrees of intensity than their parents (Weitkamp et al. 2010). Parent–youth discrepancies may arise due to not only contextual variations in emotional/behavioral problems (De Los Reyes et al. 2013) but also parents' inability to observe youths' emotional/behavioral problems where they are not present (Achenbach 2011). Further research is needed to identify the specific factors associated with the inconsistent ratings of treatment response for Anxious/Depressed symptoms and Somatic Complaints between parents and youths with ADHD.
There are several methodological limitations in our study. First, due to a lack of a placebo group, we could not determine whether the improvements in emotional/behavioral problems may be partially attributed to the placebo or maturity effect. In addition, we were unable to contrast both baseline and placebo with active drug conditions to differentiate the drug-unrelated somatic complaints from those due to drug-related side effects. Second, methylphenidate is a controlled drug in Taiwan, which prevents us from conducting a double-blinded, placebo-controlled trial as an investigator-initiated clinical trial. The bias derived by an open trial design could be reduced since in Taiwan neither a teacher nor a school nurse distributed medication to students, and thus the teachers were blinded to which medication the subjects were taking. Third, given that the stimulant comparator in the present study was OROS-methylphenidate, our findings may not be generalized to other formulations of methylphenidate or Dextro-amphetamine. Fourth, we included the study sample from only one medical center in Taipei. Thus, the study results may not be generalized to broader ethnic Chinese populations with ADHD. Fifth, allowing investigators to adjust dose without using a systematic titration schedule could have led to underdosing in one group or the other; however, doses in the current study were consistent with those in the package information. Sixth, missing data in the long-term follow-up period may result in insufficient power to detect the differences in efficacy between the two drugs.
Conclusions
Our findings suggest that information about the emotional/behavioral profiles, collected from direct caregivers, school teachers, and self-reports, is valuable in monitoring the response to pharmacological treatment in youths with ADHD.
Clinical Significance
Our findings demonstrate that both methylphenidate and atomoxetine produce significant reductions in emotional/behavioral problems measured by CBCL, YSR, and SDQ, suggesting that obtaining assessments from multiple informants is crucial in establishing a comprehensive understanding of the pharmacological effects in youths with ADHD.
Footnotes
Author Contributions
C.Y.S. and S.S.G. contributed to concept and design of the study. H.H.S., C.Y.S., and S.S.G. contributed to data acquisition/analysis/interpretation. H.H.S. and C.Y.S. contributed to drafting the article, tables, and figures, which were critically reviewed by S.S.G. All authors read and approved the final version of the article.
Acknowledgment
The authors express thanks to Ming-Fang Chen, M.S., for assistance in data analysis.
Disclosures
C.Y.S. has conducted clinical trials on behalf of and was on the speakers' bureau for Janssen-Cilag and Eli Lilly & Co., Taiwan. S.S.G. has conducted clinical trials on behalf of and was on the speakers' bureau for Janssen-Cilag, Eli Lilly & Co., and Astellas Pharma, Inc., Taiwan.