
Abstract
Objective:
Irritability is common in pediatric autism spectrum disorder (ASD) patients. This can have major implications in child development, receptivity to behavioral therapy, as well as child and caregiver well-being. A systematic review and network meta-analysis were conducted to assess the efficacy and safety of atypical antipsychotics in treating irritability in these patients.
Methods:
Studies were identified from Medline, Embase, and PsycINFO from inception to March 2018. The clinical trials database was reviewed. Studies were included if they were a double-blind, randomized controlled trial utilizing the Aberrant Behavior Checklist Irritability (ABC-I) to measure the efficacy of atypical antipsychotic monotherapy. Data extraction was carried out following the Preferred Reporting Items for Systematic Reviews and Meta-analyses for network meta-analysis guidelines. The main outcome was the reduction in irritability score using the ABC-I subscale from baseline.
Results:
Eight trials comparing four interventions—risperidone, aripiprazole, lurasidone, and placebo in 878 patients, were included. Both risperidone and aripiprazole had significantly reduced ABC-I scores than placebo. Estimates of mean differences (95% credible intervals) were risperidone, −6.89 (−11.14, −2.54); aripiprazole, −6.62 (−10.88, −2.22); and lurasidone, −1.61 (−9.50, 6.23). Both risperidone and aripiprazole had similar safety. There were only eight studies included in the analysis, however, sample sizes were not small. Variance in reporting of adverse effects limited the quality of safety analysis.
Conclusion:
Risperidone and aripiprazole were the two best drugs, with comparable efficacy and safety in pediatric ASD patients. These two medications could be beneficial in improving irritability in these patients.
Introduction
Autism Spectrum Disorder (ASD) is a neurodevelopmental disorder characterized by deficits in communication and social skills, repetitive stereotyped behaviors, as well as cognitive impairment. The Centers for Disease Control estimates that ∼1 in 59 children have been diagnosed with this disorder in the United States, with incidences occurring in all socioeconomic, ethnic, and racial groups (Baio et al. 2018). A systematic review of ASD studies estimates a prevalence of 20 per 10,000 (95% confidence interval [CI]: 4.9–82.1) (Williams et al. 2006). Both phenotypic presentation and symptom severity are highly heterogeneous. Phenotypic variability reflects a significant range of core ASD symptom severity, as well as the extent of functional impairment and developmental and psychiatric comorbidities present.
Although not ubiquitous, symptoms commonly found under the autism spectrum relate to irritable, aggressive, and self-harming behaviors manifested as aggression toward property, others, or themselves. Moderate to severe irritability alone is found in ∼20% of ASD patients (Lecavalier 2006). Irritability can impede quality of life, familial and community interactions, the implementation of interventional therapies, as well as long-term outcomes (Samson et al. 2014; Fung et al. 2016).
The Aberrant Behavior Checklist Irritability (ABC-I) subscale is a 15-item subscale to assess self-injurious behaviors, aggression, as well as temper tantrums in pediatric ASD patients (Aman et al. 1985). In 2014, Kaat et al. reported that this scale has acceptable to excellent internal consistency, and changes to evaluation are a good marker to indicate medication efficacy.
Antipsychotic medications, both typical (first generation) and atypical (second generation), have shown some efficacy in treating these symptoms in children with ASD (Posey et al. 2008). A database analysis of 2853 pediatric ASD patients found that 27% of pediatric ASD patients were receiving at least one psychotropic medication (Coury et al. 2012).
Second-generation antipsychotics (SGAs), in particular, are a widely studied and prescribed intervention in the treatment of irritable symptoms in patients with ASD (Accordino et al. 2016). Downs et al. (2016) reported the use of antipsychotic medications in 10% of ASD children referred to the South London and Maudsley NHS Foundation Trust, with risperidone and aripiprazole comprising 55% and 32% of the interventions used, respectively. Self-injurious behavior, aggression, reduced adaptive function, and parental concerns were found to be significantly related to the use of antipsychotics in these children (Downs et al. 2016).
Other SGAs have not been investigated thoroughly, with focus being on open-label studies. Open-label studies of ziprasidone have yielded more promising results, although available data are limited (Accordino et al. 2016).
SGAs have been associated with a decreased risk of development of extrapyramidal symptoms (EPS), but an increased risk of weight gain compared with typical antipsychotics (Taylor and McAskill 2000; Pierre 2005). This leads to increased risk of more serious chronic conditions, such as cardiovascular disease or diabetes, with the potential onset of obesity in these patients (Meltzer 2005; Gentile 2006). A systematic review found that risk of abnormal lipids, increased body mass index (BMI), and weight gain were highest in patients receiving olanzapine, followed by clozapine and quetiapine. Risperidone, aripiprazole, and olanzapine were associated with the highest risk of neurological side effects (Pringsheim et al. 2011). Yoon et al. (2016) recently reported a significant increase in BMI in patients taking olanzapine compared with those receiving risperidone, aripiprazole, quetiapine, or ziprasidone.
Risperidone has been shown to reduce irritability in adults with ASD and is well tolerated with mild transient sedation but with no reported EPS (McDougle et al. 1998). Similar results have been shown in trials with other SGAs (Posey et al. 2008). A double-blinded study of risperidone, in children ages 5–17, demonstrated no apparent detrimental impairment of cognitive or academic ability in doses up to 3.5 mg for 8 weeks (Aman et al. 2008).
Fung et al.'s (2016) recent meta-analyses on a broad range of interventions and in their review identified two SGAs as the most efficacious treatment in the analysis. We aim to compare SGAs for their treatment of irritability in pediatric ASDs, using a network meta-analysis (NMA). The NMA methodology has significantly extended the classical pairwise meta-analysis approach. The methodology allows synthesis of evidence involving three or more interventions, as well as combining direct and indirect evidence. These two types of evidence (direct and indirect) are used to rank treatments based on efficacy or harm. A detailed description of NMA concepts, methods, and implementation can be found in a two-part series published by the International Society for Pharmacoeconomics and Outcomes Research Task Force (Hoaglin et al. 2011; Jansen et al. 2011).
This analysis strategy has not been used before to compare antipsychotic drugs on irritability in this population. We also summarize the evidence of rates of reported side effects associated with the different drugs.
Methods
Study eligibility
Studies were included if they were a double-blinded, randomized controlled trial (RCT) of an atypical antipsychotic medication for the treatment of irritability in pediatric ASD patients, and published in English. Articles were excluded from analysis if the trial was not a monotherapy, if the outcome measure was not comparable, or if the outcome scale was not the ABC-I. Ichikawa et al. (2017) utilized the ABC-J scale (Japanese translation), which was included, as they reported equivalent reliability and validity compared with the original ABC scale (Aman et al. 1985; Ichikawa et al. 2017). Risk of bias was conducted using the Cochrane risk of bias tool (modified) for quality assessment of randomized controlled trials.
Search strategy
Medline, PsycINFO, and Embase were searched from inception (Medline: 1946, Embase: 1974, PsycINFO: 1806) until March 2018. The clinical trials database was searched for prepublication trials. Three categories were utilized in the search strategy, for English-only articles, which included comprehensive language for ASDs, irritability and aggression, as well as antipsychotic medications. The complete search strategy used is provided in the Appendix.
Data extraction
Two reviewers assessed the eligibility of all studies. Any discrepancies were resolved by consensus and, if necessary, by involving a third reviewer. Data extraction was completed independently and in duplicate. Extracted data included treatment group size, dose size and duration, ABC-I scores (baseline, change, and final were available), concurrent medications, rates of adverse events, and patient dropout rates.
Statistical methods
The effects of multiple interventions were compared by estimating mean differences (MDs) on the change score between final and baseline scores on irritability measured by the ABC-I scale or its adaptive (translated) version. Whenever a trial did not report data on mean change score, we calculated mean change score in each intervention arm as the mean final score minus mean baseline score. For a trial not reporting standard deviation (SD) of the change score, it was computed as
In a trial comparing different doses of the same pharmaceutical drug, one single arm was created for the drug, where the mean and SD change score for the arm were calculated as the weighted average of mean change score and SD change score, respectively (weights being the respective treatment arm sizes), and the arm size was the sum of arm sizes receiving different doses of the drug.
Bayesian NMA with consistency assumption (i.e., statistically similar direct and indirect evidence when both are available) was carried out using the Markov chain Monte Carlo to compare the effects of multiple competing treatments. The convergence of the chains to the posterior distribution was assessed using the Brooks/Gelman/Rubin diagnostic test as well as trace and time-series plots (Brooks and Gelman 1998). As the mean change score was continuous, normal likelihood was used (Dias et al. 2013). We used a random-effect model for the NMA to account for potential heterogeneity in the data. In the Bayesian analysis, vague priors were used for effect parameters. Goodness-of-fit was assessed using the mean residual deviance. Consistency between direct and indirect evidence was assessed using the node-split method (Dias et al. 2010). The Bayesian NMA was conducted using the R package gemtc (version 0.7).
For each of the possible treatment contrasts, the MD and the corresponding 95% credibility interval (CrI), the Bayesian analog of the confidence interval was reported. Since a higher ABC-I score represents worse irritability and the change score was defined as the final minus baseline score, a treatment is considered more efficacious than another treatment if the corresponding estimate of MD on the change score is negative and the CrI does not include zero. For each treatment, we also computed the surface under the cumulative ranking curve (SUCRA) to rank the competing treatments. SUCRA for a treatment ranges between 0 and 1, where the treatment with the highest SUCRA value is considered the most efficacious treatment (Salanti et al. 2011).
For each binary adverse outcome for every pair of treatment comparison, we simply computed the odds ratio and corresponding p-value from the 2 × 2 table when only one trial was available for the comparison. When two or more trials were available for an adverse outcome, the Mantel/Haenszel method was used for the meta-analysis. If any cell in the 2 × 2 table had zero event in a trial, corrections were made by adding 0.5 in each cell before analyzing the data.
Results
Among 2131 articles screened, 294 underwent full-text review. Of these, 14 met the eligibility criteria for qualitative analysis or the Bayesian NMA. The flow chart for the selection of trials for this review is provided in Figure 1.
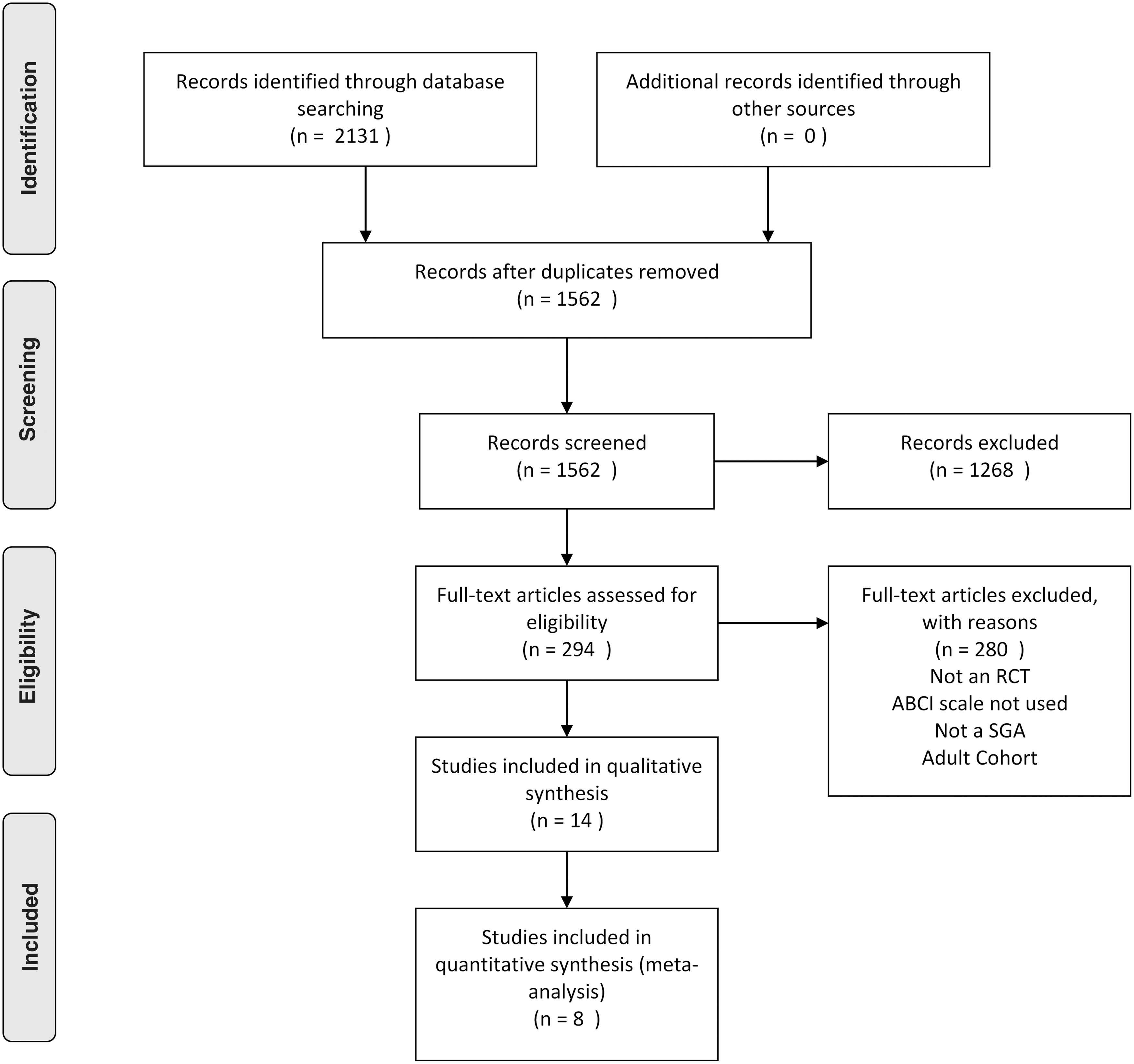
Study selection flow chart. A flow chart demonstrating the selection process of articles included in the analysis as well as in the qualitative summary.
NMA on irritability
Among 14 studies, 8 compared 4 treatments for irritability in ASD patients and were included in the Bayesian NMA. Figure 2 presents the network graph. Five trials were conducted in the United States (McCracken et al. 2002; Marcus et al. 2009; Owen et al. 2009; Kent et al. 2013; Loebel et al. 2016), one in Canada (Shea et al. 2004), one in Japan (Ichikawa et al. 2017), and one in Iran (Ghanizadeh et al. 2014). These trials encompassed 4 interventions and 878 randomized patients.
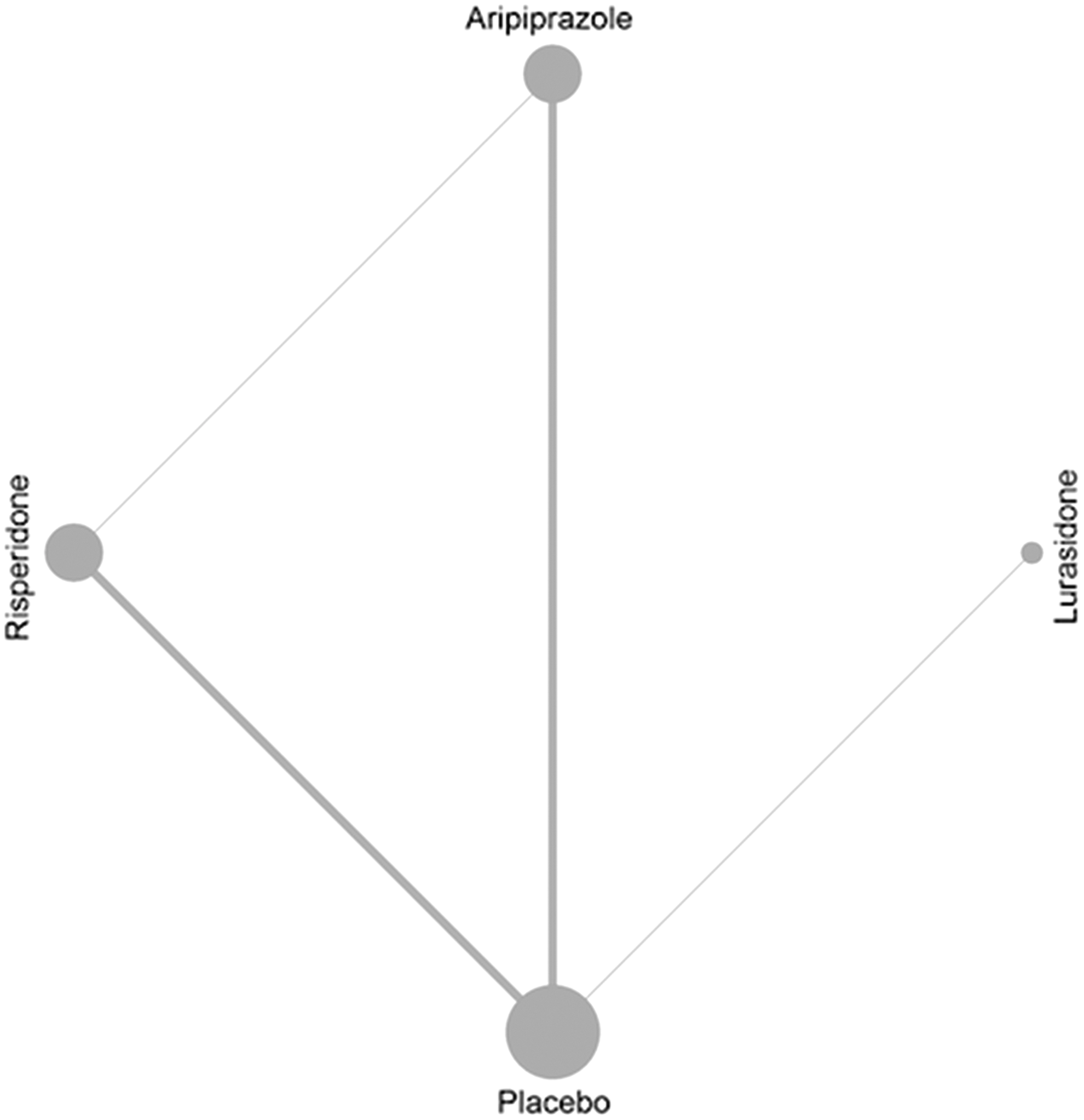
Network plot. A network graph is presented, where the number of trials in which any two treatments were compared head to head is displayed along the gray line (edge) connecting those two treatments. The radius of a node (vertex) is proportional to the number of patients assigned to the corresponding treatment in the entire network of all trials; therefore, a larger node size means a larger total number of patients were randomized to that treatment.
Seven trials used the ABC-I scale to assess the outcome of irritability, and Ichikawa et al. (2017) utilized the Japanese translation of the ABC-I. Three trials compared aripiprazole with placebo (Marcus et al. 2009; Owen et al. 2009; Ichikawa et al. 2017), three compared risperidone with placebo (McCracken et al. 2002; Shea et al. 2004; Kent et al. 2013), one compared lurasidone with placebo (Loebel et al. 2016), and one trial compared aripiprazole with risperidone (Ghanizadeh et al. 2014); whereas lurasidone was never compared with aripiprazole or risperidone (Fig. 2). Three studies were multiarm trials, where different doses of the same drugs were compared against placebo (Marcus et al. 2009; Kent et al. 2013; Loebel et al. 2016).
Risk of bias analyses, shown in Table 1, indicated no significant concerns of bias.
Risk of Bias Assessment
Assessment conducted using the Cochrane risk of bias tool (modified) for quality assessment of randomized controlled trials.
L, low; H, high; U, unclear.
When assessed using node-split method (Dias et al. 2010), there was no evidence (p-values ≥0.40) of inconsistency (i.e., incoherence) between direct and indirect evidence in the network.
Table 2 summarizes efficacy results from our NMA, and Figure 3 illustrates a density plot of the relative effects of the treatments against placebo. Lurasidone was not significantly different, with the estimate of MD in the change from baseline score of ABC-I −1.61 (95% CrI: −9.50, 6.23) compared with placebo. The estimate of MD for aripiprazole was −6.62 (95% CrI: −10.88, −2.22) and for risperidone was −6.89 (95% CrI: −11.14, −2.54), suggesting that both the drugs were significantly better than placebo in reducing the ABC-I score. Both drugs had a very similar effect when compared with each other. The SUCRAs for risperidone and aripiprazole were 82% and 78%, respectively (Fig. 4), suggesting that risperidone may be slightly better in terms of efficacy.
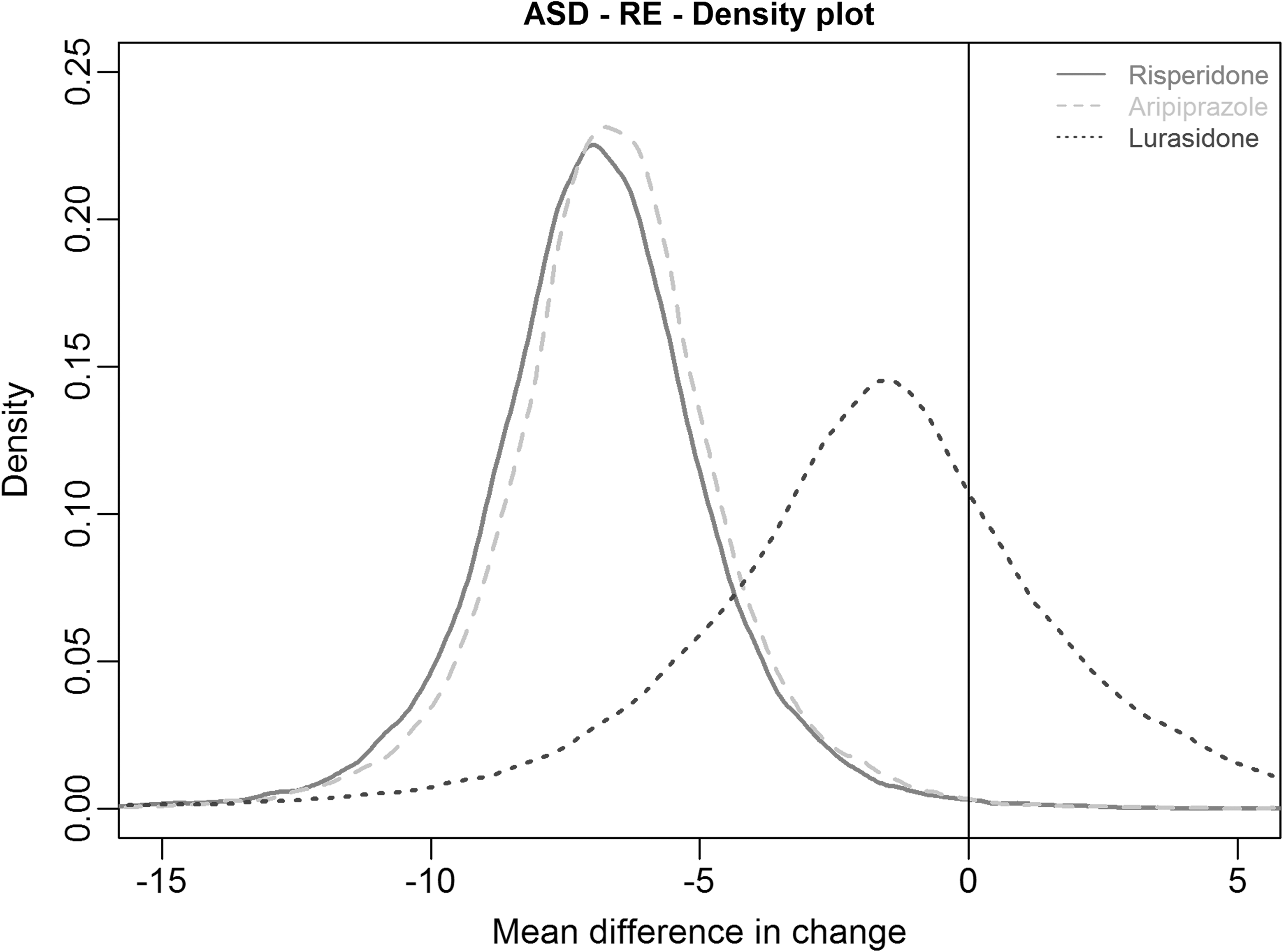
Density plot. A density plot showing the estimated densities for relative treatment comparisons between each treatment and placebo.
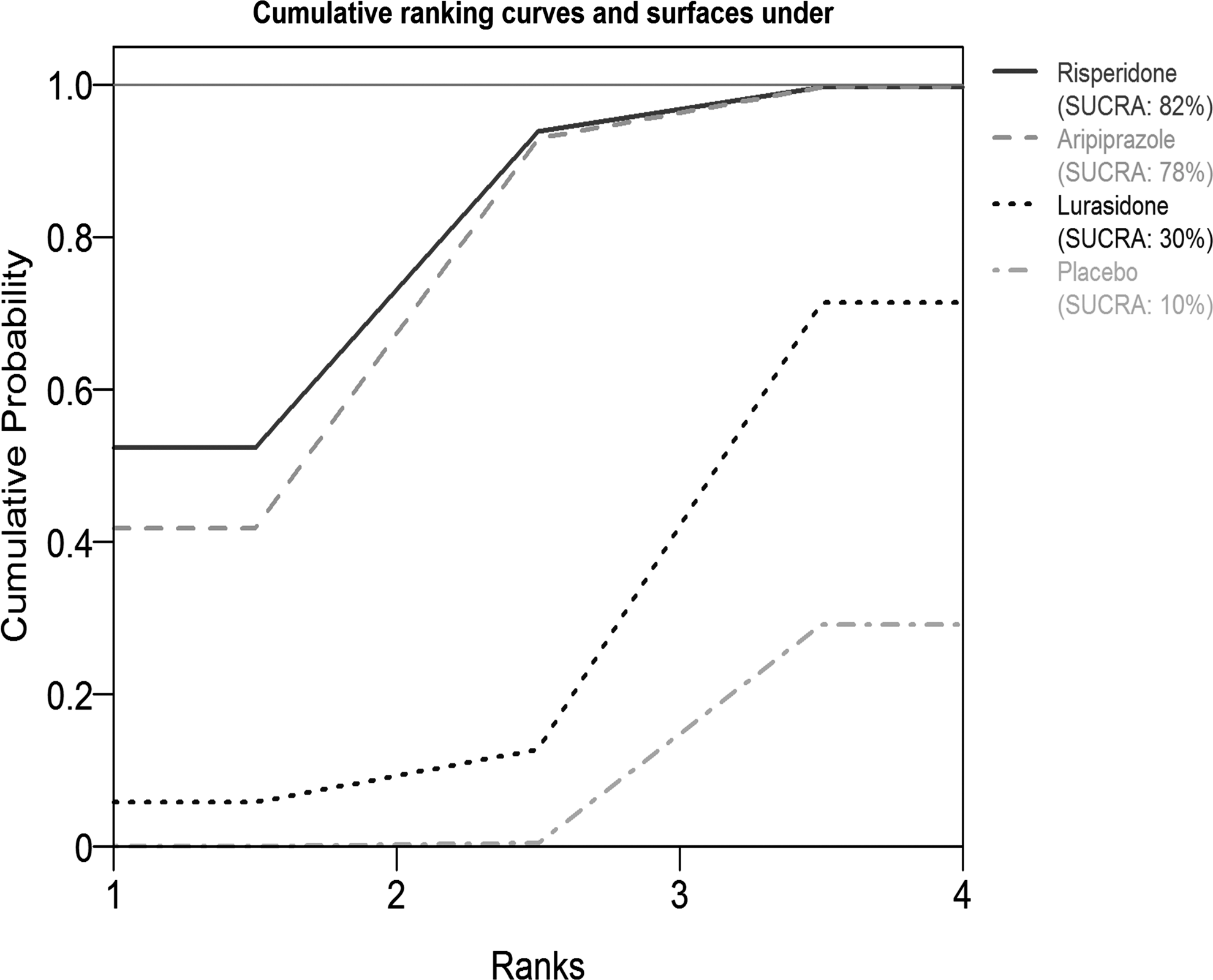
Cumulative rank probability plot. This plot shows the relative cumulative probabilities for each of the treatments in the network. SUCRA values are presented in the legend. SUCRA, surface under cumulative ranking curve.
Estimates of Mean Difference and Corresponding 95% Credible Intervals for All Possible Treatment Effects
The estimates of mean difference of treatments in the columns versus rows presented in the lower diagonal elements (while those of the row treatments vs. column treatments are presented in the upper diagonal elements).
ASD, autism spectrum disorder; RE, random effect.
Results were similar in a sensitivity analysis after removing the low-dose arm given in a study by Kent et al. (2013). The random-effect model for NMA was a good fit to the data of 16 treatment arms from eight studies, with a mean residual deviance of 16.21.
Pairwise meta-analysis of adverse events
Table 3 summarizes our meta-analysis of adverse events. Meta-analysis of adverse events demonstrated risperidone, aripiprazole, and lurasidone having comparable safety. No odds ratio between drugs was significant for any adverse event, although significant odds ratios were calculated in some studies involving all three SGAs against placebo. These events include constipation, decreased appetite, dizziness, drooling, fatigue, increased appetite, nasopharyngitis, pyrexia, rhinitis, sedation, somnolence, tachycardia, and vomiting. A p-value of <0.1 was used to determine significance in this instance. Although none of the SGAs had a significant p-value regarding weight increase, the inconsistent reporting and method of measurement between studies made a more accurate analysis of these events unfeasible.
Meta-Analysis of Adverse Event Frequencies
OR, odds ratio; CI, confidence interval; URTI, upper respiratory tract infection.
Discussion
Irritability is a common finding in pediatric ASD patients and is a key influence on school success, family and caregiver strain, and child well-being (Brereton et al. 2006; Mayes et al. 2011). Behavioral interventions to treat antecedents, alter environments, and support parents in management of impulsivity and aggression are preferred, but in highly aggressive or persistently irritable youth, medications are often important interventions (McPheeters et al. 2011).
The findings of this NMA demonstrate a significant efficacy in treating irritability in pediatric ASD patients using SGAs. Both risperidone and aripiprazole demonstrated significantly larger mean change scores in comparison with placebo, but interestingly not from one another. Both medications appear to be generally well tolerated. Such comparable tolerability and efficacy results provide clinicians with two interventions that could be clinically useful. Deciding which medication to implement is therefore based in clinical judgment, with a change in drug regimen a readily available option.
Although other SGAs have shown some promise in open-label trials, higher quality data are necessary for more conclusive comparisons between both placebo and other available SGAs. Both risperidone and aripiprazole demonstrate as the most efficacious SGAs for the treatment of irritability in pediatric ASD patients. Fung et al. (2016) recently reviewed pharmacological interventions for irritability and aggression in this population, including both risperidone and aripiprazole. Our results are consistent with their findings and demonstrate the comparable efficacies between these two medications, now using direct and indirect head to head comparisons of estimated MDs.
Two long-term studies have demonstrated risperidone's continued efficacy and tolerability over 6 months (RUPP 2005; Troost et al. 2005). Adverse events during these trials were mostly deemed not clinically significant with many not attributed to risperidone itself. There were no instances of dyskinesia during either the 6 months of treatment or the withdrawal period. High relapse rates after risperidone discontinuation were observed, with no predicting factors identified. These relapse cases post-treatment discontinuation were notable for a rapid reappearance of aggressive symptoms. Instances of weight gain during treatment were significant, and could be cause for concern regarding diabetes and other weight-associated conditions (RUPP 2005; Troost et al. 2005).
Risperidone treatment has also been associated with increased serum prolactin levels in these patients, the long-term effects of which are still unknown, making long-term studies to address the risk/benefit ratio regarding these events important (RUPP 2005; Anderson et al. 2007).
In 2012, Ishitobi et al. conducted a study assessing a transition to aripiprazole treatment in patients experiencing tolerability issues with risperidone. Outcome scores remained relatively stable, while patients experienced some improvements with regard to adverse events (Ishitobi et al. 2012). These findings suggest that replacing risperidone with aripiprazole could be beneficial in patients experiencing tolerability problems, as aripiprazole appears to maintain the efficacy of risperidone treatment (Ishitobi et al. 2012).
Findling et al. (2014) conducted a double-blinded, placebo-controlled investigation of the long-term efficacy of aripiprazole and found decreased risk of relapse with continued use, compared with placebo. Ichikawa et al. (2017) conducted an open-label extension of their trial included in this NMA (Ichikawa et al. 2018). Eighty-one percent of patients completed assessments at 48 weeks, with a mean treatment duration of 694.9 days. The authors concluded that aripiprazole was not only effective in the long-term management of irritability in pediatric ASD patients, but that it was typically safe and well tolerated (Ichikawa et al. 2018). A recent, 2-year naturalistic study compared long-term efficacies of these two SGAs and found that most discontinuations occurred in the first 6 months, and that the rates of discontinuation were similar between them at 24 months (Pozzi et al. 2016).
The limitations of this study largely involve the amount of data available for analysis. Only eight relevant RCTs were discovered using our search strategy, limiting the power of the analysis. However, the sample sizes were not small, and outcomes were measured using the same scale, improving the quality of the NMA. As well, the lurasidone treatment group was represented only by a single study, leading to greater uncertainty in the estimated mean effects between the other analyzed SGAs. There were only two studies with missing SDs for the change score and we assumed a moderate correlation of 0.6. Meta-analysis of change scores is known to be challenging in practice and one of the challenges is missing SD for change scores. Imputing the missing correlation is one of the strategies used, and that is what we adopted here.
The variance in reporting of adverse events, such as weight gain, severely limited the ability for higher quality analysis between studies. There was a sparsity of data per adverse outcome that could be analyzed, as demonstrated by wider confidence intervals. Although statistical power is increased using the meta-analysis approach, caution must be used in the interpretation of these findings. Given the small number of studies available, a detailed exploration into publication bias was not possible, although a risk of publication bias in this body of literature may exist.
More investigation is needed involving both SGAs, and other medications, in treating irritability in pediatric ASD patients. Other SGAs may be helpful in treating irritability in these patients, as described in several open-label studies. However, there is a need for RCTs investigating both their efficacy and safety, to more accurately compare them and make the most informed clinical decisions involving patient treatment. Finally, there is a dearth of literature on long-term treatment effects and tolerability. More evidence of the long-term SGA safety, efficacy, and risk of relapse would be useful for clinicians to incorporate when evaluating treatment options.
Conclusion
In conclusion, risperidone and aripiprazole are both effective treatments of irritability in pediatric patients with ASD. The data indicate comparable efficacies and safety using either risperidone or aripiprazole, and as Ishitobi et al. (2012) indicate, transitioning interventions seem a viable option if issues such as tolerability arise. Treatment goals are another important factor in decision-making regarding these interventions. Decreasing irritability in these patients could not only provide some relief in terms of stress and potential harm but could possibly allow patients to be more receptive to behavioral interventions as well, providing further relief of other core ASD symptoms. More studies are needed to assess a much wider group of medications, which could be clinically useful, as well as to determine long-term treatment effects.
Clinical Significance
This study examined available clinical data to assess the efficacy and safety of atypical antipsychotics for the treatment of irritability in pediatric patients with ASD. Irritability is a common finding in this population, and may be amenable to medical treatment. Atypical antipsychotics are frequently used for this indication, but there is a sparsity of data comparing interventions against each other. This network meta-analysis is the first to summarize direct and indirect evidence of medication effects in this population. Adverse effects were also summarized in a meta-analysis. The available data support the use of risperidone and aripiprazole for the treatment of irritability in pediatric ASD patients, with both demonstrating similar efficacy and safety.
Footnotes
Disclosures
M.S.F., M.R.S., B.N., D.R., and T.A.B.—have no disclosures to declare. J.B. holds the John D. Cameron Endowed Chair in the Genetic Determinants of Chronic Diseases, McMaster University. J.B. also acknowledges funding from the Province of Ontario Neurodevelopmental Disorders (POND) Network, through the Ontario Brain Institute (OBI); Kids Brain Health Network; the Natural Sciences and Engineering Research Council of Canada (NSERC); and the Canadian Institutes of Health Research (CIHR).
Appendix
Qualitative Summary of Efficacy and Safety of Other Second-Generation Antipsychotics
This section contains summarized results from trials of second-generation antipsychotics not included in this network meta-analysis. Randomized controlled trials (RCTs) often fail to replicate the effect sizes reported in open-label studies, and the methodological nature of open-label studies makes them inferior to randomized and blinded trials. Insufficient information is available for these interventions, due to the absence of blinding and randomization, as well as small cohort sizes. The use of unstandardized outcome assessment scales, such as the clinical global impression (CGI), is another limitation in these studies.