
Abstract
Objective:
Impulsive aggression (IA) is a maladaptive form of aggressive behavior that is an associated feature of neuropsychiatric disorders, including attention-deficit/hyperactivity disorder (ADHD). As one of the most common forms of aggressive behavior, IA is a serious clinical concern. Recognition, monitoring, and management of IA symptoms are complicated by the lack of IA-specific psychometric instruments and evidence-based treatments. A recently developed electronic observer-reported outcome instrument has been validated in children for monitoring the frequency of 15 IA-related behaviors in the context of ADHD. This study seeks to first determine if the behaviors included in the pediatric IA diary are applicable to adolescents with ADHD, and second, compare the reliability of adolescent versus parent reporters.
Methods:
We evaluated the utility of the pediatric IA diary through concept elicitation and cognitive interviews with 17 pairs of parents and adolescents (aged 13–17 years) with IA and ADHD, supplemented with 15 new behaviors potentially applicable to adolescents.
Results:
The behaviors most frequently reported by adolescents included arguing (93.8%), raising their voice/shouting/yelling (93.8%), hitting others (87.5%), slamming (87.5%), pushing/shoving (81.3%), breaking (75.0%), fighting (75.0%), throwing (75.0%), and cursing (68.8%). The behaviors most commonly reported by parents included raising their voice/shouting/yelling (94.1%), arguing (88.2%), being disrespectful/mean/rude (88.2%), slamming (88.2%), throwing (88.2%), cursing (82.4%), hitting others (82.4%), pushing/shoving (82.4%), breaking (76.5%), name-calling (76.5%), and threatening (70.6%). Of all commonly reported behaviors, only being “disrespectful/mean/rude” and “breaking” are not part of the pediatric IA diary, likely due to the imprecision of these terms. No significant usability issues were found for the IA diary device.
Conclusions:
These findings suggest that the 15-item pediatric IA diary should be applicable to adolescent populations to appropriately characterize IA behaviors in individuals with ADHD. Furthermore, this study indicated that parents may be more reliable reporters of IA behavior than adolescents.
Introduction
Impulsive aggression (IA) is a maladaptive form of aggression characterized by a variety of physical and verbal behaviors that are reactive, overt, and occur outside the acceptable social response (Jensen et al. 2007; Knapp et al. 2012; Gurnani et al. 2016; Miles et al. 2016). IA behaviors are eruptive and can arise out of frustration or annoyance or be retaliatory to provocation (whether it is real or perceived) (Saylor and Amann 2016). While adaptive aggression is a natural response to a threat—developed to protect the aggressor—IA behavior is associated with negative consequences for the aggressor, and as such, the aggressive act is accompanied by negative emotions (Barratt et al. 1999; Jensen et al. 2007; Saylor and Amann 2016). IA symptoms are a frequent cause for psychiatric referral of children and adolescents and can present with multiple neuropsychiatric disorders, including attention-deficit/hyperactivity disorder (ADHD) (Connor 2016; Saylor and Amann 2016). IA behavior in adolescents causes difficulties in peer relationships, exacerbates parental stress, and leads to detrimental developmental trajectories for the individual (Jensen et al. 2007; Connolly and Vance 2010; Saylor and Amann 2016; Wiener et al. 2016). Managing these symptoms poses a substantial challenge for clinicians, as it remains unclear how to effectively distinguish between subtypes of maladaptive aggression, given the current lack of treatments with supportive data (Connor 2016).
Guidelines for the management of IA symptomatology persistent after primary ADHD treatment currently recommend psychosocial interventions (such as social and problem-solving training, anger management, and behavioral therapy), with or without pharmacotherapy (Pappadopulos et al. 2003; Schur et al. 2003; Knapp et al. 2012). In cases where behavioral interventions do not provide sufficient response, monotherapy or combination therapies with stimulants, mood stabilizers, atypical antipsychotics, and/or alpha agonists are prescribed and have shown some efficacy in treating IA symptoms (Connor 2002; Jensen et al. 2007). However, only moderate success has been achieved in children and adolescents with persistent IA when using combination pharmacotherapy with atypical antipsychotics following primary ADHD treatment (MTA Cooperative Group 1999; Aman et al. 2004; Jensen et al. 2007).
The challenge of treating IA behavior is further compounded by the lack of an IA-specific assessment and monitoring instrument. Psychometric evaluations such as the Retrospective-Modified Overt Aggression Scale (R-MOAS) (Blader et al. 2009, 2010) and the Aggression Questionnaire (Vitiello et al. 1990) can be used to evaluate the severity of aggressive behavior and categorize aggression by subtype (planned vs. affective/impulsive), respectively, but neither of these scales is specifically designed to assess, monitor, and measure the frequency of IA behaviors. Recently, an electronic observer-reported outcome (eObsRO) instrument was developed and psychometrically validated for monitoring the frequency of 15 IA-related behaviors in children aged 6–12 years who have a primary diagnosis of ADHD and are receiving monotherapy with a U.S. Food and Drug Administration (FDA)-approved ADHD medication (Ceresoli-Borroni et al., submitted for publication).
This instrument monitors the nature and frequency of IA behaviors and is composed of an episodic diary, designed to be used by the parent, guardian, or observer immediately following an aggressive event, and an evening diary, to be used to confirm and record any remaining IA behaviors from a given day. In this way, the diary provides a contemporary snapshot of aggressive episodes within a given day, allowing the caregiver to reflect on the day and record either multiple events, or no events, within the diary. The 15-item pediatric diary includes the following behaviors: yelling, screaming, threatening, scratching, throwing, slamming, hitting self, arguing, cursing, name-calling, shoving/pushing, pulling hair, fighting, hitting others, and kicking others. These behaviors were narrowed from a broader provisional list of 30 behaviors following psychometric validation.
Although validated in children, it remains unknown whether the 15-item IA diary is applicable to evaluating IA-related behaviors in older age groups with ADHD. Understanding the application of the IA diary across both children and adolescents would be dependent on whether IA behaviors prevalent in childhood carry on or continue to change during adolescence and would thus provide novel information on IA behaviors in the context of ADHD at multiple life stages. Here, we assess whether the IA diary for children with ADHD is appropriate for use in adolescents (aged 13–17 years) through concept elicitation (CE) and cognitive interviews (CIs) with adolescents and their parents. This interview structure further facilitated the goal of determining the reliability of adolescent-reported versus parent-reported IA behaviors using the IA diary.
Methods
Participants
Adolescents paired with their parents were recruited from four study sites in the United States (Atlanta, GA; Baltimore, MD; Houston, TX; and Libertyville, IL). Eligibility for the study required that adolescent subjects be aged 13–17 years; have a diagnosis of ADHD as defined by the Diagnostic and Statistical Manual of Mental Disorders, 5th edition (DSM-5; American Psychiatric Association 2013) and confirmed by Kiddie Schedule for Affective Disorders and Schizophrenia for School-Age Children–2013 (Kaufman et al. 1997); and exhibit significant symptoms of IA based on the clinician's assessment of R-MOAS (Blader et al. 2009, 2010) and Aggression Questionnaire (Vitiello et al. 1990) scores of ≥20 and −2 to −5, respectively.
Criteria further limited study inclusion to those adolescent subjects receiving monotherapy treatment with the FDA-approved ADHD medication, as a prerequisite to the possible use of the IA diary in clinical trials in a population treated with ADHD medication. Additionally, inclusion criteria required parents of a subject to have spent significant time caring for the subject (≥20 hours per week); speak, read, and write in fluent English; and demonstrate willingness to participate in a 45- to 60-minute in-person interview. Exclusion criteria included a current or lifetime diagnosis of epilepsy, major depressive disorder, bipolar disorder, schizophrenia, personality disorder, Tourette disorder, or other unspecified psychotic disorders; or a current diagnosis of autism spectrum disorder, pervasive developmental disorder, obsessive–compulsive disorder, posttraumatic stress disorder, or any other anxiety disorder.
Recruitment targets were used to enroll adolescent subjects who were demographically representative of the prevalence of IA regarding gender (80% male and 20% female) and race (60% white, 30% black/African American, and 10% other). Before the study, written assent was obtained from each adolescent subject, and all parents or legally authorized representatives provided written informed consent to their own and their child's participation. All study procedures were approved by an independent review board and conducted in compliance with the Declaration of Helsinki.
Study interviews
Interviews were administered to adolescent and parent subjects separately to gather qualitative information about their experiences with IA and to evaluate their perceptions of the content validity, instrument interpretation, and usability of the pediatric IA diary. Whereas the content of the IA diary developed for children is narrowed to 15 behaviors commonly observed in that age group—including yelling, screaming, threatening, scratching, throwing, slamming, hitting self, arguing, cursing, name-calling, shoving/pushing, pulling hair, fighting, hitting others, and kicking others—the IA diary used in this study included an additional 15 behaviors infrequently reported in children: teasing, spitting, biting, grabbing a weapon, ripping, breaking, writing on walls/vandalizing, major damage/destruction, setting fire, hitting animals, kicking self, kicking animals, severely injuring self, severely injuring others, and severely injuring animals. These additional 15 behaviors had been included in a provisional pediatric IA diary and therefore warranted inclusion within this study, as the prevalence of all 30 behaviors in adolescents is unknown.
Adolescent and parent interviews were facilitated by the Semi-Structured Adolescent Interview Guide and Parent/Caregiver Interview Guide, respectively. Interviews began with an introduction of the interviewer, description of the aims of the study, and verbal consent from the subject. During the CE portion of the interview, interviewers asked nonleading open-ended questions about the subject's experience with IA, designed to encourage spontaneous responses and gather strong qualitative data. For example, such questions included, “What is a typical day for you in terms of your (or your child's) [subject's term for IA]?”; “Have you heard of the term ‘impulsive aggression’?”; “What happens when you get mad or angry?”; and “What are some of the aggressive behaviors?” Targeted questions were used only to clarify concepts of interest or clear confusion on a given diary item.
During the CI portion, adolescents and parents were asked to complete the IA diary electronically (using the LogPad App™ on a Nexus 5). Subjects were encouraged to verbalize their thoughts while completing the IA diary, with regular reminders from the interviewer (e.g., “What were you considering when you selected that answer?”). To gather feedback on the IA diary items as well as on the usability of the device, specific verbal probing with questions such as “How was your experience advancing to the next screen?” was also incorporated into the interviews. The interview guide was designed to support this hybrid format, allowing interviewers to obtain both spontaneous and structured feedback (henceforth referred to as “probed”) from subjects on the usability of the electronic patient-reported outcome (ePRO, as opposed to observer-reported outcome or ObsRO) format.
Finally, each subject was asked to respond to structured rating questions on a scale of 1–5 (with 1 being poor and 5 being excellent) regarding the usability of the LogPad App. All interviews were audio-recorded with the adolescent's and parent's consent and were scheduled to last up to 90 minutes.
Data analysis
All transcripts were coded and de-identified, and included summaries of demographic characteristics and health information. The coding process included well-established qualitative research methods, such as grounded theory and constant comparative methods (Glaser and Strauss 1967; Willis 2005). The coding scheme for the CE portion of the interviews catalogued concepts that were reported by adolescents or their parents “spontaneously” or needed to be “probed” by the interviewer, and any newly emerging concepts were recorded and updated and were shared between coders as they emerged.
Coding schemes for the CI portion of the interviews provided clear definitions of item interpretation types and usability issues so they could be consistently applied across coders. In addition, the intended meaning of closely related concepts was clearly defined a priori to guide coders and prevent the inclusion of repetitive concepts. Coders communicated new themes to one another and reconciled any inconsistencies in the coding process. This process generated a final report including the frequency of occurring concept codes and representative diary entry quotes.
Before full-transcript coding, intercoder agreement (ICA, the extent to which independent coders were concordant in their coding) was evaluated. ICA was determined by evaluating the percent agreement, defined as the proportion of coding decisions that reached agreement out of all coding decisions made by coder(s). Achieving greater than or equal to 90% agreement within the first 10% of transcripts was considered acceptable for ICA and was reached by all coders.
Qualitative data from the CE portion of the interviews were further assessed for conceptual saturation, in accordance with the International Society for Pharmacoeconomics and Outcomes Research Task Force recommendations (Cox et al. 2009). Saturation was considered achieved when no new information was obtained during subsequent interviews and was evaluated separately for adolescents versus parents.
To evaluate conceptual saturation, sets of concepts spontaneously emerging from the interviews were analyzed in the order in which data were collected (e.g., concepts emerging in the first 25% of interviews were compared with the next 25% of interviews, with this process repeated [i.e., the first two sets {50%} combined and compared with the next 25%] until the end of the interview period). Performing this stepwise analysis of new concepts in each individual interview facilitated a quantification of the degree to which novel concepts were—or in the case of saturation, were not—emerging with continued interviews. In addition to monitoring, if adequate sample size had been reached, this method also created a means of highlighting the emergence of concepts. This facilitated development of a comprehensive list of new concepts and identified subconcepts recurring across interviews to enable saturation of broader concepts.
Graphs visualizing the rate of concept accumulation over the course of consecutive interviews are available in Supplementary Figures S1 and S2. Concept emergence was plotted such that each new concept introduced by a subject increased the slope of the line graph, and the asymptotic limit was reached when there was no increase in slope.
Results
Demographics
Demographics of the adolescent and parent subjects enrolled in this study are summarized in Tables 1 and 2, respectively. Of the 17 pairs of adolescents and parents initially recruited, 17 parents and 16 adolescents completed the interview (with 1 adolescent unable to attend the interview due to a medical emergency before the scheduled interview date). The mean age for adolescents was 14.8 years, ranging from 13.2 to 16.7 years, with subjects in school up to the 10th grade. The majority were male (76.5%) and white (52.9%). The mean time since diagnosis as reported by the clinician, which in the majority of cases was a psychiatrist (82.4%), was 6.1 years.
Adolescent Demographics
Subject demographics reported by parent.
Not mutually exclusive; clinician or his/her representative selected more than one current or past treatment for IA for some subjects.
Stimulants named by clinicians included (number of subjects taking currently, past): methylphenidate (2, 3); dextroamphetamine (2, 1); methylamphetamine (1, 1); lisdexamfetamine (1, 0).
ADHD, attention-deficit/hyperactivity disorder; IA, impulsive aggression; ODD, oppositional defiant disorder; SD, standard deviation.
Parent Demographics
One subject selected both working full- or part-time and homemaker.
GED, general educational development; IA, impulsive aggression; SD, standard deviation.
All adolescents were being treated for ADHD with one of the following: methylphenidate (47.1%), amphetamine (47.1%), or guanfacine (5.9%). Most adolescent subjects were not receiving any treatment for their IA at the time of interview (64.7%), with half of the population having no history of taking any treatment for their IA (52.9%). Some adolescent subjects (35.3%) were currently receiving or had in the past received one or more of the following treatments for IA: methylphenidate (11.8%), dextroamphetamine (11.8%), lithium (5.9%), methylamphetamine (5.9%), lisdexamfetamine (5.9%), and psychotherapy or counseling (5.9%).
CE results
Among 16 adolescents reporting IA behaviors, CE interviews revealed a total of 28 unique concepts, 22 of which were reported spontaneously by at least 1 subject. The most frequently reported behaviors (defined as being reported by ≥66% of adolescents) included arguing (n = 15, 93.8%); raising their voice, shouting, and/or yelling (n = 15, 93.8%); hitting (n = 14, 87.5%); slamming (n = 14, 87.5%); pushing/shoving (n = 13, 81.3%); breaking (n = 12, 75.0%); fighting (n = 12, 75.0%); throwing (n = 12, 75.0%); and cursing (n = 11, 68.8%) (Fig. 1). All these concepts were already components of the pediatric IA diary, with the exception of “breaking,” which was among the larger item pool of 30 behaviors originally included in the provisional electronic diary, but not the 15-item pediatric IA diary. These behaviors were most commonly triggered by subjects feeling annoyed or offended, receiving attention they did not desire, not getting their way/being asked to do something outside of what they wanted, feeling or being provoked, or as a result of “messing around.” Seventy-three percent of the 22 spontaneously reported concepts emerged in the first group of interviews (n = 4) and 86% were reported after the second group of interviews (n = 8). Following the third cohort (n = 12) of interviews, 95% of concepts had been reported, and no new concepts emerged after the fourth cohort of interviews, suggestive of conceptual saturation (Supplementary Fig. S1).

Frequency of adolescent-reported behaviors from the
By comparison, among 17 parents reporting behaviors of IA in their adolescents, a total of 31 unique concepts emerged from CE interviews, 26 of which were reported spontaneously by at least 1 subject. The most frequently reported behaviors (defined as being reported by ≥66% of parents) included raising their voice, shouting, and/or yelling (n = 16, 94.1%); arguing (n = 15, 88.2%); being disrespectful/mean/rude (n = 15, 88.2%); slamming (n = 15, 88.2%); throwing (n = 15, 88.2%); cursing (n = 14, 82.4%); hitting others (n = 14, 82.4%); shoving and/or pushing (n = 14, 82.4%); breaking (n = 13, 76.5%); name-calling (n = 13, 76.5%); and threatening (n = 12, 70.6%) (Fig. 2). Of these concepts, being disrespectful/mean/rude and breaking are not part of the pediatric IA diary (discussed below). Similar to the adolescent reporting, 65% of the 25 spontaneously reported concepts were reported in the first group of interviews (n = 4) and 77% were reported after the second group of interviews (n = 8). Following the third cohort (n = 13) of interviews, 96% of concepts were reported, and no new concepts emerged after the fourth cohort of interviews, suggestive of conceptual saturation Supplementary Fig. S2).
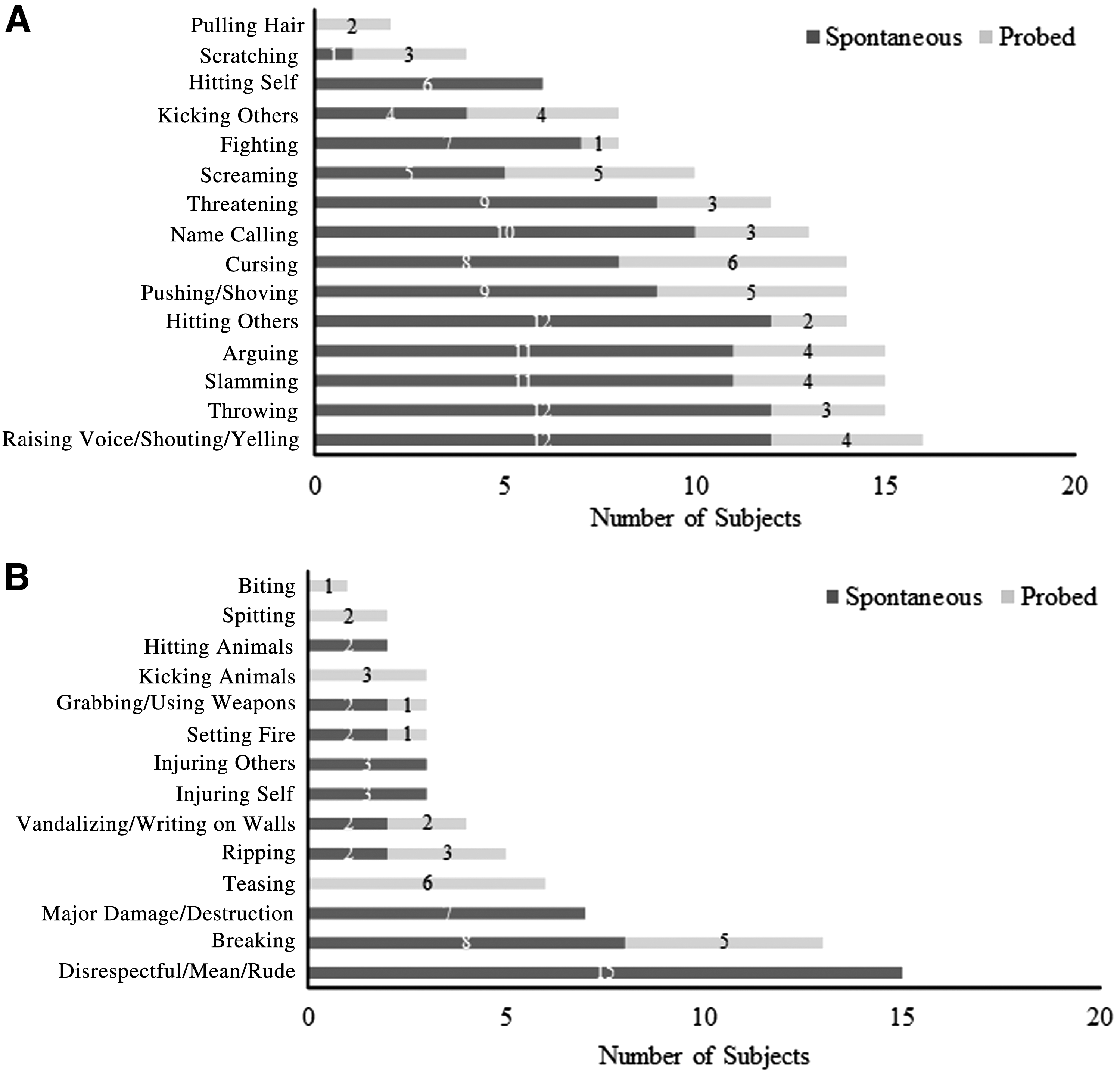
Frequency of parent-reported behaviors from the
Although parent and adolescent reports were similar in terms of CE, some behaviors were mentioned by parents but not by adolescents, and parents generally described a particular behavior in greater detail (e.g., frequency of the behavior, severity of the behavior). For example, whereas one adolescent dismissed the behavior of hitting an animal, the parent described this behavior in rich detail. Thus, there may be instances when the adolescent is less willing to describe or characterize a behavior for fear of self-incrimination, societal stigma, and/or other reasons.
CI results
CIs aimed at assessing the performance of the IA diary indicated that 100% of the instructions were understood by parents and adolescents. In addition, all parents and adolescents understood 100% (15/15) of the behaviors that are part of the 15-item pediatric IA diary (i.e., yelling, screaming, threatening, scratching, throwing, slamming, hitting self, arguing, cursing, name-calling, shoving/pushing, pulling hair, fighting, hitting others, and kicking others). The only term that elicited confusion was “breaking,” as this behavior could result from an intent to break an object (such as snapping a pencil after frustration) or could be a consequence of another aggressive behavior already included in the diary (such as throwing an object, inadvertently culminating in the object being broken).
No significant issues were found in terms of usability of the LogPad App on a Nexus 5, with most adolescent and parent subjects giving the device an excellent rating regarding overall ease of use (>90.0%), ability to select an answer and advance to the next screen (>85.0%), and sensitivity and readability (>75.0%). The most prominent usability issue reported was the appearance of the application on the device, with four subjects (12.1%) rating the appearance as 3 or lower (on a scale of 1–5, where 1 = poor and 5 = excellent), and two subjects (6.1%) giving a score of 3 or lower due to the readability of the font size.
Summary
Six verbal behaviors that are part of the 15-item pediatric IA diary were endorsed by more than half of the total subjects: yelling (93.9%), arguing (90.9%), cursing (75.8%), name-calling (69.7%), threatening (63.6%), and screaming (57.6%). Most physical behaviors directed at others were not endorsed frequently (<25%)—including spitting, biting, scratching, pulling hair, and grabbing a weapon—with the exception of shoving/pushing and fighting, which are part of the pediatric IA diary and were endorsed by 81.8% and 60.6% of total subjects, respectively.
Slamming (87.9%), throwing (81.8%), and breaking (75.8%) were the most highly endorsed physical behaviors directed at objects, with the latter behavior being the only item not part of the pediatric IA diary due to the variability in the users' definition of the term (discussed further below). Hitting (90.9%) and kicking others (51.5%), which are both included in the pediatric IA diary, were the only hitting/kicking behaviors endorsed by more than half of all subjects. Finally, behaviors related to severely injuring oneself, others, or animals were not frequently endorsed in the study population, consistent with what was seen in children.
Discussion
Collectively, these findings support the application of the 15-item pediatric IA diary in adolescents with ADHD. The results of the CE and CIs suggest that the 15-item IA diary developed for children may also be used to appropriately assess the behaviors of IA in adolescents with ADHD. Furthermore, these findings provide novel data on the perception of IA from both the adolescent and parent perspectives and demonstrate that while there were no significant differences between parent and adolescent item endorsements, parents may be more candid than adolescents when reporting the nature of IA behavior, as they tend to describe behaviors in greater detail.
The pediatric IA diary was previously developed as an eObsRO instrument for assessing the frequency of IA-related behaviors in children aged 6–12 years with ADHD (Ceresoli-Borroni et al., submitted for publication). In this study, we used CE interviews of adolescents and their parents to evaluate the relevance of the behavioral concepts of this 15-item diary in adolescents aged 13–17 years. The majority of parents and adolescents found the concepts encompassed within the pediatric IA diary to also be relevant for their own experiences, with yelling, arguing, cursing, name-calling, threatening, shoving/pushing, fighting, throwing, slamming, and hitting each being reported by >60% of the subjects. However, two items found in the pediatric IA diary—scratching and hair pulling—were not frequently endorsed (each reported by <25% of the population). The low reporting of these two behaviors may be reflective of the study's sample population, which was 77% male, given that boys tend to have shorter hair and/or nails than girls and may be less likely to pull hair or scratch in the context of fighting. Although these concepts were reported less frequently than others, these items could serve to help characterize the IA experience in subsets of adolescents, perhaps primarily those who are female. Furthermore, as the prevalence of ADHD is higher in boys than in girls in the United States, one would expect the frequency of behaviors described here in a demographically similar population to relate to predicted IA behavior in the broader ADHD population (FDA News Web Site 2017).
The CE portion of the interviews identified one concept—being disrespectful/mean/rude—that was frequently reported by parents (>60%) but was not part of the larger item pool of 30 behaviors originally included in the provisional electronic diary. This concept was parent-defined as speaking in an offensive and inappropriate manner such as “talking back” or being disruptive to parents or teachers. Notably, the parental frequency of reporting on this behavior warranted a conceptual category of its own, but the concept was not reported as frequently by adolescents (88.2% for parents vs. 56.3% for adolescents). The concept of being disrespectful/mean/rude is further complicated by the fact that it can be considered a general disposition of the IA individual, encompassing other IA behaviors already endorsed in the diary (e.g., arguing is an endorsed behavior and may include rude or disrespectful attitudes before or during an argument). Additionally, what is considered disrespectful, mean, or rude to one parent may not be for another, suggesting that it is a behavior intimately tied to the perception of the parent on the receiving end, and not an objectively observable behavior. From the adolescents' perspective, being disrespectful sometimes overlapped with “arguing,” although this varied between subjects. The low rate of self-reporting of disrespectful/mean/rude behavior may also be reflective of a reduced ability of adolescent subjects to consistently recognize these behaviors in themselves. Based on this rationale, adding a separate item to the IA diary for being disrespectful/mean/rude is not recommended.
In a similar manner, breaking was the only behavior that was highly endorsed by both adolescents and parents (75.8% and 76.5%, respectively) in the adolescent subject population that was not included in the original pediatric IA diary. However, evaluation of subject quotes regarding this behavior found that it was an imprecise term that can include an action with the intention of damaging (e.g., breaking pencils or making holes in walls) or the accidental result of an aggressive action (e.g., breaking a TV with a thrown object). These definitions, for example, would already be covered by other items assessed in this study, such as throwing (also included in the pediatric diary and cited as the most common action leading to “breaking”) or damaging. Due to the variability of the behavior (intended action vs. inadvertent consequence), the addition of “breaking” to the pediatric 15-item IA diary for use in adolescents is not recommended despite it being commonly reported.
An additional objective of this study was to evaluate the agreement of parent versus adolescent reporting within the IA diary. With respect to consistency between the parent-reported and adolescent-reported data, no significant differences were observed for the type of behaviors or number of concepts reported. However, despite the lack of observed quantitative differences between parent and adolescent reports, interviewers generally found qualitative differences between reports from members of parent/adolescent pairs. Specifically, parents were more likely to provide details about the frequency or severity of the behavior, whereas adolescents were more likely to simply acknowledge that they had done the behavior.
Although these minor differences do not affect the utility of the IA diary as a behavioral measurement tool, they do suggest that parent/caregiver reporting may be more accurate than adolescent reporting. This trend was particularly evident in other instances in which the adolescent was less willing to admit to a behavior for fear of self-incrimination and/or a societal stigma attached to a particular behavior. For example, in response to diary behaviors pertaining to treatment of animals, one adolescent subject denied injuring animals and stated that “hitting an animal means you might be a psychopath/sociopath,” whereas their parent reported the subject had indeed hurt animals and found this to be a most concerning IA behavior. Although such behavior was rarely reported across subjects, it remains important to consider the possibility of adolescents omitting severe IA behaviors during self-reporting and underscores the importance of parent/caregiver inclusion during the reporting process. However, the possibility that such severe behaviors could be omitted by adolescents and even perhaps by their caregivers, both of whom might be unwilling to admit that an upsetting act occurred, remains a limitation of a reporting device reliant on subjects or their close family members.
Nonetheless, the IA diary as reported by both adolescents and their parents achieved conceptual saturation, despite a small sample size. The cohort was typical for a qualitative study and suggests that an adequate population size was reached (Turner-Bowker et al. 2018). Saturation analysis of parent and adolescent CE interviews corroborated the efficacy of the device in picking up novel concepts, as the majority (65%) of new concepts emerged in the first half of the interview set, with the rate of new added concepts plateauing during the second half. The core, qualitatively relevant behaviors of IA were sufficiently elicited to the point of saturation (i.e., additional interviews were unlikely to yield any new relevant information related to IA) during these exercises, indicating that the included IA behaviors are a strong representation of those experienced by families impacted by IA.
In addition to data collection on IA behaviors themselves, questions on the usability of the device were incorporated into the interview process. During the CI exercise, no significant issues were found with the usability of the tool. It should be noted that the interviewing exercise consisted of all subjects using the device with no prior training, and any minor usability issues with the device are likely to be worked out with training and repeated use. These data indicate that the IA diary is a user-friendly tool.
Importantly, the prevalence of specific IA behaviors in adolescents was hitherto unknown and therefore had not been compared with that in children. Understanding the differences and similarities between childhood and adolescent IA is important, not only for assessing and monitoring IA throughout development but also to better understand the behaviors parents and clinicians can anticipate in their children and patients. The finding that the pediatric IA diary is also applicable to adolescent behavior suggests that there is a distinct common thread of behaviors encompassing persistent IA from childhood through adolescence.
It is important to note, however, that the behaviors captured were limited to those linked with IA, a form of reactive aggression, specifically to define this aggressive subtype. It would be interesting to explore how many children and adolescents with IA also exhibit forms of proactive aggression, as well as determine if there are behaviors that quantitatively overlap between these forms of aggression. Similarly, assessment of the IA diary has thus far been limited to children and adolescents with ADHD, and therefore, its reliability for monitoring IA symptoms in other disorders is currently unknown. Finally, this was a qualitative study, and while these data indicate the IA diary is a strong assessment tool for measuring IA in adolescents, its usefulness as a clinical outcome measure in adolescents remains unclear.
Conclusions
The CE and CI findings reported in this study support the use of the 15-item parent-/caregiver-reported IA diary to identify the behaviors of IA in a population of adolescents (aged 13–17 years) with ADHD. The 15-item IA diary is a novel convenient tool for assessing IA behavior in adolescents with ADHD.
Clinical Significance
IA behavior in ADHD is often persistent following ADHD treatment, and no tool for assessing IA symptoms in adolescents was previously available. The ability to capture IA behavior with the IA diary in both children and adolescents should improve the monitoring of IA symptomatology throughout development. Further validation of the IA diary, and its potential use in clinical practice, is ongoing in Phase 3 studies.
Footnotes
Disclosures
G.C.-B., T.L., N.F., S.A.C., A.N. and S.S. are employees of Supernus Pharmaceuticals, Inc.
S.T.B. is a former employee of Supernus Pharmaceuticals, Inc., and has received royalties from the Harvard University.
D.F.C. has received research and consulting fees from Shire and is a consultant for Supernus Pharmaceuticals, Inc.
C.J.E. and S.H. are employees of Endpoint Outcomes.
R.L.F. receives or has received research support, acted as a consultant, and/or served on a speaker's bureau for Aevi, Akili, Alcobra, Allergan, Amerex, American Academy of Child and Adolescent Psychiatry, American Psychiatric Press, Arbor, Bracket, Daiichi-Sankyo, Epharma Solutions, Forest, Genentech, Insys, Ironshore, KemPharm, Lundbeck, Merck, NIH, Neurim, Noven, Nuvelution, Otsuka, PCORI, Pfizer, Physicians Postgraduate Press, Roche, Sage, Shire, Sunovion, Supernus Pharmaceuticals, Inc., SyneuRx, Teva, TouchPoint, Tris, and Validus.
A.S.R. has received consulting fees, research support, and travel support from Actavis/Forest Laboratories and Lundbeck/Takeda and has received honoraria and travel support from AACAP, AAP, Case Western Reserve University, College of Neurologic and Psychiatric Pharmacists, Neuroscience Education Institute, Nevada Psychiatric Association, and NACCME. A.S.R. is on the data safety monitoring board for Aevi Genomic Medicine, Inc., Neuronetics, and NIMH. A.S.R. has received royalties from Eli Lilly, GlaxoSmithKline, Guilford Press, and Johnson and Johnson. A.S.R. has received consulting fees from Bracket and honoraria from the Child and Adolescent Psychiatric Society of Greater Washington. A.S.R. has received research support from the National Center for Advancing Translational Sciences, NINDS, Supernus Pharmaceuticals, Inc., and SyneuRx. A.S.R. has been an advisor for NICHD and the University of Cambridge. A.S.R. has received research support, stock/equity, and travel support from Pfizer Inc. A.S.R. has been an advisor for and received travel support from Sunovion Pharmaceuticals Inc.
K.E.S. has received research support from Otsuka, and received research support and served as a consultant and advisory board member for Supernus Pharmaceuticals, Inc.
Supplementary Material
Supplementary Figure S1
Supplementary Figure S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.