
Abstract
Objectives:
To characterize psychotropic use preceding antipsychotic initiation in a population of youth in foster care and to determine whether the use of intensive psychiatric services before initiating an antipsychotic differs across subgroup of youth defined by past psychotropic use.
Methods:
We identified youth in foster care in one U.S. State who initiated an antipsychotic from 2010 to 2015 and were aged ≤21 years at initiation. No antipsychotic use 1-year before the index prescription defined new use. Psychotropic class use in the year preceding the index antipsychotic prescription distinguished three subgroups: no psychotropic use, single-class use, and concomitant (>1 class) use. The temporal association of antipsychotic initiation with intensive services (psychiatric hospitalizations or emergency department visits) was estimated through regression models adjusted for psychiatric diagnoses and demographic characteristics. Logistic regression models assessed the interaction between psychotropic class subgroup and psychiatric diagnosis with the odds of hospitalization.
Results:
Of the 753 youth initiating an antipsychotic, 279 (37%) had no psychotropic use, 304 (40%) had single-class use, and 170 (23%) had concomitant use in the year before. In the year preceding antipsychotic initiation, 183 (24%) were hospitalized and 118 (16%) were hospitalized 1 month before antipsychotic initiation. The number of days between hospital discharge and antipsychotic initiation was 47 (SE = 19) days longer in concomitant users relative to youth with no psychotropic use (p = 0.01). In the year preceding antipsychotic initiation, concomitant users with severe mental illness were less likely to have a hospitalization (OR = 0.24; 95% CI = 0.06–0.93) than youth with no psychotropic use diagnosed with severe mental illness.
Conclusions:
Variation in psychotropic medication treatment, hospitalizations, and psychiatric diagnosis before antipsychotic initiation distinguished subgroups of youth initiating an antipsychotic. Single-class and concomitant users may have initiated an antipsychotic to augment existing regimen, whereas youth with no psychotropic use may have initiated an antipsychotic following a first episode crisis.
Introduction
Recent estimates indicate that 12% of youth in foster care are prescribed an antipsychotic medication (Matone et al. 2015). This is three times higher than among nonfoster care, Medicaid-insured children and adolescents (Vanderwerker et al. 2014; Matone et al. 2015). Possible reasons for the higher prevalence of antipsychotic medication use among youth in foster care include exposure to trauma, disruptions in caregiver relationships, frequent relocations to a new community, concerns of unsafe behavior toward self and others, and pressure to stabilize behavior quickly to avoid a change in foster placement (Government Accountability Office 2011; Cross et al. 2013; Vanderwerker et al. 2014).
Several states implemented policies, that is, prior authorization and informed consent, to address antipsychotic prescribing in Medicaid-enrolled youth, including those in foster care (Schmid et al. 2015; dosReis et al. 2016; Government Accountability Office 2017; Mackie et al. 2017). Recent evidence shows that these policies have led to modest reductions in antipsychotic use (Stein et al. 2014; Crystal et al. 2016; Barclay et al. 2017; Zito et al. 2018), but for youth with serious emotional and behavioral disorders, reducing antipsychotic use may not be the best practice (Government Accountability Office 2017). Despite extensive research on antipsychotic use among youth in foster care, heightened national attention to ensure judicious use, and the implementation of psychotropic monitoring policies, there is sparse information on psychotropic use or intensive psychiatric services use preceding antipsychotic initiation. It is possible that antipsychotic medications are initiated following a psychiatric hospitalization or emergency department (ED) visit, but there also may be situations where treatment is initiated before a trial of other psychotropic medications. Knowledge of the temporal association between initiation of an antipsychotic following a hospitalization or ED visit, and whether there was use of other psychotropic medication before antipsychotic initiation can place in context important patterns of care that influenced prescribing. This information can be important when considering appropriate use in the context of clinical needs within an individualized treatment planning framework (American Academy of Child and Adolescent Psychiatry 2015). This is particularly important for youth in foster care where the influence of contextual factors on antipsychotic prescribing is paramount.
Our objective was to examine variations in and temporality of intensive psychiatric services and psychotropic medication use before the start of an antipsychotic among youth in foster care. The specific aims were to (a) characterize subgroups with different patterns of psychotropic class use in the year preceding antipsychotic initiation, (b) examine the temporal associations between the most recent psychiatric-related hospitalization and ED visit with antipsychotic initiation in relation to psychotropic use in the preceding year, and (c) assess the interaction of psychiatric diagnosis and psychotropic use with psychiatric-related hospitalization in the year preceding antipsychotic initiation.
Methods
Study design and cohort identification
Using a retrospective cohort study design, we identified all youth involved in foster care in one U.S. State from 2010 through 2015 who initiated any antipsychotic medication during this time (Supplementary Table S1). A new antipsychotic user was defined as youth who had no antipsychotic use in the 365 days preceding the index antipsychotic prescription. The earliest date of an index antipsychotic prescription was January 1, 2010, to ensure that the 365-day washout period did not extend beyond January 1, 2009, which was the earliest data available. To be included in the analysis, new antipsychotic users had to be aged ≤21 years at the time of the index antipsychotic prescription and continuously involved in foster care 1-year before the index antipsychotic prescription. Continuous involvement in foster care was defined based on the time between the dates of removal and of return to the child's biological family home. All youth who are in foster care are automatically enrolled in Medicaid. The protocol was approved by the institutional review boards for the university and each state agency.
Data sources
This study used linked administrative data from child welfare with Medicaid mental health services and pharmacy claims data. Child welfare administrative data provided information on the child's age, gender, race, dates of removal from and return to the child's biological family home, dates of entry and exit from foster placement settings, and the foster placement type.
The Medicaid claims consist of mental health service claims for all services provided by the state's mental health carve-out program, and thus, all inpatient and outpatient claims were for psychiatric-related services. The pharmacy claims represent all outpatient prescription dispensings for youth in foster care within the state. Claims for inpatient and outpatient psychiatric services contained service dates, International Classification of Diseases, Ninth Revision (ICD-9) diagnosis codes, Current Procedural Terminology (CPT) codes, and place of service. Pharmacy claims for psychotropic prescriptions dispensed in outpatient pharmacies included the dispensing date, National Drug Code, generic drug name, quantity, and days supplied.
Study variables
Psychotropic class subgroups
Antipsychotic new users were characterized by medication use from other psychotropic classes in the 365 days before the index antipsychotic prescription. Individual psychotropic medications were categorized by therapeutic class as follows: antidepressants (e.g., fluoxetine, sertraline), mood stabilizers (e.g., lithium and anticonvulsant: carbamazepine, lamotrigine, and valproic acid), attention-deficit/hyperactivity disorder (ADHD) medications (e.g., stimulants and atomoxetine), antianxiety (e.g., lorazepam, buspirone), and sedatives (e.g., zolpidem); see Supplementary Table S1.
Psychotropic use was summarized in each of the twelve 30-day intervals before the index antipsychotic prescription (Fig. 1). Thirty-day intervals were used to distinguish “as needed” use from chronic treatment and to closely measure medication overlap. A medication in one of the targeted psychotropic classes, that is, antidepressant, mood stabilizer, ADHD medication, antianxiety or sedative, had to be available for ≥7 days of the 30-day interval to qualify as treatment in an interval. This mitigated misclassification due to tapering as needed use only. Concomitant use was defined as >15 days of overlapping use with two or more psychotropic classes in the 30-day interval. We identified all 30-day intervals with none, single, or concomitant use in the year preceding the index antipsychotic prescription.
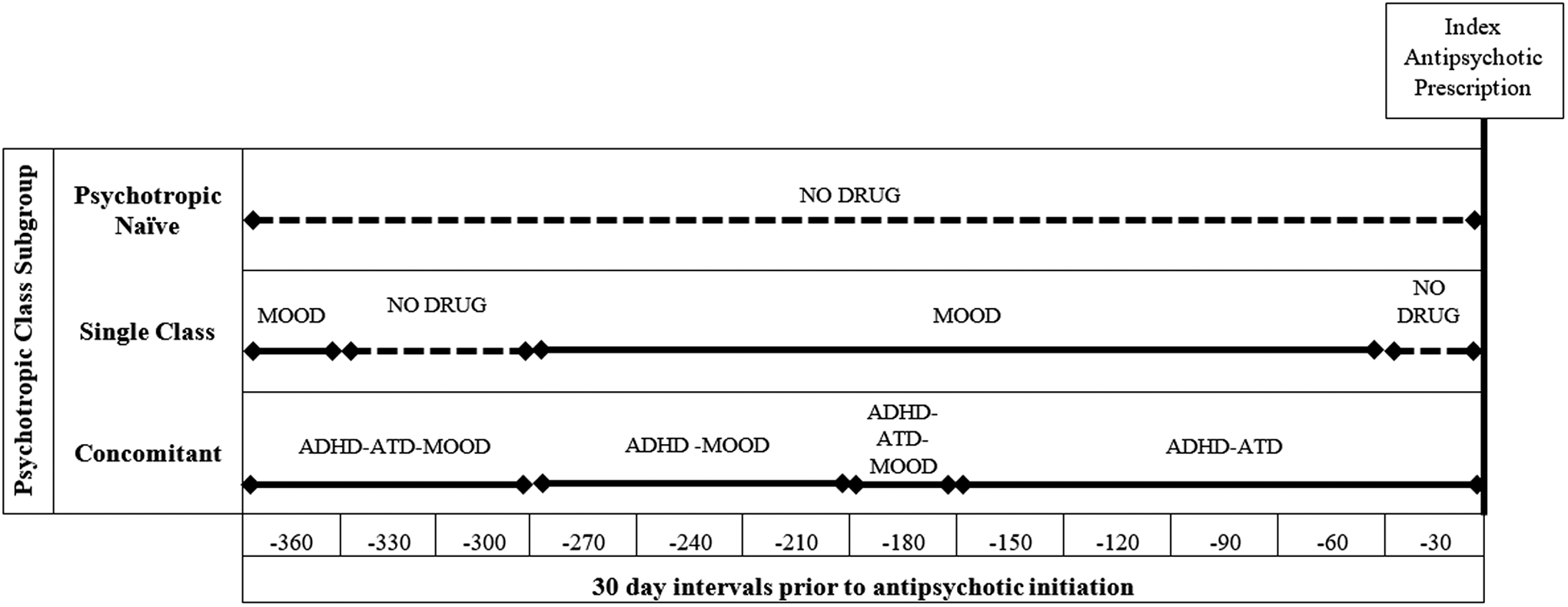
Medication patterns defining new antipsychotic user subgroups. The X-axis represents the twelve 30-day intervals before antipsychotic initiation, with interval −360 representing the month furthest away from initiation and interval −30 representing the month immediately before initiation. Dotted lines show periods of no psychotropic drug use, whereas solid lines represent periods in which a psychotropic medication was present. The medication present during the intervals is labeled above each line. ADHD, attention-deficit/hyperactivity disorder medications (e.g., stimulants and atomoxetine); ATD, antidepressant medications (e.g., fluoxetine, sertraline); MOOD, mood stabilizers (lithium and anticonvulsants, e.g., carbamazepine, lamotrigine); NO DRUG, no medication use during interval.
Psychiatric hospitalization and ED visits
Both CPT codes (hospitalization: 99221–99223, 99231–99233, 99238 and 99239; ED: 99281–99285) and place of service codes (hospitalization: 21 and 51; ED: 23) were used to distinguish hospitalizations and ED visits with a psychiatric diagnosis in the 365 days before the index antipsychotic prescription. All youth with at least one hospitalization or ED discharge in the 365 days before the index antipsychotic were classified as having received psychiatric services in these settings.
We identified the most recent hospitalization or ED discharge before the index antipsychotic prescription. Temporality was estimated by the number of days from the most recent discharge date to the index antipsychotic prescription dispensing date. A constant of one was added to all calculations to avoid zero values for discharge dates that occurred on the same day as index antipsychotic prescription dispensing.
Psychiatric diagnosis classification
The ICD-9 diagnosis codes associated with inpatient and outpatient psychiatric service claims were categorized by major diagnostic groups: severe mental illness (bipolar/mood disorder, depression, psychotic disorder/schizophrenia), disruptive behavior disorders (ADHD, conduct disorder, and oppositional defiant disorder), and emotional or internalizing disorder (anxiety and posttraumatic stress disorders [PTSD]). In the year preceding the index antipsychotic prescription, we identified all psychiatric diagnoses associated with any mental health-related visit. Total number of psychiatric diagnoses was also estimated (Supplementary Table S2).
Covariates
The child welfare administrative data provided all demographic characteristics for youth in foster care, including race, age, and gender. We estimated the number of days in foster care and the number placement changes before the index antipsychotic prescription based on the entry and exit dates for individual foster placements. Mental health service claims were used to identify outpatient office visit and family, individual, or group psychotherapy.
Statistical analyses
Demographic and clinical characteristics across psychotropic class subgroups were compared using descriptive and bivariate statistics. Bivariate chi-square was used to compare categorical variables (race, gender, severe mental illness, disruptive disorder, emotional internalizing disorder, psychotherapy, and outpatient office visit). Analysis of variance was used to compare continuous variables across the three psychotropic class subgroups (age, number of foster care placement changes, number of psychiatric diagnoses, and number of months involving single or concomitant psychotropic use). Analyses were conducted for the aggregate sample and stratified by psychotropic class subgroup.
We used multivariable linear regression models to estimate the mean difference in days since last hospitalization or ED discharge before antipsychotic initiation, and its variation across psychotropic class subgroups. Multivariable logistic regression models assessed the associations between psychotropic class subgroups and psychiatric hospitalization and ED visits within 1 year (≤365 days) and 1 month (≤30 days) before the index antipsychotic prescription. Interaction terms between psychotropic class subgroup and psychiatric diagnosis were included in the models to assess the combined impact of psychotropic class subgroup and psychiatric diagnosis on hospitalization. All models were adjusted for psychiatric diagnoses, age, gender, and race. Analyses were conducted using SAS 9.4 (Cary, NC).
Results
Characteristics of the cohort and psychotropic subgroups
The 753 youth who newly initiated an antipsychotic during the study period were, on average, aged 15 years (SD = 4.4), African American (n = 519, 69%), and male (n = 384, 51%). During the 1 year before the index antipsychotic, youth had on average 3 (SD = 2.9) foster care placement changes, 3 (SD = 1.5) comorbid psychiatric conditions, 6 (SD = 4) months of psychotropic medication use, and approximately three-quarter had psychotherapy (n = 558, 74%) (Table 1). Psychotropic class use in the 365 days preceding the index antipsychotic prescription differentiated three psychotropic class subgroups: no psychotropic use (n = 279, 37%), single-class use (n = 304, 40%), and concomitant use (n = 170, 23%). No psychotropic use defined youth who did not have any prescriptions for a psychotropic medication in the 365 days preceding the index antipsychotic. Single-class users were prescribed a medication from at least one psychotropic class and did not have any concomitant class use. Concomitant users were prescribed two or more psychotropic classes in at least one 30-day interval over the 365 days preceding the index antipsychotic prescription (Fig. 1).
Demographic and Clinical Characteristics of Youth in Foster Care Initiating Antipsychotics From 2010 to 2015
—, represents cells that are not reportable due to sample ≤11.
Sample size reported for youth with at least one diagnosis and at least one foster care placement change.
No psychotropic subgroup has 0 months of medication use.
Index defined as start of an antipsychotic.
ADHD, attention-deficit/hyperactivity disorder; ED, emergency department.
Overall, 665 (88%) had at least one psychiatric diagnosis. Among youth with no psychotropic use in the preceding year, the most common psychiatric diagnostic group was severe mental illness (n = 175, 62%), whereas disruptive behavior disorders were the most common among single-class users (n = 196, 65%) and concomitant users (n = 135, 79%). Compared with the no psychotropic use subgroup, concomitant users had more comorbid psychiatric conditions (p = 0.0004) and were more likely to have depression (39% vs. 24%; p = 0.001), ADHD (68% vs. 26%; p < 0.0001), oppositional defiant disorder (28% vs. 15%; p = 0.007), and PTSD (22% vs. 14%; p = 0.04). The use of psychotherapy in the year before antipsychotic initiation was more common among concomitant users (n = 140, 82%) than youth with no prior psychotropic use (n = 179, 64%).
Overall, 183 (24%) youth were hospitalized in the year before the index antipsychotic prescription and 118 (16%) were hospitalized 30 days before the index antipsychotic prescription. Of hospitalized youth, a larger proportion of youth with no prior psychotropic use were hospitalized 30 days before antipsychotic initiation when compared with concomitant users (77% vs. 53%; p = 0.03). In the year before the index antipsychotic prescription, 183 (24%) youth had an ED discharge and 82 (11%) occurred 30 days before the index antipsychotic prescription. Among youth with an ED visit, 36 (61%) youth with no prior psychotropic use had an ED discharge in the 30 days before the index antipsychotic prescription compared with 19 (39%) of concomitant users (p = 0.009).
Temporality of psychiatric hospitalization and ED visits to index antipsychotic prescription
The results of multivariable regression models assessing the association between the temporality of hospitalization and ED discharges with psychotropic class subgroups are presented in Table 2. Among hospitalized youth, the average days between the most recent hospitalization and antipsychotic initiation was 34.1 (SE = 18.6) for those with no prior psychotropic use, 61.0 (SE = 17.2) among single-class users, and 80.9 (SE = 19.4) among concomitant users. Relative to youth with no prior psychotropic use, the number of days between the most recent hospital discharge and antipsychotic initiation was 46.9 (SE = 18.9; p = 0.01) days longer in concomitant users. If the hospitalization occurred in the 30 days preceding the index antipsychotic prescription, the average days between discharge and antipsychotic initiation was 1.3 (SE = 1.8) for youth with no prior psychotropic use, 5.7 (SE = 1.7) in single-class users, and 2.0 (SE = 2.1) in concomitant user. The time between the antipsychotic index prescription and the most recent hospitalization was significantly longer among single-class users when compared with those with no prior psychotropic use (mean: 4.4; SE = 1.6; p = 0.007).
Temporality Between Most Recent Hospitalization and Emergency Department Visits and Antipsychotic Initiation
All models adjusted for age, race, and psychiatric diagnosis category.
Index defined as start of an antipsychotic.
ED, emergency department.
Among youth with an ED visit in the year before antipsychotic initiation, the most recent ED discharge was on average 79.9 (SE = 20.2) days before antipsychotic initiation for youth with no prior psychotropic use, 117.8 (SE = 18.5) days prior for single-class users, and 122.4 (SE = 20.5) days prior for concomitant users. The days between the most recent ED discharge and the index antipsychotic prescription among single-class users and concomitant users were on average 37.8 (SE = 17.9) and 42.5 (SE = 20.5) days longer, respectively, relative to youth with no prior psychotropic use.
Description of psychiatric diagnosis by hospitalization status
We compared the demographic and clinical characteristics in the year before the index antipsychotic prescription between hospitalized and nonhospitalized youth within each psychotropic class subgroup (Table 3). Among concomitant users, hospitalized youth had more foster care placement changes than nonhospitalized youth (3.5 vs. 2.5; p = 0.04) in the 365 days before antipsychotic initiation. On average, hospitalized youth had twice the number of comorbid psychiatric conditions than nonhospitalized youth across all psychotropic class subgroups. In youth with no prior psychotropic use, severe mental illness was the most common diagnosis in both hospitalized (n = 63, 98%) and nonhospitalized (n = 112, 52%) youth. Among single-class users, hospitalized youth were most commonly diagnosed with severe mental illness (n = 68, 92%). However, the most common diagnosis among nonhospitalized single-class youth was disruptive disorders (n = 137, 60%). Among concomitant users, disruptive disorder was the most common diagnosis in both hospitalized (n = 42, 93%) and nonhospitalized youth (n = 93, 74%).
Demographic and Clinical Characteristics by Hospitalization Status and Psychotropic Class Subgroup in the Year Before Antipsychotic Initiation Among Foster Care Youth (2010–2015)
—, represents cells that are not reportable due to sample ≤11.
Sample size reported for youth with at least one diagnosis and at least one foster care placement change.
No psychotropic use subgroup has 0 months of medication use.
ADHD, attention-deficit/hyperactivity disorder.
In multivariable logistic regression models (Table 4), we tested the interaction between psychotropic class subgroup and psychiatric diagnosis on hospitalization. We found no significant interaction between psychotropic class subgroup and disruptive disorders or emotional internalizing disorder. However, there was a significant interaction between psychotropic class subgroup and severe mental illness. When compared with youth with no prior psychotropic use who had a severe mental illness, concomitant users with severe mental illness were less likely to be hospitalized in the year before antipsychotic initiation (OR = 0.24; 95% CI: 0.06–0.93). In the 30 days before antipsychotic initiation, single-class users with severe mental illness (OR = 0.48; 95% CI: 0.25–0.93) and concomitant users with severe mental illness (OR = 0.26; 95% CI: 0.11–0.61) were less likely to have a hospitalization when compared with those who had no prior psychotropic use and had a severe mental illness.
Association Between Psychotropic Class Subgroup and Psychiatric Diagnosis with Hospitalization Before Antipsychotic Initiation Among Youth in Foster Care From 2010 to 2015
Main effects for psychotropic class subgroup not significant and not reported. No interaction observed between psychotropic class subgroup and disruptive disorders or emotional internalizing disorders.
Index defined as start of an antipsychotic.
Discussion
Our findings point to variations in the clinical needs of youth who initiate an antipsychotic. In this cohort of youth in foster care in one state, more than one-third of youth who initiated an antipsychotic did not have use of another psychotropic class before initiation, and the majority of youth with use of other psychotropic medications were single-class users. Only 24% had a psychiatric hospitalization in the year preceding the index antipsychotic prescription, and temporality of the hospitalization to antipsychotic initiation varied across psychotropic class subgroup. Compared with the other subgroups, youth with no prior psychotropic use were more likely to have a recent hospitalization preceding antipsychotic initiation. Additionally, youth with no prior psychotropic use who also had severe mental illness were more likely to be hospitalized when compared with other subgroups with the same psychiatric diagnosis.
Psychiatric hospitalization preceding antipsychotic initiation among youth with no prior psychotropic use may likely reflect a worsening of symptoms requiring hospitalization. Nearly all youth with no prior psychotropic use who were hospitalized were diagnosed with severe mental illness, namely bipolar disorder, which is an Food and Drug Administration (FDA)-approved indication for antipsychotic use in youth (Centers for Medicaid and Medicare Services 2013; McClellan et al. 2013; Daviss et al. 2016). For these youth, it is possible that initiation followed a first episode psychosis or mania requiring hospitalization and antipsychotic treatment, despite 64% previously having received psychotherapy. Antipsychotic prescribing is common in inpatient settings (Warner et al. 2007; Procyshyn et al. 2014), which corroborates our findings that 77% of youth with no prior psychotropic use had a hospitalization 30 days before the index antipsychotic prescription. The antipsychotic dispensing could reflect the first refill after discharge from the inpatient stay in which the antipsychotic was originally prescribed.
The majority (77%) of youth with no prior psychotropic use were not hospitalized before antipsychotic initiation. However, the psychiatric diagnostic profile of these youth reveal indications for treatment with over 50% diagnosed with a severe mental illness. The evidence for use of an antipsychotic among youth with no prior psychotropic use who were not diagnosed with severe mental illness is less clear. In this subgroup who were diagnosed predominantly with disruptive disorder, the use of an antipsychotic is not supported by medical evidence, and treatment guidelines recommend optimizing first-line medications and psychosocial interventions before initiating an antipsychotic (American Academy of Child and Adolescent Psychiatry 2011, 2015; Kealey et al. 2014). More than two-thirds of youth with no psychotropic use received psychotherapy before antipsychotic initiation. The antipsychotic may have been initiated to augment psychotherapy. Youth in foster care experience trauma and maltreatment (Greeson et al. 2011), which may underpin antipsychotic use. However, there is no FDA-approved medication for PTSD.
The study findings pertaining to single-class and concomitant psychotropic subgroups suggest that youth in these subgroups were less likely to have a hospitalization when compared with the psychotropic-naive subgroup. Intensive psychiatric service use did not appear to be a driver of antipsychotic initiation, even when controlling for a diagnosis of severe mental illness. It is possible that these youth exhausted a trial of other psychotropic medications and psychotherapy, and the antipsychotic was initiated as augmentation therapy. However, this hypothesis warrants further investigation. A large proportion of single-class and concomitant subgroups who had not experienced a psychiatric hospitalization before antipsychotic initiation had disruptive behavior disorders, predominantly ADHD. Antipsychotic augmentation of current stimulant medication for the management of aggression or delinquent behavior among youth with ADHD has been reported in the literature (Rodday et al. 2014; Mann et al. 2017), despite limited evidence to support such use (Pringsheim and Gorman 2012; Giles and Martini 2016). Antipsychotic augmentation may be necessary in treatment of refractory patients, after failure of a psychosocial or behavioral intervention, or other psychotropic medications (American Academy of Child and Adolescent Psychiatry 2011; Pappadopulos et al. 2011). It is possible that this was the case for these youth, particularly concomitant users in our study, as these youth received multiple psychotropic classes and more than 80% had received psychotherapy before antipsychotic initiation. Future research investigating the adequacy of the dose and duration of first-line psychotropic medications and the number of within-class drug trials before initiating an antipsychotic among these youth is needed. This information will be helpful to distinguish youth in which antipsychotic augmentation may be due to potential nonresponse to an adequate trial of a first-line medication.
In addition to the clinical implications of the study findings, we also examined foster placement stability, which is an important contextual factor relevant to youth in foster care. In this cohort, youth had on average 3 foster care placement changes in the year before antipsychotic initiation. These patterns are characteristic of foster care instability (Koh et al. 2014). Placement instability results in disruptions in the child's environment, treatment providers, and may increase the likelihood of behavioral problems (Rubin et al. 2007). Thus, maintaining stable foster placement could be a rationale for antipsychotic initiation as child behavioral problems and inpatient use often precipitate a foster care placement change (Park and Ryan 2009; Fawley-King and Snowden 2012; Cross et al. 2013). Instability resulting in changes in treatment providers also may disrupt the continuity of care provided to these youth, which is an important factor when considering antipsychotic initiation, or optimization of first-line psychotropic medications. Integrating psychotropic oversight and monitoring with family preservation initiatives within child welfare would broaden the perspective to factors that are contributing to the youth's disruptive behaviors and for which antipsychotics are prescribed.
Our findings should be interpreted in light of several limitations. Our study examined psychiatric diagnoses, psychiatric services, and psychotropic use in the 1-year preceding an index antipsychotic prescription, which may have overrepresented intensive service use. We did not examine the prior use of residential treatment or community- and family-level factors that may provide additional context for antipsychotic treatment. However, the present study provides a base from which to further explore the contextual factors associated with antipsychotic treatment. We did not have a method to determine if any of the psychotropic medications were prescribed for nonpsychiatric indications. For example, anticonvulsant medications may be prescribed for neurological indications (e.g., epilepsy, migraine treatment) and tricyclic antidepressants (TCAs) to manage physical symptoms. However, only 0.13% of youth in our study were diagnosed with epilepsy and youth prescribed TCAs represented only 0.8% of our sample. It is also possible that an antipsychotic could have been initiated during a hospitalization. However, administrative claims data limit our ability to identify medication prescribed in an inpatient setting. The generalizability of these results is limited to youth in foster care in one state who initiated an antipsychotic. Our results may not reflect patterns of care for youth in foster care in other states. Youth who had at least 12 months in foster care before the index antipsychotic may not generalize to youth who enter foster care already on an antipsychotic or are prescribed the antipsychotic soon after entry (i.e., more severe youth were not represented in the analysis). We did not have a nonfoster care comparison group of other Medicaid-enrolled youth. Further research to assess clinical variations among Medicaid-enrolled youth is warranted.
Conclusions
Our results suggest clinical variation among new antipsychotic users. The temporality of intensive psychiatric services and psychotropic treatment preceding antipsychotic initiation may differentiate subgroups of youth with different clinical needs. Psychiatric hospitalization, ED visits, and psychotropic medication use before antipsychotic initiation can inform individualized treatment planning for mental health care among foster care youth.
Clinical Significance
Psychiatric hospitalizations, ED visits, and psychotropic treatment preceding antipsychotic initiation can aid in assuring judicious use of antipsychotic medications among youth in foster care. Factors such as the temporality of previous hospitalizations and failure to respond to a trial of first-line psychotropic medications and psychotherapy are important clinical considerations when initiating an antipsychotic.
Footnotes
Disclosures
O'Mareen Spence is a recipient of a Maryland CERSI Scholar award from the FDA (Grant No. 1U01FD005946). FDA had no role in study design, data collection and analysis, decision to publish, or preparation of this article. Dr. Susan dosReis has received grant funding from the National Institute of Mental Health (NIMH) and the Patient Centered Outcomes Research Institute (PCORI), and the Pharmaceutical Research Manufacturers of America (PhRMA) Foundation. Dr. Wendy Camelo Castillo has no financial interests or potential conflicts of interest to report. Dr. Gloria Reeves has received grant funding from the NIMH and PCORI.
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.