
Abstract
Objectives:
To characterize reported adverse drug reactions (ADRs) in children and adolescents treated with antipsychotics and determine differences in relative reporting frequency between genders, age classes, and reporter types.
Methods:
Individual case safety reports of children ages 1 − 17 years in whom an antipsychotic drug was the suspected or interacting drug from the worldwide database, VigiBase, from 1968 until March 2017, were included. Reported ADRs were categorized based on the Standardized Medical Dictionary for Regulatory Activities (MedDRA) Queries and clinical reasoning. Proportional reporting ratios (PRRs) and 95% confidence intervals (95% CIs) were calculated for genders, age classes, and reporter types.
Results:
In total, 45,201 reported ADRs were included. The most frequently reported were ADRs related to extrapyramidal syndrome (14.7%), breast disorders or blood prolactin level changes (4.7%), and cardiac arrhythmias (4.6%). Differences in relative reporting frequencies were observed between age classes and reporter types, and less prominent between genders. For example, ADRs related to hyperglycemia/new-onset diabetes mellitus were less frequently reported in children ages 1 − 5 than in children ages 12 − 17 (PRR: 0.4, 95% CI: 0.2 − 0.5). ADRs related to cardiac arrhythmias were less frequently reported by consumers compared with health care professionals (PRR: 0.5, 95% CI: 0.5 − 0.6), whereas ADRs related to a change in weight/body mass index were more frequently reported by consumers (PRR: 3.2, 95% CI: 2.9 − 3.5).
Conclusion:
A wide spectrum of ADRs were reported in children treated with antipsychotics. The relative differences in reporting frequency between age classes and reporter types can be of help to tailor information about possible ADRs and to monitor for ADRs.
Introduction
Antipsychotics are frequently prescribed to children and adolescents (hereafter referred to as children) to treat psychiatric disorders, including disruptive behavior disorder, autism spectrum disorder, and attention-deficit/hyperactivity disorder (Olfson et al. 2015; Edelsohn et al. 2017). Despite the frequent use in this young population, the evidence for the efficacy and safety of antipsychotic treatment in children is scarce and off-label prescribing is common (Sohn et al. 2016). This is of concern because of the seriousness of adverse effects, the lack of knowledge of long-term effects, and the vulnerability of this population.
Effects of antipsychotics have mostly been studied in adults (Leucht et al. 2013). However, the efficacy and safety outcomes of studies in adults cannot easily be extrapolated to children (Kearns et al. 2003; Gerlach et al. 2016; Mooij et al. 2016; Adeli et al. 2018). Developmental changes in children concerning gastrointestinal function, metabolic capacity, and renal function, and the inter- and intraindividual variability in pharmacokinetics require individualized dosing of antipsychotics (Kearns et al. 2003). In addition, effects of antipsychotics in children can differ from those in adults. For example, children treated with antipsychotics have a greater risk of weight gain and somnolence compared with adults (Correll et al. 2010; Kryzhanovskaya et al. 2012). Also, the perceived severity of adverse drug reactions (ADRs) in children may differ from that in adults. For example, hyperprolactinemia may be more distressing to adolescents because it can cause a delay in pubertal maturation, menstrual disturbances, gynecomastia, and sexual dysfunction (Kinsella et al. 2012). In this study, not only age but also gender may play a role, as adolescent females treated with antipsychotics may be more prone to experience greater changes in prolactin levels than males (Roke et al. 2009; Balijepalli et al. 2018).
Although studies have looked into specific ADRs in children, an overview of the (reported) occurrence frequencies of ADRs in children treated with antipsychotics is missing. Reporting systems of ADRs are a valuable source by which to obtain such an overview and to gain knowledge on the safety of antipsychotic drug use in children. Most countries have a national reporting system in which both health care professionals and patients report suspected ADRs, which are subsequently collected in the World Health Organization's (WHO) global database of individual case safety reports (ICSRs), VigiBase (Lindquist 2008). It is unknown which ADRs are reported in children treated with antipsychotics and also who reports these ADRs.
The aim of this study was to characterize reported ADRs in children treated with antipsychotics and determine differences in relative reporting frequency between genders, age classes, and reporter types.
Methods
Setting
This study was conducted using data from VigiBase, the WHO global ICSR database (Lindquist 2008). In the aftermath of the thalidomide disaster in the early 1960s, the WHO Programme for International Drug Monitoring was established in 1968. In each country participating in this program, a national center for pharmacovigilance collects and manages spontaneous reports of suspected ADRs, for instance, by health care professionals or patients themselves. These ICSRs are sent to the Uppsala Monitoring Centre (UMC)—the WHO Collaborating Centre for International Drug Monitoring—in Sweden, which maintains the reports in VigiBase. Information available in the ICSRs includes patient demographics, suspected drugs, reported ADRs, and additional information relevant to the case (Lindquist 2008). Reported ADRs are coded at the originating national center, either according to the WHO Adverse Reaction Terminology (WHO-ART) or the Medical Dictionary for Regulatory Activities (MedDRA) (Lindquist 2008). VigiBase uses both WHO-ART and MedDRA; for this study MedDRA was used. Suspected drugs recorded on the ICSRs are coded according to the WHO Drug Dictionary (Lindquist 2008). In 2017, VigiBase contained more than 16 million ICSRs, originating from more than 120 member countries (Uppsala Monitoring Centre [UMC] 2017a, 2017b).
Selection of ADRs
Included in this study were all ICSRs that were notified since the establishment of VigiBase in 1968 until March 2017 concerning children ages 1 − 17 years, in whom an antipsychotic (ATC code N05A, excluding lithium [N05AN01]) was the suspected or interacting drug (Fig. 1).
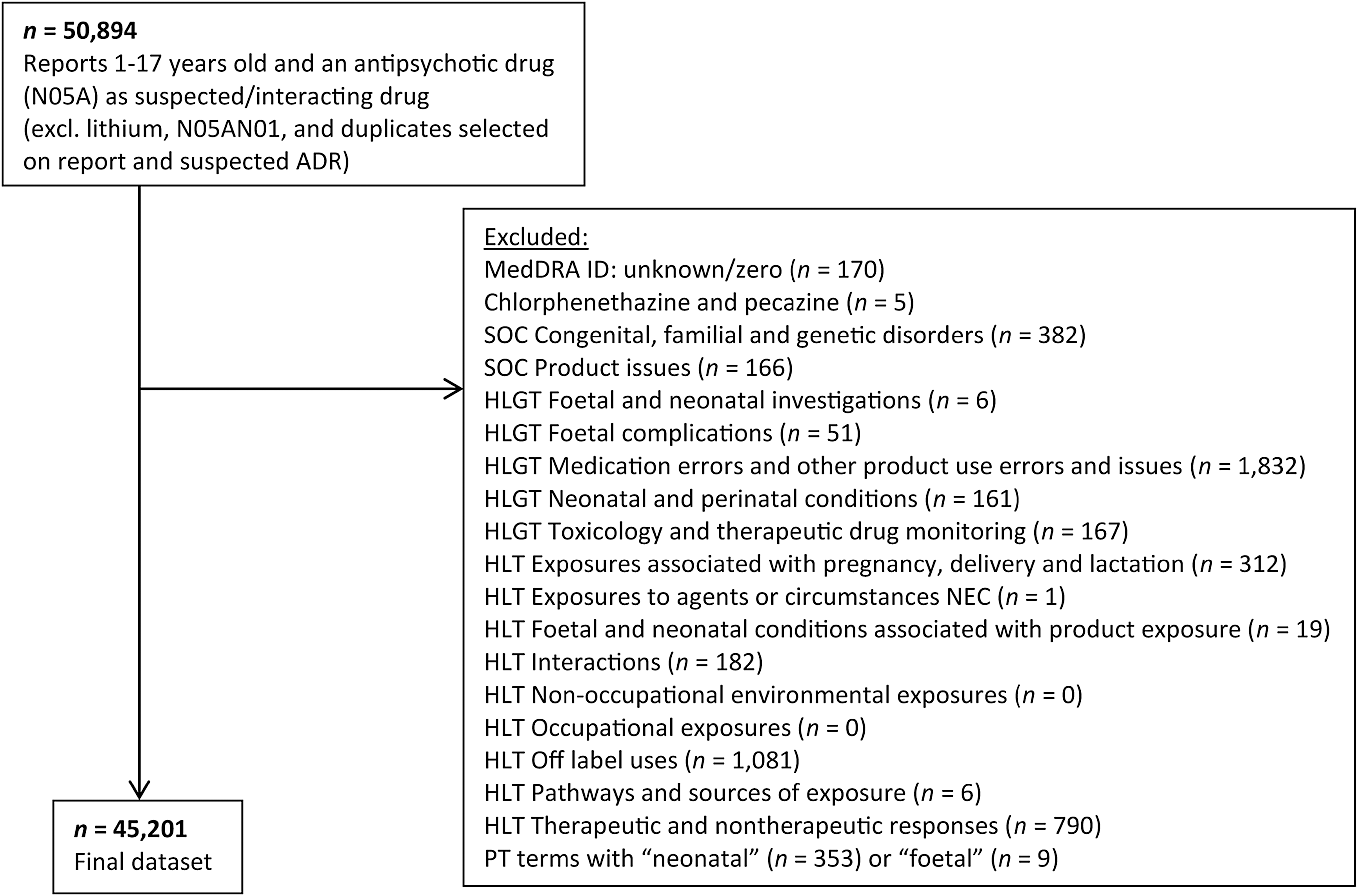
Flowchart of the process of selection of ADRs. ADR, adverse drug reaction; HLGT, high-level group term; HLT, high-level term; MedDRA, Medical Dictionary for Regulatory Activities; n, number of reported adverse drug reactions; PT, preferred term; SOC, system organ class.
Children ages <1 year and the MedDRA terms, including “neonatal” or “foetal,” were excluded, as the reported ADR in such cases was probably related to the use of an antipsychotic by the mother and not by the child itself. As not all reported MedDRA terms were ADRs, the terms in Figure 1 were excluded. Each MedDRA term has a unique MedDRA code; ICSRs without a valid MedDRA code and duplicate MedDRA codes in one ICSR were excluded.
Classification of ADRs
The unit of analysis was the reported ADR (MedDRA code). Reported ADRs were categorized according to system organ classes (SOCs) and subsequently based on Standardized MedDRA Queries (SMQs) and clinical reasoning.
The MedDRA hierarchy was used to evaluate the reported ADRs in the ICSRs. The MedDRA hierarchy consists of five levels: lowest level terms (LLTs), preferred terms (PTs), high-level terms (HLTs), high-level group terms (HLGTs), and SOCs. All reported MedDRA terms were either PTs or LLTs. Both PTs and LLTs can be linked to more than one SOC, but there is always a primary SOC. The primary SOC is the prime manifestation site if the PT or LLT relates to a disease or symptom (International Federation of Pharmaceutical Manufacturers and Associations [IFPMA] 2017a). For this study, only the primary SOCs were used (Supplementary Table S1 and Supplementary Fig. S1).
Different ADRs can be reported for the same disease or symptom. These ADRs were combined into one group based on SMQs and clinical reasoning. SMQs are validated groups of MedDRA terms that relate to the same medical condition or area of interest (International Federation of Pharmaceutical Manufacturers and Associations [IFPMA] 2017a). For the SMQs, narrow scope terms were used, but if in our opinion the broad scope terms comprised crucial ADRs that needed to be included in this study, these were used. The narrow scope terms are more specific, whereas the broad scope terms are more sensitive and include narrow terms and terms of less specific nature (International Federation of Pharmaceutical Manufacturers and Associations [IFPMA] 2017b). Reported terms can contribute to more than one SMQ; for instance, oculogyric crisis was attributed to the SMQs: extrapyramidal syndrome and ocular motility disorders. Due to this overlap, the numbers of reported ADRs (or MedDRA terms) in different SMQs cannot be combined to calculate the total number of reported ADRs (Table 1 and Fig. 2). If no SMQ was available for terms related to the same medical condition, HLGTs, HLTs, and PTs were included based on clinical reasoning. The final overview was discussed and resolved by consensus with two additional authors (T.C.G.E., E.R.H.).

Most reported ADRs stratified by reporter type and categorized by SMQs and clinical reasoning. Reported ADRs categorized by SMQs (MedDRA) and clinical reasoning (see Table 1 for details). Reference category: health care professionals. Bold denotes significant difference. MedDRA, Medical Dictionary for Regulatory Activities; n, number of reported adverse drug reactions; NEC, not elsewhere classified; PRR (95% CI), proportional reporting ratio (95% confidence interval); SMQs, Standardized MedDRA Queries.
Most Reported Adverse Drug Reactions Categorized by Standardized Medical Dictionary for Regulatory Activities Queries and Clinical Reasoning
Bold values indicate significant difference.
SMQ broad terms (MedDRA).
High-level term.
SMQ narrow terms.
High-level group term.
PT: blood prolactin, blood prolactin abnormal, blood prolactin decreased, blood prolactin increased, hyperprolactinemia, hyperprolactinemia.
PT: abnormal loss of weight, abnormal weight gain, body mass index increased, obesity, overweight, underweight, weight, weight abnormal, weight decreased, weight fluctuation, weight gain poor, weight increased.
PT: body temperature decreased, body temperature fluctuation, body temperature increased.
PT: breath sounds abnormal, respiratory rate decreased, respiratory rate increased.
MedDRA, Medical Dictionary for Regulatory Activities; n, number of reported adverse drug reactions; NEC, not elsewhere classified; PRR (95% CI), proportional reporting ratio (95% confidence interval); PT, preferred term; SMQ, Standardized MedDRA Query.
Data analysis
Descriptive statistics were used to obtain an overview of the most frequently reported ADRs. Data were stratified by gender, age and reporter type. Age was stratified into three age classes: 1 − 5, 6 − 11, and 12 − 17 years old. Reporter types were stratified into health care professionals and consumers. The former included the reporter types “physician,” “pharmacist,” “other health professional,” “general practitioner,” “specialist physician,” “dentist,” “nurse,” and “hospital,” while the latter included the reporter types “consumer/nonhealth professional” and “other.”
The relative reporting frequencies were calculated and expressed as a percentage of the total reported ADRs and of the total reported ADRs in males, females, consumers, health care professionals, or age classes. The ratios of the reported ADRs for males versus females, consumers versus health care professionals, and between age classes were expressed as proportional reporting ratios (PRRs) and 95% confidence intervals (95% CIs). The PRR was based on a two-by-two contingency table:
where a and c denote the reported ADRs among males and females, respectively, among consumers and health care professionals, respectively, or among age classes; (a + b) and (c + d) denote the total reported ADRs among males and females, respectively, among consumers and health care professionals, respectively, or among age classes.
All statistical analyses were performed using SPSS Statistics version 24.
Results
In this study, 18,950 unique ICSRs containing 45,201 reported ADRs were included of children ages 1 − 17 years with an antipsychotic drug as the suspected or interacting drug (Fig. 1). There was an average of 2.4 reported ADRs per ICSR. In total, 61 different (generic) antipsychotic drugs were included in the ICSRs, through which 1 ICSR could include more than 1 antipsychotic drug. The most frequently reported suspected antipsychotic drug was risperidone (n = 5321 ICSRs), followed by aripiprazole (n = 3687 ICSRs) and quetiapine (n = 2183 ICSRs).
When categorizing according to SMQs and clinical reasoning, the most frequently reported ADRs (Table 1) were related to extrapyramidal syndrome (n = 6630; 14.7%), breast disorders or blood prolactin level changes (n = 2131; 4.7%), cardiac arrhythmias (n = 2080; 4.6%), disturbances in consciousness (n = 2073; 4.6%), and change in weight/body mass index (BMI; n = 1959; 4.3%); together comprising one-third (32.3%) of all reported ADRs. ADRs related to a change in weight/BMI mostly regarded an increase (n = 1811; 92.4%) and less often regarded a decrease (n = 132; 6.7%) or other (e.g., weight fluctuation; n = 16; 0.8%). The results of categorizing according to SOCs are shown in Supplementary Table S1 and Supplementary Figure S1.
ADRs stratified according to gender
In total, 27,536 (60.9%) ADRs were reported in males, 16,654 (36.8%) in females, and for 1011 (2.2%) ADRs the gender was unknown (Table 1). The relative reporting frequencies differed between males and females. Concerning psychiatry-related ADRs, those related to depression and suicide/self-injury (2.3% vs. 4.4%; PRR: 0.5, 95% CI: 0.5 − 0.6), and drug abuse, dependence, and withdrawal (0.9% vs. 1.3%; PRR: 0.7, 95% CI: 0.6 − 0.8), were relatively less frequently reported in males than in females, whereas those related to hostility/aggression (2.2% vs. 1.4%; PRR: 1.6, 95% CI: 1.4 − 1.8) were relatively more frequently reported in males than in females. Other ADRs that were relatively more frequently reported in males were those related to a change in weight/BMI (4.8% vs. 3.5%; PRR: 1.4, 95% CI: 1.2 − 1.5) and breast disorders or blood prolactin level changes (5.2% vs. 4.1%; PRR: 1.2, 95% CI: 1.1 − 1.4). For the latter, the most frequently reported ADR in males was gynecomastia (n = 832; 58.3%), while in females it was galactorrhea (n = 300; 43.5%).
ADRs stratified according to age class
In total, 3232 (7.2%) ADRs were reported in children ages 1 − 5, 11,296 (25.0%) in children ages 6 − 11, and 30,673 (67.9%) in children ages 12 − 17 (Table 1). The relative reporting frequencies differed between age classes.
Concerning neurology-related ADRs, those related to disturbances in consciousness (8.3% vs. 4.2%; PRR: 2.0, 95% CI: 1.7 − 2.2) and convulsions (2.4% vs. 1.6%; PRR: 1.6, 95% CI: 1.2 − 2.0) were relatively more frequently reported in children ages 1 − 5 than in children ages 12 − 17.
Concerning psychiatry-related ADRs, those related to depression and suicide/self-injury (0.5% vs. 4.0%; PRR: 0.1, 95% CI: 0.1 − 0.2), and drug abuse, dependence, and withdrawal (0.7% vs. 1.3%; PRR: 0.6, 95% CI: 0.4 − 0.8), were relatively less frequently reported in children ages 1 − 5 than in children ages 12 − 17, and also relatively less frequently in children ages 6 − 11 than in children ages 12–17 (1.8% vs. 4.0%; PRR: 0.4, 95% CI: 0.4 − 0.5 and 0.5% vs. 1.3%; PRR: 0.4, 95% CI: 0.3 − 0.5, respectively). ADRs related to hostility/aggression were relatively more frequently reported in children ages 6 − 11 than in children ages 12 − 17 (2.9% vs. 1.5%; PRR: 1.9, 95% CI: 1.7 − 2.2).
Concerning endocrine- and metabolism-related ADRs, those related to breast disorders or blood prolactin level changes (1.5% vs. 5.0%; PRR: 0.3, 95% CI: 0.2 − 0.4) and hyperglycemia/new-onset diabetes mellitus (0.6% vs. 1.8%; PRR: 0.4, 95% CI: 0.2 − 0.5) were relatively less frequently reported in children ages 1 − 5 than in children ages 12 − 17. ADRs related to a change in weight/BMI were also relatively less frequently reported in children ages 1 − 5 than in children ages 12 − 17 (2.0% vs. 3.9%; PRR: 0.5, 95% CI: 0.4 − 0.7), while these ADRs were relatively more frequently reported in children ages 6 − 11 than in children ages 12 − 17 (6.1% vs. 3.9%; PRR: 1.5, 95% CI: 1.4 − 1.7).
Other ADRs relatively less frequently reported in children ages 1 − 5 and 6 − 11 than in children ages 12 − 17 were related to hepatic disorders (1.0% vs. 2.1%; PRR: 0.5, 95% CI: 0.3 − 0.7 and 1.4% vs. 2.1%; PRR: 0.7, 95% CI: 0.6 − 0.8, respectively) and hematopoietic cytopenias (1.8% vs. 3.8%; PRR: 0.5, 95% CI: 0.4 − 0.6 and 1.9% vs. 3.8%; PRR: 0.5, 95% CI: 0.4 − 0.6, respectively). Another pronounced difference was found in reported ADRs related to breathing abnormalities and respiratory rate, as these were relatively more frequently reported in children ages 1 − 5 than in children ages 12 − 17 (2.5% vs. 1.1%; PRR: 2.4, 95% CI: 1.9 − 3.0).
ADRs stratified according to reporter type
In total, 11,766 (26.0%) ADRs were reported by consumers and 27,350 (60.5%) by health care professionals (Fig. 2). The relative reporting frequencies differed between consumers and health care professionals. ADRs related to hepatic disorders (1.1% vs. 2.1%; PRR: 0.5, 95% CI: 0.4 − 0.6), cardiac arrhythmias (2.8% vs. 5.4%; PRR: 0.5, 95% CI: 0.5 − 0.6), and hematopoietic cytopenias (1.8% vs. 3.8%; PRR: 0.5, 95% CI: 0.4 − 0.6) were relatively less frequently reported by consumers compared with health care professionals, whereas ADRs related to breast disorders or blood prolactin level changes (9.9% vs. 3.0%; PRR: 3.3, 95% CI: 3.0 − 3.6) and change in weight/BMI (8.7% vs. 2.7%; PRR: 3.2, 95% CI: 2.9 − 3.5) were relatively more frequently reported by consumers compared with health care professionals.
Discussion
This study provides an overview of all spontaneously reported ADRs worldwide (1968–2017) in children and adolescents treated with an antipsychotic drug. Although the most frequently reported ADRs in children were related to extrapyramidal syndrome, breast disorders or blood prolactin level changes, and cardiac arrhythmias, there were a wide spectrum of reported ADRs. Between males and females, there were few prominent differences in the relative reporting frequencies of ADRs. Differences were more strongly observed between different age classes and between health care professionals and consumers.
The most reported ADRs were in line with previous studies' descriptions of ADRs associated with antipsychotics, including extrapyramidal symptoms, metabolic changes, cardiac arrhythmias, and changes in blood prolactin level (De Hert et al. 2011; Pisano et al. 2016; Krause et al. 2018). Previous studies showed differences between ADRs caused by antipsychotics in males and those in females (Smith 2010). Differences were also shown in this study, but these relative differences in reported ADRs in children worldwide were not very prominent. Certain differences in reported ADRs between males and females were expected, as gynecomastia was more reported in males and galactorrhea more in females. More variability was observed in the relative reporting frequencies between different age classes. A previous study of Sagreiya et al. (2017) showed differences in reported ADRs between children, adults, and elderly, whereas this study also shows differences in reported ADRs between younger children and adolescents.
There are various factors that can explain the relative differences in reporting of ADRs between age classes. These differences can be explained by the changes that occur in the human body during a child's development, for instance, in their anatomy and metabolic capacity (Kearns et al. 2003). Another reason for these differences may be the impact of ADRs on children's everyday lives, as in adolescents, gynecomastia can have a high (emotional) impact on the development of self-esteem and sexual identity (Kinsella et al. 2012). In addition, a fear of needles is greatest in younger children and decreases with age (McLenon and Rogers 2018), and therefore, younger children may be less monitored on laboratory parameters due to this fear and some types of ADRs are therefore not noticed. ADRs in younger children are also probably more frequently interpreted and subsequently reported by their parents, while when they grow older they may also identify and report ADRs themselves. The child's perspective can be different than the perspective of the parents or caregivers (Eiser and Varni 2013). Certain ADRs were also expected to be reported less frequently in children ages 1 − 5 than in adolescents, including those related to drug abuse, dependence, and withdrawal.
ADRs were more frequently reported by health care professionals compared with consumers. This is in line with the overall frequency of reporting, irrespective of which drug is used (Star et al. 2011). There were differences between the relative reporting frequency of ADRs reported by health care professionals and those reported by consumers. For example, hepatic disorders and cardiac arrhythmias were relatively more frequently reported by health care professionals, whereas changes in weight/BMI were more frequently reported by consumers. It may be that consumers mostly report those ADRs that influence children's quality of life, that have a high impact on their everyday lives, and are a burden to them, whereas health care professionals might not always count these ADRs as comprising a significant health risk and report more objectively examined ADRs (Schimmelmann et al. 2005). In addition, health care professionals have access to a laboratory or results of an ECG and consumers do not, whereas the latter can measure the weight of the child and experience emotional changes on a daily basis. Because of these differences, it is important for both health care professionals and consumers to report ADRs.
There are several strengths of using the pharmacovigilance system VigiBase. It is by far the largest ADR database and includes real-life events from clinical practice and not only during a study period, so that also long-term, rare, and nonspecific ADRs can come to light (Lindquist 2008; Montastruc et al. 2011). VigiBase is a heterogeneous and worldwide database, with data originating from different sources and types of reporters (Lindquist 2008). In addition, it includes an overall quality-management system (Lindquist 2008).
This study also has some limitations. A pharmacovigilance system is a passive system and includes the risk of underreporting, selective reporting, and missing data (Hazell and Shakir 2006; Hadi et al. 2017), and therefore, there is a risk of reporting bias. Data come from a variety of sources and can be reported incorrectly; no validation of the reported data was performed. Although most reports concerned suspected ADRs, no causality assessment of the evaluated ADR reports was performed nor was the seriousness of the reported ADRs taken into account. In addition, the actual number of children using antipsychotics is unknown; therefore, the use of a pharmacovigilance system implies no quantification of the true risk and no occurrence in absolute terms can be shown (Montastruc et al. 2011). ADRs were categorized by SMQ or clinical reasoning, through which some frequently reported individual ADRs were not included, for example, neuroleptic malignant syndrome and headache. ADRs were not categorized and analyzed by a suspected antipsychotic drug; this was beyond the scope of this study.
Conclusions
A wide spectrum of ADRs were reported in children treated with antipsychotics. Most prominent differences in relative reporting frequencies were observed between age classes and between health care professionals and consumers, and less prominent between genders. The relative differences in reporting frequency can be of help to tailor information about possible ADRs and to monitor for ADRs. By reporting ADRs by health care professionals, children, and their caregivers, new and rare ADRs can come to light in the short and long term, and the frequency of occurrence can become clearer, which is essential in enlarging the knowledge on safety in the use of antipsychotics in children and making more balanced choices in the therapy.
Clinical Significance
The reported ADRs can be serious and may have a great impact on the daily life of a child, and therefore, it is highly important for health care professionals to give children and their caregivers sufficient information about the ADRs that might occur and to monitor the children for ADRs. To provide sufficient information, it is important for the health care professionals to discuss ADRs with children treated with antipsychotics to become more aware of ADRs that are a burden to the child and may influence compliance to therapy. In addition, the child and the caregivers can write down their experiences on a daily basis, to evaluate changes in effect and the occurrence of ADRs in time. Regarding monitoring, clear instructions are needed. Unfortunately, most instructions on monitoring do not provide sufficient and clear information to be applicable in daily clinical practice and are often not completely followed by the health care professionals (Nederlof et al. 2015; Minjon et al. 2018). Reporting of ADRs by both health care professionals and children or their caregivers is important to gain more knowledge on the occurrence of ADRs in children treated with antipsychotics. To stimulate the spontaneous reporting of ADRs and reduce underreporting, education, training, and providing reporters with feedback and incentives are essential (Hadi et al. 2017). Monitoring, reporting, and the awareness of (possible) ADRs by health care professionals, children, and their caregivers could improve the safety of antipsychotic drug use and could help making more balanced choices for antipsychotic drug treatment in children.
Footnotes
Acknowledgment
The authors thank the national pharmacovigilance centers for contributing data to VigiBase.
Disclosures
E.V.D.B. received a travel reimbursement from Medice to attend an international scientific convention on child and adolescent psychiatry (2017). On behalf of all authors, the corresponding author states that there is no conflict of interest.
Disclaimer
The information in this article does not represent the opinion of the WHO, the UMC, or the national centers.
Supplementary Material
Supplementary Table S1
Supplementary Figure S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.